


Earthquakes, one of nature’s most spectacular events, can have far-reaching consequences for the population, including fatalities and injuries. Secondary effects, most notably landslides, tsunamis, and considerable ground motion and coseismal occurrences, are blamed for the ensuing calamities. These factors have the potential to exacerbate the already dire situation by creating conditions favourable to the spread of infectious diseases, which could cause even more casualties and delay relief efforts. This review presents a thorough narrative analysis of the literature on infectious diseases triggered by earthquakes in different regions of the world. It includes discussing the symptoms, causative agents, risk factors, and prevention strategies. Infections of the respiratory system, digestive system, and skin, as well as those transmitted by vectors, are the most common types of sickness among persons affected by the earthquake. In addition, methods are proposed for effectively preventing infectious diseases brought on by earthquakes. A robust channel for tracking and monitoring is required to detect infectious diseases in case of disaster before and after their occurrence. This strategy significantly aids in tracking epidemics, checking the accuracy of early warnings, and bolstering relief and restoration efforts.
Earthquake, Pathogens, Infectious Diseases, Disaster
An earthquake is a rapid, intense shaking of the Earth’s surface caused by releasing energy from the crust, which produces seismic waves. Throughout the annals of human history, we have witnessed many earthquakes, spanning from moderate to severe in intensity. These seismic events have wrought devastating effects on human settlements. Geophysical disaster such as earthquakes is the second most common natural disaster, including earthquakes. The outbreaks of infectious diseases occur in earthquakes where there is a primary significant loss of the original habitat and food, leading to staying in the primarily overcrowded relief shelters. In addition, it damages the basic infrastructure facilities like water and sanitation, spreading infectious diseases on a large scale. With its ripple effect, the earthquake can bring tsunami, which devastates water-borne infections.1,2
A sequence of earthquakes leading to many human casualties exemplified the hazards associated with urbanization. The frequency of the potential risks related to modern construction materials and building techniques was noticeable.3 An estimated 70% of the total population in 2015 was impacted by earthquakes, leading to almost three-quarters and trolling 307,918 deaths worldwide in developing nations.
By the middle of the 21st century, a few developing countries like India, Pakistan, Afghanistan, and Bangladesh will likely have a higher stake in population and the risk of destruction due to earthquakes.4
The amalgamation of Geological, climatic, and scientific advancements and human-led exploitation can provoke disaster. The impact of their actions on the well-being of a community can manifest instantly or gradually, and alterations in health conditions may be attributed to the primary incident or as a consequence of events that followed the calamity. The destruction of built infrastructure is typically the root cause of health outcomes, injuries, and fatalities following a disaster. Without people living in built communities, disasters do not occur.4,5 A cross-sectional study conducted in Afyon, Turkey by Ellidokuz et al. Concluded that building damage was the most critical risk factor for mortality and morbidity caused by earthquakes. The person’s position inside the room during the earthquake was another significant danger factor.6
The augmented mortality and morbidity from earthquakes can be ascribed to many factors. The variables that impact the seismo-tectonic context and geotechnical conditions of the affected region may lead to earthquakes.
This event impacts not only demographics but also sociocultural aspects and the community at large. Landslides, water pollution due to chemicals, post-event, water-logged debris, and contact with its aftermath are the most common causes of concern occurring due to partial or complete infrastructural damage.
There could be various types of injuries, such as musculoskeletal injuries such as fractures, burns, and head injuries, varying from lacerations to contusions. In addition, a large quantity of dust and debris is released when buildings fall, which can suffocate or impede breathing.7 The severity of the earthquake, including its location, magnitude, and estimated death rate, is tabulated in Table 1.
Table (1):
Earthquake with its location and death toll
| Year | Country | Magnitude of Earthquake | Estimated Death Toll | Ref. |
|---|---|---|---|---|
| 2023 | Turkey, Syria | 7.8 | 57,350 |
8 |
| 2021 | Haiti | 7.2 | 2,248 | |
| 2018 | Indonesia | 7.5 | 4,340 | |
| 2015 | Nepal, India | 7.8 | 8,964 | |
| 2011 | Japan | 9.0-9.1 | 19749 | |
| 2010 | Haiti | 7.0 | 1,00,000-3,16,000 | |
| 2009 | Indonesia | 7.6 | 1,115 | |
| 2005 | India, Pakistan | 7.6 | 87,351 | |
| 2004 | Indonesia, Sri Lanka, India, Thailand, Maldives, Somalia | 9.1-9.3 | 2,27,898 | |
| 2001 | India | 7.6 | 20,005 |
It is not possible to make accurate predictions about the diseases that may be transmitted due to the environmental effects caused by the earthquake. It is possible to categorize infectious infections linked to earthquakes as vector-borne, air-borne, water-borne, or originating from wounds. The onset of infectious illnesses might occur during the post-impact phase, which could span four days to four weeks. The recovery phase, which begins four weeks after the accident, is when victims with latent illnesses or infections with a protracted incubation period may recognize the clinical manifestation of symptoms.
At this stage, there is a risk of new imported diseases and existing endemic illnesses in the disaster-affected region spreading and transforming into epidemics.9
The tabulated data in Table 2, which pertains to the incidence of infectious diseases following destructive earthquakes worldwide between 2003 and 2023, demonstrates an increase in the rate of occurrence of these diseases after each of the earthquakes. During the post-earthquake period, the most frequently detected infections include those affecting the respiratory, gastrointestinal, and skin systems. Subsequently, wound infections are also commonly recorded.
Table (2):
Chronological record of earthquakes and the correlated outbreaks of infectious diseases
| Earthquake – Year(s) | Country | Infectious disease outbreak | Ref. |
|---|---|---|---|
| 2023 | Turkey | Diarrhea, Cholera | 10 |
| 2021 | Haiti | acute respiratory infections, diarrheal diseases, cholera and malaria | 11 |
| 2018 | Indonesia | Diarrhea, skin infection, malaria | 12 |
| 2015 | Nepal | Diarrhea | 13 |
| 2011 | Japan | Diarrhea (norovirus), influenza | 1 |
| 2010 | Haiti | Cholera | |
| 2005 | Pakistan | Diarrhea, hepatitis E, ARI, measles, meningitis, tetanus | |
| 2004 | Indonesia Tsunami | Hepatitis A and E, ARI, measles, meningitis, tetanus | |
| 2004 | Thailand Tsunami | Diarrhea | |
| 2003 | Iran | Diarrhea, ARI |
Earthquake and incidence of respiratory infection
Malla et al. study shows that, in the short-term period following earthquakes-induced disasters, upper respiratory tract infections are frequently observed among survivors.
The reason for this has been attributed to several factors, including the fact that many of the earthquake’s victims were housed in small evacuation shelters with inadequate ventilation, tainted drinking water, and poor personal hygiene, all of which may have increased the risk of contracting respiratory infectious diseases.13,14 Upper respiratory tract infection was widely observed as part of a major infectious disease outbreak following the 2003 Bam earthquake in Iran. 792 cases were reported due to low night-time temperatures within one month of the earthquake. The rate of respiratory infection following the Bam earthquake was 686 per 10000 residents, equivalent to 6.86% of the overall population.
Among common respiratory infectious diseases, pneumonia is prominent and frequently detected among survivors. Other reported respiratory infections are influenza, polymicrobial respiratory infections (RIs), viral upper respiratory tract infections, and contagious airborne diseases.15 The catastrophic 2010 earthquake in Haiti left the country’s healthcare sector gravely crippled. After that, the affected population experienced a rise in reported tuberculosis cases (693 per 100,000 person-years).15,16 Community-acquired pneumonia cases were reported after the 2011 earthquake-induced tsunami in East Japan. These comprise 43% of hospitalizations due to infectious diseases.17 Shibata et al. investigated the association between earthquake-induced tsunamis and death and concluded that the 2011 tsunami in East Japan increased the Pneumonia death risk.18
Earthquake waterborne and foodborne diseases
Diseases are spread through food and water primarily by ingestion of unhygienic food and water containing microorganisms such as bacteria, viruses, and parasites made from feces.
These diseases include gastroenteritis, shigellosis, Salmonella enterica, Francisella tularensis, Helicobacter Pylori, cholera, etc. Rotavirus, Hepatitis A, and E are virus-related diseases reported from earthquake devastation worldwide.8 In unprepared and unclean refugee camps, there was a 42% rise in instances of diarrhea after the 2005 Pakistan earthquake. In shelters for the displaced, 1.6% of those affected by the 2003 Bam earthquake in Iran had diarrhea. The most likely causes are inadequate sanitation, a shortage of drinking water, and bad hygiene.19,20
They evaluated data on possible infection from Duzce, Turkey, for four years after the 1999 earthquake. The author reported a higher prevalence rate for hepatitis A and E immediately after the 1999 earthquake in Duzce, Turkey. This seroprevalence study includes children of different age groups between 6 months to 17 years. The author concluded that after the earthquake, seroprevalence rates of both hepatitis were increased. The study also concluded that the prevalence rate has no significant difference concerning gender.20
Researchers studied the pediatric Salmonella enterica outbreak in the L’Auila, Italy, area four years after the earthquake that occurred on April 6, 2009. For this study, they adopted a method where routine investigation of salmonella infection was carried out from animal origin, and drinking water sampling was also done. The study’s results demonstrated that 155 children aged 1 to 15 had reported being infected with salmonella. Among them, 44 children were admitted to the hospital because of severe dehydration, electrolyte imbalance, and fever that was unresponsive to antipyretic and antibiotic medication. Out of all the infected individuals, four children had co-infection with rotavirus. In one of the reported cases, the 7-year-old child had right hip joint arthritis. The authors concluded that the high hospitalization rate highlighted the emergence of the pathogenic strain S. enterica after a catastrophic earthquake in 2009 because of water contamination after earthquake-induced geological changes.
Impact of earthquakes on vector-borne diseases
Anthropoid species like ticks, mosquitoes, midges, and mites spread vector-borne illnesses. Orientia tsutsugamushi is the causative agent of scrub typhus, primarily found in gardens, beaches, woodlands, and bushland. Humans get the diseases through the biting of infected mites. After the 2015 Nepalese earthquake in Gorakha and the powerful aftershocks that followed, reports of Scrub typhus epidemics surfaced nationwide, especially in the districts devastated by the earthquake. Following the earthquake and floods in 1991, deforestation increased mosquito populations, altered river flow patterns, and contributed to a notable spike in malaria cases in Costa Rica.21 Given that the annual incidence increased from 58.6 confirmed cases per 100,000 in the 12 months before the earthquake to 864 confirmed cases per 100,000 in the following 12 months at the height of the outbreak, it is possible that the outbreak, it is possible that the 2003 earthquakes in Southern Iran caused a disease outbreak.22 The reported cases of Zika virus infection increased as a result of the earthquake that took place in Ecuador in 2016.23
Manimunda et al. studied the condition of malaria in 2008 after four years of devastating earthquakes and tsunamis that hit the Nicobar group of islands in India. The authors concluded that there was a significant increase in malaria cases in post-tsunami years. The percentage of cases with Plasmodium falciparum had increased to 53% from 23% from 2006 to 2007. The research study revealed that Nancowry Island in Nicobar is highly endemic, with a high transmission probability and a high-risk region for malaria.24
Perez-Martin et al. Incidence of chickenpox in Lorca, Spain, in displaced population in temporary camps. Lorca suffered from 2 earthquakes in May 2011. During the vaccination campaign, 4 cases of chickenpox were reported. Suitable measures, which include an immunization campaign, were adopted to stop the spread of chickenpox in the surrounding areas in the aftermath of the earthquake.25
There is an augmented risk of pathogenic exposure because of severe crush injuries that occur because of being trapped under rubble for an extended period. The majority of the patients from the 2008 Sichuan earthquake were buried beneath dirt, bricks, or broken stones. There was a correlation between wound infection occurrence, time spent under debris, and the duration between injury and treatment. In wound samples, Staphylococcus aureus was the pathogen that occurred most commonly. Escherichia Coli, Acinetobacter baumannii, Enterobacter cloacae, and Pseudomonas aeruginosa were among the 73.2% of Gram-negative bacteria identified. Gram-positive bacteria, on the other hand, constituted just 24.4%.26 The 2015 earthquake in Nepal’s Gorkha region confirmed the prevalence of Gram-negative bacteria in wound infections. Besides this gas gangrene case, occurrences of tetanus and other infections were reported as well.27
After the 2009 earthquake that struck L’Aquila, central Italy, in April 2009, a retrospective evaluation of hospitalization data compared this data of 2 months with hospitalization data in the same period for the previous year. The authors observed that hospitalizations for infectious diseases increased after the earthquake while other diseases decreased. Cardiovascular, psychiatric, and gynecological infections and chronic diseases rose post-earthquake, whereas pneumological, gastroenterological, traumatic, and other diseases decreased. The authors have concluded that natural disasters like earthquakes significantly alter hospitalization patterns. The authors suggested that these findings could aid in developing tailored intervention programs for natural disasters, specifically earthquakes.28
Potential Risk Factors for Infectious Diseases Occurrence
Infectious diseases after disasters like earthquakes devastate the population, but they hamper the recovery process as well. However, our knowledge of the frequency, geographic distribution, features, and risk factors of disease epidemics worldwide after disasters is inadequate. The capability to prepare for, monitor, and respond to disease outbreaks that may arise in the aftermath of catastrophe is restricted. The earthquake has a prominent impact on the environmental conditions of the surrounding region, which may trigger infectious diseases.
The destruction of houses and the consequent displacement are prime reasons for the outbreak of infectious diseases and their subsequent spread. Takahashi et al. reported an outbreak of pneumonia after the 11th March 2011 earthquake in Japan. This massive earthquake, followed by a tsunami, destroyed houses and left many residents without basic amenities and houses. This forced residents to migrate to overcrowded shelters. The number of individuals displaced from their damaged homes amounted to nearly 11000, and they were moved to crowded facilities such as schools, community centers, and gymnasiums. This results in an increase in cases of pneumonia. Authors reported a sharp rise in pneumonia cases in the first three weeks after the earthquake.29
Poor and unscientific housing was reported as the third most common factor associated with earthquakes and subsequent infection. The aftermath of these events resulted in extensive damage to the infrastructure, leading to displacement in combination with housing risk factors, which were apparent through the high incidence of overcrowding, poor quality or temporary shelter, and camp settings.30
Using the Hospital Discharge Records as a data source, Fiasca et al. carried out a retrospective observational research to look at the possible effects of the 2009 L’Aquila earthquake on hospitalizations for bacterial meningitis. The municipalities within the impacted zone had a hospitalization rate for H. influenza in 2009 that was more than six times higher than those within the non-affected area. S. pneumonia was more common in the earthquake crater than in the nearby region. The authors have concluded that overcrowding is the leading cause of infectious disease transmission, which might result in an epidemic of acute respiratory illnesses, pneumonia, and meningitis.31
When medical facilities are destroyed, it becomes more complex and takes longer to give the afflicted people the emergency treatment they need. A couple of the immediate consequences of the partial destruction of the road network include temporary interruptions to transport services and difficulties in acquiring supplies and emergency services. One distinctive feature of the effect on lifelines is its capacity to incite contagious diseases and perhaps cause mortality among earthquake survivors.32
The risk factors that facilitate the spread of infectious diseases can be summarized as
- Heavy damage to the critical infrastructure facilities
- Lack of awareness among residents
- Survivors who are seriously injured, highly exposed to pathogens
- Drastic changes in weather and climatic conditions of the affected region
- Prolonged exposure to dust particles and particulate matter
- Overcrowded evacuation camps and emergency shelters
- Lack of basic facilities, including safe food, clean drinking water
- The dependence of individuals in affected communities who are young children, disabled, or elderly
- Poor socio-economic circumstances
- Insufficient or poor vaccine coverage due to restricted vaccination campaigns, short supplies, etc.
- Inadequate teaching and training in the prevention and management of infectious illnesses
Strategies for prevention and control
Considering the possibility of endemic infection, analyzing factors that may cause infectious diseases because of earthquakes can be beneficial in adopting and implementing effective prevention strategies. A prominent study conducted by Mavroulis S in Greece has determined that the co-occurrence of disasters and the COVID-19 pandemic presents a significant likelihood of generating compound emergencies defined by novel and unparalleled challenges.32 An earthquake mitigation strategy must include the following essential elements: establishing a reliable system for monitoring disease outbreaks, managing infectious diseases among first responders and affected populations, preventing the spread of infectious diseases in emergency shelters, and conducting education, training, and awareness-raising campaigns.
Using case studies, Gill et al. examined how various dangers interact and affect human populations. The authors of this study have synthesized a significant amount of information from numerous scientific disciplines by utilizing accessible visualization techniques. The significance of limiting hazard interactions and the importance of a comprehensive (or multihazard) strategy for evaluating natural hazards is emphasized. The conclusion of this review states that hazards interact when a primary hazard either triggers or increases the likelihood of a secondary hazard.33
Disease surveillance system
In August 2012, Iran was struck by two magnitude 6.3 and 6.4 earthquakes on the Richter scale. Following this disaster, the government established a surveillance system for 19 communicable diseases.34 In one study, the Authors highlighted some positive points about this surveillance system. Figure depicts the information flow inside Iran’s illness monitoring system following the earthquake. These include staff familiarity with the system and quick implementation with minimum costs. The system’s shortcomings have also been highlighted by the authors, including an uncalculated denominator, the lack of engagement from general hospitals and the private sector, the lack of health house staff involvement, the lack of inter-sectoral coordination, and inconsistent data collecting.
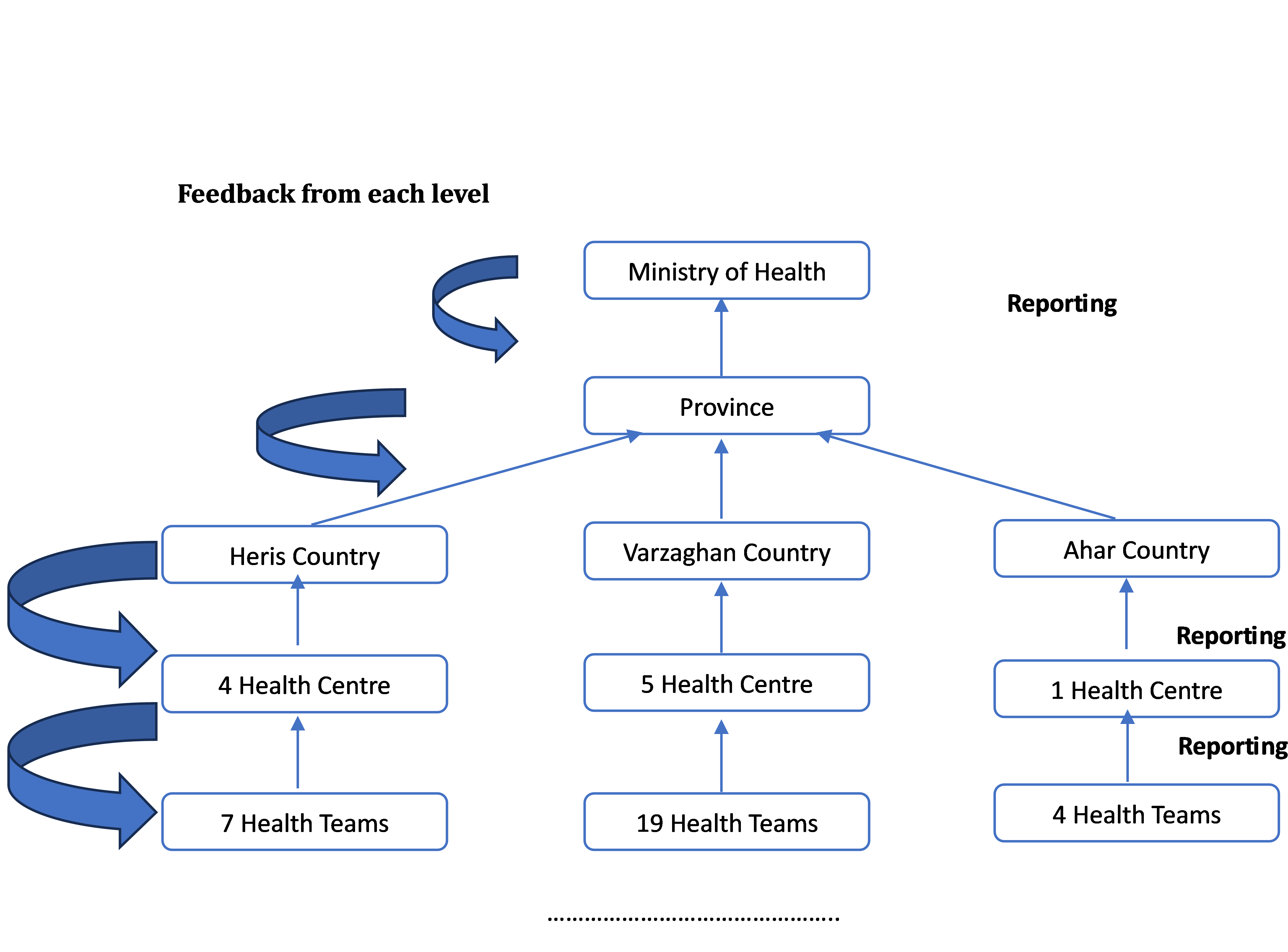
Figure. Flow of information in a disease surveillance system in after the earthquake
Authors have concluded that established surveillance systems function well to control communicable diseases. However, to successfully control the disease’s future spread, a web-based monitoring system for data gathering and recording must be established.35
In 2010, Haiti experienced an earthquake of magnitude 7.0, which caused the death of more than 2 lakh people. Haiti lacked an efficient surveillance system to provide timely data at that time. Two weeks later, the Haitian government and other agencies established the National Sentinel Site Surveillance (NSSS) system. The data from the DNS system has assisted in efficiently allocating resources and identifying successful public health interventions; however, there is still room for improvement in the system’s overall quality and data reporting.36
Turkey was devastated by a strong earthquake in 2023. The Ministry of Health uses the “Surveillance and Early Warning System” (IZCI) to rapidly track case reports and assess the potential for epidemics in seismically active areas. The ministry created the Infectious Illness Surveillance and Early Warning System (IZCI) to quickly monitor infectious illness data and analysis obtained from earthquake zones. Based on the information gathered and examined in this particular situation, no outbreak of a contagious illness has been found.37
Strategies to prevent infectious disease in emergency shelter rooms
Implementing a proper triage system helps manage the available resources effectively and efficiently. After the 2011 Japanese earthquake and tsunami, emergency shelters provided temporary accommodation and food to those in need. A study reported that because the emergency shelters were so crowded that refugees were unable to turn over, they were forced to sleep on their backs on the ground. Some people disregarded their dental hygiene, while others even refrained from coughing so as not to bother other people around. Pneumonia was caused by the factors above, as well as the combination of low temperatures, starvation, and frequent aspiration, which mainly affected elderly individuals and newborns.38
To stop the spread of infectious diseases, shelters should implement some corrective measures. These include providing ample amounts of clean, safe drinking water; preventing the spread of respiratory tract infections through the use of personal protective equipment (PPE), mosquito nets, insect repellents, and spraying; providing appropriate pharmaceutical materials and potent vaccines in sufficient quantities; providing dry and canned food; and providing adequate ventilation.
More emergency shelters of the same or other kinds should be constructed to avoid overcrowding. To prevent the spread of SARS-CoV-2 in the areas affected by the earthquakes, this tactic proved effective during the devastating earthquakes that devastated Greece during the COVID-19 pandemic.39
Strategies to prevent infectious disease in the population
When an earthquake profoundly affects the built environment and the populace in the affected area, search and rescue teams are called upon not only by the services of the affected country and those of its neighbors but also by other countries on different continents with distinct epidemiological features. Everyone in disaster management should uphold the primary rule of inflicting no damage, including rescuers, volunteer teams, and humanitarian organizations. Integrated vector management is an excellent measure to control infections. The 2010 Haitian earthquake that resulted in a cholera outbreak that claimed more lives than the earthquake’s damage to the nation’s infrastructure and structures is an example of earthquake infections. Numerous scholars have examined this outbreak. The majority of the local population’s poor adherence to personal hygiene guidelines and the poor environmental and personal hygiene standards of the aid workers’ housing was blamed for the cholera epidemic in a nation where the disease is not prevalent.40
The following measures are deemed essential to mitigate the impact on the population
- Making sure drinking water and sewerage systems are safe.
- Adhering to the current safety and hygiene protocols.
- Activities that promote awareness of hygiene and sanitation education.
- The implementation of preventive vaccination and medication programs for multiple infectious diseases is necessary.
- Stopping rumors and fake news that cause fear during a disaster and ensuring that health information management protocols deliver valid and reliable information.
- The concept of e-health and telemedicine can be invaluable during a disaster, considering qualified human resources may be delayed due to various factors.41
Earthquakes have only occurred in regions with active fractures. A rupture along these active faults would severely affect the local population and built environment in both primary and secondary ways. Several variables, such as pre-existing conditions, changes brought on by the earthquake, the physiographic and socioeconomic features of the area, and infectious disease outbreaks, can impact public health, potentially resulting in fatalities and postponing recovery. This review reveals that regions affected by destructive earthquakes that caused significant human casualties, injuries, and displacement have also reported cases of infectious diseases caused by earthquakes. Additionally, places that have suffered earthquakes resulting in substantial damage to buildings and infrastructure but with no fatalities and regions affected by avian influenza, swine flu, and avian influenza A are also included. Several factors, such as the magnitude and severity of the earthquake, its primary and secondary effects, the demographic and epidemiological features of the area, the level of education, the living conditions, and the damage to public health infrastructure, increase the risk of infectious illnesses in earthquake-affected areas.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
Not applicable.
- Kouadio IK, Aljunid S, Kamigaki T, Hammad K, Oshitani H. Infectious Diseases Following Natural Disasters: Prevention and Control Measures. Expert Rev Anti Infect Ther. 2012;10(1):95–104.
Crossref - Lechat MF. The Epidemiology of Health Effects of Disasters. Epidemiol Rev. 1990;12(1):192-198.
Crossref - Boughazi K, Rebouh S, Aiche M, Harkat N. Seismic Risk and Urbanization: The Notion of Prevention. Case of the City of Algiers. Procedia Economics and Finance. 2014;18:544-551.
Crossref - He C, Huang Q, Bai X, et al. A Global Analysis of the Relationship Between Urbanization and Fatalities in Earthquake-Prone Areas. International Journal of Disaster Risk Science. 2021;12:805-820.
Crossref - Bourque LB, Siegel JM, Kano M, Wood MM. Morbidity and Mortality Associated with Disasters. Springer. 2007:97-112.
Crossref - Ellidokuz H, Ucku R, Aydin UY, Ellidokuz E. Risk Factors for Death and Injuries in Earthquake: Cross-Sectional Study from Afyon, Turkey. Croat Med J. 2005;46(4):613-618.
- Mavrouli M, Mavroulis S, Lekkas E, Tsakris A. The Impact of Earthquakes on Public Health: A Narrative Review of Infectious Diseases in the Post-Disaster Period Aiming to Disaster Risk Reduction. Microorganisms. 2023;11(2):419.
Crossref - https://en.wikipedia.org/wiki/List_of_natural_disasters_by_death_toll (Accessed on 15 June 2024)
- Baker RE, Mahmud AS, Miller IF, et al. Infectious Disease in an Era of Global Change. Nat Rev Microbiol. 2022;20(2):193-205.
Crossref - The Lancet Responding to the Turkiye–Syria Earthquake: What Will It Take? Lancet. 2023;401(10376):525.
Crossref - https://news.un.org/en/story/2021/09/1099122 (Accessed on 15 June 2024)
- https://reliefweb.int/disaster/eq-2018-000156-idn (Accessed on 15 June 2024)
- Kanbara S, Ngatu RN, Pokhrel T, Pandey A. The 2015 Nepal Earthquake Disaster: Is the Threat of Occurrence of Communicable Disease Epidemic Over? International Journal of Indonesian National Nurses Association (IJINNA). 2018;1(1):105–110.
Crossref - Malla T, MKSSSS. Analysis of Post Earthquake Disease Pattern in a Camp at Gyampesal Gorkha. Kathmandu Univ Med J. 2016;14(55):249-253.
- Koenig SP, Rouzier V, Vilbrun SC, et al. Tuberculosis in the Aftermath of the 2010 Earthquake in Haiti. Bull World Health Organ. 2015;93:498-502.
Crossref - Ratnayake R, Finger F, Edmunds WJ, Checchi F. Early Detection of Cholera Epidemics to Support Control in Fragile States: Estimation of Delays and Potential Epidemic Sizes. BMC Med. 2020;18(1):397.
Crossref - Ohkouchi S, Shibuya R, Yanai M, Kikuchi Y, Ichinose M, Nukiwa T. Deterioration in Regional Health Status after the Acute Phase of a Great Disaster: Respiratory Physicians’ Experiences of the Great East Japan Earthquake. Respir Investig. 2013;51(2):50-55.
Crossref - Shibata Y, Ojima T, Tomata Y, et al. Characteristics of Pneumonia Deaths after an Earthquake and Tsunami: An Ecological Study of 5.7 Million Participants in 131 Municipalities, Japan. BMJ Open. 2016;6(2):e009190
Crossref - Kaya AD, Ozturk CE, Yavuz T, Ozaydin C, Bahcebasi T. Changing Patterns of Hepatitis A and E Sero-Prevalences in Children after the 1999 Earthquakes in Duzce, Turkey. J Paediatr Child Health. 2008;44(4):205-207.
Crossref - Nigro G, Bottone G, Maiorani D, Trombatore F, Falasca S, Bruno G. Pediatric Epidemic of Salmonella Enterica Serovar Typhimurium in the Area of L’Aquila, Italy, Four Years after a Catastrophic Earthquake. Int J Environ Res Public Health. 2016;13(5):475.
Crossref - Saenz R, Bissell RA, Paniagua F. Post-Disaster Malaria in Costa Rica. Prehosp Disaster Med. 1995;10(3):154-160.
Crossref - Fakoorziba MR, Baseri A, Eghbal F, Rezaee S, Azizi K, Moemenbellah-Fard MD. Post-Earthquake Outbreak of Cutaneous Leishmaniasis in a Rural Region of Southern Iran. Ann Trop Med Parasitol. 2011;105(3):217-224.
Crossref - Pacheco Barzallo D, Pacheco Barzallo A, Narvaez E. The 2016 Earthquake in Ecuador: Zika Outbreak After a Natural Disaster. Health Secur. 2018;16(2):127-134.
Crossref - Manimunda SP, Sugunan AP, Sha WA, et al. Tsunami, Post-Tsunami Malaria Situation in Nancowry Group of Islands, Nicobar District, Andaman and Nicobar Islands. Indian J Med Res. 2011;133(1):76-82.
- Perez-Martin JJ, Guirado FJR, Molina-Salas Y, Bernal-Gonzalez PJ, Navarro-Alonso, JA. Vaccination Campaign at a Temporary Camp for Victims of the Earthquake in Lorca (Spain). Hum Vaccin Immunother. 2017;13(7):1714-1721.
Crossref - Tao C, Kang M, Chen Z, et al. Microbiologic Study of the Pathogens Isolated from Wound Culture among Wenchuan Earthquake Survivors. Diagn Microbiol Infect Dis. 2009;63(3):268-270.
Crossref - Lachish T, Halperin T, Snitser O, et al. The Spectrum of Bacteria and Mechanisms of Resistance Identified from the Casualties Treated in the Israeli Field Hospital after the Earthquake in Nepal, 2015: A Retrospective Analysis. Travel Med Infect Dis. 2020;37:101707.
Crossref - Petrazzi L, Striuli R, Polidoro L, et al. Causes of Hospitalisation before and after the 2009 L’Aquila Earthquake. Intern Med J. 2013;43(9):1031-1034
Crossref - Takahashi H, Fujimura S, Ubukata S, et al. Pneumonia after Earthquake, Japan, 2011. Emerg Infect Dis. 2012;18(11):1909-1911
Crossref - Charnley GEC, Kelman I, Gaythorpe KAM, Murray KA. Traits and Risk Factors of Post-Disaster Infectious Disease Outbreaks: A Systematic Review. Sci Rep. 2021;11(1):5616.
Crossref - Fiasca F, Mattei A, Vittorini P, et al. Bacterial Meningitis Hospitalizations after the 2009 L’Aquila Earthquake: A Retrospective Observational Study. Asian J Epidemiol. 2017;11(1):46-51.
Crossref - Mavroulis S, Mavrouli M, Lekkas E. Geological and Hydrometeorological Hazards and Related Disasters amid COVID-19 Pandemic in Greece: Post-Disaster Trends and Factors Affecting the COVID-19 Evolution in Affected Areas. Saf Sci. 2021;138:105236.
Crossref - Gill JC, Malamud BD. Reviewing and Visualizing the Interactions of Natural Hazards. Reviews of Geophysics. 2014;52(4):680-722.
Crossref - Murray J, Cohen AL. Infectious Disease Surveillance, IInd Edition. In International Encyclopedia of Public Health; Elsevier. 2017:222-229.
Crossref - Noah N. Disease Surveillance. In Encyclopedia of Virology; Elsevier. 2008:44-51. eBook ISBN: 9780080547978
- Babaie J, Fatemi F, Ardalan A, Mohammadi H, Soroush M. Communicable Diseases Surveillance System in East Azerbaijan Earthquake: Strengths and Weaknesses. PLoS Curr. 2014.
Crossref - https://www.dailysabah.com/turkiye/turkiyes-health-ministry-monitors-public-health-withizci-in-quake-zone/news (Accessed on 22 Feb. 2024)
- Doran KM, Johns E, Schretzman M, et al. Homeless Shelter Entry in the Year After an Emergency Department Visit: Results From a Linked Data Analysis. Ann Emerg Med. 2020;76(4):462-467.
Crossref - Mavroulis S, Mavrouli M, Kourou A, Thoma T, Lekkas E. Multi-Hazard Emergency Response for Geological Hazards Amid the Evolving COVID-19 Pandemic: Good Practices and Lessons Learned from Earthquake Disaster Management in Greece. Sustainability. 2022;14(4):8486.
Crossref - Jafari N, Shahsanai A, Memarzadeh M, Loghmani A. Prevention of Communicable Diseases after Disaster: A Review. J Res Med Sci. 2011;16(7):956-962.
- Orata FD, Keim PS, Boucher Y. The 2010 Cholera Outbreak in Haiti: How Science Solved a Controversy. PLoS Pathog. 2014;10(4):e1003967.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.