


ISSN: 0973-7510
E-ISSN: 2581-690X
Influenza A virus (IAV) is the principal cause of seasonal flu and is often reported among pilgrims in Saudi Arabia (SA) due to their mass gatherings. The epidemiological, phylogenetic, and molecular details of A/H1N1pdm2009 in 200 clinical samples collected from hospitalized children in Riyadh during two epidemic seasons (2020/21 and 2021/22) are reported in this study. A total of 21 (10.50%) samples were positive for IAV, as determined using PCR. Fifteen isolates (71.42%) were identified as H1N1pdm2009: eight (53.33%) samples were from males, seven (46.67%) from females. The prevalence of H1N1pdm2009 isolates was significantly (p < 0.05) higher among the age group 15-64 years than the other age groups. A comparison of hemagglutinin (HA) and neuraminidase (NA) amino acid sequences between SA H1N1pdm and certain vaccine strains revealed 19 mutations relative to reference strain A/California/07/2009. Among them, eight (0.47%) were in HA, and eight (0.56%) were in NA sequences that differed from vaccine strains. All isolates of the 2020–2022 seasons exhibited N- and O-glycosylation sites comparable to vaccine strains. Phylogenetically their HA and NA genes are divided into different clades. Most of the studied isolates (five) belonged to clade 5a.1 of HA. These data identify the genetic makeup of circulating influenza virus subtypes.
Influenza A Virus, A/H1N1pdm2009, Phylogenetic Analysis, Recommended Vaccine Strains
Acute respiratory tract infections (ARTIs) have long been recognized as a major source of death and morbidity worldwide. Every year, an estimated 3.9 million individuals die from ARTIs.1 Annually, influenza, a serious respiratory virus infection, causes significant seasonal morbidity and mortality, usually during the winter. Annual influenza epidemics inflect one billion infected cases, three to five million episodes of serious illness, and estimated fatalities of 300,000-500,000.2 Influenza viruses are members of the Orthomyxoviridae family with an RNA genome that is segmented single-stranded negative-sense3; categorized into four genera: influenza A (Alphainfluenzavirus), influenza B (Betainfluenzavirus), influenza C (Gammainfluenzavirus), and influenza D (Deltainfluenzavirus).3 Only types A, B, and C affect people of all ages, causing mild to severe illness and being the cause of all previous influenza pandemics and seasonal epidemics.2,4
Influenza viruses possess two main glycoproteins with antagonistic activities: hemagglutinin (HA) and neuraminidase (NA). HA binds to the receptor for sialic acid on the cell surface, whereas NA protein releases it from host cells. Most influenza vaccinations target the HA and NA antigens on the viral surface. However, influenza vaccinations are now primarily HA-based on the market.5 Due to the rapid antigenic shift/drift of the influenza HA and NA glycoproteins, any vaccination that aims to elicit the typical neutralizing responses to HA and/or NA must manage antigenic drift.6,7 The influenza virus strains that spread across the population and mutate over time are subject to evolutionary change.8
The pandemic A/H1N1 (H1N1 pdm09) virus, which caused a worldwide outbreak in early 2009, was the product of a quadruple reassortment of IAV, which included two swine, one human, and one avian strain, presumably recombined via pigs as an intermediate mammalian host.9 The relationship between the A/H1N1 pdm09 strain and human seasonal A/H1N1 is a significant cause of misunderstanding among the general public.10,11 The A/H1N1 pdm09 HA was produced from the classic A/H1N1 swine lineage, which has diverged genetically and antigenically from the more quickly changing human seasonal A/H1N1 strain over the years.12
Saudi Arabia is among the nation’s most susceptible to spreading and evolving respiratory viruses since it hosts two major yearly global religious gatherings.13-16 The molecular and clinical epidemiological characteristics of the A/H1N1 subtype are currently poorly characterized in the Riyadh region.17-19 Over time, the influenza virus strains circulating in the population shift and change.8 The current study aims to identify the epidemiological features and genetic diversity of the A/H1N1pdm2009 in Riyadh during the winters of 2020/21 and 2021/22.
A total of 200 nasopharyngeal aspirates (NPAs) from patients with probable influenza infection and acute respiratory symptoms (rhinorrhea, cough, dyspnea, and fever) were collected during the epidemic years 2020/21 and 2021/22. Sampling was conducted during the fall-winter period between September and December of 2020/21 and 2021/22. Patients signed informed consent forms before they were permitted to participate in the study. The institutional review board (IRB) of the University Hospital provided the approval of the study protocol (Ethics Reference No. 20/5522/IRB). Data were collected and accessed for research in March 2021 and March 2022.
Detection, sequencing, and typing of IAV
Clinical samples were processed using the QIAamp Viral RNA Mini Kit (Qiagen, Hilden, Germany) to extract viral RNA. IAV was identified and typed using the One-Step Ahead RT-PCR Kit (Qiagen, Hilden, Germany) using a GeneAmp 9700 thermal cycler (Applied Biosystems, USA). Thermocycling was carried out in this study, as mentioned in Table 1. For the identification of amplified PCR products, a 100 bp Plus DNA ladder (Qiagen in Hilden, Germany) was used for comparison by electrophoresis on a 1% agarose gel stained with ethidium bromide.
Table (1):
Thermocycling conations in this study
| Step | Temperature | Time | Cycles |
|---|---|---|---|
| Reverse transcription | 50°C | 30 min. | 1 cycle |
| Initial PCR activation | 95°C | 15 min. | 1 cycle |
| Cycling: | |||
| Denaturation | 94°C | 15 sec | 40 cycles |
| Primer Annealing | 52°C | 30 sec | |
| Extension | 72°C | 2 min | |
| Final extension | 72°C | 5 min | 1 cycle |
| Hold | 4°C | ∞ | |
The HA and NA antigenic glycoprotein genes from A/H1N1pdm2009 were amplified using the same kit. Two overlapping primer sets were used to get complete HA and NA genes. The list of primers used in this study is shown in Table 2. The sequences of eight A/H1N1pdm2009 isolates were chosen to represent the whole positive sample from each of the two epidemic years (2020/21 and 2021/22). HA and NA gene sequencing was conducted commercially by Macrogen Inc., Seoul, South Korea.
Table (2):
IAV testing, typing, and sequencing primers used in this study
| Primer description | Type/ subtype | Gene | Primer name | Sequence 5’-3’ | Product Size (bp) | |
|---|---|---|---|---|---|---|
| Primers used for detection | IAV | M | M30F2/08 | ATGAGYCTTYTAACCGAGGTCGAAACG | 244 | 55°C |
| M264R3/08 | TGGACAAANCGTCTACGCTGCAG | |||||
| Primers used for typing | (H1N1) Pdm09 | HKU-SWF | TGAGCTCAGTGTCATCATTTGA | 174 | 57°C | |
| HKU-SWR | TGCTGAGCTTTGGGTATGAA | |||||
| Primers used for sequencing | H1N1 | HA | H1-F1 | AGCAAAAGCAGGGGAAAATAAAAGC | 1264 | 58°C |
| H1-R1 | CCTACTGCTGTGAACTGTGTATTC | |||||
| H1-F2 | GGGAGAATGAACTATTACTGG | 979 | 50°C | |||
| H1-R2 | AGTAGAAACAAGGGTGTTTTT | |||||
| NA | N1-F1 | AGCAAAAGCAGGAGTTTAAAATG | 1099 | 56°C | ||
| N1-R1 | CCTATCCAAACACCATTGCCGTAT | |||||
| N1-F2 | GGAATGCAGAACCTTCTTCTTGAC | 1073 | 58°C | |||
| N1-R2 | ATATGGTCTCGTATTAGTAGAAACAAGGAGTTTTTT | |||||
Sequence and phylogenetic data analysis
The A/H1N1pdm2009 whole HA and NA genes were sequence edited, divergence analyzed, mutation sites identified, and amino acid changes predicted using the BioEdit 7.0 software (Ibis Biosciences, Carlsbad, CA). The sequence data of reference strains recommended by the World Health Organization (WHO) and reference strains from known clades were collected from the GISAID and GenBank® public databases (Supplementary Table 1). The potential N-glycosylation or O-glycosylation sites were predicted using NetNGlyc 1.0.20,21 and NetOGlyc 3.1.22 According to the neighbor-joining method, the phylogeny tree was created using MEGA 7.0 (Pennsylvania State University, University Park, PA, USA). The numbers at the internal nodes of the tree represent the bootstrap values of 1,000 replicates.23
Statistical analysis
Categorical variables were compared using Fisher’s exact test. The Z-test with Bonferroni adjustment was used for the post-hoc comparison. Significance was considered at P < 0.05.
IAV detection and subtyping
During the two study seasons (winters 2020/21 and 2021/22), the prevalence of IAV was 21 (10.50%), with A/H1N1pdm2009 isolates accounting for 15 (71.42%). Age categories were divided following the population at high risk for contracting ILI (influenza-like illness) or ARI (acute respiratory sickness) into four separate age categories: 0-4, 5-14, 15-64, and ≥65 years.24,25 The frequency of A/H1N1pdm2009 isolates varied across age categories. The age group 15–64 years had a substantially greater prevalence of A/H1N1pdm2009 isolates than the other age groups (p < 0.05). Based on sex, there were more H1N1pdm2009 isolates in males, eight (53.33%), than in females, seven (46.67%) of all cases (Table 3).
Table (3):
Sample distribution across epidemic seasons, gender, and age groups
| No. of samples n (%) | Positive for IAV n (%) | Positive for H1N1pdm2009 n (%) | ||
|---|---|---|---|---|
| Season | 2020/21 | 100 (50) | 9 (42.85) | 7 (33.33) |
| 2021/22 | 100 (50) | 12 (57.14) | 8 (38.09) | |
| Total | 200 (100) | 21 (10.50) | 15 (71.42) | |
| Gender | Male | 103 (51.5) | 12 (57.14)a | 8 (53.33)a |
| Female | 97 (48.5) | 9 (42.85) | 6 (46.67) | |
|
Age in years |
0-4 | 35 (17.50) | 3 (14.29) | 2 (13.33) |
| 5-14 | 41 (20.50) | 7 (33.33) | 4 (26.67) | |
| 15-64 | 73 (36.50) | 9 (42.86)b | 7 (46.67)c | |
| ≥65 | 51 (25.50) | 2 (9.52) | 2 (13.33) |
Data are displayed as percentages (%). aSignificant difference (p < 0.05) from females. bSignificantly different (p < 0.05) from age groups 0-4 and 65 years; cSignificantly different (p 0.05) from age group 65 years.
Sequence analysis of the HA gene of A/H1N1pdm2009 isolates
Using the Clustal W algorithm, eight A/H1N1pdm2009 study isolates’ complete HA gene nucleotide sequences (1701 nucleotides) were sequenced and aligned with sequences from 45 local and international A/H1N1pdm2009 strains from different clades that were widely disseminated (Supplementary Table 1) in the Gene bank and GISAID databases. In the HA gene of A/H1N1pdm2009 isolates, 58 altered nucleotide sites (3.4%) were observed, although only 19 (32.75%) changed the amino acids. Multiple sequence alignment of amino acid sequences relative to the sequences in the prototype strain (A/California/07/2009) and current vaccine strain demonstrated that among 18 mutations, four (22.22%) had never been discovered before and were therefore thought to be unique mutations as opposed to the vaccine strains (T120A, D129N, P183S, S185T, and N2601D) (Table 4).
Table (4):
Changes in the amino acid in the HA1 domain of H1N1pdm2009 strains in comparison with the A/California/07/2009 strain
Mutation sites |
74 |
83 |
84 |
97 |
120 |
129 |
156 |
162 |
163 |
164 |
183 |
185 |
203 |
216 |
222 |
223 |
256 |
260 |
289 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
A/California/7/2009 |
S |
P |
S |
D |
T |
N |
X |
S |
K |
S |
S |
S |
S |
I |
X |
X |
A |
N |
K |
A/Saudi_Arabia/39/2020 |
S |
S |
N |
N |
A |
N |
N |
N |
Q |
S |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Saudi_Arabia/83/2020 |
S |
S |
N |
N |
A |
N |
N |
N |
Q |
S |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Saudi_Arabia/57/2020 |
R |
S |
N |
N |
A |
N |
N |
N |
Q |
T |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Saudi_Arabia/69/2021 |
R |
S |
N |
N |
A |
N |
N |
N |
Q |
T |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Saudi_Arabia/85/2021 |
R |
S |
N |
N |
A |
N |
N |
N |
Q |
T |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Saudi_Arabia/86/2021 |
R |
S |
N |
N |
T |
D |
N |
N |
Q |
T |
P |
I |
T |
T |
D |
Q |
T |
D |
K |
A/Saudi_Arabia/70/2022 |
R |
S |
N |
N |
T |
D |
N |
N |
Q |
T |
P |
I |
T |
T |
D |
Q |
T |
D |
K |
A/Saudi_Arabia/65/2022 |
R |
S |
N |
N |
T |
D |
N |
N |
Q |
T |
P |
I |
T |
T |
D |
Q |
T |
D |
K |
A/Wisconsin/67/2022 |
R |
S |
N |
N |
T |
D |
K |
N |
Q |
T |
P |
I |
T |
T |
D |
Q |
T |
E |
E |
A/Sydney/5/2021 |
R |
S |
N |
N |
T |
D |
K |
N |
Q |
T |
P |
I |
T |
A |
D |
Q |
T |
D |
E |
A/Guangdong/Maonan/SWL1536/2019 |
R |
S |
N |
N |
T |
N |
N |
N |
Q |
T |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Victoria/2570/2019 |
R |
S |
N |
N |
A |
N |
N |
N |
Q |
T |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Wisconsin/588/2019 |
R |
S |
N |
N |
A |
N |
N |
N |
Q |
T |
S |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Hawaii/70/2019 |
R |
S |
N |
N |
T |
N |
N |
N |
Q |
T |
P |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Brisbane/0/22018 |
R |
S |
N |
N |
T |
N |
N |
N |
Q |
T |
P |
T |
T |
T |
D |
Q |
T |
N |
E |
A/Michigan/45/2015 |
R |
S |
N |
N |
T |
D |
K |
N |
Q |
T |
P |
T |
T |
T |
D |
Q |
T |
N |
E |
Sequence analysis of the NA gene of H1N1pdm2009 isolates
The study strain’s NA gene sequence had 65 nucleotide mutation sites (4.61%) and 15 nucleotide substitutions that changed amino acids. The prepared NA gene sequences’ nucleotide lengths were 1410 bp. However, eight (0.56%) had never been seen before and were regarded as distinct mutations, unlike the vaccine strains (Table 5).
Table (5):
Changes in the amino acid in the NA protein of Saudi Arabian H1N1 strains (seasons 2020-2022) in comparison with the vaccine strains
Mutation sites |
51 |
72 |
74 |
77 |
81 |
128 |
253 |
257 |
|---|---|---|---|---|---|---|---|---|
A/California/7/2009 |
Q |
T |
F |
G |
V |
E |
Y |
R |
A/Saudi_Arabia/39/2020 |
Q |
I |
F |
R |
A |
E |
N |
K |
A/Saudi_Arabia/83/2020 |
Q |
T |
F |
G |
V |
E |
Y |
R |
A/Saudi_Arabia/57/2020 |
K |
T |
S |
R |
A |
K |
N |
K |
A/Saudi_Arabia/69/2021 |
Q |
I |
F |
R |
A |
K |
Y |
R |
A/Saudi_Arabia/85/2021 |
Q |
I |
F |
R |
A |
E |
N |
K |
A/Saudi_Arabia/86/2021 |
K |
I |
S |
R |
A |
K |
Y |
R |
A/Saudi_Arabia/70/2022 |
K |
T |
S |
R |
A |
K |
Y |
R |
A/Saudi_Arabia/65/2022 |
Q |
T |
F |
G |
V |
E |
Y |
R |
A/Wisconsin/67/2022 |
K |
T |
S |
R |
A |
E |
Y |
R |
A/Sydney/5/2021 |
Q |
T |
F |
G |
V |
E |
Y |
R |
A/Guangdong/Maonan/SWL1536/2019 |
K |
T |
S |
R |
A |
E |
Y |
R |
A/Victoria/2570/2019 |
K |
T |
S |
R |
A |
E |
Y |
R |
A/Wisconsin/588/2019 |
K |
T |
S |
R |
A |
E |
Y |
R |
A/Hawaii/70/2019 |
Q |
T |
F |
G |
V |
E |
Y |
R |
A/Brisbane/02/2018 |
Q |
I |
F |
R |
A |
E |
Y |
R |
A/Michigan/45/2015 |
Q |
T |
F |
R |
A |
E |
Y |
R |
Analysis of amino acid sequence N- and O-glycosylation sites
The number of sites for N-glycosylation on the HA protein of the A/H1N1pdm2009 isolates under investigation ranged between five and six. The A/H1N1pdm2009 isolates used in this study and the vaccine strains contained an N-glycosylation site. In contrast (Figure 1 A), the serine and threonine residues of the HA domain had substantial O-linked glycosylation. Two to four N-glycosylations were observed in the NA protein of A/H1N1pdm2009 sequences under investigation. Moreover, 31-36 O-glycosylation sites were observed (Figure 1 B).
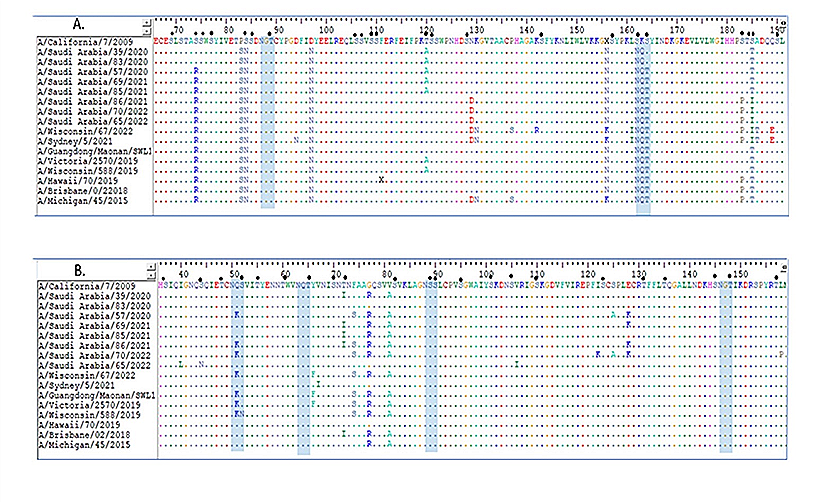
Figure 1. Alignment of amino acid sequences for two target proteins deduced from nucleotide sequences HIN1pdm2009. (A) HA amino acid sequences. (B) NA amino acid sequences. The A/California/7/2009 strain is used as a reference strain. Identical residues are shown by dots, whereas variations in amino acids are depicted by colored alphabets. Blue rectangles indicate the anticipated N-glycosylation sites. The expected O-glycosylation sites are represented by little filled circles
Phylogenetic analysis
To analyze the phylogeny of A/H1N1pdm2009 isolates, many reference sequences from GenBank and GISAID were used, including regional, global, and WHO-recommended influenza vaccine strains. The HA and NA gene sequences of the A/H1N1pdm2009 isolates were analyzed using phylogenetic methods, and the results revealed that the isolates were divided into three clades, with the majority belonging to the 5a.1 (Figures 2A and B).
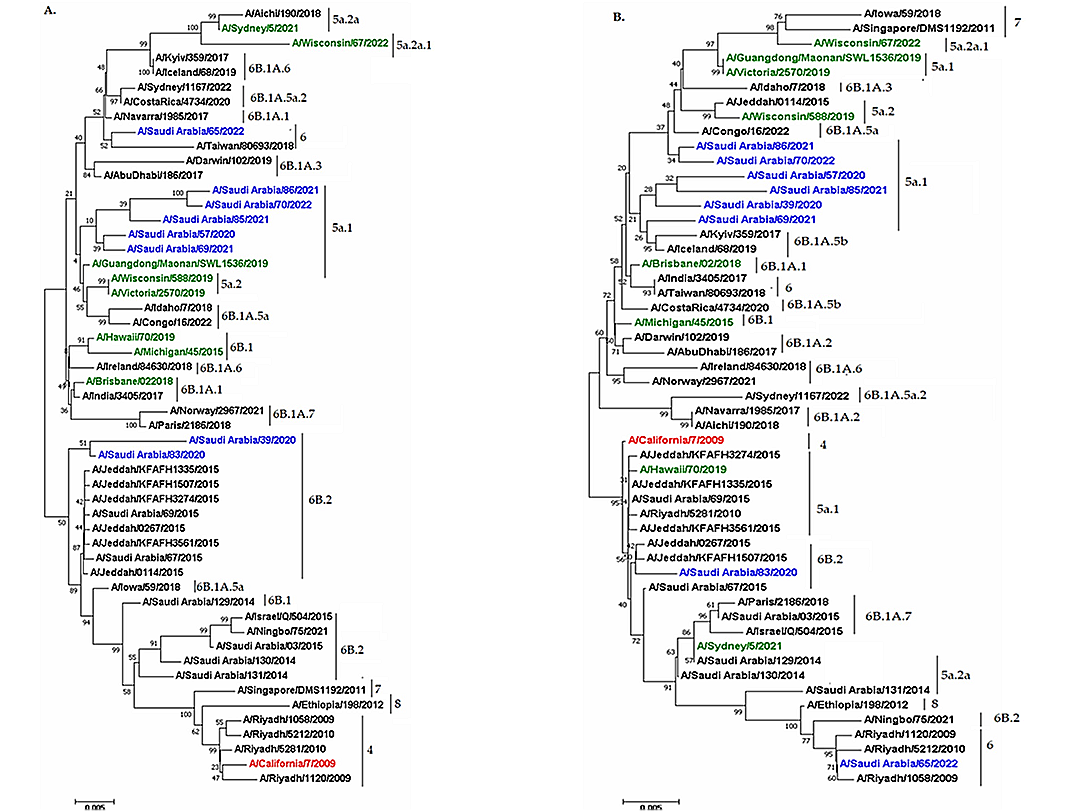
Figure 2. Phylograms of influenza H1N1pdm2009 viruses for two target genes. (A) phylogram based on based on HA gene. (B) phylogram based on NA gene. The neighbor-joining method was utilized by us of MEGA7 program. Study isolates are indicated with blue ink. Green represents the vaccine strain at the present time. The prototype strain is highlighted by red ink
Regular international labor migration into and out of the country and the large annual religious assembly of pilgrims from around the globe have contributed significantly to the diversity and spread of respiratory viruses in the Kingdom of Saudi Arabia (KSA).26 IAV-caused epidemics are to blame for all prior influenza pandemics and seasonal epidemics that have sparked public alarm around the world.2,27 Even though earlier studies in KSA identified the subtypes that cause IAV infections, current knowledge of the regional and temporal distribution of the A/H1N1pdm2009 subtype in Riyadh is not fully documented. Here, we provide an analysis of the sequence and phylogeny of the A/H1N1pdm2009 subtype observed in clinical samples from Riyadh between 2020 and 2022.
In the current study, PCR-based detection demonstrated that IAV was observed in 21 (10.50%) with A/H1N1pdm2009 isolates accounting for 15 (71.42%) during the two study seasons (winters 2020/21 and 2021/22) in Riyadh. Furthermore, among the overall cases, we discovered that eight male cases (53.33%) had higher incidence rates of the A/H1N1pdm2009 subtype than seven female cases (46.67%). People aged 15 to 64 were observed to have a considerably greater incidence of H1N1 isolates (p < 0.05), consistent with a recent investigation that showed A/H1N1pdm2009 isolates in 43 (48.8%) of the 88 IAV-positive samples in Riyadh throughout five seasonal IAVs (2014-18 and 2019/20), and that 23 (53.5%) of these isolates were more common in males and those between the ages of 30 (46.2) and (15-64).15 Similarly, between October 2015 and 2019, 526 (27.3%) cases of A(H1N1) were discovered in Jeddah. The patients’ median age was 31, and 50% were female. The majority of instances (50.2%) involved adult patients aged 19 to 60.14 During the Hajj gatherings from 2013 to 2015, seven of the 25 were subtyped as A/H1N1pdm2009.28 During the 2019 Hajj season, 185 clinical samples were tested, and 54 showed positive for the IAV. Of these, 27 samples were influenza A/H1N1 and 19/H3N2, four samples were influenza A (no type given), and four samples were influenza B.16 Additionally, a study of 15 nations in the Eastern Mediterranean Region reported that the A/H1N1pdm09 subtype was the most widely distributed; 1666 (58.5%) were A/H1N1 subtypes, followed by A/H3N2 671 (23.6%).29 The frequency of IAV fluctuated significantly throughout that time in many nations around the world, including Brazil 332 (23.62%),30 China 312 (3.1%),31 and Senegal 3993 (75%).32
In this study, considering multiple sequence alignment of amino acid sequences with respect to the sequences of the prototype strain (A/California/07/2009) and current vaccine strains, eight out of the 19 mutation sites in the HA gene have been observed (T120A, D129N, P183S, S185T, and N2601D) (Table 4). Early research indicated that P83S (100%) was the most frequent alteration in Cuban genomes. Further, S203T and D222E (Ca antigenic site), N156K and S162N (Sa antigenic site), and A186T and S203T were discovered in 85.7% of cases in comparison to the reference strain A/California/07/2009 (H1N1). Other significant alterations reported at antigenic sites included S203T and D222E (Ca antigenic site), N156K and S162N (Sa antigenic site), and A186T and S203T observed in 85.7% of patients as compared to the prototype strain A/California/07/2009 (H1N1).33 According to a recent study, the amino acid substitutions of S101N, N146D, P100S, D114N, K180Q, S202T, and S220T represent the majority of Indian isolates relative to (A/California/07/2009).34 According to previous reports.35 The globular head domain of the HA protein in A/H1N1 viruses possesses five sites of antigenicity, namely Ca1, Ca2, Cb, Sa, and Sb. Even a single amino acid mutation can impact the virus’s immunogenicity and the vaccine’s capacity to protect these critical sites for establishing antigenicity.36
Vaccination remains the best method of protection against influenza virus infections and their consequences, particularly for at-risk populations such as small children, older adults, and persons with underlying medical conditions.37-39 The HA and NA proteins were chosen as targets for the creation of a universal influenza virus vaccine. To improve the strategic control of influenza vaccination, a deeper comprehension of HA evolution and variation is required. Any vaccination strategy that aims to elicit the typical neutralizing responses to HA and/or NA must successfully manage antigenic drift. Therefore, IAV HA and NA antigenic drift should be considered as a possible target for a universal influenza vaccine. According to findings from HA sequence variation studies, HA changes in amino acids at Sa (residues 128 and 129, 156-160, 162-167) and Sb (residues 187-198) antigenic sites during infection are required for the selection of influenza vaccine strains.6 The Saudi Ministry of Health offered the following strains of the trivalent inactivated influenza virus vaccine: A/Singapore/INFIMH-16-0019/2016(H3N2)-like virus, A/Michigan/45/2015(H1N1) pdm-09 virus, and influenza B/Colorado/06/2017-like virus (B/Victoria/2/87 lineage).40 WHO has identified and recommended more than 28 vaccine strains.41 Representative 2023-2024 northern hemisphere vaccine strain A/Wisconsin/67/2022 and the 25 (H1N1) pdm09 strains exhibited nucleotide and amino acid similarity of 98.41-99.22% and 98.41-99.36%, respectively.11
In the current study, phylogenetic analysis of HA and NA sequences of A/H1N1pdm2009 isolates divided into three clades, with the majority belonging to the 5a.1. An earlier study reported that all the A/H1N1pdm2009 strains belonged to clade 6 viruses, where 73 (92%) grouped into sub-clade 6b.1 and 7 (8%) grouped into clade 6b.2 in Riyadh, Saudi Arabia, between 2014 and 2015.13 The A/H1N1 isolates have no significant connection to any strains used in influenza vaccines. Phylogenetic research, however, indicated that IAV strains did not typically cluster within regional isolates, which implies that travel may have contributed to the virus’s global spread.42 The WHO recommendations related to the influenza vaccines for utilization in both the northern and southern hemispheres were made with knowledge of the currently circulating viruses globally based on the year-round work of the WHO Global.43
The N-glycosylation sites A/H1N1pdm2009 isolates used in this study were from strains 5 and 6. Moreover, these N-glycosylation sites were observed in the vaccine strains. Variations in the N- and O-linked glycosylation of the HA and NA proteins can have an impact on the host specificity, pathogenicity, and infectivity of an influenza strain by altering the biological characteristics of HA and NA or indirectly by reducing binding to the receptor and blocking antigenic regions of the protein. In previous studies, it was reported that seasonal viruses had more glycosylation sites on the head of the HA and NA than A/H1N1 pdm09, and that two glycosylation sites (glycosylation sites 50 and 68) on the stalk of the NA in A/H1N1 pdm09 were probably substituted by two more glycosylation sites (glycosylation sites 44 and 70) in the seasonal strains.44,45 Furthermore, recent research has indicated that the HA globular head domain’s glycosylation serves to physically cloak the antigenic sites, inhibiting antibody identification and enabling viral evasion of antibody-mediated neutralization.6,46
The small cross-sectional sample size of this study was the major limitation. Additionally, the study is unable to identify a cause for recurrent infections. For a deeper understanding of the A/H1N1pdm2009 circulation pattern, additional rigorous studies focusing on larger sample sizes scattered over KSA in successive epidemic seasons are required.
PCR-based detection demonstrated that IAV was observed in 21 (10.50%), with A/H1N1pdm2009 isolates accounting for 15 (71.42%), during the two study seasons (winters 2020/21 and 2021/22) in Riyadh. In the overall number of cases, males (eight [53.33%]) were more likely to have the A/H1N1pdm2009 subtype than females (seven [46.67%]) (p < 0.05). Multiple sequence alignment of amino acid sequences relative to the sequences of the prototype strain (A/California/07/2009) and current vaccine strains showed that there were 19 mutations-eight (0.47%) in HA gene sequences and eight (0.56%) in NA gene sequences that differed from vaccine strains. These isolates shared N-glycosylation sites with the strains used in vaccines. The A/H1N1pdm2009 isolates were divided into three clades. These isolates primarily belonged to 5a.1. Additionally, a comparable grouping was observed in the NA phylogenetic tree and the HA tree. The A/H1N1pdm2009 isolates have no strong ties to any strains used in influenza vaccines. The current findings highlight the necessity to confirm the importance of these alterations and regularly check the effectiveness of vaccines considering new variants.
Additional file: Additional Table S1.
ACKNOWLEDGMENTS
None.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript and/or in the supplementary files.
ETHICS STATEMENT
The study was approved by the Institutional Review Board (IRB), University Hospital, with reference no. 20/5522/IRB.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Umuhoza T, Bulimo WD, Oyugi J, Musabyimana JP, Kinengyere AA, Mancuso JD. Prevalence of human respiratory syncytial virus, parainfluenza and adenoviruses in East Africa Community partner states of Kenya, Tanzania, and Uganda: A systematic review and meta-analysis (2007-2020). PloS one. 2021;16(4):e0249992.
Crossref - Krammer F, Smith GJD, Fouchier RAM, et al. Influenza. Nat Rev Dis Primers. 2018;4(1):3.
Crossref - Noda T. Native morphology of influenza virions. Front Microbiol. 2012;2:269.
Crossref - Skelton RM, Huber VC. Comparing influenza virus biology for understanding influenza D virus. Viruses. 2022;14(5):1036.
Crossref - Sautto GA, Kirchenbaum GA, Ross TM. Towards a universal influenza vaccine: different approaches for one goal. Virol J. 2018;15(1):17.
Crossref - Sriwilaijaroen N, Suzuki Y. Molecular basis of the structure and function of H1 hemagglutinin of influenza virus. Proc Jpn Acad Ser B Phys Biol Sci. 2012;88(6):226-249.
Crossref - Ma L, Zheng H, Ke X, et al. Mutual antagonism of mouse-adaptation mutations in HA and PA proteins on H9N2 virus replication. Virol Sin. 2024;39(1):56-70.
Crossref - Brussow H. The beginning and ending of a respiratory viral pandemic-lessons from the Spanish flu. Microb Biotechnol. 2022;15(5):1301-1317.
Crossref - Al Hajjar S, McIntosh K. The first influenza pandemic of the 21st century. Ann Saudi Med. 2010;30(1):1-10.
Crossref - Lu QC, Zhang TY, Bundhun PK, Chen C. One “misunderstood” health issue: demonstrating and communicating the safety of influenza a vaccination in pregnancy: a systematic review and meta-analysis. BMC Public Health. 2021;21(1):703.
Crossref - Xu D, Chen L, Ji L, Yan W. Genetic characterization of influenza A (H1N1) pdm09 virus in 2023 in Huzhou, China. J Clin Virol Plus. 2024;4(2):100178.
Crossref - Meningher T, Hindiyeh M, Regev L, Sherbany H, Mendelson E, Mandelboim M. Relationships between A (H1N1) pdm09 influenza infection and infections with other respiratory viruses. Influenza and other Respir Viruses. 2014;8(4):422-430.
Crossref - Naeem A, Elbakkouri K, Alfaiz A, et al. Antigenic drift of hemagglutinin and neuraminidase in seasonal H1N1 influenza viruses from Saudi Arabia in 2014 to 2015. J Med Virol. 2020;92(1):3016-3027.
Crossref - Althaqafi A, Farahat F, Alsaedi A, et al. Molecular detection of influenza A and B viruses in four consecutive influenza seasons 2015-16 to 2018-19 in a tertiary center in Western Saudi Arabia. J Epidemiol Glob Health. 2021;11(2):208-215.
Crossref - Dudin GA, Aziz IM, Alzayed RM, et al. Genetic diversity and evolutionary kinetics of influenza A virus H3N2 subtypes circulating in Riyadh, Saudi Arabia. Vaccines. 2023;11(3):702.
Crossref - El-Kafrawy SA, Alsayed SM, Faizo AA, et al. Genetic diversity and molecular analysis of human influenza virus among pilgrims during Hajj. Heliyon. 2024;10(1):e23027.
Crossref - Al-Sharif HAA, Molecular Identification and Genetic Diversity of Respiratory Viruses Isolated from Patients Attending King Abdulaziz University Hospital: King Abdulaziz University Jeddah; 2021 https://platform.almanhal.com/Files/4/235793. Accessed May 12th, 2023.
- Hakami AR, Alshahrani AJ, Alshehri OA, Saif A, Alshehri AA. Distribution of influenza A and B antibodies and correlation with ABO/Rh blood grouping. Int J Res Med Sci. 2022;10(12):2724-2730.
Crossref - Dandachi I, Alrezaihi A, Amin D, et al. Molecular surveillance of influenza A virus in Saudi Arabia: whole-genome sequencing and metagenomic approaches. Microbiology Spectrum. 2024;12(8):e00665-00624.
Crossref - WHO CC. WHO information for the molecular detection of influenza viruses. World Health Organisation. 2017. Accessed May 12th, 2023.
- Gupta R, Jung E, Brunak S. Prediction of N-glycosylation sites in human proteins. 2004. https://services.healthtech.dtu.dk/services/NetNGlyc-1.0/. Accessed May 12th, 2023.
- Julenius K, Molgaard A, Gupta R, Brunak S. Prediction, conservation analysis, and structural characterization of mammalian mucin-type O-glycosylation sites. Glycobiology. 2005;15(2):153-164.
Crossref - Kumar S, Stecher G, Tamura K. MEGA7: molecular evolutionary genetics analysis version 7.0 for bigger datasets. Mol Biol Evol. 2016;33(7):1870-1874.
Crossref - WHO. WHO Regional Office for Europe guidance for influenza surveillance in humans. 2009. Accessed May 12th, 2023.
- Beaute J, Zucs P, Korsun N, et al. Age-specific differences in influenza virus type and subtype distribution in the 2012/2013 season in 12 European countries. Epidemiol Infect. 2015;143(14):2950-2958.
Crossref - Alshiban NM, Aleyiydi MS, Nassar MS, et al. Epidemiologic and clinical updates on viral infections in Saudi Arabia. Saudi Pharm J. 2024;32(7):102126.
Crossref - Low ZY, Wong KH, Yip AJW, Choo WS. The convergent evolution of influenza A virus: Implications, therapeutic strategies and what we need to know. Curr Res Microb Sci. 2023;5:100202.
Crossref - Cobbin JCA, Alfelali M, Barasheed O, et al. Multiple sources of genetic diversity of influenza A viruses during the Hajj. J Virol. 2017;91(11):e00096-00017.
Crossref - Elhakim M, Rasooly MH, Fahim M, et al. Epidemiology of severe cases of influenza and other acute respiratory infections in the Eastern Mediterranean Region, July 2016 to June 2018. J Infect Public Health. 2020;13(3):423-429.
Crossref - Belucci TR, Marra AR, Edmond MB, et al. Evaluation of Influenza A H1N1 infection and antiviral utilization in a tertiary care hospital. BMC Infect Dis. 2018;18(1):579.
Crossref - Yan Y, Ou J, Zhao S, et al. Characterization of influenza A and B viruses circulating in southern China during the 2017-2018 season. Front Microbiol. 2020;11:1079.
Crossref - Toure CT, Fall A, Andriamandimby SF, et al. Epidemiology and Molecular Analyses of Influenza B Viruses in Senegal from 2010 to 2019. Viruses. 2022;14(5):1063.
Crossref - Ramos AP, Herrera BA, Ramirez OV, et al. Molecular and phylogenetic analysis of influenza A H1N1 pandemic viruses in Cuba, May 2009 to August 2010. Int J Infect Dis. 2013;17(7):e565-e567.
Crossref - Sharma V, Sharma M, Dhull D, Kaushik S, Kaushik S. Phylogenetic analysis of the hemagglutinin gene of influenza A (H1N1) pdm09 and A (H3N2) virus isolates from Haryana, India. Virusdisease. 2019;30(3):336-343.
Crossref - Caton AJ, Brownlee GG, Yewdell JW, Gerhard W. The antigenic structure of the influenza virus A/PR/8/34 hemagglutinin (H1 subtype). Cell. 1982;31(2 Pt 1):417-427.
Crossref - Samal SK. Structural vaccinology approaches to enhance efficacy, stability, and delivery of protective antigens. Reverse Vaccinology. 2024:217-235.
Crossref - Ray R, Dos Santos G, Buck PO, et al. A review of the value of quadrivalent influenza vaccines and their potential contribution to influenza control. Hum Vaccin Immunother. 2017;13(7):1640-1652.
Crossref - Grohskopf LA, Sokolow LZ, Broder KR, Walter EB, Fry AM, Jernigan DB. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices-United States, 2018-19 influenza season. MMWR Recommendations and Reports. 2018;67(3):1-20.
Crossref - Incalzi RA, Consoli A, Lopalco P, et al. Influenza vaccination for elderly, vulnerable and high-risk subjects: a narrative review and expert opinion. Intern Emerg Med. 2024;19(3):619-640.
Crossref - Khan R, Ahmed A, Zeitounie R, Khandekar R. Impact of influenza vaccine in reduction of incidence and severity of influenza-like illness. East Mediterr Health J. 2021;27(9):884-891.
Crossref - Lin Y, Wharton SA, Whittaker L, et al. The characteristics and antigenic properties of recently emerged subclade 3C.3a and 3C.2a human influenza A(H3N2) viruses passaged in MDCK cells. Influenza other Respir Viruses. 2017;11(3):263-274.
Crossref - Gass Jr JD, Dusek RJ, Hall JS, et al. Global dissemination of Influenza A virus is driven by wild bird migration through arctic and subarctic zones. Mol Ecol. 2023;32(1):198-213.
Crossref - Bruno A, Goni N, Cristina J. Spatial, temporal and evolutionary insight into seasonal epidemic Influenza A virus strains near the equatorial line: The case of Ecuador. Virus Res. 2023;326:199051.
Crossref - Wei C-J, Boyington JC, Dai K, et al. Cross-neutralization of 1918 and 2009 influenza viruses: role of glycans in viral evolution and vaccine design. Sci Transl Med. 2010;2(24):24ra21-24ra21.
Crossref - Sun S, Wang Q, Zhao F, Chen W, Li Z. Glycosylation site alteration in the evolution of influenza A (H1N1) viruses. PloS one. 2011;6(7):e22844.
Crossref - Kim P, Jang YH, Kwon SB, Lee CM, Han G, Seong BL. Glycosylation of hemagglutinin and neuraminidase of influenza a virus as signature for ecological spillover and adaptation among influenza reservoirs. Viruses. 2018;10(4):183.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.