

ISSN: 0973-7510
E-ISSN: 2581-690X
Both rheumatoid arthritis and periodontitis are complex multifactorial disorders, characterized not only by a dysfunction of basic inflammatory and tissue destructive mechanisms, but also by an altered adaptive and innate immune response in individuals. IL-22 plays an important role in inflammation, including chronic inflammatory diseases and infectious diseases. This study aimed to evaluate the serum levels of IL-22 and ACPA in RA patients. The study included 45 rheumatoid arthritis patients and 35 apparently healthy controls. Enzyme-linked immunosorbent assay (ELISA) has been used for estimation the levels of IL-22 and ACPA in serum of two studied groups. The present results revealed that mean serum levels of IL-22 and ACPA were significantly higher in patients than in healthy controls (p<0.02, p<0.04) respectively. On the other hand, there is no correlation was found between serum level of antibody (IgG-ACPA) and serum level of cytokine (IL-22), (r=0.79; p=0.606). Elevation serum level IL-22 could be involved pathogenesis of RA in association with ACPA level.
Rheumatoid Arthritis, Cytokines, IL-22, ACPA.
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease with articular as well as systemic consequences, is outlined by a dynamic pathobiology with chronic synovitis as the epicenter of immunologic responses, inflammation and tissue destruction, occurring as a response to microbial exposure or a putative antigen in genetically predisposed host. The aetiology of RA remains unknown, although a complex interplay exists between genetic and environmental factors1, 2. Periodontitis (PD), which is the world’s commonest inflammatory disease often resulting in destruction of alveolar bone and tooth loss, has been suggested as an environmental determinant for the occurrence and severity of RA3, 4).
The bidirectional relationship between RA and PD is regulated by genetic and environmental factors and inflammatory events with immunoregulatory imbalance5,6,7. Furthermore, the association among PD and RA has been extensively addressed in recent years, emphasizing the role of gingival microorganisms, particularly P gingivalis, as the underlying link between dental and rheumatic pathology via citrullination8. Citrullination or deamination is the term used for a genetic modification of the amino acid arginine in a protein into the amino acid citrulline and caused by enzymatic activity through peptidyl-arginine deaminases (PAD) enzyme. It has been found that P. gingivalis is currently the only known bacterium with the expression of PAD which is involved in citrullination. Anti-citrullinated protein antibodies (ACPA) are highly specific for RA and have been implicated in disease etiology, it may be detected in roughly 50-60% of patients with early RA9.
Interleukin (IL)-22 is a member of the IL-10 family of cytokines that has been extensively studied since its discovery in 200010. It is primarily produced by CD4 T cells and NK cells, plays an important role in inflammation, including chronic inflammatory diseases and infectious diseases11. In RA IL-22 responses are increased in peripheral blood and joints, IL-22 induces RANKL, and the magnitude of IL-22 response correlates with inflammatory markers, RA disease activity scores and degree of bone damage12. Díaz-Zúñiga et al13 showed that increased levels of IL 22 produced by Th22 lymphocytes are associated with the pathogenesis of periodontitis, in particular, with osteoclast resorptive activity and severity of disease. This study aimed to evaluate the serum levels of ACPA and IL-22 RA patients.
Forty five patients with RA their age range (25– 68) years and 35 apparently healthy individuals as control their ages were matched with the patients were enrolled in this study. The patients were from attendants seeking treatment in the rheumatology clinic in Baghdad Teaching Hospital, Baghdad. The subjects were without treatment and with no other chronic or systemic diseases.
Serum samples were separated from the whole blood, aliquated and stored at -20ºC until used. The level of ACPA and IL-22 were estimated by using commercially available sandwich enzyme-linked immunosorbent assay (ELISA) kit and performed as recommended in leaflet with kit (MyBiosource; USA). Statistical analyses were done using SPSS v19. The serum ACPA and IL-22 were expressed as mean ± standard error, the significance of differences in mean was assessed using the student’s t-test. Analyses where the P-value was <0.05 were considered to be statistically significant.
The current study was performed on 45 RA patients and 35 healthy individuals without any systemic disease. There were 34 females and 11 males in the patients, and there were 22 females and 13 males in the healthy individuals group. Table (1) and figure (1) showed that the mean age of patients was 43.72±1.61 years, whereas for healthy subjects was 43.34±1.88 years with no significant differences (p>0.05).
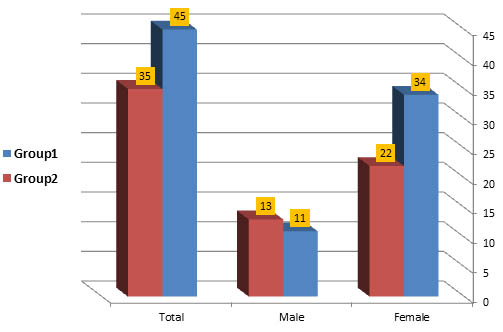
Fig. 1. Age and gender distribution of two studied groups
Table (1):
Age and gender distribution of two studied groups
| Patients Group 1 | Control Group 2 | P-Value | |
|---|---|---|---|
| Age | 0.99NS | ||
| Age range | (25-68) | (26-68) | |
| Mean ± SE | 43.72±1.61 | 43.34±1.88 | |
| Gender | |||
| Female | 34 (75.56%) | 22 (62.86%) | |
| Male | 11 (24.44%) | 13 (37.14%) |
Table (2):
Differences in mean levels of serum IL-22 and ACPA concentration between the two studied groups
Patients |
Control |
P (T-test) |
|
|---|---|---|---|
Serum IL-22 Pg/ml |
|||
Minimum |
8.10 |
6.70 |
|
Maximum |
500.00 |
125.00 |
|
Mean |
68.03 |
32.10 |
|
SE |
12.78 |
4.57 |
|
NO. |
45 |
35 |
|
ACPA-IgG U/ml |
|||
Minimum |
3.40 |
3.20 |
|
Maximum |
50.00 |
45.10 |
|
Mean |
19.62 |
14.07 |
|
SE |
2.23 |
1.95 |
|
NO. |
45 |
35 |
Table (3):
Correlation between serum levels of IL-22 and ACPA-in patients
| IL-22 | ACPA-IgG | |||
|---|---|---|---|---|
| Spearman’s rho | IL-22 Pg/ml | Correlation Coefficient | 1.000 | 0.79 |
| P-value | – | .606 | ||
| N | 45 | 45 | ||
The study showed statistically significant elevation in mean serum levels of IL-22 and ACPA in RA patients with chronic periodontitis (68.03±12.78 pg\ml; 19.62±2.23 U/ml respectively) compared to healthy control (32.10±4.57 pg\ml; 14.07±1.95 U/ml respectively), (p<0.02; p<0.04), as shown in table and fig. (2). On the other hand, there is no correlation was found between serum level of antibody (IgG-ACPA) and serum level of cytokine (IL-22), (r=-0.79; p=0.606), table (3).
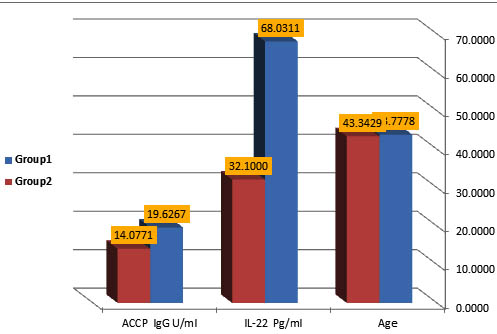
Fig. 2. Difference in mean levels of serum IL-22 Pg/ml and ACPA-IgG (U/ml) concentration between the two studied groups
The vital paths involved in the pathogenesis of RA have confirmed the crucial role of pro-inflammatory cytokines and inflammatory cells. On the other hand, there are significant amounts of data highlighting the potential role of bacteria (P. gingivalis) in promoting different types of arthritis, as well as the influence of periodontitis (as etiological or modulating factor) in different pathologies, including cardiovascular disorders, diabetes, and inflammatory rheumatic diseases as RA and SLE14, 15.
The present work is found increase in serum levels of IL-22 and ACPA in patients with RA when compared to controls, which is in accordance with the observations of the previous researchers16, 17. Zhao and colleagues reported that the serum IL-22 levels and the percentages of circulating Th22, IL-22+Th1, and IL-22+Th17 cells were significantly higher in RA patients than in healthy individuals, suggesting that the major IL-22-producting CD4+Th cells may act through the overproduction of IL-22 to stimulate the pathogenesis of RA16. However, in the animal model mimicking RA in human, IL-22 plays an important role in the productions of inflammatory components, hampering Th1 plasticity and favoring Th17 maintenance and survival, pointing to the potential therapeutic benefits by blocking IL-22 in preventing immune-complex deposition and joint destruction in RA patients18, 19. Other study using an experimental model in which mice are immunized against collagen generating an autoimmune response in the joints, mice deficient in IL-22 had decreased incidence of arthritis and pannus formation20.
Jarallah et al17 showed significant elevation of serum ACPA levels in in sera of RA patients. Other study done Molitor et al. reported that ACPA titters were considerably higher in RA patients with periodontitis than in patients with only RA, they suggested that the P. gingivalis a gram-negative anaerobic bacterium that is recognized to be the only bacteria known to express PAD enzyme which has been identified as a susceptibility factor for RA. P. gingivalis may, therefore, play a role in peptide citrullination and involved in loss of self tolerance and development of RA21.
Another interesting finding in this study the correlation between IL-22 and ACPA levels this was come in line with previous data have shown that complexes of ACPA induce robust cytokine production from human macrophages22. This effect is mediated by the cross-linking of Fc³ receptor IIa on macrophages, representing a strong activation signal for cytokine release23. The leading role of autoantibodies in triggering cytokine release in patients with RA is also reflected by clinical observations which show that patients with RA with autoantibodies exhibit a more severe disease course (24). In conclusion elevation serum level IL-22 could be involved pathogenesis of RA in association with ACPA level.
ACKNOWLEDGMENTS
Thanks to all donors enrolled in the present study.
- Payne JB, Gloub LM and Thiele GM, et al. The link between periodontitis and rheumatoid arthritis: a periodontist‘s persective. Curr Oral Health Rep. 2015; 2: 20-29
- Koziel J, Mydel P and Potempa J. The link between periodontal disease and rheumatoid arthritis: an updated review. Curr Rheumatol Rep. 2014; 16: 408.
- Saini R. Periodontitis and rheumatoid arthritis: Inflammatory relationship. J Pharm Bioallied sci. 2011; 3(3): 464-465.
- DePablo P, Dietrich T and McAlindon TE. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J Rheumatol. 2008; 35: 70–6.
- Joseph R, Jose Raj MG and Sundareswaran S, etal. Does a biological link exist between periodontitis and rheumatoid arthritis. World J. Rheumatology. 2014; 4(3): 80-87.
- Araujo VM, Melo IM and Lima V. Relationship between periodontitis and rheumatoid arthritis: review of the literature. Mediat Inflam. 2015; 259074: 1–15.
- Saini R. Periodontitis and rheumatoid arthritis: inflammatory relationship. J Pharm Bioallied Sci. 2011; 3(3): 464–465.
- Valesini G, Gerardi MC and Iannuccelli C, et al. Citrullination and autoimmunity. Autoimmun Rev. 2015; 14(6): 490–497.
- Wegner N, Lundberg K and Kinloch A, et al. Autoimmunity to specific citrullinated proteins gives the first clues to the etiology of rheumatoid arthritis. Immunol Rev 2010; 233: 34–54.
- Dumoutier, L, Louahed J, and Renauld J. Cloning and characterization of IL-10-related T cell-derived inducible factor (IL-TIF), a novel cytokine structurally related to IL-10 and inducible by IL-9. J. Immunol. 2000; 164: 1814–1819. doi: 10.4049/jimmunol. 164.4.1814.
- Zenewicz LA and Flavell RA. Recent advances in IL-22 biology. Int Immunol. 2011; 23: 159–163.
- DaRocha LF Jr, Duarte AL, Dantas AT, Mariz HA and Pitta Ida R, et al. Increased serum interleukin 22 in patients with rheumatoid arthritis and correlation with disease activity. J Rheumatol. 2012; 39: 1320–1325.
- Díaz-Zúñiga J, Melgar Rodríguez S, Rojas L, Alvarez C, Monasterio G, Carvajal P and Vernal R. Increased levels of the T-helper 22-associated cytokine (interleukin-22) and transcription factor (aryl hydrocarbon receptor) in patients with periodontitis are associated with osteoclast resorptive activity and severity of the disease. Journal of Periodontal Research. 2017; 52(5): 893-902.
- Abdul-hassan Abbas A. Role of Pro- and Anti- Inflammatory Cytokines in Rheumatoid Arthritis: correlation with Disease Severity. Fac. Med. Baghdad. 2010; 52: 284-289.
- Maresz KJ, Helvard A and Sroka A, et al. Porphyromonas gingivalis facilitates the development and progression of destructive arthritis through its unique bacterial peptidylarginine deiminase (PAD). PLoS Pathog. 2013; 9: 81003627.
- Zhao, L. et al. IL-22+CD4+T cells in patients with rheumatoid arthritis. International Journal of rheumatic diseases. 2013; 16: 518–526.
- Jarallah FM, Al-Safi K and Al- Ghurabi BH. Evaluation of serum anti-cyclic citrullinated peptide antibodies level in rheumatoid patients with and without periodontitis. J Bagh College Dentistry. 2015; 24(4): 83-87.
- Justa S, Zhou X and Sarkar S. Endogenous IL-22 plays a dual role in arthritis: regulation of established arthritis via IFN-gamma responses. Journal pone. 2014; e93279-93280.
- Corneth OB et al. Loss of IL-22 inhibits autoantibody formation in collagen-induced arthritis in mice. European journal of immunology. 2016; 46: 1404–1414.
- Geboes L, Dumoutier L and Kelchtermans H, et al. Proinflammatory role of the Th17 cytokine interleukin-22 in collagen-induced arthritis in C57BL/6 mice, Arthritis Rheum. 2009; 60: 390-391.
- Molitor J, Alonso A and Wener M, et al. Moderate to severe adult periodontitis increases risk of rheumatoid arthritis in non-smokers and is associated with elevated ACPA titers: the ARIC study. Arthritis Rheum 2009; 60(10): 433-434.
- Clavel C, Ceccato L, Anquetil F, Serre G and Sebbag M. Among human macrophages polarised to different phenotypes, the M-CSF-oriented cells present the highest pro-inflammatory response to the rheumatoid arthritis-specific immune complexes containing ACPA. Ann Rheum Dis. 2016; 75: 2184–2191.
- Clavel C, Nogueira L, Laurent L, Iobagiu C, Vincent C, Sebbag M and Serre G. Induction of macrophage secretion of tumor necrosis factor alpha through Fc³ receptor IIa engagement by rheumatoid arthritis-specific autoantibodies to citrullinated proteins complexed with fibrinogen. Arthritis Rheum. 2008; 58: 678–688.
- McInnes IB and Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med. 2011; 365: 2205–2219.
© The Author(s) 2018. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.