


ISSN: 0973-7510
E-ISSN: 2581-690X
Helicobacter pylori (H. pylori)-induced inflammation increases the risk of developing various upper gastrointestinal conditions which may progress to gastric cancer (CA). Early prediction and detection of infection are crucial for reducing cancer-induced mortality rates. The present case-control study aimed to investigate the combination of serum and molecular markers and H. pylori-associated gastro-duodenal conditions as risk factors for predicting CA development in dyspeptic patients. Consecutive gastric biopsies and blood samples were collected from 100 adult dyspeptic patients. Serum IgG antibody levels against H. pylori were determined, and receiver operating characteristic (ROC) analysis was performed. The expression of the virulence genes cagA and vacA was evaluated by polymerase chain reaction (PCR). A significant association was reported between the disease condition and the status of several risk factors, such as family history, serum IgG antibody concentration, and the virulence genes cagA and vacA. Among the 71 H. pylori-positive patients, 35.2% (25/71) had CA. Both cagA and vacA genes were found in 46 out of 71 (64.7%) patients, and 92% (23/25) of CA patients carried the cagA+vacA s1 gene. ROC analysis of the serum IgG concentrations revealed AUC values of 0.81 and 0.78 for differentiating patients with non-ulcer dyspepsia from those with ulceration/inflammation and CA, respectively. The concordance between the IgG-positive and PCR-positive patients was 84% (k value=0.41). Patients who had a family history of CA with an increased serum IgG concentration and the presence of H. pylori cagA-vacA s1 genotypes may be considered strong predictors of future development of gastric pathologies, including CA.
Gastric Cancer, Receiver Operating Characteristic Analysis, Serum IgG Antibody, Virulence Genes, Non-ulcer Dyspepsia, Gastric Inflammation, Cancer Biomarkers
Helicobacter pylori (H. pylori)-induced inflammation has been significantly associated with the development of a spectrum of upper gastrointestinal diseases, such as chronic gastritis and peptic ulcer disease, which are precursors to gastric cancer (CA), one of the world’s most common types of cancer among humans. Geographically, CA is a common cancer type with the highest incidence in most parts of Asian countries, like India, China, Japan, Korea and Mongolia.1-3 This high impact of cancer is mainly due to factors such as lack of awareness, socio-economic factors, food/dietary habits and diverse environmental and genetic factors. The mechanism of H. pylori pathogenesis being related to host-bacteria interactions which is initiated by clinically important virulence genes has been documented in various studies.4-7 These include the cytotoxin associated gene A (cagA) and vacuolating cytotoxin gene (vacA) with allelic variants; the signal sequences s1/s2; and the mid region genes m1/m2, which have an association with an increased risk of developing CA.4-7
Diagnosis of CA is often delayed due to a lack of distinguishable clinical symptoms during the early stages of the disease until it advances to its later stages. Early detection and diagnosis are crucial for the prevention of CA. Therefore, to predict and detect this disease at an early stage, there is an urgent need for cancer biomarkers that greatly contribute to its early diagnosis and treatment and thereby decrease CA mortality rates.8,9
Studies have shown that the CA patients have a significantly higher prevalence of H. pylori antibodies than non-cancer controls. Since H. pylori infection induces a local and systemic type of immune response, the serum IgG antibody concentration can be used as a potential predictor of the development of CA in patients.8-10
Molecular methods such as PCR have been widely used for detecting cagA and vacA genes of H. pylori. These genotypes can be used as markers for infections since the specificity and sensitivity of PCR are similar to those of culture.11-13 Primary isolation and culture of H. pylori are often difficult, as false-negative results may arise owing to a number of factors, such as its fastidious, microaerophilic nature and requirement of lengthy culture times.11,13,14 Therefore, an attempt was made to detect the virulent genotypes by PCR directly from gastric biopsy samples, and the serum IgG antibody levels were evaluated, as combined detection of these biomarkers is expected to increase the efficiency of diagnosis.
In view of the clinical and epidemiological importance of this gastric bacterium, the aim of our present study was to analyze the combination of serum and molecular markers and gastroduodenal conditions associated with H. pylori infection as risk factors for predicting gastric cancer development among dyspeptic patients.
Study design and study population
A hospital-based case-control study was conducted from December 2022 to November 2023 in the Microbiology laboratory in a tertiary care hospital situated in Guwahati, North eastern part of India.
The study population included 100 consecutive patients who were referred for routine upper gastrointestinal tract endoscopy for suspected gastritis, peptic ulcers or gastric carcinoma in the Department of Gastroenterology of our hospital and State Cancer Institute, Guwahati, Assam, during our study period and suffered from dyspeptic symptoms like abdominal discomfort, vomiting, nausea, bloating or fullness of the stomach were enrolled in our study. Prior to endoscopy, a peformed structured questionnaire was designed on paper to collect the self-reported information on the patients’ clinical history, age, sex, family history, smoking and alcohol history, intake of H2 blockers, etc. Informed written consent was obtained from all the patients included in the study or their guardians.
Out of 100, 71 (71%) were male patients whereas 29 (29%) were female patients. The age range of the patients was 11-84 years, with a mean age of 51.98 years and a SD of 16.45 years. On the basis of age, patients were grouped into two groups: 0-40 years and >40 years. All patients were also categorized into three groups based on the type of clinical lesion visible during endoscopic procedures: Group 1, Non-Ulcer Dyspepsia (NUD); Group 2, Ulcer and Inflammation (UIN); and Group 3, Gastric Cancer (CA). Of these, 35 patients had NUD, 38 had UIN, which included inflammation, chronic/erosive gastritis, and peptic ulcer disease, and the remaining 27 patients had CA.
Selection of cases and controls
The case (n=27) group included patients who had histopathologically confirmed lesions of CA, and the control group (n=73) included patients with signs other than CA, which included NUD (n=35) and UIN (n=38), during endoscopic procedures.
The present study was approved by the human ethics committee of our institution and was carried out according to the committee guidelines (Letter No. MC/190/2007/Pt-11/MAR-2020/23 dated 4/6/2020).
Clinical sample collection
Two gastric biopsy samples were obtained from each patient and placed in phosphate-buffered saline, one for the rapid urease test (RUT) and another for polymerase chain reaction (PCR) analysis. Additionally, serum samples were collected from the same patients for anti-H. pylori IgG antibody determination.
Detection of serum IgG antibody levels against H. pylori
Anti-Helicobacter pylori IgG antibodies in the serum samples of patients were estimated using the H. pylori IgG assay kit (Vidas, BioMerieux, France). According to the kit instructions, a test value of ≥1 was considered as a positive result and a test value of <0.75 was considered as a negative result. Sample values between these cutoffs was designated as equivocal.15
DNA extraction and PCR amplification
Genomic DNA was extracted from the biopsy samples using a Mini DNA extraction kit (QIAamp, QIAGEN, Germany) according to the kit instructions. After DNA extraction, the presence of H. pylori in the patients was confirmed by PCR targeting the urease gene of H. pylori (ureA) and 16S rRNA gene. For samples positive for both of these genes, the H. pylori virulence genes cagA and vacA with alleles s1, m1, s2 and m2 were amplified by multiplex PCR for determination of virulence. Primers used for all the PCR assays were designed on the basis of our previous studies4 (Table 1).
Table (1):
PCR primers for amplification of UreA, 16S rRNA, CagA and VacA genes
DNA region amplified |
Primer name |
Sequence (5́ – 3′) |
Amplicon size (bp) |
|---|---|---|---|
UreA |
HPU1 HPU2 |
GCCAATGGTAAATTAGTT CTCCTTAATTGTTTTTAC |
411 |
16S rRNA |
16S-F 16S-R |
GCTAAGAGATCAGCCTATGTCC TGGCAATCAGCGTCAGGTAATG |
522 |
CagA |
cag5c-F cag3c-R |
GTTGATAACGCTGTCGCTTC GGGTTGTATGATATTTTCCATAA |
350 |
VacA s1/VacA s2 |
VAI-F VAI-R |
ATGGAAATACAACAAACACAC CTGCTTGAATGCGCCAAAC |
259 (s1) 286 (s2) |
VacA m1/ VacA m2 |
VAG-F VAG-R |
CAATCTGTCCAATCAAGCGAG GCGTCAAAATAATTCCAAGG |
567 (m1) 642 (m2) |
PCR assay was carried out in a reaction volume 20 µl containing 2X PCR master mix (Promega Corporation, Madison, WI), MgCl2, deoxynucleotides, Taq polymerase, 50 ng of template DNA and 10 µM of the corresponding primers. The mixture was amplified as follows: initial denaturation at 95°C for 5 min, followed by 35 cycles of denaturation for 1 minute at 94°C, 1 minute of annealing (45°C for ureA gene, 55°C for 16S rRNA gene and cagA-vacA genes) and 1 min of extension at 72°C. The final extension was continued at 72°C for 5 min. For all PCR assays, genomic DNA from H. pylori ATCC strain 26695 was used as a positive control, and nuclease-free water was used as a template for the negative control. The amplified DNA products were analyzed via agarose gel electrophoresis.
Statistical data analysis
Data analysis was performed using the Epi-Info software (version 7.1.3; Atlanta, Georgia, US). Chi-square test was used for the data analysis, and a p value ≤0.05 was considered to be statistically significant. ROC curve analysis was performed to investigate the sensitivity and specificity of the serum IgG concentration against H. pylori for the prediction of CA. The concordance between the serum IgG antibody concentration and PCR assay results among CA-positive patients was measured using Cohen’s kappa coefficient. A kappa value of >0.70 indicated high agreement, a value between 0.40 to 0.70 as moderate or good agreement, and <0.40 as poor agreement.16
Detection of H. pylori in gastric biopsy samples
In this study, out of 100 gastric biopsy samples subjected to PCR and RUT, a total of 71 (71%) samples were positive for H. pylori ureA and 16S rRNA genes, whereas a total of 62 (62%) samples gave positive results by RUT. All RUT positive (n=62) samples were positive for H. pylori ureA and 16S rRNA genes. And the remaining RUT negative samples (n=9) also gave positive results by PCR.
Therefore, the overall rate of H. pylori positivity in our study was 71% (71/100) by PCR. An increased rate of H. pylori infection was observed in males (69%, 49/71) aged >40 years (80.2%; 57/71) compared with those aged less than 40 years. CA patients (case group) had a positivity rate of 35.2% (25/71), whereas the control group had a positivity rate of 64.7% (46/71) (UIN= 18/71; 25.3%, NUD = 28/71; 39.4%) (Tables 2 and 3).
Table (2):
Demographic profile and risk factors associated with H. pylori infection in the patients included in the study (n=100)
| Variables | H. pylori positive | H. pylori negative | |
|---|---|---|---|
| (n=71, %) | (n=29, %) | ||
| Age grp (yrs) (n=100) | 0-40 | 14 (19.7) | 11 (37.9) |
| >40 | 57 (80.2) | 18 (62.0) | |
| Sex (n=100) | Male | 49 (69.0) | 22 (75.8) |
| Female | 22 (30.9) | 7 (24.1) | |
| Family history with infection (n=100) | Yes | 18 (25.3) | 4 (13.7) |
| No | 53 (74.6) | 25 (86.2) | |
| Smoking habit (n=100) | Yes | 26 (36.6) | 9 (31.0) |
| No | 45 (63.3) | 20 (68.9) | |
| Alcohol habit (n=100) | Yes | 27 (38.0) | 11 (37.9) |
| No | 44 (61.9) | 18 (62.0) | |
| H2 blocker (n=100) | Yes | 34 (47.8) | 19 (65.5) |
| No | 37 (52.1) | 10 (34.4) | |
| Serum IgG status (n=100) | IgG seropositive | 45 (61.9) | 17 (58.6) |
| IgG seronegative | 26 (36.6) | 12 (41.3) | |
| CagA-VacA Status (n=100) | |||
| CagA-VacA genes | CagA-VacA Positive | 46 (64.7) | 0 |
| CagA-VacA negative | 25 (35.2) | 29 (100) | |
| VacA positive (n=46) | |||
| VacA gene | VacA s1 | 45 (97.8) | 0 |
| VacA m1 | 33 (71.7) | 0 | |
| VacA s2 | 1 (2.17) | 0 | |
| VacA m2 | 13 (28.2) | 0 | |
Seropositivity among H. pylori-positive patients
The percentage of H. pylori-positive patients who were seropositive for anti-Helicobacter pylori IgG antibodies in our study was 61.9% (45/71) (Table 1). It was substantially common in CA patients (18/25, 72%) than in controls (27/46; 58.6%) (Table 3, Table 4). It was also found to be greater in patients with UIN than in NUD patients (OR 1.81; 95% CI, 0.63-5.18; p < 0.001) (Figure 1).
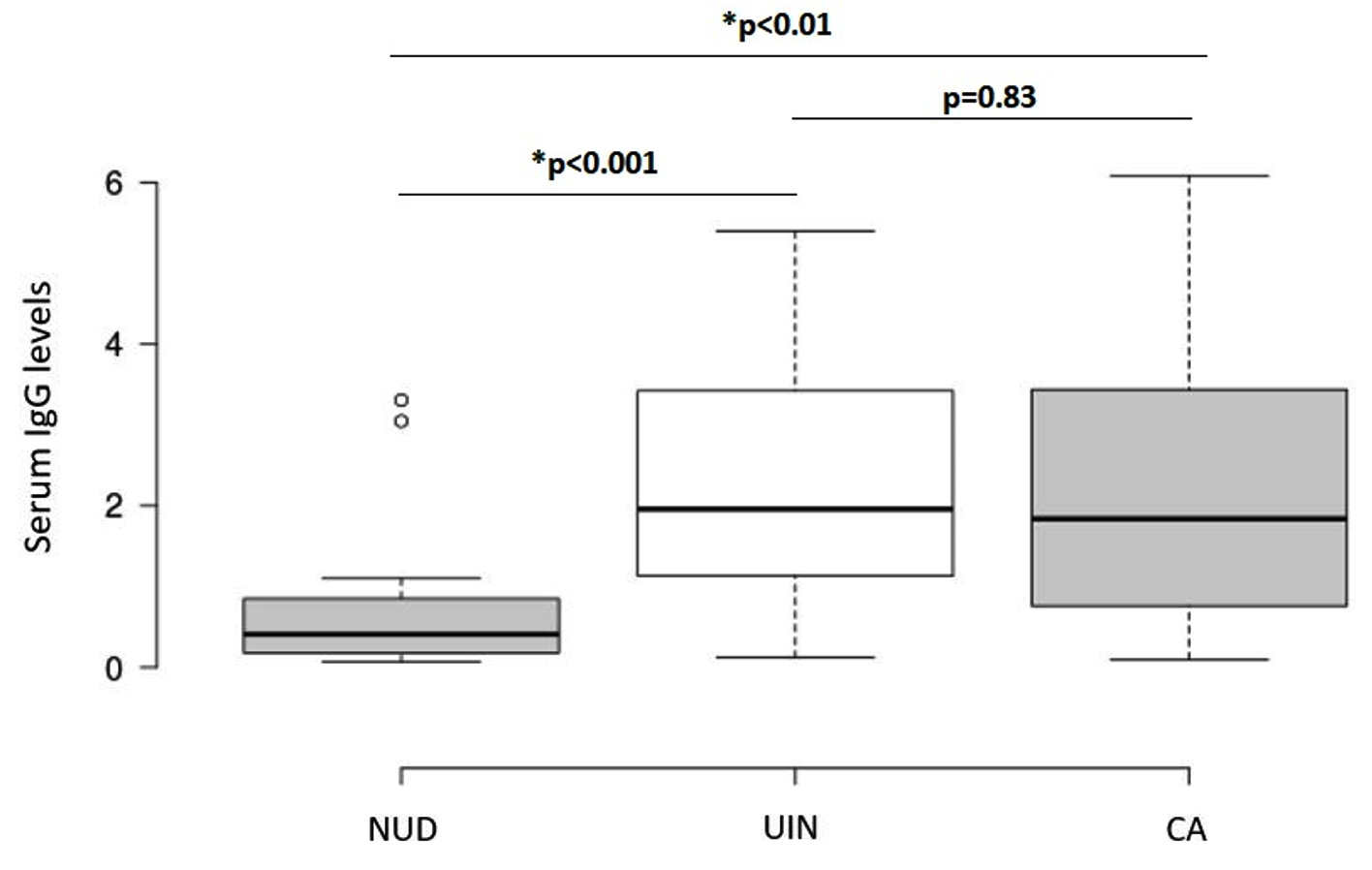
Figure 1. Anti-H. pylori IgG antibody titers according to the type of gastric lesion. A p value of ≤0.05 was considered to be statistically significant. NUD-Non-ulcer dyspepsia, UIN-Ulcer and inflammation, CA-Gastric cancer
Molecular analysis of H. pylori virulence genes
Among the 71 total H. pylori-positive patients, 46 (64.7%) had both the cagA and vacA genes. Out of 46 vacA gene positive, 45 (97.8%) belonged to vacA s1 allele and 33 (71.7%) belonged to vacA m1 allele. The prevalence of the vacA s2 genotype was 2.17% (1/46), and the vacA m2 genotype was found in 28.2% (13/46) patients (Table 2).
Association between status of H. pylori infection and its associated risk factors
Our study revealed significant associations between disease status and several risk factors, such as family history, H2 blocker use, serum IgG status, and the virulence factors cagA and vacA (p < 0.05) (Table 3). Patients who had a family history of gastric cancer were associated with higher incidence of infection (48%) than controls (13%) (p < 0.001; OR= 6.15; 95% CI, 1.92-19.68) (Table 3, Table 4).
Table (3):
Association and analysis of H. pylori associated risk factors with the disease conditions among 71 H. pylori-positive patients and controls
| Variables (Risk factors) | Clinical Conditions | OR | 95% CI | P value (significant at ≤0.05*) | ||||
|---|---|---|---|---|---|---|---|---|
| Cases (n=25, %) | Controls (n=46, %) | |||||||
| CA (a) (n=25,%) | UIN (b) (n=28,%) | NUD (c) (n=18,%) | Total (b+c) (n=46,%) | |||||
| Age grp (yrs)
(n=71) |
0-40 | 3 (12) | 8 (28.5) | 3 (16.6) | 11 (23.9) | 0.43 | 0.11-1.73 | 0.29 |
| >40 | 22 (88.0) | 20 (71.4) | 15 (83.3) | 35 (76.0) | ||||
| Sex (n=71) | Male | 18 (72.0) | 19 (67.8) | 12 (66.6) | 31 (67.3) | 1.24 | 0.43-3.62 | 0.91 |
| Female | 7 (28.0) | 9 (32.1) | 6 (33.3) | 15 (32.6) | ||||
| Family history (n=71) | Yes | 12 (48.0) | 5 (17.8) | 1 (5.5) | 6 (13.0) | 6.15 | 1.92-19.68 | 0.003457* |
| No | 13 (52.0) | 23 (82.1) | 17 (94.4) | 40 (86.9) | ||||
| Smoking habit (n=71) | Yes | 11 (44.0) | 7 (25.0) | 8 (44.4) | 15 (32.6) | 1.62 | 0.6-4.42 | 0.26049 |
| No | 14 (56.0) | 21 (75.0) | 10 (55.5) | 31 (67.3) | ||||
| Alcohol habit (n=71) | Yes | 11 (44.0) | 7 (25.0) | 9 (50) | 16 (34.7) | 1.47 | 0.54-3.99 | 0.174677 |
| No | 14 (56.0) | 21 (75.0) | 9 (50) | 30 (65.2) | ||||
| H2 blocker (n=71) | Yes | 7 (28.0) | 17 (60.7) | 10 (55.5) | 27 (58.6) | 0.27 | 0.1-0.78 | 0.04* |
| No | 18 (72.0) | 11 (39.2) | 8 (44.4) | 19 (41.3) | ||||
| Serum IgG status (n=71) | IgG sero- positive | 18 (72.0) | 22 (78.5) | 5 (27.7) | 27 (58.6) | 1.81 | 0.63-5.18 | 0.001* |
| IgG sero- negative | 7 (32.0) | 6(21.4) | 13 (72.2) | 19 (41.3) | ||||
| CagA-VacA status | ||||||||
| CagA- VacA | Positive | 23 (92.0) | 20 (71.4) | 3(16.6) | 23 (50.0) | 11.5 | 2.43-54.52 | <0.00001* |
| Negative | 2 (8.0) | 8 (28.5) | 15 (83.3) | 23 (50.0) | ||||
| VacA status | ||||||||
| VacA | VacAs1 | 23 (92.0) | 20 (71.4) | 2 (11.1) | 22 (47.8) | 11.5 | 2.43-54.52 | <0.00001* |
| VacA m1 | 15 (60.0) | 15 (53.5) | 3 (16.6) | 18 (39.1) | ||||
| VacA s2 | 0 | 0 | 1 (5.5) | 1 (2.17) | ||||
| VacA m2 | 8 (32.0) | 5 (17.8) | 0 | 5 (10.8) | ||||
Table (4):
Association between the significant risk factors (family history, Serum IgG and CagA-VacA status) and disease conditions in H. pylori positive patients
| Positive Variables | Control group | Cases group | P value (significant at ≤ 0.05*) | |||
|---|---|---|---|---|---|---|
| NUD (a) | UIN (b) | Total (a+b) | CA | |||
| Total | 18 | 28 | 46 | 25 | ||
| Family history | 1 (5.5%) | 5 (17.8%) | 6 (13%) | 12 (48%) | 0.003457* | |
| Serum IgG positive | 5 (27.7%) | 22 (78.5%) | 27 (58.6%) | 18 (72%) | 0.001* | |
| CagA-VacA status | CagA + VacA positive | 3 (16.6%) | 20 (71.4%) | 23 (50%) | 23 (92%) | <0.00001* |
| VacA s1 positive | 2 (11.1%) | 20 (71.4%) | 22 (47.8%) | 23 (92%) | <0.00001* (VacA) | |
| VacA m1 positive | 3 (16.6%) | 15 (53.5%) | 18 (39.1%) | 15 (60%) | ||
| VacA s2 positive | 1 (5.5%) | 0 | 1 (2.17%) | 0 | ||
| VacA m2 positive | 0 | 5 (17.8%) | 5 (10.8) | 8 (32%) | ||
Regarding the association between virulence factors cagA and vacA and disease conditions, the vacA s1 genotype was highly prevalent in CA cases (92%) than in the control group (47.8%) (p < 0.00001). Highest positivity of the cytotoxic cagA+vacA s1 gene combination was detected in CA patients (23/25; 92%), with an odds ratio (OR) of 11.5 (95% CI, 2.43-54.52; p < 0.0001), compared with that in the control group (23/46; 50%). Patients with NUD and UIN had positivity rates of 16.6% (3/18) and 71.4% (20/28), respectively, for both the cagA and vacA genes (Table 3, Table 4 and Figure 2).
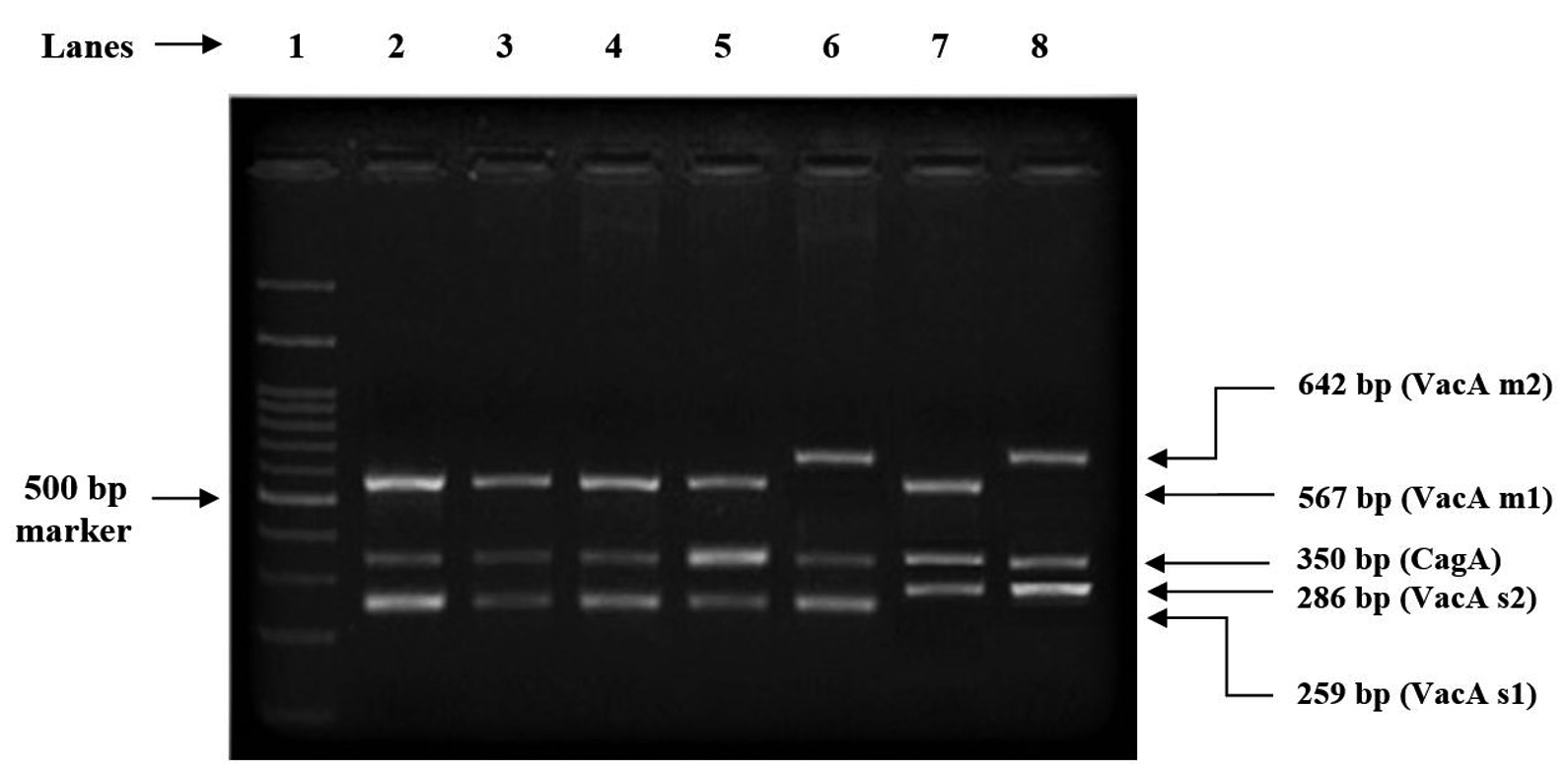
Figure 2. Amplification of virulence genes of H. pylori – CagA, VacA s1, VacA m1, VacA s2 and VacA m2 by multiplex PCR; Lane 1: 100 bp DNA ladder; Lane 2 to 5: CagA VacA s1m1 genotype; Lane 6: CagA VacA s1m2 genotype; Lane 7: CagA VacA s2m1 genotype; Lane 8: CagA VacA s2m2 genotype
The incidence of infection in patients with a history of consumption of alcohol was significantly greater (p < 0.05) in the NUD group (50%) than in the UIN group (25%). In contrast, this percentage was lower in patients with UIN (25%) than in patients with CA (44%). However, CA patients with a history of smoking and alcohol consumption had a significantly greater infection rate (p < 0.05) (56%) than in UIN patients (32.1%) (Table 3).
Agreement between the serum IgG antibody concentration and PCR assay results
The concordance between the serum IgG positivity and PCR positivity among the CA patients was 84%, with a k-coefficient of 0.41 indicating moderate agreement (p < 0.05).
Receiver operating characteristic curve (ROC) analysis
ROC curves were drawn for the patients with NUD, UIN and CA, and the area under the curve (AUC) was determined. According to standard values, an AUC value of >0.9 indicated high accuracy for the test, 0.7-0.9 indicated moderate accuracy, 0.5-0.7 indicated low accuracy and 0.5 indicated a chance result.17 A cutoff value of 0.215 was used to distinguish patients with NUD from those with UIN (AUC = 0.81), with a sensitivity of 89% and specificity of 72%. A cutoff value of 0.26 was used to distinguish patients with CA from those with NUD (AUC = 0.78), with a sensitivity of 92% and specificity of 66% (Figure 3a and 3b).
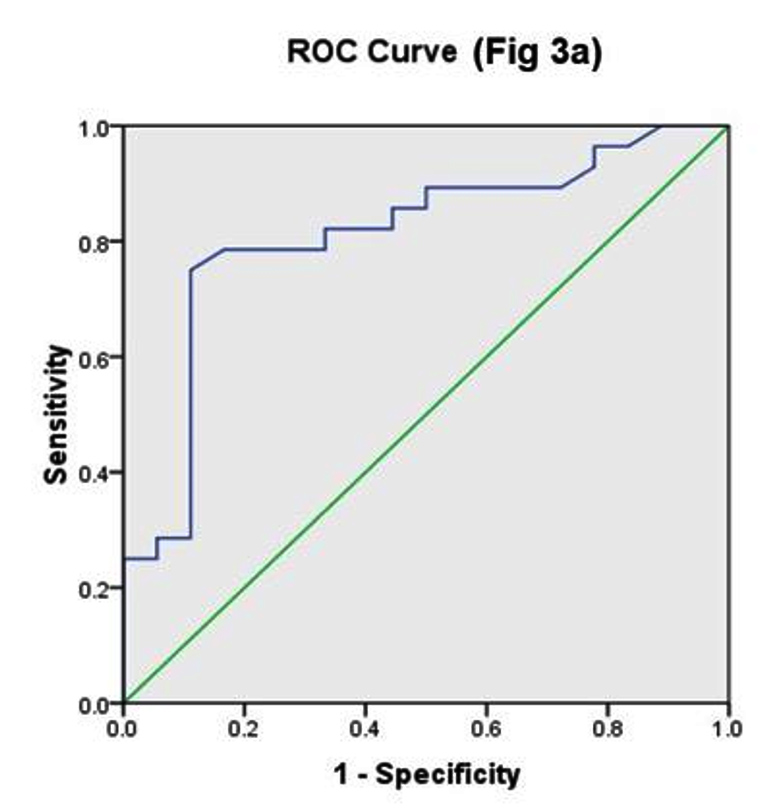
Figure 3a. Comparison of ROC areas among patients with NUD and UIN
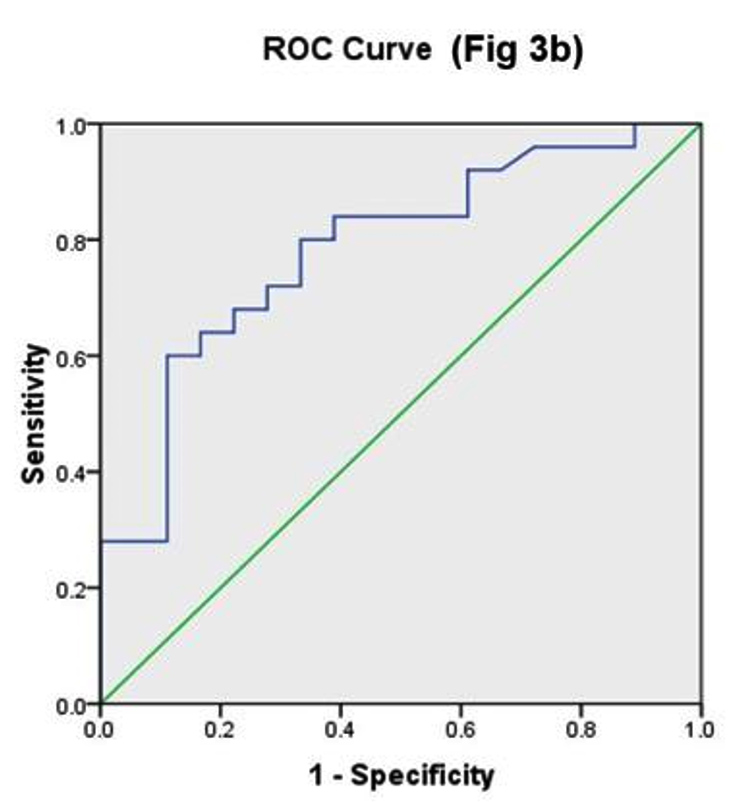
Figure 3b. Comparison of ROC areas among patients with CA and NUD
This current study examined the ability of markers and gastroduodenal conditions associated with H. pylori to predict disease outcome, which may help in identifying individuals regarding their risk of future occurrence of gastrointestinal pathology, including gastric cancer.
High prevalence of CA among family members or relatives may be attributed to the fact that CA patients and members of the same family may share potential factors associated with risk of infection, such as environmental exposure to infection, a common diet and the genetic aspects that may play a crucial role in regulating various immune mechanisms to H. pylori infection.18 Previous studies conducted in China, Korea and other western regions have reported that a family history of CA in a first-degree relative, for example, having a cancer-affected member of the same family, is associated with a 10-fold increased risk of upper gastrointestinal tract cancer.18-22 Various H. pylori genotype characterization studies revealed the vacAs1 genotype to be associated with high levels of cytotoxic activity than other allelic variants.4,23,24 Numerous studies from India and other parts of the world have demonstrated that both the vacA s1 and cagA genes are significantly associated with CA.5,7,24-26 Our results were consistent with those of a study performed by Andreson et al., in which there was a 99% correlation between the presence of the cagA gene and the vacA signal sequence type s1a.27 The reason for this difference in expression is unclear, but both the cagA and vacA genotypes may be structurally or functionally interrelated and may play a putative role in the clinicopathological manifestations of this disease.28,29 Early detection of strains harboring such virulence determinants could be helpful in providing information on patient groups at high risk for gastric cancer.
Our analysis indicated near high or moderate accuracy of serum IgG as a diagnostic biomarker for detecting the presence of infection, thus differentiating between individuals with NUD, UIN or CA. However, in endemic countries such as India, where the CA incidence is high, only the serum IgG concentration is not sufficient to determine the presence of H. pylori in detecting high-risk CA population; therefore, family history combined with molecular data should always be taken into consideration.
Although the serum IgG status of the infected patients in our study was greater in the CA patients than in the controls, the H. pylori positivity rate in the CA patients was lower than that in the controls (64.7%; 46/71). A North Indian study also found greater prevalence of H. pylori in the control group than in the cases group (80% vs 78%).30 The presence of serum IgG antibody in the blood is indicative of bacterial invasion, due to which there is a decrease in colonization. This can be considered indirect evidence that even if the H. pylori positivity rate in CA patients was lower than that in controls in our study, the mere absence of infection cannot be ruled out without accessing serum IgG levels.
During our course of study, H. pylori infection was generally assessed after the patient presented with onset or development of cancer. This may also explain why there was more positivity in the control group than in the case group, possibly reflecting the fact that the development of CA with the onset of severe atrophy and intestinal metaplasia may lead to the loss of colonization of this gastric pathogen in the stomach mucosa.31
Study limitations
A major limitation of our study is that a limited number of clinical samples were analyzed. Therefore, a definite strategy that could guide clinicians in the evaluation of definite cutoff values for disease prediction and discrimination of diseased and non-diseased populations could not be achieved. For these reasons, the cutoff values achieved need to be considered representative values and thus need to be further authenticated in larger clinical samples. Additionally, no healthy subjects were included in the study as controls.
In conclusion, a family history of CA, an increased serum IgG concentration and the presence of the cagA–vacA s1 genotype of H. pylori may be considered strong predictors of future gastric pathologies, including cancer. NUD patients and patients with UIN infected with virulent genotypes may require more attention for treatment and eradication to prevent the risk of developing further gastric complications. We believe that this study provides a foundation for the prediction and analysis of the course of gastric adenocarcinoma development as well as its prevention and will facilitate future and ongoing research in this field.
ACKNOWLEDGMENTS
The authors would like to acknowledge the Department of Health Research, Ministry of Health and Family Welfare, Government of India, for providing financial support for the study. The authors also thank the staff of the endoscopy unit of the Department of Gastroenterology and State Cancer Institute, Gauhati Medical College, Guwahati, Assam, India, for providing the gastric biopsy samples and blood samples required for the study.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
This study was supported by the Department of Health Research, Ministry of Health and Family Welfare, Government of India, under the HRD scheme “Fellowship Programme to Young Scientists” vide Sanction letter No.12014/32/2020-HR/E-Office:8047051, dated 07/08/2020.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Gauhati Medical College and Hospital, Gauhati, India, vide letter No. MC/190/2007/Pt-11/MAR-2020/23 dated 4/6/2020.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Morgan E, Arnold M, Camargo MC, et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020-40: A population-based modelling study. E Clinical Medicine. 2022;47:101404.
Crossref - Misra V, Pandey R, Misra SP, Dwivedi M. Helicobacter pylori and gastric cancer: Indian enigma. World J Gastroenterol. 2014;20(6):1503-1509.
Crossref - Rahman R, Asombang AW, Ibdah JA. Characteristics of gastric cancer in Asia. World J Gastroenterol. 2014;20(16):4483-4490.
Crossref - Sarma A, Saikia L, Bhuyan RK, Hussain ME. Molecular identification and detection of virulent factors in Helicobacter pylori from gastric biopsy samples of patients attended at Assam Medical College and Hospital, Dibrugarh, Assam, India. Indian J Med Microbiol. 2017;35(4):600-603.
Crossref - Memon AA, Hussein NR, Miendje DVY, Burette A, Atherton JC. Vacuolating cytotoxin genotypes are strong markers of gastric cancer and duodenal ulcer-associated Helicobacter pylori strains: a matched case-control study. J Clin Microbiol. 2014;52(8):2984-2989.
Crossref - Saber T, Ghonaim MM, Yousef AR, et al. Association of Helicobacter pylori cagA Gene with Gastric Cancer and Peptic Ulcer in Saudi Patients. J Microbiol Biotechnol. 2015;25(7):1146-1153.
Crossref - Venkateshwari A, Krishnaveni D, Venugopal S, Shashikumar P, Vidyasagar A, Jyothy A. Helicobacter pylori infection in relation to gastric cancer progression. Indian J Cancer. 2011;48(1):94-98.
Crossref - Shiota S, Yamaoka Y. Biomarkers for Helicobacter pylori infection and gastroduodenal diseases. Biomark Med. 2014;8(9):1127-1137.
Crossref - Nishizuka SS, Nakatochi M, Koizumi Y, et al. Anti-Helicobacter pylori antibody status is associated with cancer mortality: A longitudinal analysis from the Japanese DAIKO prospective cohort study. PLOS Glob Public Health. 2023;3(2):e0001125.
Crossref - Yu JH, Zhao Y, Wang XF, Xu YC. Evaluation of Anti-Helicobacter pylori IgG Antibodies for the Detection of Helicobacter pylori Infection in Different Populations. Diagnostics. 2022;12(5):1214.
Crossref - Mégraud F, Lehours P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin Microbiol Rev. 2007;20(2):280-322.
Crossref - Monteiro L, de Mascarel A, Sarrasqueta AM, et al. Diagnosis of Helicobacter pylori infection: noninvasive methods compared to invasive methods and evaluation of two new tests. Am J Gastroenterol. 2001;96(2):353-358.
Crossref - van Zwet AA, Thijs JC, Kooistra-Smid AM, Schirm J, Snijder JA. Sensitivity of culture compared with that of polymerase chain reaction for detection of Helicobacter pylori from antral biopsy samples. J Clin Microbiol. 1993;31(7):1918-20.
Crossref - Allahkarami S, Shahhosseiny MH, Roodbari NH and Esmaeili D. Comparison of Two Rapid Urease Test (RUT) and Culture Diagnostic Methods with PCR Technique to Detect Helical and Coccoid Forms of Helicobacter pylori in Clinical and Environmental Samples.
J Pure Appl Microbiol. 2015;9(1):33-40 - Lee SY, Moon HW, Hur M, Yun YM. Validation of western Helicobacter pylori IgG antibody assays in Korean adults. J Med Microbiol. 2015;64(5):513-518.
Crossref - McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276-822.
Crossref - Fischer JE, Bachmann LM, Jaeschke R. A readers’ guide to the interpretation of diagnostic test properties: clinical example of sepsis. Intensive Care Med. 2003;29(7):1043-1051.
Crossref - Choi HG, Chun W, Jung KH. Association between gastric cancer and the family history of gastric cancer: a cross-sectional study using Korean Genome and Epidemiology Study data. Eur J Cancer Prev. 2022;31(5):408-414.
Crossref - Yaghoobi M, Bijarchi R, Narod SA. Family history and the risk of gastric cancer. Br J Cancer. 2010;102(2):237-242.
Crossref - Wu R, Yang C, Ji L, Fan ZN, Tao YW, Zhan Q. Prevalence of gastric cancer precursors in gastroscopy-screened adults by family history of gastric cancer and of cancers other than gastric. BMC Cancer. 2020;20(1):1110.
Crossref - Song M, Camargo MC, Weinstein SJ, et al. Family history of cancer in first-degree relatives and risk of gastric cancer and its precursors in a Western population. Gastric Cancer. 2018;21(5):729-737.
Crossref - Man J, Ni Y, Yang X, et al. Healthy Lifestyle Factors, Cancer Family History, and Gastric Cancer Risk: A Population-Based Case-Control Study in China. Front Nutr. 2021;8:774530.
Crossref - Keikha M, Ali-Hassanzadeh M, Karbalaei M. Association of Helicobacter pylori vacA genotypes and peptic ulcer in Iranian population: a systematic review and meta-analysis. BMC Gastroenterol. 2020;20(1):266.
Crossref - Miehlke S, Kirsch C, Agha-Amiri K, et al. The Helicobacter pylori vacA s1, m1 genotype and cagA is associated with gastric carcinoma in Germany. Int J Cancer. 2000;87(3):322-327.
Crossref - Mukhopadhyay AK, Kersulyte D, Jeong JY, et al. Distinctiveness of genotypes of Helicobacter pylori in Calcutta, India. J Bacteriol. 2000;182(11):3219-3227.
Crossref - Brasil-Costa I, Souza CdeO, Monteiro LCR, Santos MES, de Oliveira EHC, Burbano RMR. H. pylori Infection and Virulence Factors cagA and vacA (s and m Regions) in Gastric Adenocarcinoma from Para State, Brazil. Pathogens. 2022;11(4):414.
Crossref - Andreson H, Loivukene K, Sillakivi T, et al. Association of cagA and vacA genotypes of Helicobacter pylori with gastric diseases in Estonia. J Clin Microbiol. 2002;40(1):298-300.
Crossref - Abdullah M, Greenfield LK, Bronte-Tinkew D, Capurro MI, Rizzuti D, Jones NL. VacA promotes CagA accumulation in gastric epithelial cells during Helicobacter pylori infection. Sci Rep. 2019;9(1):38.
Crossref - Jones KR, Whitmire JM, Merrell DS. A Tale of Two Toxins: Helicobacter Pylori CagA and VacA Modulate Host Pathways that Impact Disease. Front Microbiol. 2010;1:115.
Crossref - Misra V, Misra SP, Singh MK, Singh PA, Dwivedi M. Prevalence of H. pylori in patients with gastric cancer. Indian J Pathol Microbiol. 2007;50(4):702-707.
- Helicobacter and Cancer Collaborative Group. Gastric cancer and Helicobacter pylori: a combined analysis of 12 case control studies nested within prospective cohorts. Gut. 2001;49(3):347-353.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.