


ISSN: 0973-7510
E-ISSN: 2581-690X
Pneumonia continues to be a major cause of morbidity and mortality in children. Pneumonia is the leading killer of children worldwide. For the diagnosis of pneumonia, the World Health Organization has introduced guidelines for the management of cases to reduce the mortality of these diseases on the basis of simple clinical signs followed by the empirical treatment with antibiotics. More than 99% of deaths related to pneumonia among children occur in countries having a low and middle income. To study the Radiological finding of Community-Acquired Pneumonia (CAP) in children. Across sectional study was conducted in which the sample size for the study was calculated from the expected prevalence of CAP based on other studies (74%). The sample size calculated by the required criterion for this study is 96. I was able to cover 118 patients as per the inclusion criteria in this study. The Patients of pediatric age groups and either sex attending tertiary care hospital with complaints suggestive of CAP. In this study total number of patients are 118 included who presented with the signs and symptoms suggestive of pneumonia. The findings of chest X-Ray of Right Lung with respect to different bacterial agents. Consolidation of the Right upper lobe is found to be statistically significant with respect to Streptococcus pneumonia and consolidation of the right lower lobe is found to be statistically significant with respect to bacteria Staphylococcus aureus whereas there is no statistically significant association with respect to other bacteria. The radiological finding of CAP in children attending pediatric OPD was observed that there was no association with any other bacteria.
Community Acquired Pneumonia(CAP), Hospital Acquired Pneumonia (HAP), chest X-Ray (CXR)
Pneumonia continues to be a major cause of mortality and morbidity in children. Pneumonia is the leading killer of children worldwide. As per the reports, in 2013 it is estimated that about 9 lakhs deaths have been occurred due top pneumonia. More than 99% deaths related to pneumonia among children occurs in the countries having low and middle income.1 Although chest radiograph is the preferred diagnostic modality for pneumonia, less than half of the world’s population has access to basic radiology services.2,3 For the diagnosis of pneumonia, the World Health Organization has introduced guidelines for the management of cases to reduce the mortality of these diseases on the basis of simple clinical signs followed by the empirical treatment with antibiotics4 Clinically, severity of respiratory tract infection may vary in ranges, from simple illness like common cold to severe illness like pneumonia.5 Generally there is a belief that lower respiratory tract below larynx level is usually sterile.6 An upper respiratory tract infection is followed by pneumonia. Microorganisms causing infections of Lower Respiratory tract are usually transmitted from close personal contact by means of the droplets. Organisms may be inhaled, Following initial colonization of the nasopharynx which leads to a pulmonary focus of infection. Less commonly, the initial upper airway colonization results in bacteremia, with subsequent seeding of the lung parenchyma.7
Typically, pneumococcal pneumonia presents acutely over the affected lobe with fever, non-productive cough, decreased breath sounds or crackles and tachypnea. Atypical pneu¬monia, often has a more non-specific presentation with gradually worsening cough, sore throat, myalgia, fever, malaise, headache, and photophobia. Mycoplasma causing Pneumonia may also have extrapul-monary symptoms such as arthritis, meningoencephalitis or myocarditis.8, 9 Moreover, the specificity and sensitivity of the physical examination findings are really very less as an average sensitivity of 58% and specificity of 67%, therefore, it is really necessary to differentiate CAP from the other conditions by using chest radiograph. Sometimes etiological diagnosis can be suggested by radiological results, like tuberculosis is suggested by cavitation’s in the upper lobe and Staphylococcus aureus infection suggested by pneumatoceles. Only by clinical presentation it is difficult to determine the etiology of infection. Instead, support of laboratory results is more useful for the physician to diagnose.10
Aims and objectives
To study the Radiological finding of CAP in children.
The study was conducted in the Department of Microbiology, Himalayan Institute of Medical Sciences (HIMS), Swami Ram Nagar, Dehradun, a tertiary care teaching hospital over a period of 12 months from January – December, 2018. Subjects were recruited from patients presenting in pediatric OPD of tertiary care hospital with a symptoms suggestive of community acquired pneumonia and written informed consent was taken from parents/guardian. Ethical clearance was obtained from Institutional Ethical Committee. All data were handled confidentially and anonymously.
The cross sectional study was conducted in which the sample size for the study was calculated from the expected prevalence of CAP based on other studies (74%). The following formula was used to evaluate the sample size for the study:
N= Z21-α (1-P)/ 12
N= sample size, Z= 1.96 for 95% confidence interval; P= prevalence. The prevalence =79.1% ≈ 80% (8)
α= level of significance which is taken to be 5%.
l= relative error (10 % of prevalence P).
The sample size calculated by the required criterion for this study is 96. I was able to cover 118 patients as per the inclusion criteria into this study. The Patients of pediatric age groups and either sex attending tertiary care hospital with complains suggestive of CAP were included like fast breathing, Fever (>37.8°C), Cough, Pleuritic chest pain, Difficulty breathing, Chest in drawing, Inability to feed/ drink, Altered mental status and the exclusion criteria of this study was the Children with Hospital acquired pneumonia, ventilator associated pneumonia, with active tuberculosis, malignancy and the use of antibiotics in the 48 hours that preceded enrollment.
In this study total number of patients are 118 included who presented with the signs and symptoms suggestive of pneumonia. On follow up, 9 patients were diagnosed as cases of pulmonary tuberculosis and 2 patients as cases of diphtheria. Therefore these 11 cases were further excluded and the results were calculated in the remaining 107 cases.
The total number of cases shows the demographic profile of 107 the pneumonia patient. Maximum number 54 (51%) of cases were <1 age group, followed as 13 (12%) of cases were 1-3 age group and minimum number 9 (8%) of cases were in 4-5 age group. In gender wise distribution 72 (67.3%) were male and 35 (32.7%) were female.
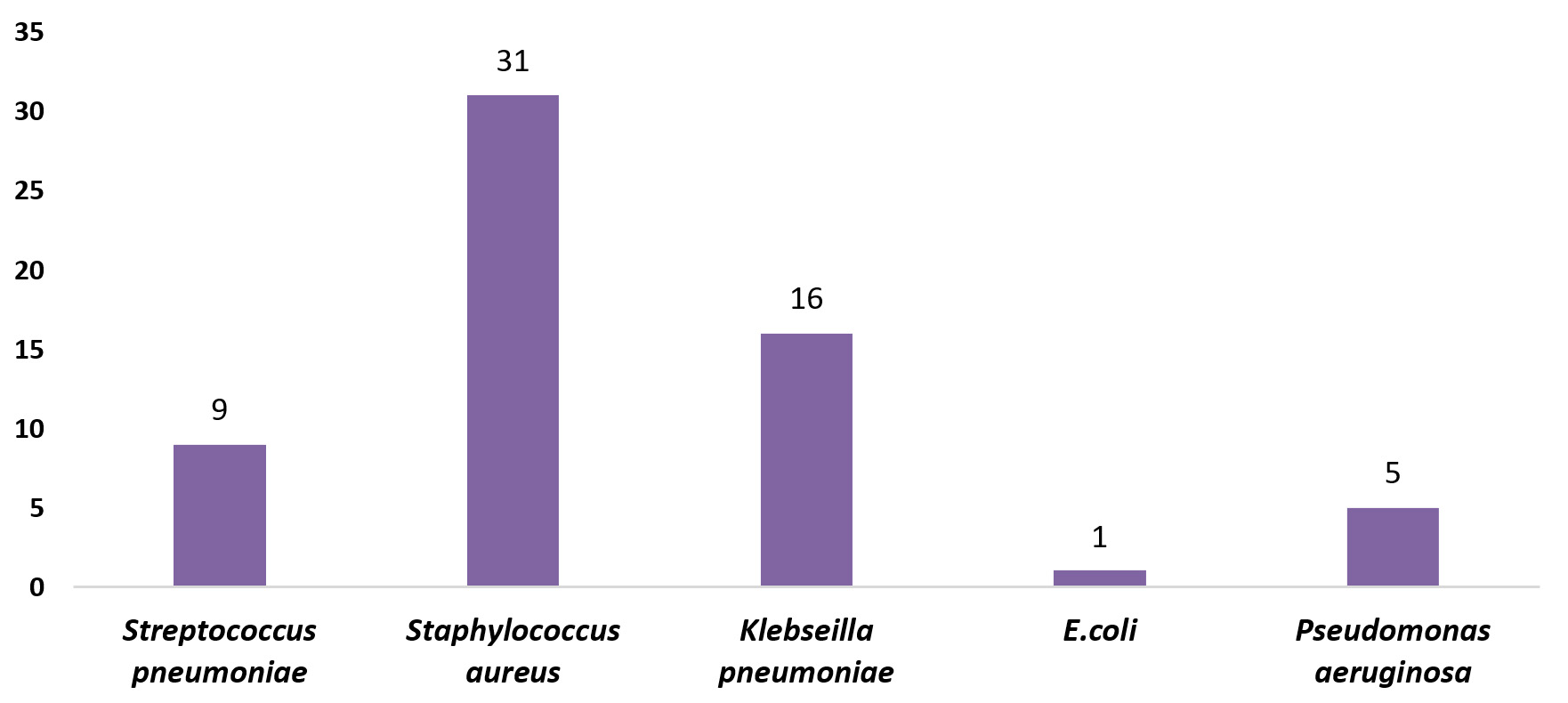
Fig. 1. Identification of the prevalence of bacterial agent through culture method
Table (1):
Distribution of Pneumonia patients according to Demography.
| variable | category ( years) | Frequency (%) |
|---|---|---|
| age
|
<1 | 54(51) |
| 1-3 | 13(12) | |
| 4-5 | 9(8) | |
| 6-12 | 16(15) | |
| 13-18 | 15(14) | |
| sex
|
male | 72(67.3) |
| female | 35(32.7) |
The above figure shows the prevalence of bacterial agent through culture method. Staphylococcus aureus shows the maximum frequency (31), followed as Klebsieilla is (16), Streptococcus is (9), Pseudomonas aeruginosa is (5) and E.coli(1) which shows the minimum frequency.
Table (2):
Prevalence of Bacterial pneumonia in patient.
Variable |
No. of Patients (Percentage) |
|---|---|
Bacterial pneumonia |
72(67.2) |
Other(pneumonia due to other causes) |
35(32.7) |
Total cases |
107 (100) |
This Table 2 shows the classification of bacterial Pneumonia patient. Majority of the cases were observed with bacterial pneumonia (67.2%) followed by other were (32.7%).
Table (3):
Chest X-Ray findings with respect to Bacterial pneumonia.
| Anatomical site of lung | Lobes | consolidation | Bacterial cause | p-value | |
|---|---|---|---|---|---|
| present | absent | ||||
| Left lung | upper lobe | Present | 23 | 7 | 0.115 |
| lower lobe | Present | 27 | 10 | 0.139 | |
| Right lung | upper lobe | Present | 37 | 28 | 0.024 |
| middle lobe | Present | 37 | 28 | 0.024 | |
| lower lobe | Present | 8 | 26 | 0.2 | |
*(p-value<0.05 is considered statistically significant)
@ N1=97 (Total N=107, Where Chest X-Ray of 10 patients was not done)
The Table 3 shows the association of consolidation findings on chest X-Ray with the bacterial cause of pneumonia. Right lung consolidation is found to be statistically significant (i.e. p- value of upper lobe= 0.024 and middle lobe=0.024) with respect to bacterial cause.
Table (4):
Consolidation as seen on CXR Left Lung with respect to bacterial agents.
| Bacteria | Consolidation: Left upper lobe | Consolidation : Left lower lobe | ||||||
|---|---|---|---|---|---|---|---|---|
| Present | Absent | p-value | Present | Absent | p-value | |||
| Streptococcus pneumoniae | Present | 3 | 5 | 0.95 | 6 | 6 | 0.275 | |
| Staphylococcus aureus | Present | 10 | 18 | 0.907 | 12 | 16 | 1 | |
| Klebsiellapneumoniae | Present | 6 | 8 | 0.576 | 6 | 8 | 1 | |
| Escherichia coli (E.coli) | Present | 0 | 1 | 0.445 | 1 | 0 | 0.244 | |
| Pseudomonas aeruginosa | Present | 2 | 3 | 0.866 | 3 | 2 | 0.419 | |
| Mycoplasma pneumoniae | Present | 1 | 2 | 0.865 | 1 | 2 | 0.865 | |
| Chlamydophilapneumoniae | Present | 3 | 6 | 0.728 | 4 | 5 | 0.202 | |
*(p-value<0.05 is considered statistically significant)
The Table 4 shows findings of chest X-Ray of Left Lung with respect to different bacterial agents. There is no statistically significant finding.
Table (5):
Consolidation as seen on CXR Right Lung with respect to bacterial agents.
| Bacteria | Right Upper Lobe | Right Middle Lobe | Right Lower Lobe | ||||||
|---|---|---|---|---|---|---|---|---|---|
| present | absent | p-value | present | absent | p-value | present | absent | P-value | |
| Streptococcus pneumoniae | 6 | 2 | 0.038 | 5 | 3 | 0.25 | 6 | 2 | 0.097 |
| Staphylococcus aureus | 10 | 18 | 0.423 | 11 | 17 | 0.77 | 9 | 19 | 0.028 |
| Klebsiellapneumoniae | 5 | 9 | 0.632 | 5 | 9 | 0.632 | 8 | 6 | 0.418 |
| Escherichia coli (E.coli) | 0 | 1 | 0.398 | 0 | 1 | 0.398 | 0 | 1 | 0.336 |
| Pseudomonas aeruginosa | 2 | 3 | 0.952 | 2 | 3 | 0.952 | 3 | 2 | 0.563 |
| Mycoplasma pneumoniae | 2 | 1 | 0.328 | 2 | 1 | 0.265 | 2 | 1 | 0.265 |
| Chlamydophilapneumoniae | 5 | 4 | 0.285 | 5 | 4 | 0.157 | 4 | 5 | 0.586 |
*(p-value<0.05 is considered statistically significant)
The Table 5 illustrates findings of chest X-Ray of Right Lung with respect to different bacterial agents. Consolidation of Right upper lobe was statistically significant (p-value=0.038) with respect to Streptococcus pneumonia and consolidation of right lower lobe is found to be statistically significant (p-value=0.028) with respect to bacteria Staphylococcus aureus whereas there is no statistically significant association with respect to other bacteria.
A total of 118 patients were included in the study with the complaints suggestive of CAP. On follow up, 9 patients were diagnosed as cases of pulmonary TB and 2 patients as cases of diphtheria. Therefore, these 11 cases were excluded and the results were calculated in the remaining 107 cases. Chest radiographic findings help in predicting pneumonia outcomes and can be an important tool for assessing disease severity.
The current study illustrates the demographic profile of age and sex of the pneumonia patient. Maximum number 54 (51%) of patient were under in <1years age group, followed as 13 (12%) of cases were 1-3 year age group and minimum number 9 (8%) of cases were in 4-5 year age group. The results were similar to a case-control study by Aftab S et al. which was conducted in Pakistan. An increased risk of pneumonia was reported in younger children (2-6 months) as compared older children.11
Among all the cases 72 (67.3%) were male and 35 (32.7%) were female. In a study done by Kengne M et al there were 144 (72%) males and 56(28%) females. Approximately, the male to female ratio was 3:1.12 Almirall, et al. in their study reported that pneumonia occurs more commonly in males than female patients. According to Almirall J et al., a case-control study in Brazil reported that the excess risk of pneumonia in boys.13
Our study has focused only on the bacterial causes of pneumonia in the patient. Majority of the cases were observed with bacterial pneumonia 72 (67.2%) followed by other were in 35 (32.7%). According to the Revised WHO classification of pneumonia, out of 107 patients, the maximum number of patients have severe pneumonia 89 (83.2%) followed by pneumonia 18 (16.8%).14 which is slightly comparable to our study.
The recent study also looks upon the association of consolidation findings on chest X-Ray with the bacterial cause of pneumonia. Right lung consolidation is found to be statistically significant (i.e. p-value of upper lobe= 0.024 and middle lobe=0.024) with respect to bacterial cause. But in a study conducted by Ianniello et al, the association on chest X-Ray; 37/60 patients showed a statistically significant right lung consolidation, and 23/60 patient showed left lung consolidation.15
In this study, the anatomical site of the left both upper and lower with respect to the bacterial cause shows statistical insignificant association, while in the right lung it shows statistically significant association with the bacterial cause. The consolidation on chest X-Ray showed statistically significant association with right upper lobe in Streptococcus pneumonia cases, while Staphylococcus aureus showed statistically significant with right lower lobe. Slightly similar to Okamoto K at el study that the right middle lobe is found statistically significant in Streptococcus pneumonia cases but in the right upper and lower lobes has been statistically significant Staphylococcus aureus.16 Meanwhile both the studies are slightly equivalent to each other.
Chest radiography continues to be a valuable method for case identification in correlation with clinical signs and symptoms of pneumonia. In the present study, radiological finding of CAP in children attending pediatric OPD was observed. It was found that CXR finding of right upper lobe was statistically significant with Streptococcus pneumoniae and that of right lower lobe with Staphylococcus aureus. No association with any other bacteria was found.
ACKNOWLEDGMENTS
We are thankful to the Swami Rama Himalayan University for providing us the opportunity for carrying out this work and financial assistance. We reserve special thanks for Department of Biostatistics and Department of Microbiology, HIMS, SRHU, Dehradun, Uttarakhand, India.
CONFLICT OF INTEREST
The authors declares that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
NP and GM conceptualize and design the study. NP, GM, NA, BK and RKA did the literature review. NP and GM did the Acquisition, analysis and interpretation of data. NP, GM, NA, BK and RKA wrote, edited and reviewed the manuscript.All authors read and approved the final version of manuscript for publication.
FUNDING
This project was funded by Swami Rama Himalayan University, Dehradun, India. (letter number – SRHU/Reg/Int/2018- 277.
ETHICS STATEMENT
This work was done as per the recommendations of the ethical committee of the Swami Rama Himalayan University. SRHU/HIMS/ETHICS/2019/47.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript
- United Nations Children’s Fund. Committing to child survival: a promise renewed. Progress Report. 2013. UNICEF; New York, NY.
- Andronikou S, McHugh K, Abdurahman N, et al. Paediatric Radiology seen from Africa. Part I: providing diagnostic imaging to a young population. Pediatric Radiology. 2011;41(7):811-825.
Crossref - Lynch T, Bialy L, Kellner JD, et al. A systematic review on the diagnosis of pediatric bacterial pneumonia: when gold is bronze. PLoS One. 2010;5(8):e11989.
Crossref - World Health Organization. Acute respiratory infections in children: case management in small hospitals in developing countries. 5th ed. Geneva: WHO, 1990.
- Reka D. Clinical, Bacteriological and Radiological Study of Community Acquired Pneumonia. Tamilnadu, Chennai; 2018.
- Epidemiology of Community-Acquired Pneumonia. J Assoc Physicians India. 2013;61(7 Suppl.):7-8.
- Matti K, Docent MR. Pediatric Community Acquired Pneumonia – A serological study on etiology with special focus on newly identified agents. 2009. http://urn.fi/urn:isbn:978-951-44-7744-7
- Gereige RS, Laufer PM. Pneumonia. Pediatric Review. 2013;34(10):438-455.
Crossref - Boyd K. Back to the Basics: Community-Acquired Pneumonia in Children. Pediatric Annals. 2017;46(7):257-261.
Crossref - Lode HM. Managing community-acquired pneumonia: E European perspective. Respir Med. 2007;101(9):1864-1873.
Crossref - Aftab S, Ejaz I, Waqar U, et al. Risk Factors for Childhood Pneumonia in North Eastern Pakistan: A Case-Control Study. Malaysian Journal of Paediatrics and Child Health. 2020;22:26-34.
- Kengne M, Lebogo MBB, Nwobegahay JM, Ondigui BE. Antibiotics susceptibility pattern of Streptococcus pneumoniae isolated from sputum cultures of human immunodeficiency virus infected patients in Yaounde, Cameroon. Pan Afr Med J. 2018;31:16.
Crossref - Almirall J, Bolibar I, Balanzo X, Gonzalez CA. Risk factors for community-acquired pneumonia in adults: A population-based case-control study. Eur Respir J. 1999;13:349-355.
Crossref - Revised WHO Classification and Treatment of Pneumonia in Children at Health Facilities: Evidence Summaries. Geneva: World Health Organization; 2014.
- Ianniello S, Piccolo CL, Buquicchio GL, Trinci M, Miele V. First-line diagnosis of paediatric pneumonia in emergency: lung ultrasound (LUS) in addition to chest-X-ray (CXR) and its role in follow-up. Br J Radiol. 2016;89(1061):1-8.
Crossref - Okamoto K, Hanaoka J. Surgical outcome of combined subsegmentectomy in the right upper lobe for GGO -dominant early stage lung cancer: Analysis of 7 cases. Respir Med Case Rep. 2019;26:123-125.
Crossref
© The Author(s) 2021. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.