


ISSN: 0973-7510
E-ISSN: 2581-690X
Antibiotic resistance is considered a widespread problem with global health implications, leading to increased patient morbidity and impacting the selection of effective antibiotics, consequently influencing patient recovery. This study aimed to assess antibiogram resistance patterns of bacterial records at the Islamic Hospital in Jordan using a retrospective study during the period 2020-2022. A total of 9369 samples obtained from different patients were cultured. Data were processed and analyzed with SPSS v.23.0. The results showed that 2841 (30.3%) samples were positive for bacterial infections. Microbial profiles of positive samples indicated the highest proportion for Escherichia coli, 39%, followed by Klebsiella pneumoniae 12% were the most frequent Gram-negative bacterial isolates, whereas Staphylococcus aureus 13% and Streptococcus pneumoniae 4% were the most common Gram-positive bacterial isolates. Interestingly, multidrug-resistant bacteria comprised 61.7% of the isolates. The percentage of multi-drug resistance in isolates of Staphylococcus aureus, Escherichia coli, and Klebsiella pneumoniae was 68.7%, 73.1%, and 72%, respectively. Escherichia coli was most resistant to ampicillin (89%) and most sensitive to imipenem (100%). Klebsiella pneumoniae showed a 100% sensitivity to meropenem but 49% resistance to ceftriaxone. Pseudomonas aeruginosa was the most sensitive to amikacin and colistin (86% and 100%, respectively). Staphylococcus aureus isolates have resistance rates of 78% for ciprofloxacin, 35.6% for clindamycin and an overall resistance rate of 68.7%. These findings indicate multiple resistance for isolated bacteria. Therefore, antimicrobial resistance should be monitored continuously, and patients should be treated based on anti-microbial susceptibility tests.
Antibiogram, Antimicrobial Resistance, Bacterial Isolates, Clinical Specimen, Jordan
Multi-drug resistance (MDR) microbial limits treatment choices and is becoming a global health problem. The severity of diseases caused by bacteria and other microbes that have developed resistance is rising worldwide.1 A consequence of that increase in healthcare expenses is a cause of the community’s health and economic problems.
According to the 2020 World Health Organization (WHO) report, MDR is one of the most serious worldwide risks in infectious diseases.2 Medicines are becoming less effective, and germs are becoming more resistant to both first and last-line medicines, according to data collected throughout the world. As a result, the effects of antibiotic resistance might be thought of as clinical, economic, and societal factors.3 Moreover, Hospital patients develop an infection during their admission and critical care unit stay.4
MDR has a huge impact; new bacterial strains will reduce healthcare services.5 Microbial infections cause at least 25% of the world’s 60 million deaths yearly.6 Clinical infections with drug-resistant pathogens continue to be major causes of morbidity and mortality among hospitalized patients and in the community, affecting developed countries, middle-income countries, and middle countries like Jordan despite tremendous advances in infection control procedures.5-7
In clinical and community settings, the most frequently isolated organisms from infections include Escherichia coli, Staphylococcus aureus, Streptococcus pneumoniae, Pseudomonas aeruginosa. and Klebsiella pneumoniae.8,9 They are also the bacteria that are now most seriously resistant to antibiotics, such as carbapenem-resistant Enterobacteriaceae.10
Drug resistance is a serious problem in low-income nations because of the high incidence of illnesses, inappropriate use of antibiotics, over-the-counter access to medications, and limitations on the availability of testing for antibiotic susceptibility.10-13 Therefore, continuous monitoring of the rise of drug resistance is required to facilitate the proper choice of antimicrobial drugs and lower diseases like nosocomial illness brought on by the rise of drug-resistant bacteria.14 The current state of antibiotic use will cause approximately 10 million people to be at risk by 2050.15
One of the main strategies suggested by the USA-CDC and the Jordanian Ministry of Health to reduce the spread of MDR is early detection as an action at the local and regional levels. Regretfully, comprehensive information regarding the antibiogram of bacterial pathogens isolated from illnesses from several Middle Eastern study participants, including Jordan, is lacking. Therefore, this study seeks to provide extensive information on microbial profiles and antibiogram patterns for patients from a private Islamic Hospital ISH during 2020-2022. Furthermore, our work gathered over three years of information on aerobic bacteria from patients at ISH General Hospital. The data presented here indicate the most abundant MDR pathogenic bacteria that might be developed in the hospitals in Jordan. In addition, provides information on antibiotic sensitivity, which is considered very important for physicians and decision-makers at the Ministry of Health in terms of establishing a medical protocol for the antibiotics used for the patients in hospitals.
Research sample
The research samples of this study were obtained from patients in a private, multispecialty teaching hospital called Islamic Specialized Hospital (ISH), located in Amman, Jordan. A retrospective study was conducted during the period January 2020 – December 2022. All regular and referral cases from the area receive medical care. Every year, 300 new patients, on average, pass through it. The research population consisted of all presumed bacterial infection patients admitted to ISH.
Ethical approval
The study was conducted in accordance with The Institutional Review Board (IRB) committee at Balqa Applied University, granted ethical approval (ref. No. ERC 18/2/3/18/2620). The ISH Office of the Medical Director granted permission to collect data. The paperwork did not include the name and other patient identifications to maintain privacy.
Identification of microorganisms
All the bacterial isolates under the study were identified depending on biochemical tests and morphological characteristics.16 The identification was confirmed using the Vitek-2 system (BioMeriuex, France). Clinical specimens were obtained using standard operating procedures as indicated by Freeman et al.17 These included swabs from Urine samples, vaginal and cervical discharge, pus discharge, blood, cerebral fluids, urethral discharge, stool, eye discharge, ear discharge, other body fluids and semen. Depending on the source of the specimen, each sample was cultivated onto Blood agar, Mannitol Salt agar, MacConkey agar, Xylose Lysine Deoxycholate agar, Chocolate agar, or Thayer-Martin agar (Oxoid, UK) depending on the material’s source and was then aerobically incubated for 24 hours at 37°C. To guarantee purity and get single colonies, all isolates were cultivated on nutrient agar and incubated for 24 hours at 37°C. Following the isolation of bacterial colonies on culture media, isolates were identified by morphological characteristics, biochemical identification and Vitek 2 bacterial identification system (bioMerieux). The initial phenotypic examination for the isolates was first determined by analyzing the growth characteristics of colonies on differential medium; these consist of pigmentation, consistency, elevation, edge, and size.18 As well as using Gram stain for bacteria. The biochemical examinations are carried out to verify colony identification at the generic level. One of these is the production of catalase, oxidase, and deoxyribonuclease (Dnase). Other abilities include the ability to perform the mixed acids pathway (Methyl red test), use citrate as a carbon source, use Triple Sugar Iron (TSI, HIMEDIA®) agar with the production (or not) of hydrogen sulfide, and the production of coagulase enzyme.19 In accordance with the manufacturer’s instructions, identification of the isolated bacteria was carried out using the Vitek 2 system using identification cards for gram-negative bacilli (ID-GNB) and gram-positive cocci (ID-GPC) (bioMerieux) to determine the genus and species. With software update 2.01, the VITEK 2 system reported the results automatically.20
Variables of the study
Patients who did not get antibiotics within the preceding 15 days and who visited the ISH Microbiology Laboratory from January 2020 -December 2022 were all eligible for culture. Antimicrobial susceptibility tests were performed for every bacterial isolate. The primary variable was a culture-confirmed bacterial illness; the independent variables were age, antibiotic usage, sex, and clinical sample type.
Antimicrobial susceptibility testing
The sensitivity of the isolated bacteria toward several antibiotics was determined using Muller Hinton Agar (Oxoid, UK) and Kirby-Bauer disk diffusion susceptibility tests.21 Bacterial isolates were tested for susceptibility to Ampicillin 10 µg, Penicillin 10 µg, Amoxicillin and Clavulanic acid (AMC) 30 µg, Meropenem 10 µg, Imipenem 10 µg, Ceftazidime 30 µg, Ceftriaxone 30 µg, Gentamicin 20 µg, Chloramphenicol 30 µg, Gentamicin 10 µg, Ciprofloxacin 5 µg, Amikacin 30 µg, Cefepime 30 µg, Colistin 10 µg, Trimethoprim/sulfamethoxazole 25 µg, and clindamycin 2 µg. The antibiotics selection was based on readily accessible medications and antibiotics routinely recommended by physicians, in line with Magiorakos et al., resistance data were analyzed using zone sizes from the Clinical and Laboratory Standards Institute (CLSI) suggestion.22-26
Quality control
The American Type Culture Collection (ATCC) standard reference strains, including E. coli ATCC-25922 and S. aureus ATCC-25923, were used to confirm the effectiveness of the culture medium. Data was reviewed for accuracy, consistency, clarity, and completeness before data entry.
Data analysis
IBM SPSS Statistics for Windows, version 23 (IBM Corp, Armonk, NY, USA), was used to analyze the data. The frequency, percentage, mean, and standard deviation were all used in the descriptive statistical analysis. P-values less than 0.05 were considered statistically significant.
Patient demographic characteristics
Over three years (2020-2022), 9369 bacterial cultures from nine different body locations were evaluated. Urine samples numbered 4966 (53%), vaginal and cervical discharge 937 (10%), pus discharge 750 (8%), blood 750 (7.9%), cerebral fluids 562 (6%), urethral discharge 375 (4%), stool 282 (3%), eye discharge 281 (3%), ear discharge 187 (2%), other body fluids 187 (2%) and semen 93 (0.9%). Further, a total of 5341 (57%) samples were obtained from female patients, whereas 4028 (43%) samples were related to male patients. The mean ± SD age of the patients was 32.5 ± 8.6 years, and 3279 (35%) patients were in the age group of 15-29 years (Table 1).
Table (1):
Correlation between Socio-demographic details and type of isolated bacteria
| Parameter | Total N (%) | Isolates Status | P-value | ||
|---|---|---|---|---|---|
| Positive for bacterial infections N (%) | Gram-Positive N (%) | Gram-Negative N (%) | |||
| Sex | 0.0001* | ||||
| Female | 5341 (57%) | 1955 (68.8%) | 782 (40%) | 1173 (60%) | |
| Male | 4028 (43%) | 886 (31.2%) | 257 (29%) | 629 (71%) | |
| Age (years) | 0.04*
|
||||
| ≤14 | 1405 (15%) | 301 (21.4%) | 54 (18%) | 247 (82%) | |
| 15–29 | 3279 (35%) | 1294 (39.5%) | 292 (22.5%) | 1002 (77%) | |
| 30–44 | 2998 (32%) | 666 (22.2%) | 93 (13.9%) | 573 (86%) | |
| 45–59 | 1124 (12%) | 433 (38.5%) | 52 (12%) | 381 (88%) | |
| ≥60 | 563 (6%) | 147 (26.2%) | 49 (33.3%) | 98 (67%) | |
The chi-squared test (χ2) has been used with a significance level of p-value ≤0.05; Bold values indicated the statistically significant values p-values
The proportion of isolated pathogens
A total of 9369 specimens were tested during a study period; the number of samples cultivated annually is shown in Figure 1. A total of 2841 (30.3%) of tested specimens were positive for bacteria in culture, and a total of 3123 pure isolates of different types of bacteria were obtained. Among the 3123 bacteria isolated, 2841 (91%) were single isolates, while 282 (9.9%) were mixed isolates. Table 1 shows that among the 2841 positive samples, the percentage of Gram-negative bacterial isolates was substantially more significant at 1802 (63.4%) compared to the Gram-positive group at 1039 (36.6%)
(P = 0.04). Out of 2841 positive cultures, there was a significantly higher proportion of bacterial isolates in females 1955 (68.8%) compared to males 886 (31.1%) (P = 0.0001). The most frequently isolated microorganisms from clinical specimens were E. coli (39%), followed by S. aureus (13%) and K. pneumoniae (12%) (Figure 1).
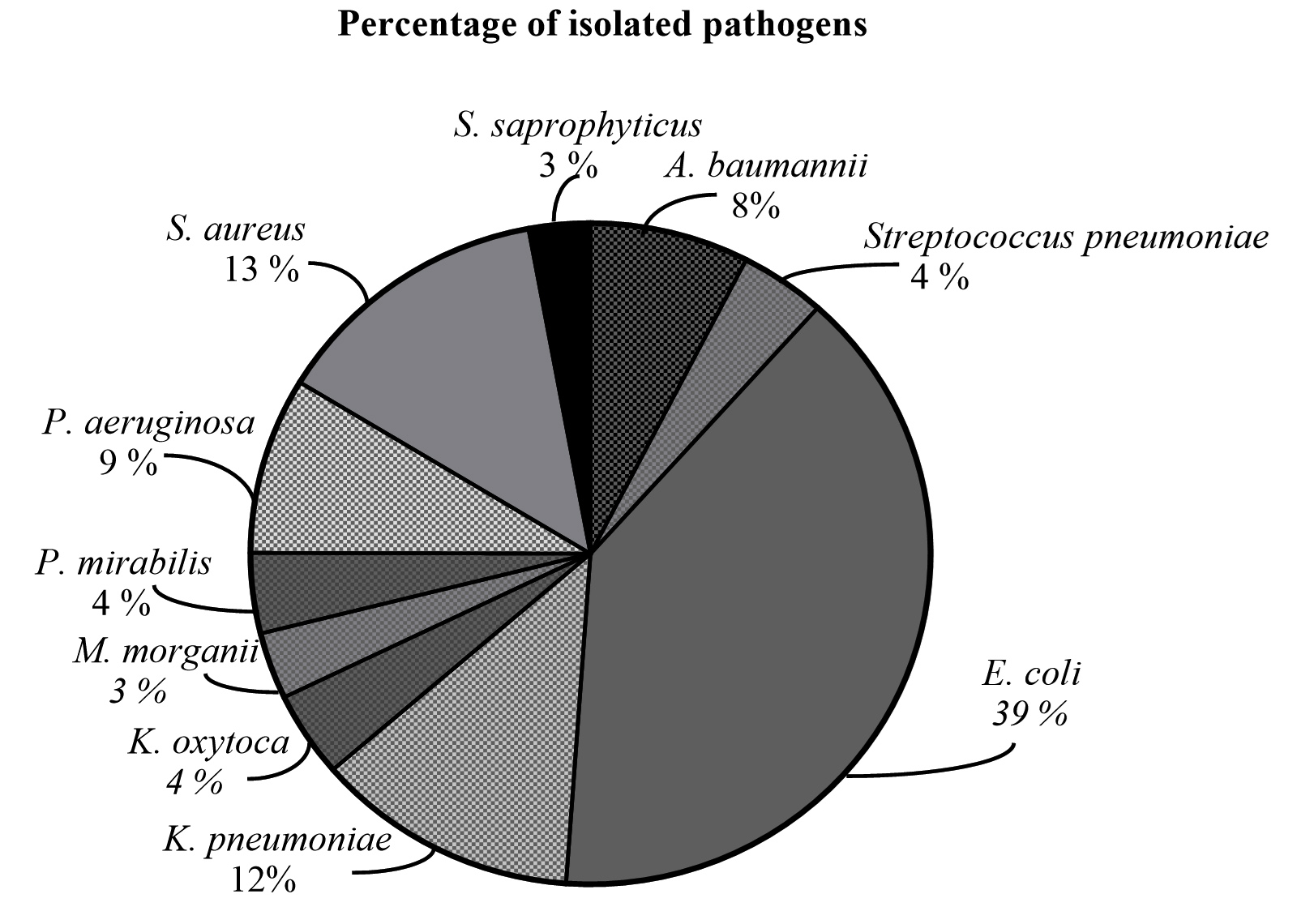
Figure 1. Bacteria profile for Islamic Specialized Hospital (ISH) specimens, Amman, Jordan
This study showed that there was greatest resistance to Ampicillin, Ciprofloxacin, and Clindamycin in 2020, as well as Ceftazidime, SXT, and Gentamicin in 2021, compared to 2022, which had the highest resistance to Imipenem and Penicillin of all year (Table 2). A calculation of the mean percentage resistance revealed that the three drugs with the highest mean percentage resistance were Ampicillin (70%), Ciprofloxacin (52%), and Clindamycin (52%). In contrast, Penicillin (14%), Amikacin (16%), and Imipenem (17%) had the lowest mean per cent resistance across three years (Table 2).
Table (2):
Resistance Percentage of antimicrobial agents in the Islamic Specialized Hospital (ISH)
| Antimicrobial | 2020 | 2021 | 2022 | Mean % resistance | |||
|---|---|---|---|---|---|---|---|
| N | R% | N | R% | N | R% | ||
| Ampicillin | 375 | 82 | 517 | 72 | 490 | 55 | 70 |
| AMC | 543 | 33 | 687 | 44 | 685 | 46 | 41 |
| Cefepime | 678 | 37 | 918 | 44 | 939 | 37 | 39 |
| Colistin | 241 | 0 | 241 | 0 | 241 | 0 | 0 |
| Ceftazidime | 678 | 43 | 918 | 44 | 939 | 43 | 43 |
| Ceftriaxone | 673 | 40 | 877 | 41 | 810 | 40 | 40 |
| Ciprofloxacin | 678 | 52 | 939 | 52 | 52 | 52 | 52 |
| SXT | 673 | 60 | 68 | 810 | 52 | 52 | 60 |
| Clindamycin | 242 | 59 | 47 | 262 | 50 | 50 | 52 |
| Gentamicin | 678 | 28 | 30 | 939 | 26 | 26 | 28 |
| Imipenem | 678 | 17 | 16 | 939 | 18 | 18 | 17 |
| Meropenem | 678 | 17 | 17 | 939 | 16 | 16 | 16 |
| Amikacin | 678 | 15 | 17 | 939 | 16 | 16 | 16 |
| Penicillin | 62 | 9 | 11 | 156 | 22 | 22 | 14 |
N: Number of isolates tested; R%: percentage of isolates that tested resistant to the antibiotic
Further, all identified bacteria showed various degrees of resistance to the tested drugs (Table 3). More than 50% of resistance rates were seen against Ampicillin, Amoxicillin and Clavulanic acid (AMC), Ciprofloxacin, Ceftazidime, Trimethoprim/Sulfamethoxazole, and Ceftriaxone. Only Acinetobacter baumannii showed resistance to Meropenem and Imipenem at levels over 90%. The total resistance percentage of the E. coli isolates was 36%. The isolates showed resistance to Ampicillin (89%), Amoxicillin and Clavulanic acid (47%), Trimethoprim/Sulfamethoxazole (51%), and Ciprofloxacin (50%) except Amikacin, Imipenem, Gentamicin, and Meropenem. The total resistance of Klebsiella spp. was 31%, whereas the percentage of overall resistance for Staphylococcus and Streptococcus isolates was 25% and 20%, respectively (Table 3). All medications except meropenem, Amikacin, and Imipenem were resistant to Klebsiella pneumoniae. Similarly, only Ceftazidime, Imipenem, Colistin, Meropenem, and Amikacin were effective against Pseudomonas aeruginosa. 39% of bacterial isolates were resistant overall (Table 3).
Table (3):
Antimicrobial resistance profiles of isolated bacteria from ISH Patients
| Antibiotic type | Acinetobacter baumannii R (%) | Streptococcus pneumoniae R (%) | Escherichia coli R (%) | Klebsiella pneumoniae R (%) | Klebsiella oxytoca R (%) | Morganella morganii R (%) | Proteus mirabilis R (%) | Pseudomonas aeruginosa R (%) | Staphylococcus aureus R (%) |
|---|---|---|---|---|---|---|---|---|---|
| AMC | 99.2 | ND | 47 | 41 | 53 | ND | 23.6 | 96 | ND |
| Ampicillin | 99.6 | 8 | 89 | ND | ND | ND | 65.3 | 97 | ND |
| Cefepime | 93 | ND | 43 | 43 | 46 | 7.6 | 12.6 | ND | 70 |
| Ceftazidime | 99 | ND | 49 | 47 | 50.6 | 11.3 | 20.6 | 23.6 | ND |
| Ceftriaxone | 98 | 2 | 48 | 47 | 51 | 11 | 22.0 | ND | 56 |
| Ciprofloxacin | 95 | 42 | 50 | 42 | 65.5 | 39.6 | 29.1 | 31.3 | 78 |
| SXT | 92 | 36 | 51 | 44 | 57.3 | 52.1 | 59.2 | 58 | 14.6 |
| Clindamycin | ND | ND | ND | ND | ND | ND | ND | ND | 35.6 |
| Gentamicin | 89 | ND | 17 | 13 | 17 | 17.3 | 20.6 | 23.3 | 85 |
| Imipenem | 95 | ND | 0.3 | 0 | 0 | 0 | 0 | 25.0 | 68 |
| Meropenem | 94 | ND | 0 | 0 | 0 | 0 | 0 | 21.3 | 63 |
| Amikacin | 90 | ND | 1 | 1.6 | 4.3 | 0 | 0 | 16.0 | 81 |
| Penicillin | ND | 7 | ND | ND | ND | ND | ND | ND | ND |
| Colistin | 0 | ND | ND | ND | ND | ND | ND | 0.3 | ND |
| Overall antimicrobial resistance | 95 | 20 | 36 | 28 | 34 | 15 | 23 | 39 | 61 |
| Over all (%) resistant = 39 | |||||||||
R (%), Resistance percentage toward each tested antibiotic
The three highly abundant bacteria that were most often isolated were Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa, which were shown with various MRD (Figure 2). Escherichia coli was observed to be resistant to Ampicillin (89%) and extremely susceptible to Imipenem (100%). K. pneumoniae exhibited a 100% susceptibility to Meropenem but a 49% resistance to Ceftriaxone. S. aureus isolates have resistance rates of 78% for ciprofloxacin, 35.6% for clindamycin and an overall resistance rate of 68.7%, as shown in Figure 2.
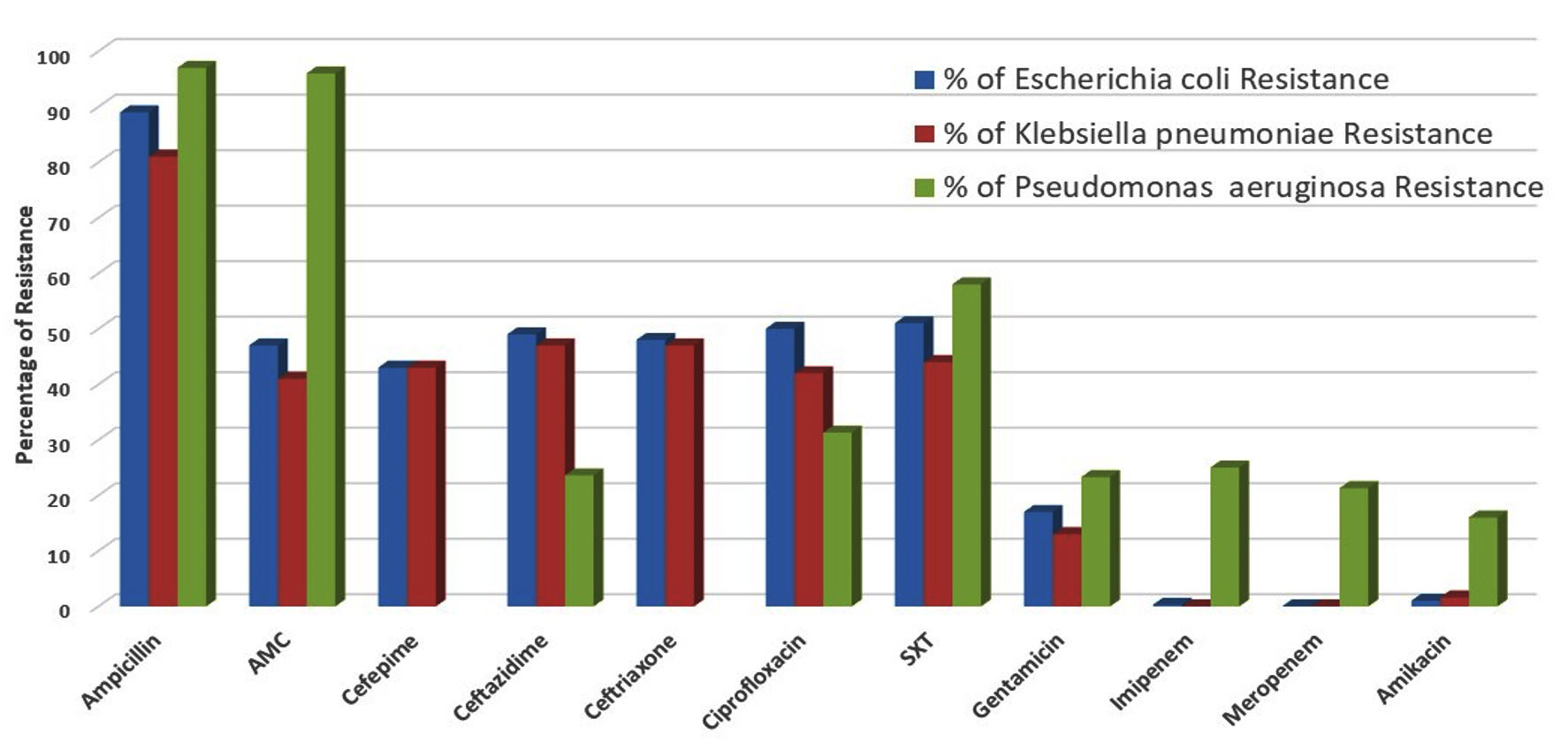
Figure 2. The percentage resistance patterns for the three most prevalent bacterial isolates from ISH patients
Among 3123 isolates, 120 (3.8%) were sensitive to all antibiotics tested. Most isolates (96.2%) resisted at least one antibiotic tested. MDR status was assigned to 61.7% of the isolates overall. Table 4 shows that the MDR rates of isolates of S. aureus, E. coli, and Klebsiella pneumoniae were 68.7%, 73.1%, and 72%, respectively.
Table (4):
Antibiotic Resistance Patterns of Bacterial Isolates from the ISH in Amman, Jordan
| Bacterial Isolate | Antibiogram (N % resistance)a | Overall MDR | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Name of bacteria | N | R0 | R1 | R2 | R3 | R4 | R5 | R6 | R7 | R8 | |
| Acinetobacter baumannii | 241 | 0 | 0 | 40 (16.6) | 97 (40.2) | 104 (43) | 0 | 0 | 0 | 0 | 201 (83.4) |
| Streptococcus pneumoniae | 130 | 11 (8.4) | 13 (10) | 30 (23.1) | 31 (23.8) | 19 (14.6) | 17 (13) | 9 (6.9) | 0 | 0 | 76 (58.5) |
| Escherichia coli | 1258 | 23 (2) | 105 (10) | 211 (19) | 302 (26) | 314 (30) | 167 (14) | 103 (7) | 33 (5) | 0 | 919 (73.1) |
| Klebsiella pneumoniae | 399 | 8 (2) | 24 (6) | 80 (20) | 55 (14) | 88 (22) | 80 (20) | 40 (10) | 24 (6) | 0 | 287 (72) |
| Klebsiella oxytoca | 133 | 9 (7) | 32 (27) | 11 (8) | 0 | 21 (19) | 44 (35) | 16 (14) | 0 | 0 | 81 (61) |
| Morganella morganii | 104 | 21 (20) | 31 (30) | 29 (28) | 16 (15) | 4 (4) | 2 (2) | 1 (1) | 0 | 0 | 23 (22.1) |
| Proteus mirabilis | 125 | 14 (11) | 28 (23) | 26 (21) | 33 (26) | 20 (16) | 3 (2) | 1 (1) | 0 | 0 | 57 (45.6) |
| Pseudomonas aeruginosa | 275 | 31 (11) | 45 (17) | 114 (41) | 39 (14) | 18 (6) | 15(6) | 13 (5) | 0 | 0 | 85 (30.9) |
| Staphylococcus aureus | 427 | 0 | 69 (16) | 107 (25) | 120 (28) | 60 (14) | 0 | 9 (2) | 0 | 0 | 189 (68.7) |
| Staphylococcus saprophyticus | 31 | 3 (10) | 12 (38) | 9 (30) | 4 (13) | 2 (6) | 1 (2) | 1 (1) | 0 | 0 | 8 (25.8) |
| Total | 3123 | 120 (3.8) | 357 (11.4) | 666 (21.3) | 722 (23.1) | 662 (21.2) | 329 (10.5) | 210 (6.7) | 57 (1.8) | 0 | 1926 (61.7) |
aThe resistance range for RI – R8 was one to eight antibiotics, R0 sensitive to all tested antibiotics
As the world continues dealing with the COVID-19 pandemic side effects,27 an important threat emerged: the Multi-Drug Resistance (MDR) of bacteria. COVID-19 fears changed how people get healthcare and how doctors prescribe medicines, including antibiotics. The misuse of antibiotics as prophylactic drugs might have increased the COVID-19 pandemic; thus, more people get to use the antibiotics randomly, which accelerated the emergence of MDR, especially during the COVID-19 pandemic; other factors, agricultural and industrial practices might also have contributed to an increase in MDR bacteria in Jordan. Therefore, this study aimed to provide information on microbial profiles and antibiotic resistance patterns during and post-COVID-19.
Overuse and Misuse of antibiotics might be the main cause of developing MDR bacteria through the prescribing of unnecessary antibiotics for conditions like viral infections. For example, the COVID-19 pandemic has increased the rate of MDR through the unnecessary use of antibiotics as prophylactics.28 Furthermore, the antibiotics are available over the counter in Jordan, allowing patients to use them without a reference to medical protocols. This leads to improper use and development of MDR strains of bacteria. Also, another factor that might contributed to MDR is the improper diagnosis of disease and administration of an excessive dose of antibiotics without bacterial cultivation in hospitals.29 Furthermore, antimicrobial resistance and antibiotic-resistant bacteria can be transmitted directly during harvesting operations from food-producing animals to people by either direct contact with animals or ingestion of animal products, especially when cooked in an improper manner.30,31
This study aimed to explain bacterial profiles over 2020-2023; around 33% of cultures (3123 out of 9369) were examined and tested positive for microbial growth. Also, the some-demographic data indicates that among 2841 tested positive patients, 1955 (68.8%) of the patients were females, and 886 (31.1%) were males (P < 0.05). It seems that women experience these infections at a younger age than men, possibly due to the frequent association between E. coli and K. pneumoniae and female genital infections. The risk of urinary tract infections (UTIs) significantly increases with age. This may explain why our analysis revealed age as a predictor of antibiotic resistance development, particularly for antibiotics used to treat UTIs.32
Microbial profiles indicated that Gram-negative bacteria were the most frequently isolated bacteria. The widespread isolation of Gram-negative bacteria can be attributed to their minimal nutritional needs, frequent presence in clinical settings, and resistance to a wide variety of medications found in hospital environments.33 Around 39% of isolated bacteria was E. coli, which is the most common isolate of gram-negative bacteria in the current study. This was analogous to research and studies from other parts of Jordan.34 The frequency of E. coli infections may be explained by the pathogen’s virulence factors and interactions with the host.35 Additionally, Staphylococcus aureus emerged as the second-most isolated gram-positive pathogen, which was in agreement with a previous investigation done by Al-Tamimi et al and Ennab et al.36,37 Moreover, E. coli, Pseudomonas aeruginosa, and K. pneumoniae were the species that were isolated the most frequently gram-negative in the current study. The findings were comparable to similar research.38-40 The isolates’ prevalence might be attributed to their frequent presence in hospital settings. Additionally, common skin and gut flora such as S. aureus, S. saprophyticus, E. coli, and Klebsiella spp. can be transferred from their native environment to other sterile areas via skin and soft tissue holes, leading to the spread of infection and serious health problems. The current research findings offer valuable insights into microbial profiles in hospitals in Jordan.
The use of antibiotics is important in treating bacterial infections. However, many antibiotics are facing resistance from bacteria. Antibiotic resistance levels varied across the bacteria tested. Ampicillin, Amoxicillin-Clavulanic acid, Ciprofloxacin, Ceftazidime, Trimethoprim/ Sulfamethoxazole, and Ceftriaxone showed more than 50% resistance rates. Acinetobacter baumannii is an emerging and significant multidrug-resistant (MDR) pathogen in hospitals, particularly in intensive care units (ICUs). It is considered a major nosocomial pathogen causing a high mortality rate.41 Further, this study also revealed a high resistance rate for Acinetobacter baumannii to most antibiotic agents; it showed resistance to Imipenem and Meropenem at levels exceeding 90%, which is extremely concerning. This is a compelling reason for the World Health Organization (WHO) to include Carbapenem-resistant Acinetobacter baumannii (CRAB) in its global priority list.
E. coli isolates had a total resistance rate of 36%, with Ampicillin (89%), Amoxicillin – Clavulanic acid (47%), Trimethoprim/Sulfamethoxazole (51%), and Ciprofloxacin (50%). E. coli is considered one of the groups of eight bacterial species highlighted by the WHO as a key MDR concern and serves as a sentinel organism for antimicrobial resistance development in blood and urine.42 Resistance against b-lactam, Cephalosporin and Carbapenem antibiotics is increasingly documented, and many studies have reported increases in E. coli resistance to more than one class of antibiotics.43
In overall resistance, 31% of Klebsiella species showed resistance. Streptococcus pneumoniae and Staphylococcus aureus showed 20% and 61%, respectively. This could be due to the substantial usage of the mentioned antibiotics. Since they are the most readily available and reasonably priced, they are also the most utilized in the community.44 Similarly, isolates that were resistant to the same microbial agent at a 70% rate were identified in Jordan.45 Variations in sample size, research environment, prescription pattern, antibiotic treatment, and causative organism epidemiology between sites may all be reflected in the differences in resistance percentages.
The present investigation revealed that E. coli and Klebsiella spp. were resistant to Ampicillin, Amoxicillin-Clavulanic acid, Ceftriaxone, and Ceftazidime. This proved that infections resulting from bacteria resistant to another commonly used group of antibiotics, including third-generation Cephalosporins, constitute a significant problem in the study area. Of the isolates, 120 (3.8%) were sensitive to all antibiotics tested, while most isolates (96.2%) resisted at least one antibiotic tested. These results were similar to findings from other regions of Jordan.36 As a whole, MDR was found in 61.7% of the isolates. 69% and 73% of S. aureus and E. coli isolates were MDR. Klebsiella pneumoniae demonstrated a 72% MDR in this investigation. This suggested the presence of a high proportion of MDR in Jordan, which required frequent assessment to help the decision-makers in the medical sector establish a protocol for the proper use of antibiotics to reduce MRD at the local level. Furthermore, these findings might consider a call for establishing a statewide antimicrobial monitoring program at global levels and strict compliance with the antibiotic strategy to stop the spread of bacteria resistant to drugs.
The common isolates were E. coli, Streptococcus pneumoniae, S. aureus, Pseudomonas aeruginosa, and K. pneumoniae. Most isolates resisted Ciprofloxacin, Ampicillin, Trimethoprim/Sulfamethoxazole, and Cephalosporin Antimicrobials. The frequency of isolates resistant to multiple drugs is also concerning. As a result, it is advised that hospitals have stringent antibiotic use rules in place, that physicians be supported in making reasonable antibiotic therapy decisions, and that the list of dependable medication sources is updated regularly. As a result, other antibiotics should be utilized for therapy rather than the medications discovered to be the most resistant. In the case of switching medicines, there are a few things to consider, including the cost and safety of the antibiotic in the target group. There is no assurance, however, that the new standard of treatment will not contribute to the establishment of new resistant strains unless all levels of the health system follow stringent standards for the judicious use of these “valuable” antibiotics.
ACKNOWLEDGMENTS
The authors express their gratitude to Mr. Hassan Battah (Microbiology Section, Department of Laboratory, Islamic Specialized Hospital ISH, Amman, Jordan) and Mr. Yasser Fodeh (Head, Department of Laboratory, ISH) for their assistance in gaining access to patient data.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
GHM conceptualized the study. NMFAL supervised the study. MTS performed the experiments. ASF performed the statistical analysis and validated the data. NMFAL visualized the study. AAA interpreted the data. JDA prepared original draft. MEAW wrote and reviewed the manuscript. NMFAL and MEAW edited the manuscript. All authors read and approved the final manuscript for publication.
FUNDING
None.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Balqa Applied University, with approval ref. No. ERC 18/2/3/18/2620.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Pulingam T, Parumasivam T, Gazzali AM, et al. Antimicrobial resistance: Prevalence, economic burden, mechanisms of resistance and strategies to overcome. Eur J Pharm Sci. 2022;170:106103.
Crossref - Mirzayev F, Viney K, Linh NN, et al. World Health Organization recommendations on the treatment of drug-resistant tuberculosis, 2020 update. Eur Respir J2021;57(6):20003300.
Crossref - Muteeb G, Rehman MT, Shahwan M, Aatif M. Origin of antibiotics and antibiotic resistance, and their impacts on drug development: A narrative review. Pharmaceuticals 2023;16:(11)1615.
Crossref - Leistner R, Kohlmorgen B, Brodzinski A, et al. Environmental cleaning to prevent hospital-acquired infections on non-intensive care units: a pragmatic, single-centre, cluster randomized controlled, crossover trial comparing soap-based, disinfection and probiotic cleaning. EClinicalMedicine. 2023;59:101958.
Crossref - Kanan M, Ramadan M, Haif H, et al. Empowering low-and middle-income countries to combat AMR by minimal use of antibiotics: A way forward. Antibiotics. 2023;12(10):1504.
Crossref - Alividza V, Mariano V, Ahmad R, et al. Investigating the impact of poverty on colonization and infection with drug-resistant organisms in humans: a systematic review. Infect Dis Poverty. 2018;7(1):1-11.
Crossref - Al Dabbagh M, Alghounaim M, Almaghrabi RH, et al. A narrative review of healthcare-associated Gram-negative infections among pediatric patients in middle eastern countries. Infect Dis Ther. 2023;12(5):1217-1235.
Crossref - Cerceo E, Deitelzweig SB, Sherman BM, Amin AN. Multidrug-resistant gram-negative bacterial infections in the hospital setting: overview, implications for clinical practice, and emerging treatment options. Microb Drug Resist. 2016;22(5):412-431.
Crossref - Furuya EY, Lowy FD. Antimicrobial-resistant bacteria in the community setting. Nat Rev Microbiol. 2006;4(1):36-45.
Crossref - Tarin-Pello A, Suay-Garcia B, Perez-Gracia M-T. Antibiotic resistant bacteria: current situation and treatment options to accelerate the development of a new antimicrobial arsenal. Expert Rev Anti Infect Ther. 2022;20(8):1095-1108.
Crossref - Godman B, Egwuenu A, Haque M, et al. Strategies to improve antimicrobial utilization with a special focus on developing countries. Life. 2021;11(6):528.
Crossref - Haque M. Antimicrobial use, prescribing, and resistance in selected ten selected developing countries: A brief overview. Asian J Pharm Clin Res. 2017;10(8):37-45.
Crossref - Sulis G, Sayood S, Gandra S. Antimicrobial resistance in low-and middle-income countries: current status and future directions. Expert Rev Anti Infect Ther. 2022;20(2):147-160.
Crossref - Friedrich AW. Control of hospital acquired infections and antimicrobial resistance in Europe: the way to go. Wiener Medizinische Wochenschrift. 2019;169:25-30.
Crossref - Zheng Y, Liu J, Tang PK, Hu H, Ung COL. A systematic review of self-medication practice during the COVID-19 pandemic: implications for pharmacy practice in supporting public health measures. Frontiers in Public Health. 2023;11:1184882.
Crossref - Al-Dhabaan FA. Morphological, biochemical and molecular identification of petroleum hydrocarbons biodegradation bacteria isolated from oil polluted soil in Dhahran, Saud Arabia. Saudi J Biol Sci. 2019;26(6):1247-1252.
Crossref - Freeman KP, Cook JR, Hooijberg EH. Standard operating procedures. J Am Vet Med Assoc. 2021;258(5):477-481.
Crossref - Ogodo AC, Agwaranze DI, Daji M, Aso RE. Microbial techniques and methods: basic techniques and microscopy. Analytical Techniques in Biosciences. 2022:201-220.
Crossref - Hasan RS, Alomari SM, Thamer RA, Haddad MF. Risks, Identification, and Antibiotic Susceptibility Against High Prevalence of Bacterial Infection in Contact Lens Solutions. J Angiother. 2024;8(3):1-10.
Crossref - Wallet F, Loiez C, Renaux E, Lemaitre N, Courcol RJ. Performances of VITEK 2 colorimetric cards for identification of gram-positive and gram-negative bacteria. J Clin Microbiol. 2005;43(9):4402-4406.
Crossref - Yin D, Guo Y, Li M, et al. Performance of VITEK 2, E-test, Kirby-Bauer disk diffusion, and modified Kirby-Bauer disk diffusion compared to reference broth microdilution for testing tigecycline susceptibility of carbapenem-resistant K. pneumoniae and A. baumannii in a multicenter study in China. Eur J Clin Microbiol Infect Dis. 2021;40(6):1149-1154.
Crossref - Reller LB, Weinstein M, Jorgensen JH, Ferraro MJ. Antimicrobial susceptibility testing: a review of general principles and contemporary practices. Clin Infect Dis. 2009;49(11):1749-55.
Crossref - Cherkaoui A, Schrenzel J. Total laboratory automation for rapid detection and identification of microorganisms and their antimicrobial resistance profiles. Front Cell Infect Microbiol. 2022;12:807668.
Crossref - Cusack TP, Ashley EA, Ling CL, et al. Impact of CLSI and EUCAST breakpoint discrepancies on reporting of antimicrobial susceptibility and AMR surveillance. Clin Microbiol Infect. 2019;25(7):910-911.
Crossref - Hombach M, Bottger EC, Roos M. The critical influence of the intermediate category on interpretation errors in revised EUCAST and CLSI antimicrobial susceptibility testing guidelines. Clin Microbiol Infect. 2013;19(2):E59-E71.
Crossref - Sader HS, Ferraro MJ, Reller LB, Schreckenberger PC, Swenson JM, Jones RN. Reevaluation of Clinical and Laboratory Standards Institute disk diffusion breakpoints for tetracyclines for testing Enterobacteriaceae. J Clin Microbiol. 2007;45(5):1640-1643.
Crossref - Dmour I, Al-Hamaideh KD, Al-Qudeh SA, Al-Shawabkeh JD. Self-care interventions among the Jordanians during the COVID-19 lockdown: A cross-sectional study of community pharmacists’ observations. J Appl Pharm Sci. 2023;13(8):212-222.
Crossref - Strathdee SA, Davies SC, Marcelin JR. Confronting antimicrobial resistance beyond the COVID-19 pandemic and the 2020 US election. Lancet. 2020;396(10257):1050-1053.
Crossref - Xu C, Kong L, Gao H, Cheng X, Wang X. A Review of Current Bacterial Resistance to Antibiotics in Food Animals. Front Microbiol. 2022;13:822689.
Crossref - Ahmed SK, Hussein S, Qurbani K, et al. Antimicrobial resistance: Impacts, challenges, and future prospects. J Med Surg Public Health. 2024;2:100081.
Crossref - Woolhouse M, Ward M, Van Bunnik B, Farrar J. Antimicrobial resistance in humans, livestock and the wider environment. Philos Trans R Soc B Biol Sci. 2015;370(1670):20140083.
Crossref - Fagan M, Lindbæk M, Grude N, et al. Antibiotic resistance patterns of bacteria causing urinary tract infections in the elderly living in nursing homes versus the elderly living at home: An observational study. BMC Geriatr. 2015;15:98.
Crossref - Cerceo E, Deitelzweig SB, Sherman BM, Amin AN. Multidrug-resistant gram-negative bacterial infections in the hospital setting: overview, implications for clinical practice, and emerging treatment options. Microb Drug Resist. 2016;22(5):412-431.
Crossref - Abu-Sini MK, Maharmah RA, Abulebdah DH, Al-Sabi MNS. Isolation and identification of coliform bacteria and multidrug-resistant Escherichia coli from water intended for drug compounding in community pharmacies in Jordan. Healthcare. 2023;11(3):299.
Crossref - Sarowska J, Futoma-Koloch B, Jama-Kmiecik A, et al. Virulence factors, prevalence and potential transmission of extraintestinal pathogenic Escherichia coli isolated from different sources: recent reports. Gut Pathog. 2019;11:1-16.
Crossref - Al-Tamimi M, Albalawi H, Isied W, et al. Gram-positive bacterial infections and antibiotics resistance in Jordan: current status and future perspective. Jordan Med J. 2022;56(1).
Crossref - Gharaibeh MH, Alyafawi DA, Elnasser ZA, Lafi SQ, Obeidat HM. Emergence of mcr-1 gene and carbapenemase-encoding genes among colistin-resistant Klebsiella pneumoniae clinical isolates in Jordan. J Infect Public Health. 2022;15(8):922-929.
Crossref - Karlowsky JA, Bouchillon SK, El Mahdy Kotb R, Mohamed N, Stone GG, Sahm DF. Carbapenem-resistant Enterobacterales and Pseudomonas aeruginosa causing infection in Africa and the Middle East: A surveillance study from the ATLAS programme (2018-20). JAC Antimicrob Resist. 2022;4(3):dlac060.
Crossref - Nasser M, Gayen S, Kharat AS. Prevalence of b-lactamase and antibiotic-resistant Pseudomonas aeruginosa in the Arab region. J Glob Antimicrob Resist. 2020;22:152-160.
Crossref - Barakat H, Alkabeer IA, Aljutaily T, et al. Phenolics and Volatile Compounds of Fennel (Foeniculum vulgare) Seeds and Their Sprouts Prevent Oxidative DNA Damage and Ameliorates CCl4-Induced Hepatotoxicity and Oxidative Stress in Rats. Antioxidants. 2022;11(12):2318.
Crossref - Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629-655.
Crossref - Ibrahim DR, Dodd CER, Stekel DJ, t al. Multidrug-Resistant ESBL-Producing E. coli in Clinical Samples from the UK. Antibiotics. 2023;12(1):169.
Crossref - Abdel-Qader DH, Albassam A, Ismael NS, et al. Awareness of antibiotic use and resistance in Jordanian Community. J Prim Care Community Health. 2020;11:2150132720961255.
Crossref - Hamza OA, Omran R. Multidrug Drug Resistance of Escherichia coli and Klebsiella Isolated from Iraqi Patients and Microbiota. J Biosci Med. (Irvine) 2022;10(11):240-252.
Crossref - Al-Baz AA, Maarouf A, Marei A, Abdallah AL. Prevalence and antibiotic resistance profiles of carbapenem-resistant Klebsiella pneumoniae isolated from Tertiary Care Hospital, Egypt. Egypt J Hosp Med. 2022;88(1):2883-2890.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.