

ISSN: 0973-7510
E-ISSN: 2581-690X
The aim of this study was to detect bacterial infection of: Chlamydia trachomatis, Ureaplasma spp. and Mycoplasma, from Saudi women samples. Samples were 100 from pregnant women attending the obstetrics and Gynecology clinic at Alymamah Hospital, Riyadh, Saudi Arabia during March 2013 to March 2014. DNA was successfully amplified from 56 samples. The results of this study indicated more reliable method which detected Chlamydia trachomatis, Ureaplasma spp. and Mycoplasma which caused vaginitis in lower genital, showed high frequency of both Mycoplasma spp (44.6%) and Ureaplasma spp (30.4%) infection among Saudi pregnant women. Association of Mycoplasma spp, Ureaplasma spp, and C. trachomatis has been observed but no association was observed between M. hominis, M. genitalium and U.urealyticum.
Chlamydia, Mycoplasma; Ureaplasma; Vaginitis.
Infection screening of pregnant women before 37 weeks, between conception and birth may help decrease preterm birth and low birth weight and over growth of bacterial species normally present in the vagina along with anaerobic bacteria cause the disease. (Hillier et al., 1993) .M. genitalium genome very small comprises 580 Kbp, with a capacity to encode only 482 genes. (Fraser et al., 1995). (Antonio et al., 1999). and (May et al., 1999). Though, M. genitalium genome being so small it is capable to cause the most frequently reported like pelvic inflammatory disease (PID). (Glass et al., 2006). Mycoplasma hominis is an opportunistic human mycoplasma. Two pathogenic human species, M. genitalium and Ureaplasma parvum, reside within the same natural niche as M. hominis: the urogenital tract. These three species have overlapping, but distinct, pathogenic roles. (Pereyre et al.,2009). Mycoplasma genitalium is well established as a cause of urethritis and has also been associated with cervicitis, endometritis and pelvic infection. (Ross et al.,2009). To estimate the accuracy of the clinical diagnosis of the three most common causes of acute vulvovaginal symptoms (bacterial vaginosis, candidiasis vaginitis, and trichomoniasis vaginalis) using a traditional, standardized clinical diagnostic protocol compared with a DNA probe laboratory standard had been reported by (Lowe et al.,2009). The prevalence of M. genitalium and C. trachomatis were 2.5% and 2.8%, respectively. The M. genitalium was strongly associated with post-termination pelvic inflammatory disease. The increased risk for pelvic inflammatory disease associated with M. genitalium infection after termination of pregnancy suggests a causal relationship. (Bjartling, et al., 2010). Mycoplasma hominis and Ureaplasma urealyticum has historically been the subject of attention, but Mycoplasma genitalis which causes male urethritis in addition to colonizing the female genital tract and the division of Ureaplasma into two species, urealyticum and parvum, has also added new taxonomic clarity . (Larsen and Hwang 2010). Mycoplasma genitalium is a sexually transmitted organism associated with non-gonococcal urethritis in men and several inflammatory reproductive tract syndromes in women such as cervicitis, pelvic inflammatory disease, and infertility. There was evidence for an association of M. genitalium with endometritis and pelvic inflammatory disease (PID), but additional studies are necessary to confirm this. The evidence as to whether M. genitalium can cause adverse pregnancy outcomes such as preterm labor is conflicting. But the authors of some studies on M. genitalium as a cause of infertility have reported this association. These species are very difficult to culture; thus, nucleic acid amplification testing is the only method available for M. genitalium detection (Cazanave et al. 2012) and (Sena et al., 2012). Bacterial vaginitis correlates to a decrease or loss of the normally present protective lactobacilli that helps in maintaining vaginal acidic pH through the metabolism of glucose- glycogen. Ljubomir et al.,2014). and (Mirmonsef et al.,2014). Mycoplasma genitalium is a sexually transmitted organism commonly treated with azithromycin. However, macrolide resistance has been reported and is associated with point mutations in the 23S rRNA gene. (Touati, et al., 2014). In a study of mycoplasma associated with trichomoniasis, vaginal infection, mycoplasma was found almost exclusively in women infected with sexually transmitted pathogen Trichomonas vaginalis, but rarely observed in women with no diagnosed disease. (Fettweis, et al., 2014). PCR technology is widely used in the diagnoses of bacterial infection such as polyarthritis with axial involvement in a young female and for acute lymphoblastic leukemia.( Balsat et al., 2014). The objectives of the present study are to detect bacterial species causing birth before the time of delivery so that it may minimize consequences of low birth weight and subsequent occurrences of the disease. The objectives include also to established a reliable PCR based detection of bacterial infectious for routinely application, both symptomatic and asymptomatic women with pregnancy.
The study population was randomly sampled in duplicate from hundred pregnant women visiting ‘Al Yamamah’ hospital in Riyadh, Saudi Arabia, who Showed both symptomatic and asymptomatic vaginitis and had no antibiotic treatment for 2 months before the date of examination. The study lasted over a period of a year (March 2013–March 2014). The samples were collected by the nurses in obstetrics and Gynecology departments. A written consent was obtained from each of the study participants.
The protective mucous membrane on the exterior of the cervix was first wiped of exudate, a swab was inserted into the endocervical canal, passing the squamo-columnar junction, to permit the acquisition of columnar epithelial cells which are the main reservoir of the organism, firmly rotated and then withdrawn. The swabs containing the samples were stored in ice and later stored in -20 freezers.
Data collection
An interview questionnaire for clinical and obstetric history was delivered. Data included age, first delivery, previous abortion, use of contraceptives, date and time of sample collection and symptoms of lower genital tract infection (bacterial vaginitis.
DNA Extraction
Total genomic DNA was extracted by using DNA Mini Kit (Qiagen, USA) following the manufacturer’s instructions. Using a fluorometer (Hoefer DyNA Quant 200; Pharmacia Biotech, Piscatawaym, N.J.) the quantity and quality of the DNA was determined. DNA was also run on a 1% agarose gel to determine the consistency and purity. The stock DNA samples were diluted with sterile TE buffer to make a working solution of 10 Kg ml–1 for use in PCR analysis.
Polymerase chain reaction
Six specific primers for the detection of six different microorganisms (Chlamydia trachomatis, Ureaplasma spp, U. urealyticum, Mycoplasma spp., M. hominis, and M. genitalium) were used for PCR amplification (Table 1). The specific primer pair used for the detection of C. trachomatis amplified its outer membrane protein A (ompA) gene. To detect Ureaplasma spp specific 16S rRNA primer pairs were used and for U. urealyticum specific primer pair targeting multiple banded antigens (MBA) in upstream region was used. For Mycoplasma spp primer pair for 16S rRNA for universal region was used. Similary for M. hominis primer pair specific for 16S RNA of M. hominis, that amplified 334 bp of amplicon, were used. The primer pair for M. genitalium amplified 281 bp adhesion gene fragments. All the six primer pairs were dissolved in sterilized distilled water at a concentration of 10 pmol/µl. Amplification reactions were performed in volumes of 25 µl using ‘GoTaq Green Master Mix 2X (Promega, USA). It is optimized for PCR reactions. In each reaction 50 Kg of DNA samples were used along with 20 pmol/ µl of primer. PCR amplification was performed in Eppendorf Master Cycler Gradient PCR machine. The following PCR program was used: (1) one cycle for 10 min at 95oC; (2) 35-45 cycles at 95oC for 1 min, 52-62.9oC (depending on the Tm of the primers) for 1.5 min and 72oC for 1 min; (3) one cycle for 10 min at 72oC, followed by a soaking at 4oC.
Table (1):
Specific primer pairs used in this study for detection of Chlamydia trachomatis, Ureaplasma spp. and Mycoplasma, from Saudi women samples.
| organism | Primer 5-3 | Annealing Temperature/°c | Amplicon size | Reference |
|---|---|---|---|---|
| Mycoplasma spp | F1: GGGAGCAAACAGGATTAGATACCCT | 52 | 287 bp | Choppa et al., 1998 |
| R2:TGCACCATCTGTCACTCTGTTAACCTC | ||||
|
M. genitalium |
F: AGTTGATGAAACCTTAACCCCTTGG | 62.9 | 281bp | Jensen et al., 1991 |
| R: CCGTTGAGGGGTTTTCCATTTTTGC | ||||
| M. hominis | F: CAATGGCTAATGCCGGATACGC | 54.5 | 334 bp | Blanchard et al., 1993 |
| R: GGTACCGTCAGTCTGCAAT | ||||
| C. trachomatis | F: ATGAAAAAACTCTTGAAATCG | 62 | 1100 bp | Jurstrand et al., 2010 |
| R: ACTGTAACTGCGTATTTGTCTG | ||||
| Ureaplasma spp | F: GGGTGCGACGTATCAGATAGTTG | 58 | 84 bp | Choppa et al., 1998 |
| R: TGTGGCTGTTCTACCTCTCAGTACA | ||||
| U. urealyticum | F: GTATTTGCAATCTTTATATGTTTTCG | 55 | 476 bp | Kong et al., 2000 |
| R: TTTGTTGTTGCGTTTTCT |
Electrophoresis
PCR products were separated by electrophoresis according to their molecular weight on 1.5% (w/w) agarose gels submerged in 1x TBE buffer and then stained with ethidium bromide (10 mg ml–1) solution for 20 min. The DNAs were visualized on a UV trans illuminator and documented The amplified fragment was estimated by running 100 pb Ladder (Bio Rad) in the gel as standard size marker.
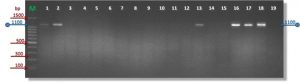
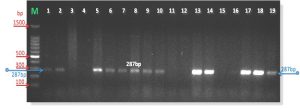
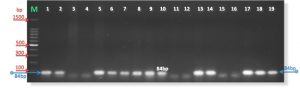
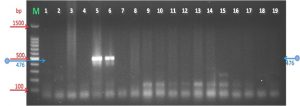
DNA was successfully amplified from 56 samples out of 100 samples (See fig. 1). Eleven out of 56 samples (19.7%) were detected for C. trachomatis with 1100 bp (See fig. 2). Twenty five out of 56 samples (44.6%) for Mycoplasma spp were positive with amplicon 287 bp (see fig 3).
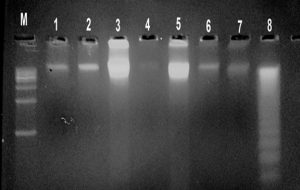 M: is marker 1500bp Lanes 1—8: are DNA isolated from Chlamydia trachomatis, Ureaplasma spp. and Mycoplasma which was used for PCR template
M: is marker 1500bp Lanes 1—8: are DNA isolated from Chlamydia trachomatis, Ureaplasma spp. and Mycoplasma which was used for PCR templateFig. 1. DNA isolated from Chlamydia trachomatis, Ureaplasma spp. and Mycoplasma which was used for PCR template
 F: ATGAAAAAACTCTTGAAATCG
F: ATGAAAAAACTCTTGAAATCGR: ACTGTAACTGCGTATTTGTCTG
M: is marker 1500bp
Lanes 1—19: are samples of PCR product after gel electrophoresis
Fig. 2. PCR amplification products of Chlamydia trachomatis (1100 bp with primers)
F: GGGAGCAAACAGGATTAGATACCCT
R: TGCACCATCTGTCACTCTGTTAACCTC
M: is marker 1500bp
Lanes 1—19: are samples of PCR product after gel electrophoresis
Fig. 3. PCR amplification products of Mycoplasma spp (287 bp) with primers
By using specific primer targeting MBA genes, two were positive out of 56 samples for M. hominis (3.6%) with amplified fragment of size 334 bp (See fig. 4). While one (1.8%) for M. genitalium with 281 bp (See fig. 5). Six specific taxon-directed 16S rRNA gene primer pairs were used in PCR assay to detect the presence of vaginal bacteria (see table 1). The Prevalence of bacterial vaginitis infection according to the age of the patients (See fig.6).
F: CAATGGCTAATGCCGGATACGC
R: GGTACCGTCAGTCTGCAAT
M: is marker 1500bp
Lanes 1—19: are samples of PCR product after gel electrophoresis
Fig. 4. PCR amplification products of M. hominis(334bp) with primes
F: AGTTGATGAAACCTTAACCCCTTGG
R: CCGTTGAGGGGTTTTCCATTTTTGC
M: is marker 1500bp
Lanes: 20—38: are samples of PCR product after r gel electrophoresis
Fig. 5. PCR amplification products of M. genitalium(281bp) with primers
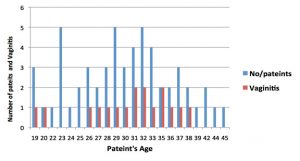
Fig. 6. Prevalence of bacterial vaginitis according to patient’s age, and number of individuals
Mixed infection was observed in this study which may be due to the association of Mycoplasma spp, Ureaplasma spp, and C. trachomatis. No association was observed between M. hominis, M. genitalium and U. urealyticum. These results indicated more reliable method which detected bacteria causing vaginitis in lower genital. The results of this study showed high frequency of both Mycoplasma spp (44.6%) and Ureaplasma spp (30.4%) infection among Saudi pregnant women. Bacterial vaginitis correlates to a decrease or loss of the normally present protective lactobacilli that helps in maintaining vaginal acidic pH through metabolism of glucose- glycogen that produce lactic acid. Hydrogen peroxide (H2O2) produced by some Lactobacilli spp also helps in maintaining a low pH, which inhibits bacterial over growth. Thus a considerable loss of these protective lactobacilli may lead to vaginitis that could further lead to premature rupture of membranes, HIV, PID, preterm birth and low birth weight (May A. D. et al., 1993) and (Antonio et al., 1999). Diagnoses of vaginitis using traditional method based on clinical symptoms, microscopy, amine odor test and pH test of vaginal fluid, about two third of the cases of bacterial vaginitis were misdiagnosed in women with vaginal complaints. Furthermore, infection may be asymptomatic as high as 50% of cases (Lowe et al., 2009). Cross-sectional samples from rural South Africa women were tested for Mycoplasma genitalium. Overall, 10.8% of women were infected with M. genitalium either in the vagina or in the rectum. (Hay B et al., 2015). We studied six specific primers for the detection of six different microorganisms (Chlamydia trachomatis, Ureaplasma spp, U. urealyticum, Mycoplasma spp., M. hominis, and M. genitalium) by using PCR amplification. Their specificity and accuracy were very high and reliable. Lower genital tract infections are the main cause of preterm birth. Infants born preterm are with low birth weight and often develop immediate complications that require significant long term health-care resources. Therefore, we propose screening and treatment of such infections as a preventive measure. Preterm birth is a major public health problem in maternity homes and hospitals.
This study was conducted to determine if PCR can be reliable and useful to detect and quantify several of the lower genital tract bacteria that cause bacterial vaginitis. The results showed that PCR can be reliable to detect Chlamydia trachomatis, Ureaplasma spp, U. urealyticum, Mycoplasma spp., M. hominis, and M. genitalium in lower genital tract samples. The results of this study showed high frequency of both Mycoplasma spp (44.6%) and Ureaplasma spp (30.4%) infection among Saudi pregnant women. Mixed infection has also been observed which may be due to the association of Mycoplasma spp, Ureaplasma spp, and C. trachomatis. No association was observed between M. hominis, M. genitalium and U. urealyticum. PCR assays have advantage over the two most commonly used methods for detecting lower genital tract bacteria; the Amsel criteria and the Gram stain, in that it is more sensitive. In conclusion, this study indicates that it is feasible to use PCR to detect and quantify the numbers of bacterial related vaginitis.
ACKNOWLEDGMENTS
This project was supported by King Saud University, deanship of Scientific Research, College of Science Research Center. I would like to express my sincere gratitude and deep gratefulness to this Deanship and to all my colleagues for their advice
- Hillier, S.L., Krohn, M.A., Rabe, L.K., Klebano¡, S.J. and Eschenbach, D.A: The normal vaginal flora, H2O2-producing lactobacilli, and bacterial vaginosis in pregnant women. Clin. Infect. Disea. 1993; 16, Suppl 4, S273-S281.
- Fraser CM, Gocayne JD, White O, Adams MD, Clayton RA, Fleischmann RD, Bult CJ, Kerlavage AR, Sutton G, Kelley JM, Fritchman RD, Weidman JF, Small KV, Sandusky M, Fuhrmann J, Nguyen D, Utterback TR, Saudek DM, Phillips CA, Merrick JM, Tomb JF, Dougherty BA, Bott KF, Hu PC, Lucier TS, Peterson SN,Smith HO, Hutchison CA 3rd, Venter JC: The minimal gene complement of Mycoplasma genitalium; Scien 1995; 270, 5235, 397-403.
- Antonio MA, Hawes SE, Hillier SL: The identification of vaginal Lactobacillus species and the demographic and microbiologic characteristics of women colonized by these species. J. Infec. Disea. 1999; 180, 6, 1950-1956.
- May A. D. Antonio, Stephen E. Hawes, and Sharon L. Hillier: The Identification of Vaginal Lactobacillus Species and the Demographic and Microbiologic Characteristics of Women Colonized by these Species. J. Infect. Disea, 1999; 180, 6, 1950–1956.
- Glass JI, Assad-Garcia N, Alperovich N, Yooseph S, Lewis MR, Maruf M, Hutchison CA 3rd, Smith HO, Venter JC: Essential genes of a minimal bacterium. Proc. Natl. Acad .Sci, 2006; 103, 2, 425–430.
- Pereyre S, Sirand-Pugnet P, Beven L, Charron A, Renaudin H, Barre A, Avenaud P, Jacob D, Couloux A, Barbe V, de Daruvar A, Blanchard A, Bébéar C: Life on arginine for Mycoplasma hominis: clues from its minimal genome and comparison with other human Urogenitalmycoplasmas 2009; J.PLoS.Genet. 5,10, ee1000677,doi:10.1371/journal.pgen.1000677.
- Ross JD, Brown L, Saunders P, Alexander S. Mycoplasma genitalium in asymptomatic patients: implications for screening. Sex Transm Infect, 2009; 85, 6, 436-437.
- Lowe NK, Neal JL, Ryan-Wenger NA: Accuracy of the clinical diagnosis of vaginitis compared to a DNA probe laboratory standard. Obstet. Gynec. 2009; 113, 1, 89–95.
- Bjartling C, Osser S, Persson K: The association between Mycoplasma genitalium and pelvic inflammatory disease after termination of pregnancy. Briti. j. obstet. Gynaeco. 2010; 364, 117, 361-364.
- Larsen B, Hwang J: Mycoplasma, Ureaplasma, and adverse pregnancy outcomes: a fresh look. Infect. Disea. obstet. Gyneco. 2010; ID 521921, 7 pages
- Cazanave C, Manhart LE, Bébéar C: Mycoplasma genitalium, an emerging sexually transmitted pathogen. Medici. Malad. Infect. 2012; 42, 9, 381-3892.
- Sena AC, Lensing S, Rompalo A, Taylor SN, Martin DH, Lopez LM, Lee JY, Schwebke JR. Chlamydia trachomatis, Mycoplasma genitalium, and Trichomonas vaginalis infections in men with nongonococcal urethritis: predictors and persistence after therapy. J. Infect Dis, 2012; 206, 3, 357-365.
- Ljubomir Petricevic, Konrad J. Domig, Franz Josef Nierscher, Michael J. Sandhofer, Maria Fidesser, Iris Krondorfer, Peter Husslein, Wolfgang Kneifel & Herbert Kiss: Characterisation of the vaginal Lactobacillus microbiota associated with preterm delivery. Scienti. Repor. 2014; 4, 5136, doi: 10.1038/srep05136.
- Mirmonsef Paria, Anna L. Hotton, Douglas Gilbert, Derick Burgad, Alan Landay, Kathleen M. Weber,Mardge Cohen,,Jacques Ravel, Gregory T. Spea,Anna L. Hotton, Douglas, Gilbert, Derick Burgad, Alan Landay, Kathleen M. Weber, Mardge Cohen, Jacques Ravel, Gregory T. Spear: Free Glycogen in Vaginal Fluids Is Associated With Lactobacillus Colonization and Low Vaginal pH.2014; Briti. j. obstet. Gynaeco. 9, 7, e102467. doi:10.1371/0102467.
- Touati A, Peuchant O, Jensen JS, Bébéar C, Pereyre S: Direct detection of macrolide resistance in Mycoplasma genitaliumisolates from clinical specimens from France by use of real-time PCR and melting curve analysis. J. Clin. Microbio. 2014; 52, 5, 1549-1555.
- Fettweis JM, Serrano MG, Huang B, Brooks JP, Glascock AL, Sheth NU, Vaginal Microbiome Consortium, Strauss JF 3rd, Jefferson KK, Buck GA: An emerging Mycoplasma associated with trichomoniasis, vaginal infection and disease. Publi. Libra. Scien, 2014; 9, 10, e110943. doi: 10.1371/.0110943.
- Balsat M, Galicier L, Wargnier A, Pereyre S, Itzykson R, Zouakh M, Bébéar C, Boissel N: Diagnosis of Ureaplasma urealyticumseptic polyarthritis by PCR assay and electrospray ionization mass spectrometry in a patient with acute lymphoblastic leukemia.; J. Clin Microbio, 2014; 52, 9, 3456-34568.
- Hay B, Dubbink JH, Ouburg S, Le Roy C, Pereyre S, Van der Eem L, Morré SA, Bébéar C, Peters RP: Prevalence and macrolide resistance of Mycoplasma genitaliumin South Africa. Women. Sex. Transm.Dis, 2015; 42, 3, 140-242.
- Ladefoged SA, Christiansen G: Physical and genetic mapping of the genomes of five Mycoplasma hominisstrains by pulsed-field gel electrophoresis. J. Bacteriol, 1992; 174, 7, 2199–2207
© The Author(s) 2016. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.