


ISSN: 0973-7510
E-ISSN: 2581-690X
In rural communities, the blaNDM-1 gene in the gut microbiota may be contributing to the growing issue of antibiotic resistance. This gene enables bacteria to produce enzymes that break down antibiotics, making treatments less effective. The limited healthcare resources and frequent exposure to resistant bacteria in these areas could further amplify this problem, increasing the risk of difficult-to-treat infections among the population. The objective of this study was to evaluate the antimicrobial susceptibility of Escherichia coli [E. coli] strains isolated from healthy individuals and to assess the prevalence of blaNDM-1 gene carriage. The samples were cultured and identified as gut commensal by conventional method. Then antibiotic susceptibility test using the Kirby Bauer disc diffusion method were carried out. Carbapenem-resistant organisms were isolated, and the blaNDM-1 was identified by polymerase chain reaction. This study includes 187 Healthy participants faecal samples were obtained from people in and around the Chengalpattu area. Out of 187 samples, 110 showed E. coli growth, 63 showed Enterococci species growth, and 14 showed no growth. Among the 110 E. coli isolates, 24 (21.8%) were sensitive to all drug classes, and 86 (78.2%) were multidrug resistant. Only 8(7.27%) of the 110 E. coli tested positive for carbapenem resistance. Out of 110 E. coli isolates, only (2.7%) had the blaNDM-1 gene. This study discovered that rural communities that are unlikely to be subjected to obvious antibiotic pressure had a high incidence of MDR microorganism faecal carriage. Finding resistance genes in commensal bacteria is alarming. This has the ability to spread and emerge in the environment.
E. coli, blaNDM-1 Gene, Multi-drug Resistant, Carbapenem Resistant
In recent years, research on the diversity and purpose of the gut microbiota has considerably grown as a result of improvements in bacterial genome sequencing technologies. However, regarding species of bacteria and relative quantities, each person’s gut microbiota is distinct.1 The phylum Firmicutes and Bacteroides comprise 90% of the gut microbiota in adulthood.2 Therefore, it is acknowledged that the E. coli species that belong to the Proteobacteria phylum are not the dominant bacterial species in the human microbiota of the gut. A mere one per cent of the human intestinal microbiome is usually made up of E. coli species.3
Monitoring and effectively controlling the spread of hospital-acquired infections caused by Gram-negative bacteria resistant to carbapenems is paramount for public health.4 These infections pose a significant threat, especially when linked to major carbapenemases capable of hydrolyzing a broad range of β-lactams and carbapenems. Notably, Klebsiella pneumoniae carbapenemase (KPC), Verona integron-encoded metallo-β-lactamase (VIM), Imipenemase (IMP), Oxacillinase-48 (OXA-48), and New Delhi metallo-β-lactamase (NDM) are of particular concern due to their heightened resistance to various carbapenems. The widespread dissemination of these carbapenemases on diverse plasmids poses a challenge for control efforts. As such, it is crucial to put in place thorough strategies to stop and manage the dissemination of these infections and the linked carbapenemase enzymes.5
For many years, there has been extensive research on plasmids, which are carriers of resistance genes, commonly referred to as R-factors. The comprehension of the dissemination of antimicrobial resistance has been enhanced with the identification of more condensed and adaptable genome components like transposons and genetic cassettes, often associated with integron. These plasmids are notorious for their ability to transfer resistant genes to new species. The global health crisis is heavily influenced by two major factors – the surge of multidrug-resistant (MDR) bacterial infections and antimicrobial resistance (AMR).6 AMR affects all types of bacteria, thus it is crucial to continually monitor medication resistance profiles, ensure accurate diagnosis, and implement strict antibiotic stewardship practices. Commensal microbes, especially those in the intestines, may contain AMR genes as a result of recurrent exposure to antibiotics and certain parenteral preparations. This renders the typical commensal bacteria present in git particularly vulnerable to the appearance of AMR-producing genes.
Most MBL-producing microorganisms are also tolerant to aminoglycosides and fluoroquinolones. The international medical community has to be extremely concerned about the rising number of illnesses brought on by Enterobacteriaceae that produce carbapenemase. The ability of the majority of E. coli strains to inherit Mobile Genetic Elements, such as plasmids, through horizontal gene transfer has been found, enabling the bacteria to produce resistant infections.7 A repository for plasmids harbouring genes responsible for virulence or AMR may also exist in commensal E. coli. Conjugation results in the development of conjugative antimicrobial classes other than β-lactams, which increases multi-drug resistance (MDR) and reduces the number of available treatment alternatives.8
The rising incidence of NDM-1 enzyme-producing bacteria poses a critical public health threat, necessitating continuous surveillance to effectively track their transmission and mitigate the risks associated with metallo-beta-lactamase-mediated antibiotic resistance within communities. The main objective of this study is to investigate the antimicrobial susceptibility of E. coli isolated from healthy individuals, with a focus on identifying plasmid-borne genes associated with antimicrobial resistance, particularly the blaNDM-1 gene.
Population of interest and faecal samples
A total of 187 faecal samples that were collected from healthy villagers were included in the current investigation. This cross-sectional study was carried out at the SRM Medical College Hospital and Research Centre’s Department of Microbiology between June 2022 and January 2023. The institution’s ethical committee gave the study approval with the ethical no. 8412/IEC/2022.
Sample Size: 187 stool Samples
Sample size calculation
p = 4.4
q = 95.6
n = z²*p*q
d2
n = (1.96)2 *4.4*95.6
8.8
n = 187
They had to be in satisfactory health, be devoid of any intestinal or other issues, and not have taken any antibiotics during the previous three months. These healthy individuals were essentially picked as a criterion. The faecal samples specimens were collected in sterile, custom-made containers, which were then covered with stretch film and sealed. Immediately after, they were brought to the microbiological lab and kept maintained at
4°C until the process.
Faecal bacterial culture and characterization
The faecal samples were cultivated within an hour of the collection time. Faecal samples were cultivated on Nutrient agar and MacConkey agar media, and the agar plates were then incubated overnight at 37°C. Gram-staining and biochemical assays were used to further identify the lactose-fermenting colonies that were indicative of the E. coli bacterium. From 187 non-repetitive faecal samples collected from healthy persons who had not taken antibiotics in the three months before the collection of the faecal sample, around 110 E. coli isolates were discovered. These isolates were stored in glycerol stock medium at 20°C for use in PCR experiments and antibiotic susceptibility testing.
Assessment of microbial sensitivity to antimicrobial agents
In the research, the Kirby-Bauer disc diffusion technique was employed on Mueller-Hinton agar (MHA) to evaluate the susceptibility of E. coli isolates to antibiotics. This assessment was conducted in accordance with the guidelines set forth by the Clinical and Laboratory Standards Institute (CLSI) for the year 2022. A total of 15 antibiotics [HiMedia Laboratories Pvt. Limited, Maharashtra], spanning different antimicrobial classes, were tested. The zone sizes around the antibiotic discs were interpreted as either Sensitive (S) or Resistant (R) based on the CLSI breakpoints. The standard strain used for quality control during the antimicrobial susceptibility testing was E. coli ATCC 25922.
Assessment for detection of carbapenemase production
In AST, meropenem-resistant bacterial isolates having inhibitory zones of ≤19 mM were thought to be carbapenemase producers. Confirmatory assays for the formation of carbapenemase were also performed on these isolates.9
Validation of carbapenemase production
Modified carbapenemase inactivation-method
The modified Carbapenemase Inactivation Method (mCIM) was conducted following the guidelines outlined in the 32nd Edition M100 from CLSI.10 This method entailed exposing a bacterial suspension containing microorganisms that produce carbapenemase to a 10 µg meropenem (MRP) disc for a two-hour duration. If the tested organism produced carbapenemase, it would break down the carbapenem in the disc, while MRP would maintain its antimicrobial properties otherwise.
In this test, 1 µl of the test microorganism was combined with 2 mL of trypticase soy broth (TSB) in a vial using a non-reactive inoculating loop. The bacterial mixture was then briefly mixed for 10-15 seconds through vortexing, and a 10 gram disc of Meropenem (MRP disc, Himedia) was aseptically added to the bacterial solution. The vial was kept at room temperature and incubated at 35°C and 2°C for a duration of 4 hours and 15 minutes. Before concluding the 4 hour carbapenem inactivation phase, a mixture of the mCIM indicator bacteria (ATCC 25922 E. coli) was prepared to match a standard turbidity of 0.5 McFarland. Subsequently, this suspension was applied to the surface of a Muller Hinton Agar (MHA) plate (Himedia) using the standard technique for disc diffusion susceptibility testing.
Subsequently, the MRP disc was placed on the infected MHA plate and incubated for 18 to 24 hours at 35°C and 2°C in an open-air setting. Using a 10 µl inoculating loop, the disc was removed from the TSB bacterial solution.
Carba NP test
The procedure was performed according to the CLSI guidelines (32nd Edition M100). “A” reagent named phenol red (such as red to yellow/orange) that measures pH variations can be used to detect it. Bacteria grown on the Muller-Hinton Agar Medium (MHA) were suspended in 1.5 mL of Eppendorf tube with 100 L of 20 mM Tris buffer, and the mixture was then vortexed for 5 seconds. 100 µl of indicator solution (pH 7.8) was added to the suspension. Tube “A” contains 6 mg/mL of imipenem powder/12 mg/mL of imipenem + cilostatin injectable; tube “B” is the control. Both tubes were mixed thoroughly for 5-10 seconds until red/orange. The tubes were then incubated at 37°C for 2 hours. The test organisms were compared and the results were interpreted.
Extraction of plasmid DNA
3 milliliters of Luria-Bertani (LB) broth were inoculated with one to two separate colonies of E. coli. This mixture was then incubated under aerobic conditions at a temperature of 37°C for a duration ranging from 18 to 24 hours. The pure culture was then subjected to an additional alkaline-lysis treatment. After the extraction process, the plasmids were resuspended in Tris-EDTA (TE) buffer and preserved at a temperature of -20°C for subsequent analysis.11
Gene amplification for blaNDM-1
To target the specific carbapenemase gene, blaNDM-1, a Polymerase Chain Reaction (PCR) test was employed. The PCR reaction solution, using Thermofisher 2x Master Mix, was prepared as follows: 25 mL of the master mix, 5 mL of distilled water, 0.5 mL of both the forward and reverse primers, along with 6 mL of the purified plasmid, were separately introduced into individual amplification tubes. The PCR cycling, temperature, and timing parameters were meticulously adhered to in accordance with the manufacturer’s recommendations. The primers utilized for detecting the blaNDM-1 gene were as follows:
NDM F GGTTTGGCGATCTGGTTTTC
NDM R CGGAATGGCTCATCACGATC12
Visualization of pcr products through gel electrophoresis
The PCR products were analyzed using gel electrophoresis on a 1.5% agarose gel prepared with tris-acetate-EDTA (TAE) buffer and subsequently treated with 0.1 µl of ethidium bromide dye for staining. The controls and the samples were loaded into the well.
K. pneumoniaeATCC BAA2156 was used as a positive control and E. coli ATCC 25922 as negative control.13 The PCR products amplified 475 bp internal fragment of the gene.14
Isolation and identification
In this study of a cross-sectional nature, a total of 187 faecal samples were collected from individuals of various age groups who were in good health in the Kachadimangalam, Potheri, and Kavanur villages of Chengalpattu district. The present study involves about 81 (43%) samples were collected from Kachadimangalam village, 57 (31%) samples from Kavanur, and 49 (26%) samples from Potheri.
Gender-wise distribution showed that 116 (62%) were females and 71 (38%) were males. In Kachadimangalam, 66 (81%) were females and 17 (19%) were males. In Kavanur village, 34 (59.6%) were females and 23 (40.4%) were males. In Potheri, 18 (36.7%) were females and 31 (63.3%) were males, respectively.
In the current study population, 36 (19.2%) samples were obtained from individuals in the age group below 18 years, 74 (39.6%) individuals belonged to the age group of 19-40 years, 51 (27.2%) belonged to 41-60 years of age and 26 (14%) were above 60 years (Table). In the current investigation, 187 non-repetitive faecal samples from healthy people who had not taken antibiotics in the three months before the faecal sample collection from villages yielded 110 E. coli isolates. These 110 E. coli isolates demonstrated the normal phenotypic traits of E. coli, such as the cultural traits, on McConkey, and certain biochemical responses.
Table:
Socio-Demographic Characteristics of study participants (n = 187)
| Risk factors | Kachadimangalam Village n (%) | Potheri Village n (%) | Kavanur Village n (%) |
|---|---|---|---|
| Total = 81 | Total = 49 | Total = 57 | |
| Below 18 years | 11 (13.5) | 7 (14.2) | 18 (31.5) |
| 19-40 | 31 (38.3) | 27 (55.1) | 16 (28.1) |
| 41-60 | 23 (28.4) | 9 (18.3) | 19 (33.3) |
| Above 60 | 16 (19.8) | 6 (12.3) | 4 (7.1) |
| Sex | |||
| Male | 15 (18.5) | 31 (63.2) | 23 (40.3) |
| Female | 66 (81.5) | 18(36.8) | 34 (59.7) |
| Education level | |||
| Literate | 37 (45.7) | 21 (42.9) | 27 (47.3) |
| Illiterate | 44 (54.3) | 28 (57.1) | 30 (53.7) |
| Antibiotic awareness | |||
| Yes | 19 (23.4) | 10 (20.5) | 9 (15.8) |
| No | 62 (76.6) | 39 (79.5) | 48 (84.2) |
| Duration of antibiotic use | |||
| Prescribed | 31 (38.4) | 20 (40.8) | 24 (42.1) |
| Stopped when better | 50 (61.6) | 29 (59.2) | 33 (57.9) |
| When sick visits | |||
| Hospital | 35 (43.3) | 24 (48.9) | 26 (49.1) |
| Pharmacy | 46 (56.7) | 25 (51.1) | 27 (50.9) |
Antibiotic Resistance
The antimicrobial resistance characteristics of 110 E. coli isolates against 15 different antimicrobial agents. Among them, above 60 years were higher in ratio followed by 41-50 years, 19-40 years and below 18 years (Figure 1). Out of 110 E. coli, Female were more predominant than male (Figure 2). Among these isolates, 86 (78.2%) displayed resistance to two or more of the tested antibiotics, while 24 (21.8%) exhibited susceptibility to these antimicrobial substances. The majority of isolated E. coli showed greater antimicrobial agent resistance rates. Imipenem and meropenem showed the highest sensitivity (92.8%), followed by amikacin (67.9%) and gentamicin (57.1%). The findings of the current investigation revealed that aminoglycosides (47/110, 42.9%) had the lowest resistance rate, while lactams (82/110, 75%) and quinolones (69/110, 62.5%) and tetracyclines (61/110, 55.4%) had the greatest resistance frequency. However, the most significant level of resistance, reaching up to 75%, was noted for both ampicillin and trimethoprim/sulfamethoxazole. Following closely was the resistance rate for ceftriaxone at 73.2%, and then for cefuroxime, ceftazidime, aztreonam, and cefepime at 71.4%. Amoxicillin-clavulanate showed a resistance rate of 66.1%, while fluoroquinolones stood at 62.5%, tetracycline at 55.4%, and cefoxitin at 64%. Gentamicin exhibited a resistance rate of 42.9%, and amikacin had a lower resistance rate of 32.1%.
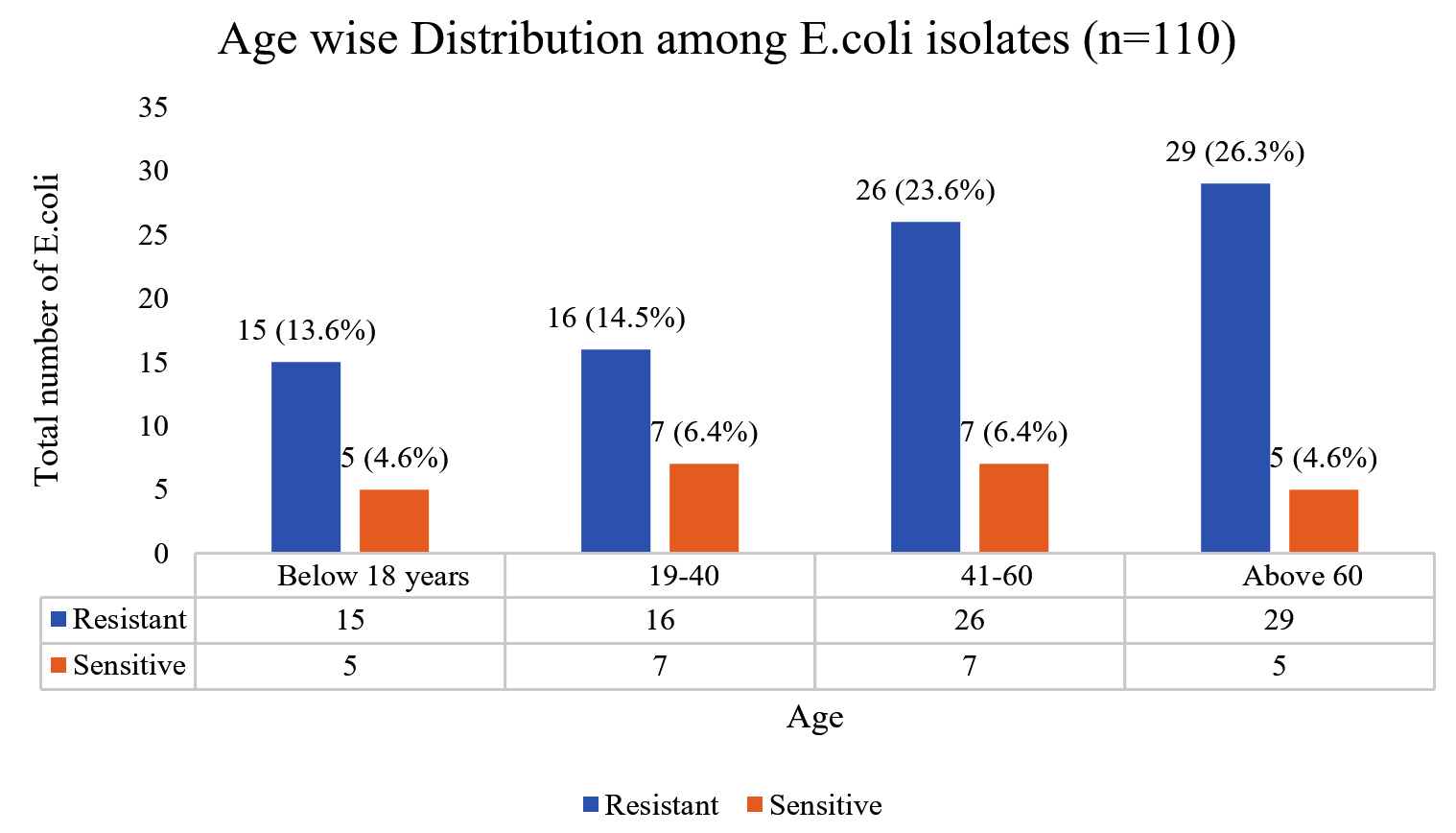
Figure 1. Age wise Distribution among E. coli isolates (n = 110)
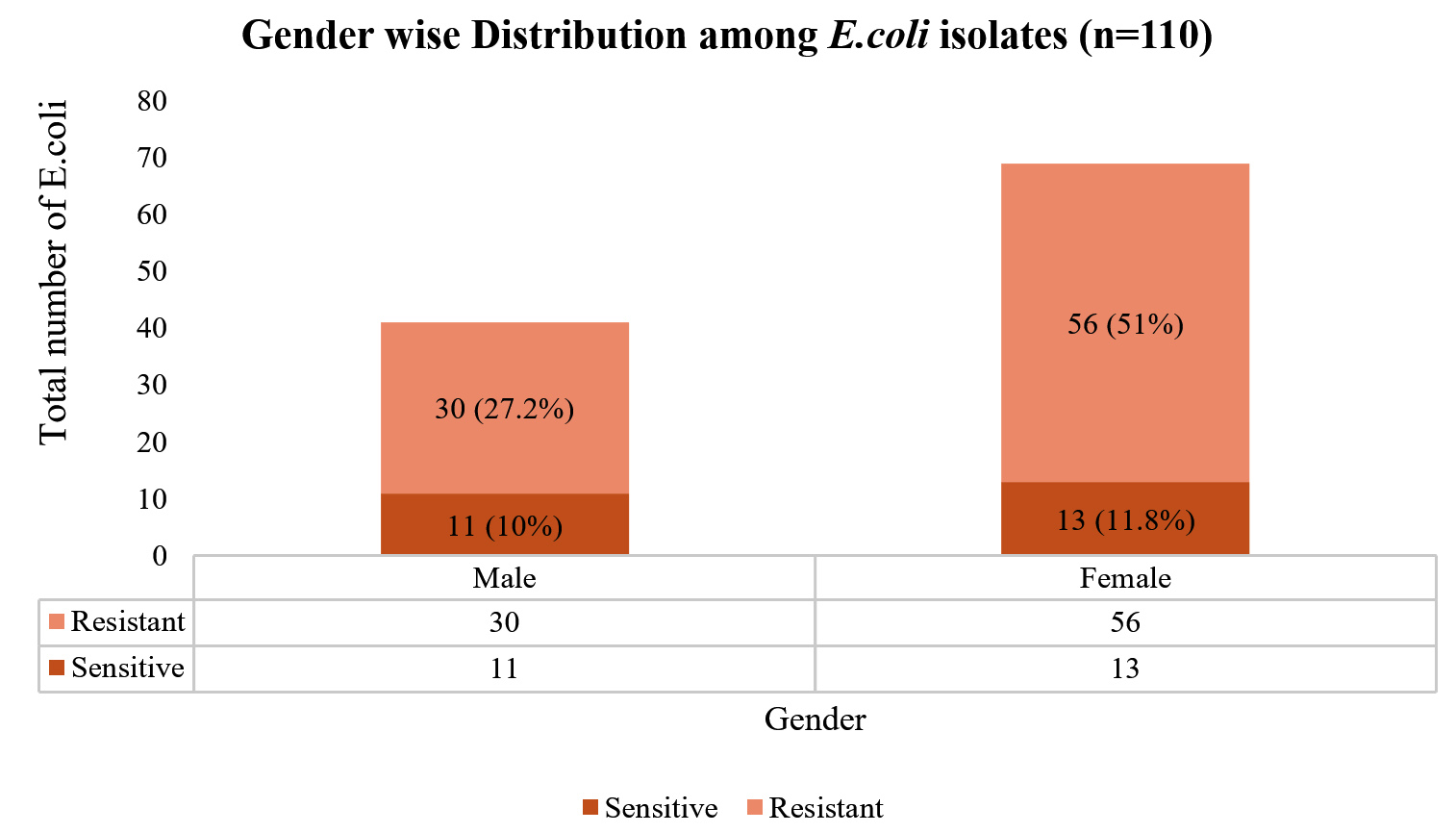
Figure 2. Gender wise Distribution among E. coli isolates (n = 110)
Molecular studies
Among the 86 isolates displaying resistance to two or more classes of antimicrobial agents, 8 (7.2%) were initially identified as potentially carbapenem-resistant and underwent a confirmatory test for the same, which were validated using mCIM and CarbaNP test. Further examination was conducted on these resistant isolates to check for the presence of MBL genes. When examining the presence of the blaNDM-1 gene, it was found that, out of the 8 carbapenem-resistant isolates, PCR detected the presence of the blaNDM-1 gene in three of them (Figure 3 and Figure 4).
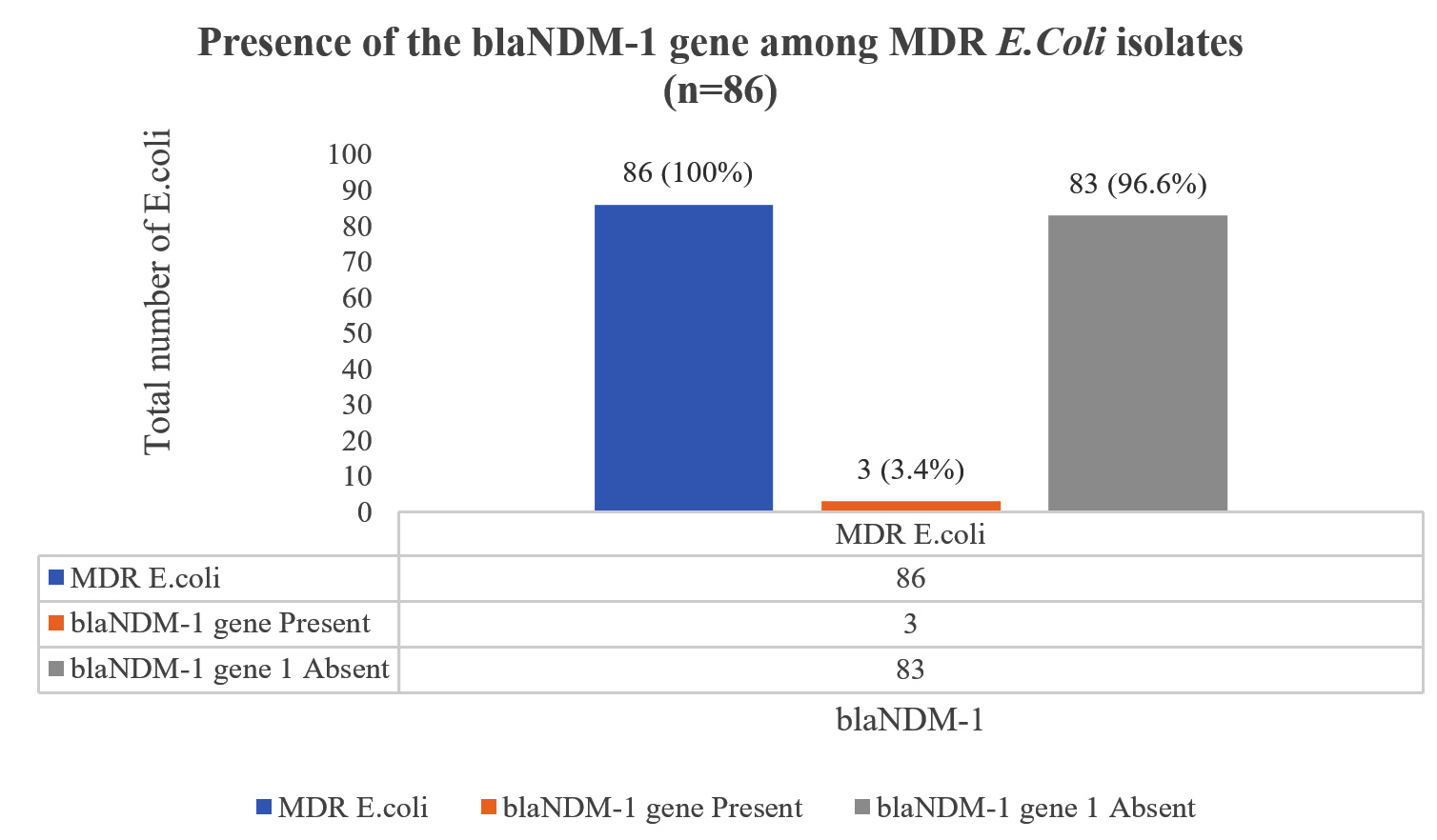
Figure 3. Presence of the blaNDM-1 gene among MDR E. coli isolates (n = 86)
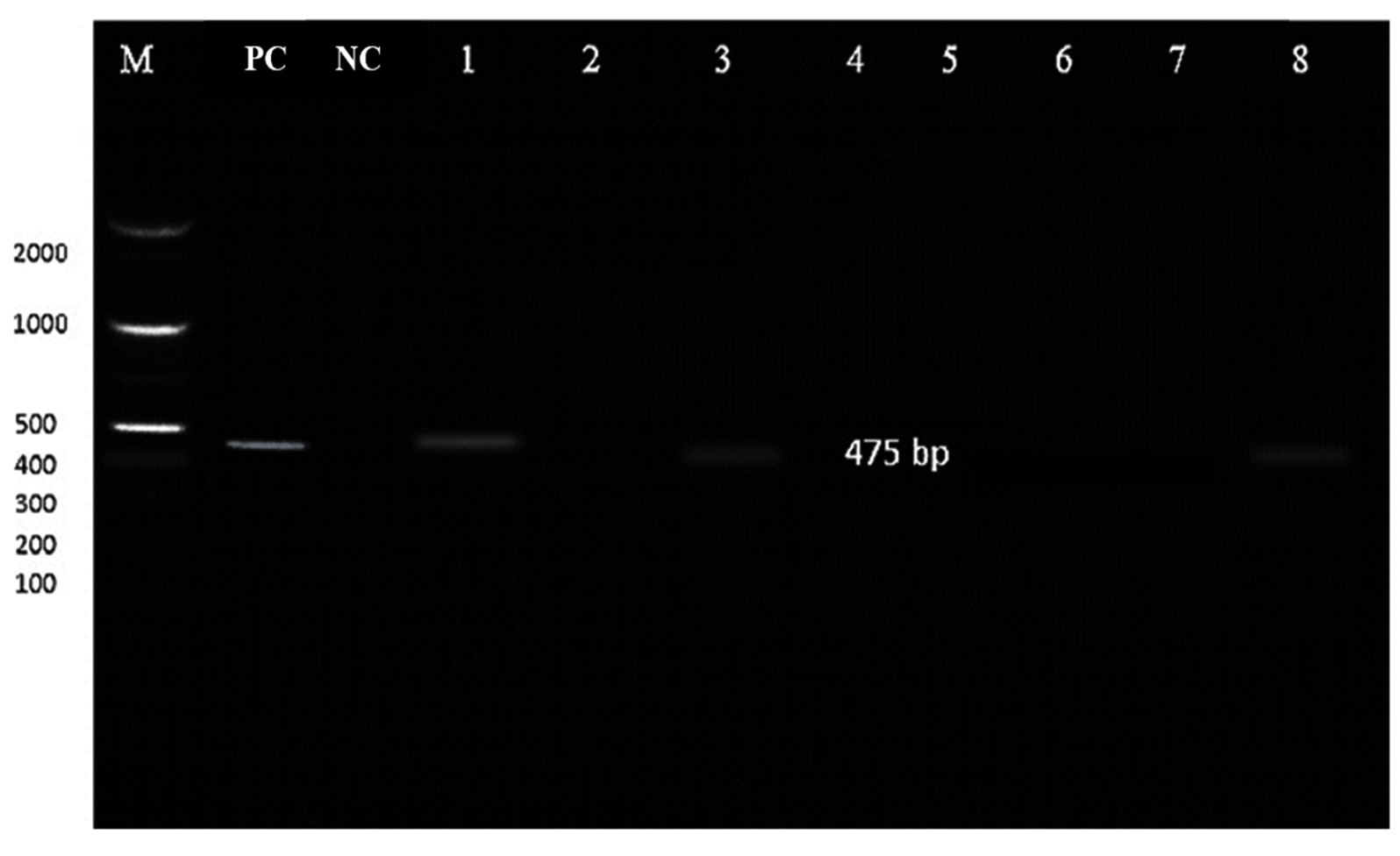
Figure 4. Gel Electrophoresis of blaNDM-1 gene in three isolates
E. coli in the gut serves as a significant source of antimicrobial resistance (AMR) genes, making a substantial impact on the effectiveness of treatments in both human and animal contexts.15 It is imperative to understand the multi-drug resistance (MDR) patterns and pathogenicity of these bacteria to mitigate risks and prevent therapeutic failures, especially in infections caused by MDR strains. Most experts attribute the rise in antimicrobial resistance to human activities, particularly the overuse and misuse of antibiotics, posing a significant public health concern, especially regarding E. coli’s inherent or acquired resistance to certain antibiotic classes.
In this study, females (62%) were more prevalent than males (38%). These findings closely mirrored a study by Antony et al., where females (67.9%) were more predominant than males (32.1%). Moreover, a significant portion of the study participants fell in the 19-40 years age group (74, 39.5%). These results were consistent with Antony et al.’s study, which also showed a majority (38.9%) in the age group of 20-40 years.16 Regarding antibiotic resistance, ampicillin and trimethoprim/sulfamethoxazole exhibited the highest resistance rates at 75%, followed by ceftriaxone (73.2%), cefuroxime, ceftazidime, aztreonam, and cefepime (71.4%). In contrast, lower resistance rates were observed for gentamicin (42.9%) and amikacin (32.1%). These findings aligned with investigations on AMR patterns of gut microbiota E.coli by Tawfick et al., highlighting higher resistance rates for ampicillin (72.0%), trimethoprim/sulfamethoxazole (71.9.5%), and tetracycline (60.5%).17 Additionally, a study by Danielle et al. across various regions demonstrated commensal E. coli isolates having resistance rates of 69%, 70%, 56%, and 17% against ampicillin and trimethoprim/sulfamethoxazole.18
Within this research, it was found that around 78.2% of the 110 E. coli isolates obtained from the faecal samples of healthy individuals demonstrated resistance to two or more classes of antibiotics, signifying a state of multidrug resistance (MDR). Similarly, a study by Shirajum et al. reported an MDR E. coli incidence of 75.09%, aligning with the present findings.19 Among these MDR E. coli isolates, 7.2% were carbapenem-resistant, consistent with another study by Nasheed et al., which reported a 6.2% carbapenem-resistant rate.20 These occurrences could be attributed to poor sanitation and inadequate antibiotic therapy, contributing to AMR escalation.
Notably, this study revealed sensitivity to Imipenem (92.8%) and Meropenem (92.8%), followed by Amikacin (67.9%) and Gentamicin (57.1%). The findings aligned with Fahimeh et al.’s research, which highlighted meropenem, imipenem, and gentamicin as the most potent antibiotics, exhibiting susceptibility rates of 98.5%, 98.5%, and 55.4%, respectively.21
Nevertheless, the frequency of carbapenemases, specifically Metallo-β-lactamases (MBLs), has notably risen, leading to heightened resistance against carbapenems-a critical antibiotic class often considered the final resort against multidrug-resistant Gram-negative bacteria. In this research, 2.72% of E. coli isolates carried the blaNDM-1 gene, resembling a study by Anisha Thapa et al., where 2.1% of E. coli isolates expressed the blaNDM-1 gene.22
The findings of this investigation underscore the urgent need for early pathogen detection and appropriate management to ensure effective treatment and prevent the spread of such strains. Routine monitoring of AMR and enhancing laboratory capabilities for detecting resistant genes are vital for doctors and policymakers to implement appropriate measures.
Further studies are required, including environmental sampling and an analysis of prescription patterns in the area, to accurately assess the extent of multidrug resistance (MDR) in the community. Continuous surveillance efforts should be implemented to monitor the alarming situation. Strict enforcement of regulations concerning antibiotic procurement, prescriptions, and patient compliance is essential. Future genomic studies should track E. coli resistance evolution, investigate blaNDM-1 gene spread in gut microbiota, explore resistance mechanisms and identify environmental reservoirs in rural areas.
Multi-drug resistant (MDR) bacterial proliferation is a growing concern on a global scale, particularly in less developed regions. This study revealed a notable risk of antibiotic-resistant E. coli bacteria being present in the faecal of healthy individuals due to prior antibiotic use, environmental exposure or ingestion of contaminated food and water. The findings emphasized a high prevalence of MDR, with 78.2% of E. coli isolates displaying multidrug resistance. Additionally, the blaNDM-1 gene was identified in 2.72% of these isolates. This has the potential for widespread distribution and may also be expressed under antibiotic pressure. The spread of these genes could negatively impact treatment strategies for community-acquired infections. This study underscores the critical importance of curbing unrestricted access and inappropriate usage of antibiotics in both public and private healthcare setups. Implementing stringent regulations to govern over-the-counter availability and promoting responsible pharmaceutical use, alongside regular enforcement of antibiotic stewardship programs in healthcare institutions, is imperative to combat the escalating threat of antimicrobial resistance.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
The study was approved by the Institutional Ethical Committee, SRM Medical College Hospital and Research Centre, Chengalpattu, India, with reference number 8412/IEC/2022.
- Qin J, Li R, Raes J, et al. A human gut microbial gene catalogue established by metagenomic sequencing. Nature. 2010;464(7285):59-65.
Crossref - Milani C, Ferrario C, Turroni F, et al. The human gut microbiota and its interactive connections to diet. J Hum Nutr Diet. 2016;29(5):539-546.
Crossref - Eckburg PB, Bik EM, Bernstein CN, et al. Diversity of the human intestinal microbial flora. Science. 2005;308(5728):1635-1638.
Crossref - Meletis G. Carbapenem resistance: overview of the problem and future perspectives. Ther Adv Infect Dis. 2016;3(1):15-21.
Crossref - Bush K, Bradford PA. Epidemiology of β-Lactamase-Producing Pathogens. Clin Microbiol Rev. 2020;33(2):e00047-19.
Crossref - Meletis G, Malousi A, Tychala A, et al. Probable Three-Species In Vivo Transfer of blaNDM-1 in a Single Patient in Greece: Occurrence of NDM-1-Producing Klebsiella pneumoniae, Proteus mirabilis, and Morganella morganii. Antibiotics. 2023;12(7):1206.
Crossref - Pierce VM, Simner PJ, Lonsway DR, et al. Modified Carbapenem Inactivation Method for Phenotypic Detection of Carbapenemase Production among Enterobacteriaceae. J Clin Microbiol. 2017;55(8):2321-2333.
Crossref - Shibata N, Doi Y, Yamane K. PCR typing of genetic determinants for metallo-β-lactamases and integrases carried by gram-negative bacteria isolated in Japan, with focus on the class 3 integron. J Clin Microbiol. 2003;41(12):5407-5413.
Crossref - Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 32nd ed. CLSI; 2022. CLSI document M100.
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 32nd ed. CLSI; 2022. CLSI document M100
- Kachkin DV, Khorolskaya JI, Ivanova JS, Rubel AA. An Efficient Method for Isolation of Plasmid DNA for Transfection of Mammalian Cell Cultures. Methods Protoc. 2020;3(4):69.
Crossref - Antony S, Ravichandran K, Kanungo R. Multidrug-resistant Enterobacteriaceae colonising the gut of adult rural population in South India. Indian J Med Microbiol. 2018;36(4):488-493.
Crossref - Mahmoodi F, Rezatofighi SE, Akhoond MR. Emerging of Commensal Escherichia coli Carrying Resistance Genes Against Carbapenems, a Threat to Public Health. Research Square. 2020:1-9.
Crossref - Thapa A, Upreti MK, Bimali NK, et al. Detection of NDM Variants (blaNDM-1, blaNDM-2, blaNDM-3) from Carbapenem-Resistant Escherichia coli and Klebsiella pneumoniae: First Report from Nepal. Infect Drug Resist. 2022;15:4419-4434.
Crossref - Mahmoodi F, Rezatofighi SE, Akhoond MR. Emerging of Commensal Escherichia Coli Carrying Resistance Genes Against Carbapenems, a Threat to Public Health. Research Square; 2020. 1-9
Crossref - Antony S, Ravichandran K, Kanungo R. Multidrug-resistant Enterobacteriaceae colonising the gut of adult rural population in South India. Indian J Med Microbiol. 2018;36(4):488-493.
Crossref - Tawfick MM, Elshamy AA, Mohamed KT, El Menofy NG. Gut Commensal E. coli, a High-Risk Reservoir of Transferable Plasmid-Mediated Antimicrobial Resistance Traits. Infect Drug Resist. 2022;15:1077-1091.
Crossref - Ingle DJ, Levine MM, Kotloff KL, Holt KE, Robins-Browne RM. Dynamics of antimicrobial resistance in intestinal Escherichia coli from children in community settings in South Asia and sub-Saharan Africa. Nat Microbiol. 2018;3(9):1063-1073.
Crossref - Monira S, Shabnam SA, Ali SI, et al. Multi-drug resistant pathogenic bacteria in the gut of young children in Bangladesh. Gut Pathog. 2017;9:19.
Crossref - Arum N, Ghafur A, Kazi M, et al. Prevalence of faecal carriage of Carbapenemase Producing Enterobacteriaceae in healthy Indian subjects from the community. Indian J Med Microbiol. 2022;40(3):374-377.
Crossref - Shenoy KA, Jyothi EK, Ravikumar R. Phenotypic identification & molecular detection of bla (ndm-1) gene in multidrug resistant Gram-negative bacilli in a tertiary care centre. Indian J Med Res. 2014;139(4):625-631
- Manchanda V, Rai S, Gupta S, et al. Development of TaqMan real-time polymerase chain reaction for the detection of the newly emerging form of carbapenem resistance gene in clinical isolates of Escherichia coli, Klebsiella pneumoniae, and Acinetobacter baumannii. Indian J Med Microbiol. 2011;29(3):249-253.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.