


ISSN: 0973-7510
E-ISSN: 2581-690X
Due to the emergence of antimicrobial-resistance (AR) as a public health threat, the Saudi National Action Plan (SNAP) was implemented in 2017, incorporating various strategies to combat AR. To evaluate the effectiveness of SNAP and the impact of COVID-19, the study analyzed pre- and post-pandemic rates of AR, methicillin-resistant Staphylococcus aureus (MRSA), and multidrug resistance (MDR) among Gram-positive bacteria at a private medical center in Saudi Arabia. This study reviewed the cases of all patients who had been diagnosed with Gram-positive bacterial infection between January 2017 and December 2021. Bacterial strain identification was conducted using VITEK-2 ID-GP cards, while AR, MRSA, and MDR were defined using AST-GP 67 and AST-ST02 cards, all adhering to the manufacturer’s recommended protocols. The five-year study from 2017 to 2021 yielded 6,271 Gram-positive bacteria isolates from patients in a Saudi private hospital. Though the rate of AR initially declined between 2017 and 2019, it spiked significantly from 2020 to 2021. Similarly, the MRSA rate exhibited a substantial decrease (p < 0.05) from 2017 to 2019, followed by a significant rise (p < 0.05) between 2020 and 2021. Out of the isolated pathogens, 1,031 (16.44%) exhibited MDR, with all isolates showing a marked increase (p < 0.05) in MDR from 2020 to 2021. The study highlights the aggravating impact of the COVID-19 pandemic on AR, underscoring the need for the SNAP to intensify its efforts in combating AR.
Antimicrobial Resistance, Saudi National Action Plan, Gram-positive Bacteria, Multi-drug Resistance
The rampant misuse of antimicrobials over the past eight decades has emerged as a critical threat to global health, fostering the emergence of antimicrobial-resistant bacteria that pose an increasingly daunting challenge to treat.1-3 These resistance bacteria are estimated to contribute to 700,000 deaths worldwide each year, with projections indicating a staggering rise to 10 million annual deaths by 2050.4,5 AR is particularly problematic in Gram-positive bacteria, such as Staphylococcus, Streptococcus, and Enterococcus species. These bacteria cause a variety of infections, such as skin infections, pneumonia, and sepsis.6 Therefore, the overuse and improper prescription of antimicrobials significantly contribute to the emergence of methicillin-resistant Staphylococcus aureus (MRSA) and multidrug-resistant (MDR) bacteria.4-6
The World Health Organization (WHO) has implemented a global strategy to combat AR.7,8 This strategy emphasizes raising awareness about AR and its repercussions, supporting research and scientific gatherings to advance knowledge and evidence on AR, optimizing antimicrobials usage, reducing infection rates through effective sanitation and hygiene measures, and increasing investment in novel vaccines, medications, and other AR-fighting interventions.7 In 2017, the Saudi Ministry of Health developed the Saudi National Action Plan (SNAP) on AR. The SNAP is aligned with the WHO’s global action plan and includes many of the same strategies.9-11 The SNAP also includes specific targets for reducing AR in Saudi Arabia, such as reducing the number of MRSA infections by 50% by 2025.9
However, the COVID-19 pandemic has also prompted lifestyle and precautionary measure changes in hospitals and the community, causing the inappropriate and excessive use of antimicrobials for many patients, which could contribute to increased AR.6 The objective of this study was to examine AR trends in Gram-positive bacteria at a private hospital in Riyadh, Saudi Arabia. The study spanned five years, from 2017 to 2021, and involved 6,271 isolates.
Study design
The study employed a retrospective approach, spanning from January 2017 to December 2021, at a 120-bed private medical center in Riyadh, Saudi Arabia. The study examined specimens that had been conclusively diagnosed with a Gram-positive bacterial infection, with a specific focus on those infected with methicillin-susceptible Staphylococcus aureus (MSSA), Coagulase-negative Staphylococci (CoNS), MRSA, Strep. agalactia, Strep. pyogenes, or Enterococcus species; the analysis excluded any Gram-positive bacteria other than those specified. A total of 6,271 Gram-positive bacterial isolates were gathered, identified, and evaluated for their antimicrobials-susceptibility. These isolates were sourced from various units, including outpatient care (2,610/6,271; 41.62%), emergency (2,080/6,271; 33.17%), intensive care unit (581/6,271; 9.27%), multi-service ward (359/6,271; 5.72%), women’s care unit (500/6,271; 7.97%), coronary care unit (30/6,271; 0.48%), progressive care unit (87/6,271; 1.39%), and the labor, delivery, and recovery room (24/6,271; 0.38%). The specimen types collected were urine (2,423/6,271; 38.64%), blood (1,076/6,271; 17.16%), wound (977/6,271; 15.58%), vaginal (1,180/6,271; 18.81%), throat (107/6,271; 1.70%), and other (508/6,271; 8.10%).
Characterizing bacteria and assessing their susceptibility to antimicrobials
The harvested bacteria were cultured on plates containing 5% sheep blood agar (Watin Biolife, KSA) and incubated at 37°C under 5% CO2 for 24 hour. After incubation, a single to three carefully chosen colonies were inoculated into 3 mL of sterile 0.45% sodium chloride solution adjusted to achieve a turbidity of 0.5 McFarland. These bacterial suspensions were subsequently loaded onto testing cards, specifically VITEK-2 ID-GP for identification and AST-GP 67 for antimicrobial-susceptibility testing (AST) of Staphylococcus spp., Enterococcus spp., and S. agalactiae, or AST-ST02 for AST of Streptococcus spp., following the manufacturer’s guidelines.
The VITEK device is an automated fluorescence-based tool that efficiently identifies bacteria and determines their antimicrobial-susceptibility in one step, adhering to the values established by the Clinical and Laboratory Standards Institute (CLSI).12,13 The device compares the growth of the patient’s isolates to those of known minimal inhibitory concentration (MIC) levels stored in the VITEK-2’s server, thus determining the MIC for a particular isolate. The VITEK software (v. 8.01) then uses a standard guideline established by the CLSI to determine interpretive breakpoints.13 Additionally, as per the CLSI’s recommendation, control strains were also administered to ensure the quality of the results including S. aureus ATCC 25923, Enterococcus faecalis ATCC 29212, Strep. agalactiae ATCC 12401, Strep. pyogenes ATCC 19615, and Staphylococcus epidermidis ATCC 12228.13,14
Bacteria are classified as MDR if they exhibit resistance to at least one antimicrobial from three or more distinct antimicrobial categories.15 The study utilized the following antimicrobials for AST: Amoxicillin/Clavulanate (AMC), Penicillin (P), Ciprofloxacin (CIP), Ampicillin (AMP), Cefazolin (CEF), Linezolid (LZD), Gentamicin (CN), Tetracycline (TE), Tigecycline (TGC), Ceftriaxone (CRO), Azithromycin (AZM), Rifampicin (RD), Clindamycin (DA), Trimethoprim/Sulfamethoxazole (SXT), Levofloxacin (LEV), Oxacillin (OX), and Vancomycin (VA). In addition, the antimicrobial-susceptibility testing system used MIC reference ranges according to the manufacturing guidelines.
Ethics statement
The study received ethical approval from the Ethics Committee (ERC) of the College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia. The ERC granted a waiver of patient informed consent due to the retrospective and analytical nature of the study, which relied on data extracted from medical records. In addition, the data were made anonymous and analyzed to protect the privacy of the individuals involved. The study adhered to the ethical principles outlined in the Declaration of Helsinki.
Statistical analysis
Data relevant to the study was collected from the hospital’s laboratory information system (LIS) and then loaded into spreadsheet software (Excel, Microsoft Corp.) for statistical analysis. A mixed-model analysis was implemented using SAS (Statistical Analysis System) software to compare data across different years. To compensate for multiple comparisons, Tukey’s method was utilized, and results with a p-value less than 0.05 were considered statistically significant.
The patterns of antimicrobial-resistance among Gram-positive bacteria from 2017 to 2021
The five-year study resulted in the collection of 6,271 Gram-positive bacterial isolates (Table). Among the isolated organisms, Strep. agalactiae was the most common (3,377/6,271; 53.85%), and the least isolated organism was Strep. pyogenes (90/6,271; 1.44%). Strep. agalactiae exhibited declining or constant resistance to most antimicrobials during the study period, except for antimicrobial AZM and SXT, where resistance levels grew over time. The strongest AR decrease in Strep. agalactiae was shown to be with LEV by -15% (151/656, 23%; 110/689, 16%; 108/719, 15%; 45/639, 7%; 54/674, 8% for the years 2017, 2018, 2019, 2020, and 2021, respectively), however, the strongest AR increasing in Strep. agalactiae was shown to be with AZM by +26% (177/656, 27%; 207/689, 30%; 316/719, 44%; 326/639, 51%; 357/674, 53% for the years 2017, 2018, 2019, 2020, and 2021, respectively). For Strep. pyogenes, the strongest AR decrease was shown to be with DA by -29% (8/19, 42%; 5/22, 23%; 10/30, 33%; 1/4, 25%; 2/15, 13% for the years 2017, 2018, 2019, 2020, and 2021, respectively), however, the strongest AR increasing was observed for AZM with +21% (6/19, 32%; 7/22, 32%; 10/30, 33%; 3/4, 75%; 8/15, 53% for the years 2017, 2018, 2019, 2020, and 2021, respectively).
Table:
Antimicrobial-resistance of isolated Gram-positive bacteria from 2017 to 2021
| Organism name | Year | Number of stains | AMC | AMP | AZM | CIP | CEF | CN | CRO | DA | LEV | LZD | OX | P | RD | SXT | TE | TGC | VA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Strep. agalactiae (Group B Streptococcus) | 2017 | 656 | 0/656 (0%) | 0/656 (0%) | 177/656 (27%, 25-29) | 0/656 (0%) | 328/656 (50%, 47-53) | 151/656 (23%, 19-27) | 0/656 (0%) | 144/656 (22%, 20-24) | 72/656 (11%, 9-13) | 0/656 (0%) | |||||||
| 2018 | 689 | 0/689 (0%) | 0/689 (0%) | 207/689 (30%, 26-34) | 0/689 (0%) | 330/689 (48%, 45-51) | 110/689 (16%, 13-19) | 0/689 (0%) | 117/689 (17%, 15-19) | 117/689 (17%, 14-20) | 0/689 (0%) | ||||||||
| 2019 | 719 | 0/719 (0%) | 0/719 (0%) | 166/719 (23%, 19-27) | 0/719 (0%) | 324/719 (45%, 41-49) | 108/719 (15%, 13-17) | 0/719 (0%) | 108/719 (15%, 13-17) | 71/719 (10%, 8-12) | 0/719 (0%) | ||||||||
| 2020 | 639 | 0/639 (0%) | 0/639 (0%) | 326/639 (51%, 47-55) | 0/639 (0%) | 179/639 (28%, 25-31) | 45/639 (7%, 6-8) | 0/639 (0%) | 6/639 (1%) | 543/639 (85%, 81-89) | 0/639 (0%) | ||||||||
| 2021 | 674 | 0/674 (0%) | 0/674 (0%) | 357/674 (53%, 49-57) | 0/674 (0%) | 303/674 (45%, 42-48) | 54/674 (8%, 6-10) | 0/674 (0%) | 166/674 (25%-22-28) | 47/674 (7%, 6-8) | 0/674 (0%) | ||||||||
| Strep. pyogenes (Group A Streptococcus) | 2017 | 19 | 0/19 (0%) | 0/19 (0%) | 6/19 (32%, 25-39) | 0/19 (0%) | 8/19 (42%, 38-46) | 2/19 (11%, 5-17) | 0/19 (0%) | 2/19 (11%, 5-17) | 4/19 (21%, 18-24) | 0/19 (0%) | |||||||
| 2018 | 22 | 0/22 (0%) | 0/22 (0%) | 7/22 (32%, 25- 39) | 0/22 (0%) | 5/22 (23%, 17-29) | 1/22 (5%) | 0/22 (0%) | 1/22 (5%) | 4/22 (18%, 14-22) | 0/22 (0%) | ||||||||
| 2019 | 30 | 0/30 (0%) | 0/30 (0%) | 10/30 (33%, 25-41) | 0/30 (0%) | 10/30 (33%, 27-39) | 3/30 (10%, 5-15) | 0/30 (0%) | 2/30 (6%) | 5/30 (17%, 12-22) | 0/30 (0%) | ||||||||
| 2020 | 4 | 0/4 (0%) | 0/4 (0%) | 3/4 (75%, 60-90) | 0/4 (0%) | 1/4 (25%) | 0/4 (0%) | 0/4 (0%) | 1/4 (25%) | 1/4 (25%) | 0/4 (0%) | ||||||||
| 2021 | 15 | 0/15 (0%) | 0/15 (0%) | 8/15 (53%, 45-61) | 0/15 (0%) | 2/15 (13%) | 2/15 (13%) | 0/15 (0%) | 0/15 (0%) | 5/15 (33%, 25-41) | 0/15 (0%) | ||||||||
| MSSA | 2017 | 183 | 0/183 (0%) | 53/183 (29%, 25-33) | 31/183 (17%, 13-21 | 0/183 (0%) | 9/183 (5%, 3-7) | 4/183 (2%, 1-3) | 6/183 (3%, 1-5) | 103/183 (56%, 51-61) | 0/183 (0%) | 11/183 (6%, 2-4) | 28/183 (15%, 12-18) | 0/183 (0%) | 4/183 (2%, 1-3) | ||||
| 2018 | 112 | 1/112 (1%) | 28/112 (25%, 22-28) | 8/112 (7%, 5-9) | 0/112 (0%) | 1/112 (1%) | 7/112 (6%, 4-8) | 0/112 (0%) | 81/112 (72%, 69-75) | 1/112 (1%) | 2/112 (2%, 1-3) | 10/112 (9%, 8-10) | 0/112 (0%) | 1/112 (1%) | |||||
| 2019 | 137 | 0/137 (0%) | 37/137 (27%, 24-30) | 12/137 (9%, 7-11) | 0/137 (0%) | 3/137 (2%, 1-3) | 3/137 (2%, 1-3) | 0/137 (0%) | 67/137 (49%, 41-56) | 0/137 (0%) | 8/137 (6%, 4-8) | 15/137 (11%, 8-14) | 0/137 (0%) | 0/137 (0%) | |||||
| 2020 | 107 | 0/107 (0%) | 35/107 (33%, 31-35) | 10/107 (9%, 8-10) | 0/107 (0%) | 1/107 (1%) | 8/107 (7%, 6-8) | 0/107 (0%) | 78/107 (73%, 70-76) | 0/107 (0%) | 5/107 (5%, 3-7) | 9/107 (8%, 6-10) | 0/107 (0%) | 0/107 (0%) | |||||
| 2021 | 216 | 43/216 (20%, 17-23) | 67/216 (31%, 28-34) | 43/216 (20%, 16-24) | 24/216 (11%, 10-12) | 9/216 (4%, 3-5) | 24/216 (11%, 8-14) | 0/216 (0%) | 202/216 (94%, 91-97) | 0/216 (0%) | 30/216 (14%, 12-16) | 24/216 (11%, 9-13) | 0/216 (0%) | 0/216 (0%) | |||||
| MRSA | 2017 | 149 | 78/149 (52%, 50-54) | 76/149 (51%, 47-55) | 45/149 (30%, 26-34) | 73/149 (49%, 45-53) | 49/149 (33%, 31-35) | 40/149 (27%, 23-31) | 58/149 (39%, 36-42) | 22/149 (15%, 13-17) | 24/149 (16%, 13-19) | 21/149 (14%, 12-16) | |||||||
| 2018 | 124 | 33/124 (27%, 25-29) | 52/124 (42%, 40-44) | 21/124 (17%, 14-20) | 19/124 (15%, 12-18) | 1/124 (1%) | 3/124 (2%) | 31/124 (25%, 22-28) | 30/124 (24%, 21-27) | 1/124 (1%) | 1/124 (1%) | ||||||||
| 2019 | 116 | 34/116 (29%, 26-32) | 52/116 (45%, 43-47) | 38/116 (33%, 31-35) | 16/116 (14%, 12-16) | 0/116 (0%) | 1/116 (1%) | 27/116 (23%, 19-27) | 22/116 (19%, 16-22) | 0/116 (0%) | 0/116 (0%) | ||||||||
| 2020 | 83 | 18/83 (22%, 21-23) | 27/83 (33%, 29-37) | 7/83 (8%, 7-9) | 3/83 (4%, 3-5) | 0/83 (0%) | 7/83 (8%, 7-9) | 7/83 (8%, 6-10) | 22/83 (27%, 24-30) | 0/83 (0%) | 0/83 (0%) | ||||||||
| 2021 | 251 | 145/251 (58%, 63-53) | 135/251 (54%, 57-51) | 95/251 (38%, 36-40) | 123/251 (49%, 54-44) | 23/251 (9%, 7-11) | 73/251 (29%, 27-31) | 75/251 (30%, 27-33) | 73/251 (29%, 27-31) | 13/251 (5%, 4-6) | 23/251 (9%, 5-13) | ||||||||
| CoNS | 2017 | 125 | 98/125 (78%, 75-81) | 55/125 (44%, 41-47) | 75/125 (60%, 55-65) | 50/125 (40%, 37-43) | 26/125 (21%, 19-23) | 25/125 (20%, 16-24) | 94/125 (75%, 71-79) | 0/125 (0%) | 35/125 (28%, 26-30) | 30/125 (24%, 22-26) | 11/125 (9%, 7-11) | 18/125 (14%, 11-17) | |||||
| 2018 | 171 | 123/171 (72%, 70-74) | 130/171 (76%, 71-81) | 72/171 (42%, 39-45) | 51/171 (30%, 27-33) | 72/171 (42%, 40-44) | 2/171 (1%) | 128/171 (75%, 73-77) | 7/171 (4%, 3-5) | 48/171 (28%, 24-32) | 68/171 (40%, 36-44) | 2/171 (1%) | 2/171 (1%) | ||||||
| 2019 | 163 | 88/163 (54%, 51-57) | 90/163 (55%, 52-58) | 46/163 (28%, 25-31) | 28/163 (17%, 14-20) | 44/163 (27%, 25-29) | 2/163 (1%) | 91/163 (56%, 53-59) | 8/163 (5%, 4-6) | 28/163 (17%, 15-19) | 52/163 (32%, 30-34) | 2/163 (1%) | 2/163 (1%) | ||||||
| 2020 | 81 | 55/81 (68%, 65-71) | 62/81 (77%, 72-82) | 33/81 (41%, 35-47) | 33/81 (41%, 39-43) | 41/81 (51%, 48-54) | 0/81 (0%) | 56/81 (69%, 66-72) | 2/81 (2%) | 26/81 (32%, 30-34) | 27/81 (33%, 30-36) | 0/81 (0%) | 0/81 (0%) | ||||||
| 2021 | 340 | 276/340 (81%, 85-77) | 241/340 (71%, 67-75) | 187/340 (55%, 51-59) | 180/340 (53%, 48-58) | 109/340 (32%, 29-35) | 31/340 (9%, 8-10) | 241/340 (71%, 67-75) | 31/340 (9%, 7-11) | 109/340 (32%, 29-35) | 92/340 (27%, 25-29) | 31/340 (9%, 8-10) | 31/340 (9%, 8-10) | ||||||
| Enterococcus spp. | 2017 | 98 | 3/98 (3%, 2-4) | 2/98 (2%, 1-3) | 15/98 (15%, 13-17) | 0/98 (0%) | 4/98 (4%, 3-5) | 7/98 (7%, 5-9) | |||||||||||
| 2018 | 85 | 2/85 (2%, 1-3) | 1/85 (1%) | 15/85 (18%, 16-20) | 0/85 (0%) | 2/85 (2%, 1-3) | 5/85 (6%, 5-7) | ||||||||||||
| 2019 | 78 | 2/78 (3%, 2-4) | 2/78 (3%, 1-5) | 11/78 (14%, 11-17) | 0/78 (0%) | 2/78 (3%, 2-4) | 2/78 (3%, 2-4) | ||||||||||||
| 2020 | 79 | 3/79 (4%, 2-6) | 2/79 (3%, 2-4) | 16/79 (20%, 15-25) | 0/79 (0%) | 1/79 (1%) | 6/79 (6%, 4-8) | ||||||||||||
| 2021 | 106 | 5/106 (5%, 2-8) | 5/106 (5%, 2-8) | 30/106 (28%, 25-31) | 0/106 (0%) | 4/106 (4%, 3-5) | 5/106 (5%, 2-8) |
Data presented as n/N (%, 95% CI). AMC (Amoxicillin/Clavulanate), AMP (Ampicillin), AZM (Azithromycin), CIP (Ciprofloxacin), CEF (Cefazolin), CN (Gentamicin), CRO (Ceftriaxone), DA (Clindamycin), LEV (Levofloxacin), LZD (Linezolid), OX (Oxacillin), P (Penicillin), RD (Rifampicin), SXT (Trimethoprim/Sulfamethoxazole), TE (Tetracycline), TGC (Tigecycline), VA (Vancomycin).
For MSSA and MRSA, the proportion of AR isolates was 755/6,271 (12.04%) and 723/6,271 (11.53%), respectively. For MSSA, the greatest decline in AR occurred for treatment with TE at -4% (28/183, 15%; 10/112, 9%; 15/137, 11%; 9/107, 8%; 24/216, 11% during the period of 2017, 2018, 2019, 2020, and 2021, respectively), though for MRSA, the greatest decrease was for LZD with -24% (49/149, 33%; 1/124, 1%; 0/116, 0%; 0/83, 0%; 23/251, 9%). However, the strongest AR increasing for MSSA was observed for P with +38% (103/183, 56%; 81/112, 72%; 117/137, 85%; 78/107, 73%; 202/216, 94% for the years 2017, 2018, 2019, 2020, and 2021, respectively), while for MRSA, the strongest AR increasing was observed for TE with +14% (22/149, 15%; 30/124, 24%; 22/116, 19%; 22/83, 27%; 73/251, 29%).
For CoNS and Enterococcus species, the proportion of AR strains was 880/6,271 (14.03%) and 446/6,271 (7.11%), respectively. In CoNS, only four antimicrobials exhibited a decrease in resistance levels throughout the study period including CIP with -5%, LZD with -11%, OX with -4% and VA with -5%, while Enterococcus species displayed decreased resistance only for VA with -2%. However, the strongest AR increasing for CoNS was observed for AZM with +27% (55/125, 44%; 130/171, 76%; 90/163, 55%; 62/81, 77%; 99/140, 71% for the years 2017, 2018, 2019, 2020, and 2021, respectively), while for Enterococcus species, the strongest AR increasing was observed for LEV with +13% (15/98, 15%; 15/85, 18%; 13/78, 17%; 16/79, 20%; 30/106, 28%).
The prevalence of MRSA and MDR Gram-positive bacteria has increased from 2017 to 2021
For MRSA clinical isolates, 723/2,358 (30.66%) were obtained from Staphylococcus species in total (Figure 1). The proportion of MRSA decreased significantly (p < 0.05) with values of -4.72% (32.60% to 27.88%) for the years 2017 to 2019, respectively. However, the overall data demonstrated a significant increase (p < 0.05) in MRSA from 2017 compared to 2021 with +8.75% (32.60% to 41.35%, respectively). The highest rate of increase was displayed (p < 0.05) with +13.47% (27.88% to 41.35%) from 2019 compared to 2021, respectively.
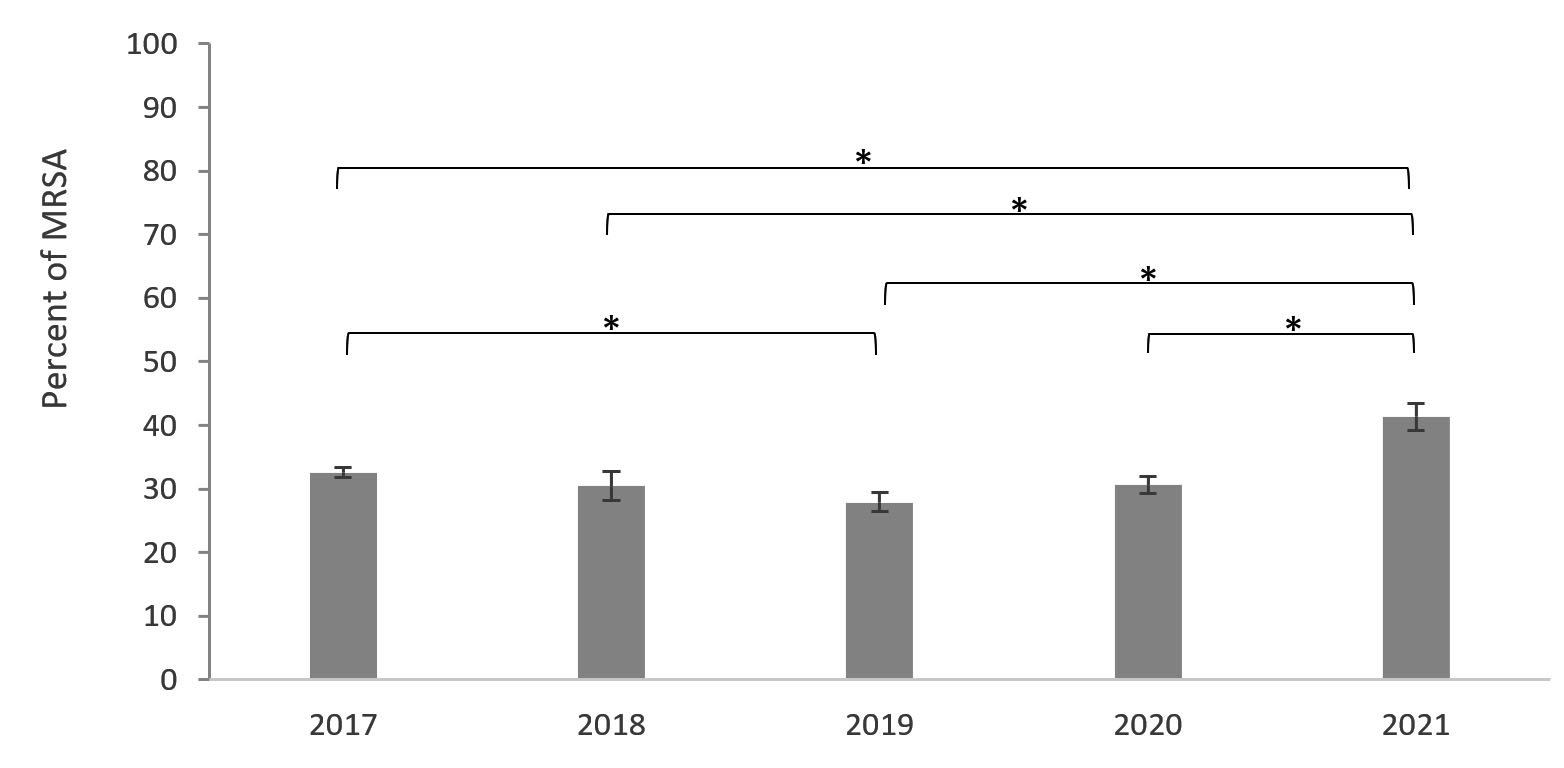
Figure 1. A five-year evaluation of MRSA. Results were presented as percentage ±SD of MRSA of isolated bacteria compared to Staphylococcus species. Mixed-model analysis was performed for the multiple comparisons, and * indicates a significant difference in MRSA between years (p < 0.05).
The proportion of Gram-positive isolates that were MDR was 1031/6,271; 16.44%
(Figure 2). The most isolated MDR bacteria was CoNS (315/880; 35.80%), followed by MRSA (174/723; 24.07%), and MSSA (136/755; 18.01%). Overall, the percentage of MDR bacteria among AR isolates from a specific genus dropped significantly from 2017 to 2020 (p < 0.05); however, Strep. pyogenes and Enterococcus species were exceptions to this trend (Figure 2). Interestingly, all pathogens displayed a significant increase in MDR (p < 0.05) from 2020 to 2021. It is noteworthy that MSSA demonstrated the greatest escalation in MDR cases with +9% (17%, 31/183; 26%, 56/216) for the years 2017 and 2021, respectively.
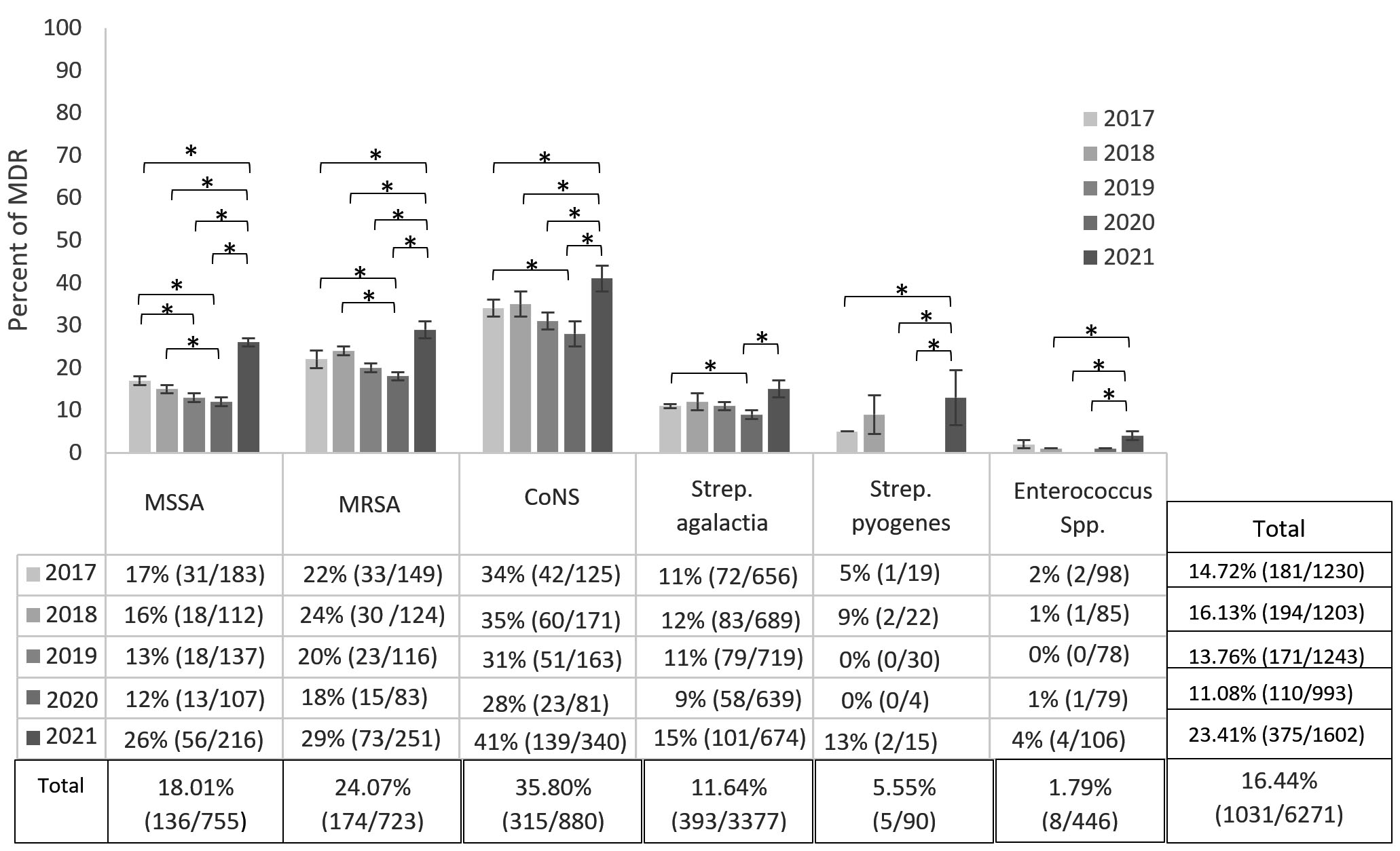
Figure 2. A five-year evaluation of MDR of isolated gram-positive bacteria. Results were presented as percentage ±SD of MDR of isolated bacteria compared to their antibiotic resistance strain. Mixed-model analysis was performed for the multiple comparisons, and * indicates a significant difference in MDR between years (p < 0.05)
The proliferation of AR pathogens is a serious worry for physicians and scientists.3 In Saudi Arabia, the easy accessibility of antimicrobials without a prescription, coupled with self-medication practices and incomplete antibiotic courses, fuels the emergence of AR bacteria.16,17 A 2014 study demonstrated that approximately 78% of people in Saudi Arabia had self-medicated with antimicrobial drugs at some point in their lives.17 Another study conducted in 2015 revealed that antimicrobial misuse is prevalent in Saudi Arabia, with almost 64% of individuals consuming antimicrobials without a prescription and approximately 71% failing to complete prescribed antibiotic regimens.16 The absence of programs to monitor AR has caused healthcare staff and patients using antibiotics inappropriately.18 This enables bacteria to transfer AR genes and resistance-boosting factors, contributing to the spread of MRSA and MDR bacteria. These infections can be more difficult to treat and can lead to higher mortality rates.19-21 Additionally, the introduction of effective antimicrobial drugs has slowed down, and the options for overcoming AR are limited.19,20
This study aimed to determine the levels of AR, including MRSA and MDR, in major Gram-positive bacterial pathogens found in patients at a private Saudi Arabian hospital. From January 2017 through December 2021, a total of 6,271 Gram-positive bacteria isolates were accumulated for analysis. This study found a high prevalence of Strep. agalactiae (3,377/6,271; 53.85%), similar to the 76.2% reported by Atif Asghar in Hera General Hospital in Makkah, Saudi Arabia.21 Interestingly, this study deviates from those of Aldawsari et al. and Al Mutair et al., who reported Staph. aureus as the leading Gram-positive bacteria in their Saudi Arabian studies.22,23
From 2017 to 2019, the study observed a general decrease in AR in all studied bacteria. This is consistent with findings from other studies, such as those by Aldawsarie et al. and Wang et al., which were conducted after the implementation of a national action plan to combat AR.22,24 MSSA exhibited the dramatic drop with the antibiotic CIP (-8%), while for MRSA had DA (-35%), and Enterococcus species had VA (-4%). Contrary to this study, an Iranian study, absent systematic antibiotic guidelines, reported continuous increases in AR against most antibiotics. In particular, from 2015 to 2018, the study found that the resistance of Staph. aureus to CIP increased by 46%, the resistance of Enterococcus species to AMP increased by 13%, and CoNS to CN increased by 14%.25 The contrast between the findings of this study and the study conducted in Iran emphasizes the importance of monitoring AR. This research identified instances where specific bacterial strains completely overcame their resistance to certain antimicrobials within a three-year period. Similarly, MRSA treated with LZD exhibited a significant decline in resistance, transitioning from 49/149 isolates in 2017 to 0/116 isolates in 2019 (a decrease from 33% to 0%).
The results of this study suggest that monitoring AR is crucial in the fight against potentially devastating infections, its benefits are undeniable. This approach helps track drug resistance in bacteria, leading to better antimicrobial choices, shorter hospital stays, and ultimately, saving lives.26 In addition, SNAP tackles the treat of drug-resistant infections head-on, both by closely monitoring their spread through sentinel sites and by safeguarding critically important antibiotics from overuse in animal agriculture.10 While the long-term effects of these two recently implemented strategies are promising, more data is needed to fully understand their impact.
In March 2017, SNAP took a big step in tackling antimicrobial resistance by adapting and implementing the WHO’s global surveillance system, GLASS. This powerful tool, designed to track drug-resistant bacteria, prioritized monitoring MRSA and MDR strains. In addition, recognizing the looming threat of MRSA and MDR bacteria, the Saudi Arabia Health Ministry, in April 2017, requested a stewardship program key performance indicator (KPI). This KPI, would monitor the effectiveness of interventions against these drug-resistant superbugs, ensuring they stay under control.10 After implementing these strategies, the data revealed a significant decrease in the prevalence of MRSA and MDR isolate (p < 0.05). This decrease is consistent with findings from other studies, such as those by US Centers for Disease Control and Prevention (CDC) and Majumder et al.27,28 The decline of MRSA and MDR unlocks a double win; treatment success rates rise, reducing complications and hospital stays, while healthcare systems face less strain from these stubborn infections.6,29,30
In early 2020, the first case of COVID-19 was reported in Saudi Arabia.31 Since then, scientists have cautioned against the misuse of antimicrobial drugs, even though there is clinical evidence that suggests that bacterial co-infections can occur during viral epidemics.31,32 Antimicrobial use is expected to be high in Saudi Arabian Hospitals due to the severity of the diseases treated and the number of interventions given to patients.32,33 A recent study found that, during the COVID-19 outbreak, there was an increase in the sale of non-prescription antimicrobial drugs by Saudi pharmacies. In 2020, a study showed a reduction in the total number of isolated pathogens in the hospital, as well as a reduction in AR, MRSA, and MDR. This was likely due to COVID-19 control measures such as school closures, and lockdowns. However, in 2021, another study displayed that AR increased for most isolated Gram-positive bacteria and significantly increased for MRSA (p < 0.05) compared to all previous years. In addition, all isolated pathogens showed a significant increase for MDR in 2021 compared to other years. These findings are consistent with other studies that have shown that the misuse of antibiotics during COVID-19 can lead to an increase in AR bacteria and MDR.6,32,33 A systemic review estimated that a staggering 88% of people engaged in self-medication with antimicrobials and other drugs during the pandemic.34 Another study from India found that approximately of 216 million doses of antibiotics were sold in 2020 alone.35
While this study demonstrates the effectiveness of SNAP’s strategies in reducing AR from 2017 to 2019, it’s important to acknowledge some limitations that may influence the interpretation of this study: 1) missing clinical data: the study lacked access to vital information like treatment outcomes and mortality rates linked to Gram-positive bacteria, limiting the study analysis scope; 2) incomplete control groups: for some variables, this study couldn’t establish appropriate control groups, potentially impacting the strength of the study comparisons; 3) Enterococcus genus: we couldn’t identify specific Enterococcus species, hampering the study ability to pinpoint AR and infection rates within this genus; 4) policy dynamics ignored: the analysis didn’t factor in potential annual changes in hospital policies driven by COVID-19, physician recommendations, and antibiotic availability; 5) Gram-negative exclusion: the study focused solely on Gram-positive bacteria, excluding a major category relevant to AR trends; 6) Variable sample sizes: year-to-year disparities in the number of tested isolates could introduce inconsistencies in the data. However, during COVID-19, the misuse of antibiotics led to an increase in AR for most isolated pathogens. Therefore, to reach a significate AR reduction and a 50% reduction in MRSA by 2025 as indicated in SNAP, more work needs to be done to implement the SNAP strategies and increase the public’s awareness about AR. To truly solidify the impact of SNAP’s plan, future studies encompassing more hospitals and a wider timeframe are crucial.
This study revealed that the implementation of SNAP had led to a marked reduction in AR among Gram-positive bacteria, with significant success against MRSA and MDR. Furthermore, this research from 2017 to 2019 exhibited that certain bacterial strains acquired complete susceptibility to certain antimicrobials. Notably, MSSA strains demonstrated fully susceptibility to VA, and MRSA strains achieved complete susceptibility to LZD. Though implemented strategies aimed to manage antimicrobial-resistance, the pandemic unfortunately witnessed a rise in resistance to all types of antimicrobials. This underlines the urgency of further research to optimize control measures and keep pace with this evolving threat.
ACKNOWLEDGMENTS
The author would like to thank all the Hospital Laboratory members and Imam Mohammad Ibn Saud Islamic University for their support. The author is also thankful for and appreciates Bayan Abalkhail’s data analysis and comments on the article.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Ethics Committee (ERC) of the College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia.
- O’Brien TF, Clark A, Peters R, Stelling J. Why surveillance of antimicrobial resistance needs to be automated and comprehensive. J Glob Antimicrob Resist. 2018;17:8-15.
Crossref - Sharahi JY, Azimi T, Shariati A, Safari H, Tehrani MK, Hashemi A. Advanced strategies for combating bacterial biofilms. J Cell Physiol. 2019;234(9):14689-14708.
Crossref - Ventola CL. The antibiotic resistance crisis: part1: causes and threats. PT. 2015;40(4):277-283.
- Dadgostar P. Antimicrobial resistance: Implications and Costs. Infect. Drug Resist. 2019;12:3903-3910.
Crossref - O’Neill J. Antimicrobial Resistance Tacking a crisis for the Health and Wealth of Nations/the review on Antimicrobial Resistance Chaired by Jim O’Neill. Available online: https://wellcomecollection.org/works/pdpck35v Accessed May 23, 2024
- Fernandez-Espigares L, Hernandez-Chico I, Exposito-Ruiz M, Rosales-Castillo A, Navarro-Mari JM, Gutierrez-Fernandez J. Antibiotic Resistance Changes in Gram-Positive Bacteria from Urine Cultures: Development Analysis in a Health Area of South-East Spain. Antibiotics. 2023; 12(7):1133.
Crossref - World Health Organization. Global action plan on antimicrobial resistance; 2016. Availble online: https://www.who.int/publication/i/item/9789241509763 Accessed May 23, 2024
- World Health Organization. Global action plan on antimicrbial resistance surveillance system (GLASS) report: early implementataion 2017-2018. 2017. Available online: https://www.who.int/publications/i/item/9789241515061. Accessed May 23, 2024
- Saudi Ministry of Health. WHO publishes the saudi national action plan for combating antibiotic-resistant bacteria on its portal. Available online: https://www.moh.gov.sa/en/ministry/mediacenter/news/pages/news-2017-11-19-002.aspx Accessed on May 23, 2024
- Public Health Authority. Antimicrobial resistance (AMR) action plan kingdom of Saudi Arabia 2022-2025. Available online: https://cdn.who.int/media/docs/default-source/antimicrobial-resistance/amr-spc-npm/nap-library/kingdom-of-saudi-arabia-nap-amr-2022-2025.pdfsfvrsn=722aaed5_3&download=true Accessed May 23, 2024
- National Guard Health Affairs. Infection prevention and control manual. 2013. Available online: https://www.moh.gov.sa./ccc/deocuments/GCC%20infection%20control%20manual%202013%20revisedOPT.pdf Accessed May 23, 2024
- Funke G, Monnet D, deBernardis C, von Graevenitz A, Freney J. Evaluation of the VITEK 2 system for rapid identification of medically relevant gram-negative rods. J Clin Microbiol. 1998;36(7):1948-1952.
Crossref - Clinical and Laboratory Standards Institute. Performace standards for antimicrobial suspectibility testing; Twenty-fouth Informational Supplement. 2014. Availabel online: https://webstore.ansi.org/standards/clsi/clsim100s24?srsltid=afmBoopFC2LRLtS1j9byRBj1 WkUdXI5pWU4S2Y0AsFOS9Yc8tTu6ePKi. Accessed May 23, 2024
- Wang M, Wei H, Zhao Y, et al. Analysis of multidrug-resistant bacteria in 3223 patients with hospital-acquired infections (HAI) from a tertiary general hospital in China. Bosn J Basic Med Sci. 2019;19(1):86-93.
Crossref - Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268-281.
Crossref - El Zowalaty ME, Belkina T, Bahashwan SA, et al. Knowledge, awareness, and attitudes toward antibiotic use and antimicrobial resistance among Saudi population. Int J Clin Pharm. 2016;38(5):1261-1268.
Crossref - Al Rasheed A, Yagoub U, Alkhashan H, et al. Prevalence and predictors of self-medication with antibiotics in Al Wazarat Health Center, Riyadh City, KSA. Biomed Res Int. 2016;12:1-8.
Crossref - Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015:109(7):309-318.
Crossref - Laws MR, Shaaban A, Rahman KM. Antibiotic resistance breakers: current approaches and future directions. FEMS Microbiol Rev. 2019;43(5):490-516.
Crossref - Alabdullatif M, Atreya CD, Ramirez-Arcos S. Antimicrobial peptides: an effective approach to prevent bacterial biofilm formation in platelet concentrates. Transfusion. 2018;58(8):2013-2021.
Crossref - Asghar AH. Frequency and antibiotic susceptibility of gram-positive bacteria in Makkah hospitals. Ann Saudi Med. 2011;31:462-468.
Crossref - Aldawsari A, Tawfik K, and Al-Zaggi I. Antimicrobial-resistant bacteria and prescription of antibiotics at a tertiary care hospital in Riyadh, Saudi Arabia. Cureus. 2020;12(12):e12098.
Crossref - Al Mutair A, Alhumaid S, Al Alawi Z, et al. Five-year resistance trends in pathogens causing healthcare-associated infections at a multi-hospital healthcare system in Saudi Arabia, 2015-2019. J Glob Antimicrob Resist. 2021;25:142-150.
Crossref - Wang S, Hu YJ, Little P, et al. The impact of the national action plan on the epidemiology of antibiotic resistance among 352,238 isolates in a teaching hospital in China from 2015 to 2018. Antimicrob Resist Infect Control. 2019;8:22.
Crossref - Azimi T, Maham S, Fallah F, Azimi L, Gholinejad Z. Evaluating the antimicrobial resistance patterns among major bacterial pathogens isolated from clinical specimens taken from patients in Mofid Children’s Hospital, Tehran, Iran: 2013-2018. Infect Drug Resist. 2019;12:2089-2102.
Crossref - Browne AJ, Kashef Hamadani BH, Kumaran EAP, et al. Drug-resistant enteric fever worldwide, 1990 to 2018: a systematic review and meta-analysis. BMC Med. 2020;18(1):1.
Crossref - Jones M, Jernigan JA, Evans ME, Roselle GA, Hatfield KM, Samore MH. Vital signs: trends in Staphylococcus aureus infections in veterans affairs medical centers – United States, 2005-2017. MMWR Morb Mortal Wkly Rep. 2019;68(9):220-224.
Crossref - Majumder M, Rahman S, Cohall D, et al. Antimicrobial stewardship: Fighting antimicrobial resistance and protecting global public health. Infect Drug Resist. 2020;13:4713-4738.
Crossref - Founou RC, Founou LL, Essack SY. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS One. 2017;12(12):e0189621.
Crossref - Peters L, Olson L, Khu DTK, et al. Multiple antibiotic resistance as a risk factor for mortality and prolonged hospital stay: A cohort study among neonatal intensive care patients with hospital-acquired infections caused by gram-negative bacteria in Vietnam. PLoS One. 2019;14(5):e0215666.
Crossref - Natto ZS, Alshaeri HK. Characteristics of first cases of coronavirus disease 2019 and the effort to prevent the early spread of COVID-19 in Saudi Arabia. Risk Manag Healthc Policy. 2021;14:315-321.
Crossref - Kabrah A, Bahwerth F, Alghamdi S, et al. Antibiotics usage and resistance among patients with severe acute respiratory syndrome coronavirus 2 in the intensive care unit in Makkah, Saudi Arabia. Vaccines. 2022;10(12):2148.
Crossref - Taha I, Abdou Y, Hammad I, et al. Utilization of antibiotics for hospitalized patients with severe coronavirus disease 2019 in Al-madinah Al-munawara, Saudi Arabia: a Retrospective Study. Infect Drug Resist. 2022;15:7401-7411.
Crossref - Quincho-Lopez A, Benites-Ibarra CA, Hilario-Gomez MM, et al. Self-medication practices to prevent or manage COVID-19: a systematic review. PLoS One. 2021;16(11):e0259317.
Crossref - Sulis G, Batomen B, Kotwani A, Pai M, Gandra S. Sales of antibiotics and hydroxychloroquine in India during the COVID-19 epidemic: an interrupted time series analysis. PLoS Med. 2021;18(7):e1003682.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.