

ISSN: 0973-7510
E-ISSN: 2581-690X
Ureaplasma urealyticum and Mycoplasma hominis are most important genital mycoplasma responsible for many genitourinary tract infections. Nongonococcal urethritis (NGU) and bacterial prostatitis are most clinically significant infections that affect a wide spectrum of male age groups. The incorrect or inappropriate diagnosis and susceptibility testing leads to unsuitable medication and as a results delay of recovery and bad squeal like infertility. During a period of sex months, twenty two expressed prostate secretion (EPS) samples and eighteen urethral swabs were collected from patients with age (44.55±21.22 years). All samples were inoculated to strip and after 24 hours at 37° C the results recorded. The results of detection of genital mycoplasma revealed that only 3 (16.7%) of expressed prostate secretion samples give positive results for both Ureaplasma urealyticum and Mycoplasma hominis while 10 (45.5%) urethral swab were positive for both Ureaplasma urealyticum and Mycoplasma hominis. Common age group of prostatitis infected with genital mycoplasma is (41-60 years) while urethritis was detected among all three groups. The results of antibiotic susceptibility revealed that all isolates were fully sensitive (100%) to all antibiotics incorporated within the well except for erythromycin, roxithromycin, tetracyclin and levofloxacin in which one isolate (7.7%) was exhibit resistance in both Ureaplasma urealyticum and Mycoplasma hominis. The current study conclude the genital mycoplasmas (Ureaplasma urealyticum and Mycoplasma hominis) are predominant among non gonococcal urethritis and the macrolides still the choice for treatment while prescription of quinolones and tetracyclin must be under control due to emergence of resistance isolates.
U. urealyticum, M. hominis, Prostatitis, EPS.
Mycoplasmas are cell wall lacking, small bacteria that not effected by cell wall synthesis inhibiting antibiotics. Clinically significant Mycoplasmas includes Ureaplasma urealyticum, Mycoplasma pneumoniae, Mycoplasma genitalium, and Mycoplasma hominis1. As a causative agents of non-gonococcal, con-chlamydial urethritis and prostatitis Ureaplasma urealyticum and Mycoplasma hominis were recovered from many males and females undergoing sexually transmitted disease with variable percentage2,3.
Inflammation of urethra called urethritis and it is may be due to bacterial, viral and trichomonal infection. Bacteria urethritis is most common and be on two form: gonococcal and nongonococcal urethritis. Nongonococcal urethritis is emerge due to bacterial infection other than those caused by gonococci. Commonly bacterial causes of nongonococcal urethritis comprises: C. trachomatis, U. urealyticum and M. hominis[4,5].Bacterial prostatitis is the infection of prostate gland and regards hard-treated urologic illness that need 2-12 weeks of antibiotics treatment to be cured effectively. Genitourinary mycoplasmas (U. urealyticum and M. hominis) can cause prostatitis and may implicated in the prostate cancer development [6,7].
Both of U. urealyticum and M. hominis were associated with sexually transmitted diseases and have the ability to destroy genitourinary epithelial cells8,9. Three species have been isolated from the surface of the genitourinary tract mucosa: M. hominis, U. urealyticum and recently discovered Mycoplasma genitalium10,11,12. M. hominis colonizes the genito-urinary tract and behave as an opportunistic pathogen, causing urethritis, cervicitis, pelvic inflammatory disease or chorioamnionitis. U. urealyticum regarded the common pathogen among men with urethritis and its complications13,14.
Abuse and misuse of antibiotics leads to emerging of antibiotics resistance which push a risk for human health. Due to that they are targeting cell wall, the â-lactam antibiotics and vancomycin are not active against Mycoplasmas and their susceptibility be conferred to only agents that inhibit protein synthesis, including aminoglycosides, macrolides, tetracycline chloramphenicol. They are also sensitive to that anti-topoisomerases antibiotics like fluoroquinolones15. Spreading of resistance to tetracycline and erythromycin leading to the use of clindamycin, fluoroquinolones or other macrolides following the failure of treatment with tetracycline or erythromycin16,17,18.
The current study aimed to detect genital mycoplasma (U. urealyticum and M. hominis) and their antibiotic susceptibility among non-gonococcal urethritis and prostatitis patients in Hilla city-Iraq.
Samples
Twenty two expressed prostate secretion (EPS) samples and eighteen urethral swabs were collected from patients with age (44.55±21.22 years) during a period of 6 months. All samples were transferred directly to transport media supplied with kit19,20.
Mycoplasma IES Plus Kit Principle
It is Dehydrated culture medium based assay for the screening, indicative enumeration and the identification of UU (U. urealyticum) and MH (M. hominis) in genitourinary tract of human. In the case of positive screening result, Mycoplasma IES Plus provides an extra strip for further susceptibility testing, which is partially based on CLSI (Clinical and Laboratory Standards Institute) recommendations. The mixed medium is prepared by mixing the freeze-dried powder and the diluent. After Mycoplasma has been cultivated, urease in UU will breakdown the urea and release NH3. Release of NH3 also occur by MH via breakdown of arginine by arginase leading to increases the pH of the liquid medium, the result is judged according to the color change of the indicator. The strip contains 11 antibiotics. Changing the color to red meaning growth of UU, MH or both although presence of antibiotics which reveal resistance to the specific antibiotic in the well21.
Mycoplasma IES Plus Kit Component
The kit components includes:
1-10 strips (with 30 wells have dehydrated culture medium and another supplied with antibiotics with different concentration).
2- 10 vial of Freeze-dried Powder
3- 10 vial transport medium
4- 1 vial of mineral oil
The scheme of strip and component of each well were mentioned below (figure 1):
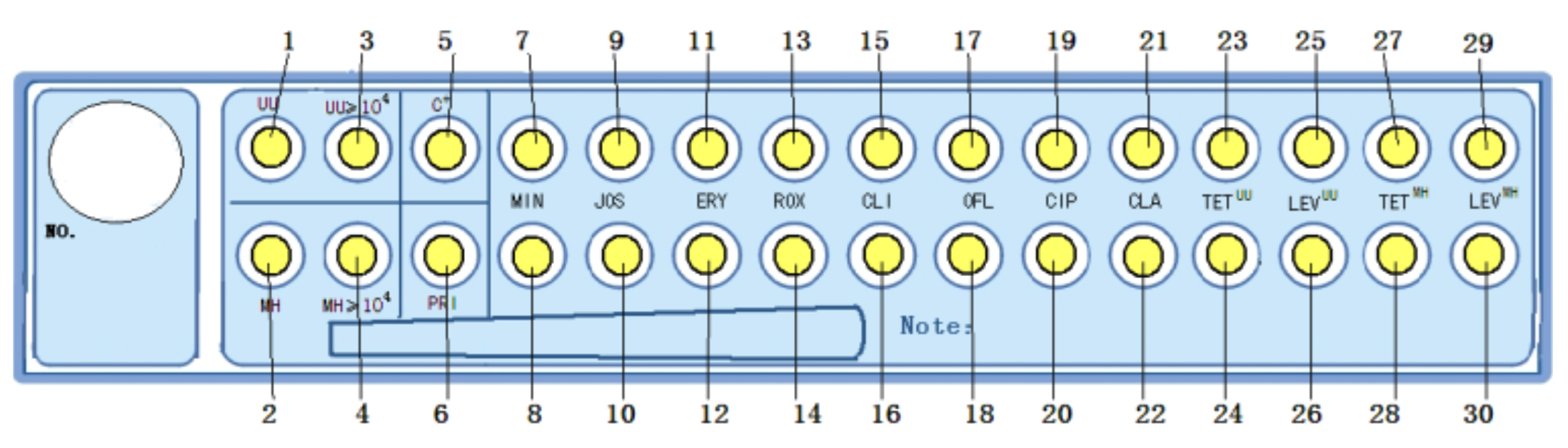
Fig. 1. Show the Mycoplasma IES Plus strip
Culture and identification and Enumeration (wells no. 1, 2, 3, 4, 5) Well no. 1 (UU): identification of U. urealyticum, Well no. 2 (MH): identification of M. hominis, Well no. 3 (UU e” 104): enumeration of U. urealyticum, Well no. 4 (MHe”104): enumeration of M. hominis and Well no. 5 (C+): positive control (table 1).
Table (1):
Show the wells for identification and enumeration..
Wells # |
Tests |
Principal Substrate |
|---|---|---|
No.1 |
UU |
Lincomycin |
No.2 |
MH |
Erythromycin |
No.3 |
UU≥104 |
Lincomycin and inhibition agent |
No.4 |
MH≥104 |
Erythromycin and inhibition agent |
No.5 |
C+ |
N/A |
Susceptibility tests (wells no. 6 to 30)
These wells are used to test the susceptibility of the strain with 11 antibiotics (table 2).
Table (2):
Show the wells for antibiotic susceptibility.
| Wells | Antibiotics and | Abbreviations | Concentrations mg/l | |
|---|---|---|---|---|
| No.6 | Pristinamycin | PRI | 2 | |
| No.7 and 8 | Minocycline | MIN | 2 | 8 |
| No.9 and 10 | Josamycin | JOS | 2 | 8 |
| No.11 and 12 | Erythromycin | ERY | 8 | 16 |
| No.13 and 14 | Roxithromycin | ROX | 1 | 4 |
| No.15 and 16 | Clindamycin | CLI | 0.25 | 0.5 |
| No.17 and 18 | Ofloxacin | OFL | 1 | 4 |
| No.19 and 20 | Ciprofloxacin | CIP | 1 | 2 |
| No.21 and 22 | Clarithromycin | CLA | 1 | 4 |
| No.23 and 24 | Tetracycline | TETUU | 1 | 2 |
| No.25 and 26 | Levofloxacin | LEVUU | 2 | 4 |
| No.27 and 28 | Tetracycline | TETMH | 4 | 8 |
| No.29 and 30 | Levofloxacin | LEVMH | 1 | 2 |
Strip Inoculation
The sample transferred directly to the transport medium, mixed well and transferred completely to the freeze-dried powder, and shake to mix completely. After the sample is inoculated, 0.5 ml of the inoculated medium incubated at 36-38 ! for 24 hours and if the color of the culture medium does not turn to red or peachblow, the sample could be deemed to be negative and no further operations are needed. When the color of the culture medium turns to red or peachblow, a 100 ìl of the culture medium will dispensed to the wells of strip, the strip was shacked to dissolve the coated materials and then one drop of the mineral oil will added to prevent evaporation during incubation. The cover the strip placed and the strip will incubated at 36-38 °C for 24 hours. The yellow color indicate negative results while peachblow to red indicate positive results.
The results of detection of genital mycoplasma revealed that only 3 (16.7%) of expressed prostate secretion samples give positive results for both Ureaplasma urealyticum and Mycoplasma hominis while 10 (45.5%) urethral swab were positive for both. The common age group of prostatitis infected with genital mycoplasma is (41-60 years) while urethritis was detected among all three groups (table 3). The positive and negative results for both Ureaplasma urealyticum and Mycoplasma hominis were showed in figure (2) and (3) respectively.
Table (3):
Distribution of genital mycoplasma among different age groups.
| Age group (Year) | Prostatitis n=18 | Urethritis n=22 | ||
|---|---|---|---|---|
| Positive (%) For both UU and MH | Negative (%) For both UU and MH | Positive (%) For both UU and MH | Negative (%) For both UU and MH | |
| 1-20 | 0 | 1 | 2 | 3 |
| 21-40 | 0 | 0 | 4 | 1 |
| 41-60 | 3 | 14 | 4 | 8 |
| Total | 3 (16.7) | 15 (83.3) | 10 (45.5) | 12 (54.5) |

Figure (2): Show the positive results of culture for both U. urealyticum and M. hominis

Figure (3): Show the negative results of culture for both U Ureaplasma urealyticum and Mycoplasma hominis.
Many studies stated that the coexistence of Ureaplasma urealyticum and Mycoplasma hominis was common and the affected age group 30-50 years. M. hominis is found as a colonizer of the Genito-urinary tract in sexually active, and is also associated with bacterial vaginosis22,23,24,25. U. urealyticum and M. hominis are prominent pathogens among men with urethritis and its complications and occur more frequently in the semen of prostatitis patients11,26.
lacking of cell wall, target of beta-lactam antibiotics and vancomycin, the most common and appropriate medication for urogenital infections caused by mycoplasmas depends upon tetracyclines, macrolides, and quinolones[15,27]. The results of antibiotic susceptibility revealed that all isolates were fully sensitive (100%) to all antibiotics incorporated within the well except for erythromycin, roxithromycin, tetracyclin and levofloxacin in which one isolate (7.7%) was exhibit resistance in both Ureaplasma urealyticum and Mycoplasma hominis.
Table (4):
Antibiotics susceptibility among Ureaplasma urealyticum and Mycoplasma hominis.
| Antibiotics (mg/l) | Antibiotic Susceptibility of U. urealyticumn=13 | Antibiotic Susceptibility of M. hominisn=13 | ||
|---|---|---|---|---|
| Sensitive | Resistance | Sensitive | Resistance | |
| Pristinamycin (2) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Minocycline (2) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Minocycline (8) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Josamycin (2) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Josamycin (8) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Erythromycin (8) | 12 (92.3%) | 1(7.7%) | 12 (92.3%) | 1(7.7%) |
| Erythromycin(16) | 12 (92.3%) | 1(7.7%) | 12 (92.3%) | 1(7.7%) |
| Roxithromycin (1) | 12 (92.3%) | 1(7.7%) | 12 (92.3%) | 1(7.7%) |
| Roxithromycin(4) | 12 (92.3%) | 1(7.7%) | 12 (92.3%) | 1(7.7%) |
| Clindamycin (0.25) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Clindamycin (0.5) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Ofloxacin (1) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Ofloxacin(4) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Ciprofloxacin (1) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Ciprofloxacin (2) | 13 (100%) | 0(0.00%) | 13 (100%) | 0(0.00%) |
| Clarithromycin (1) | 12 (92.3%) | 1(7.7%) | 12 (92.3%) | 1(7.7%) |
| Clarithromycin (4) | 12 (92.3%) | 1(7.7%) | 12 (92.3%) | 1(7.7%) |
| Tetracycline (1) UU | 12 (92.3%) | 1(7.7%) | – | – |
| Tetracycline (2) UU | 12 (92.3%) | 1(7.7%) | – | – |
| Levofloxacin (2) UU | 13 (100%) | 0(0.00%) | – | – |
| Levofloxacin (4) UU | 13 (100%) | 0(0.00%) | – | – |
| Tetracycline (4) MH | – | – | 13 (100%) | 0(0.00%) |
| Tetracycline (8) MH | – | – | 13 (100%) | 0(0.00%) |
| Levofloxacin (1) MH | – | – | 13 (100%) | 0(0.00%) |
| Levofloxacin (2) MH | – | – | 13 (100%) | 0(0.00%) |
Our data was highly similar with those gathered from many studies which found that all genital mycoplasma were fully sensitive to doxycycline, josamycin, ofloxacin and pristinamycin27,28,29,30,31. Resistance to erythromycin were recorder for both of Ureaplasma urealyticum and Mycoplasma hominis isolated from genital samples of sexually active individuals. Resistance to erythromycin among mycoplasmsas is naturally occur while resistance to tetracyclin and quinolones can be attributed to antibiotic targets mutation and it may be related to higher pathogenicity15,32,33.
The current study conclude that the genital mycoplasmas (Ureaplasma urealyticum and Mycoplasma hominis) are common among non gonococcal urethritis and the macrolides still the choice for treatment while prescription of quinolones and tetracyclin must be under control due to emergence of resistance isolates.
- Greenwood, D. Medical Microbiology, With STUDENTCONSULT online access, 18: Medical Microbiology. Elsevier Health Sciences., 2012; pp. 400-410.
- Ikonomidis, A., Venetis, C., Georgantzis, D., Giaslakiotis, V., Kolovos, V., Efstathiou, K., Moschou, M., Êoutsiaris, Å. and Panopoulou, M., Prevalence of Chlamydia trachomatis, Ureaplasma spp., Mycoplasma genitalium and Mycoplasma hominis among outpatients in central Greece: absence of tetracycline resistance gene tet (M) over a 4-year period study. New microbes and new infections, 2016; 9: pp.8-10.
- Fife, K., Williams, J.A., Fortney, S., Qadadri, B. and Ermel, A., P3. 120 Prevalence of ureaplasma urealyticum in urine of men attending a sexually transmitted disease clinic. Sex Transm Infect; 2017; 93: A138.
- Le, P.T., Hamasuna, R., Matsumoto, M., Furubayashi, K., Hatanaka, M., Kawai, S., Yamaguchi, T., Uehara, K., Murakami, N., Yoshioka, M. and Nakayama, K., The detection of microorganisms related to urethritis from the oral cavity of male patients with urethritis. Journal of Infection and Chemotherapy, 2017; 23(10): pp.668-673.
- Valentine-King, M.A. and Brown, M.B., Antibacterial Resistance in Ureaplasma Species and Mycoplasma hominis Isolates from Urine Cultures in College-Aged Females. Antimicrobial Agents and Chemotherapy, 2017; 61(10): pp.e01104-17.
- Barykova, Y.A., Logunov, D.Y., Shmarov, M.M., Vinarov, A.Z., Fiev, D.N., Vinarova, N.A., Rakovskaya, I.V., Baker, P.S., Shyshynova, I., Stephenson, A.J. and Klein, E.A., Association of Mycoplasma hominis infection with prostate cancer. Oncotarget, 2011; 2(4): p.289.
- Hung, S.C., Lai, S.W., Tsai, P.Y., Chen, P.C., Wu, H.C., Lin, W.H. and Sung, F.C., Synergistic interaction of benign prostatic hyperplasia and prostatitis on prostate cancer risk. British journal of cancer, 2013; 108(9): pp.1778-1783.
- Varela, J.A., Otero, L., Garcia, M.J., Palacio, V., Carreno, F., Cuesta, M., SÁnchez, C. and Vazquez, F. Trends in the prevalence of pathogens causing urethritis in Asturias, Spain, 1989–2000. Sexually transmitted diseases, 2003; 30(4): pp.280-283.
- Al-Marzoqi, A.H., Obaies, H. and Saad, A.M. Molecular and Cytopathological study on etiological agents responsible of Sexually Transmitted diseases. International Journal of PharmTech Research, 2016; 9(6): 357-365.
- Uusküla, A. and Kohl, P.K. Genital mycoplasmas, including Mycoplasma genitalium, as sexually transmitted agents. International journal of STD & AIDS, 2002; 13(2): pp.79-85.
- Mändar, R., Raukas, E., Türk, S., Korrovits, P. and Punab, M. Mycoplasmas in semen of chronic prostatitis patients. Scandinavian journal of urology and nephrology, 2005; 39(6): pp.479-482.
- Barykova, Y.A., Logunov, D.Y., Shmarov, M.M., Vinarov, A.Z., Fiev, D.N., Vinarova, N.A., Rakovskaya, I.V., Baker, P.S., Shyshynova, I., Stephenson, A.J. and Klein, E.A. Association of Mycoplasma hominis infection with prostate cancer. Oncotarget, 2011; 2(4): pp.289-297.
- Taylor-Robinson, D. and Lamont, R.F. Mycoplasmas in pregnancy. BJOG: An International Journal of Obstetrics & Gynaecology, 2011; 118(2): pp.164-174.
- Zdrodowska-Stefanow, B., Klosowska, W.M., Ostaszewska-Puchalska, I., Bulhak-Koziol, V. and Kotowicz, B. Mycoplasma hominis and Ureaplasma urealyticum infections in male urethritis and its complications. Adv Med Sci, 2006; 51: pp.254-257.
- Waites, K.B., Katz, B. and Schelonka, R.L. Mycoplasmas and ureaplasmas as neonatal pathogens. Clinical microbiology reviews, 2005; 18(4): pp.757-789.
- Pereyre, S., Renaudin, H., Charron, A., Bébéar, C. and Bébéar, C.M. Emergence of a 23S rRNA mutation in Mycoplasma hominis associated with a loss of the intrinsic resistance to erythromycin and azithromycin. Journal of Antimicrobial Chemotherapy, 2006; 57(4): pp.753-756.
- Mardassi, B.B.A., Aissani, N., Moalla, I., Dhahri, D., Dridi, A. and Mlik, B. Evidence for the predominance of a single tet (M) gene sequence type in tetracycline-resistant Ureaplasma parvum and Mycoplasma hominis isolates from Tunisian patients. Journal of medical microbiology, 2012; 61(9): pp.1254-1261.
- Dégrange, S., Renaudin, H., Charron, A., Bébéar, C. and Bébéar, C.M. Tetracycline resistance in Ureaplasma spp. and Mycoplasma hominis: prevalence in Bordeaux, France, from 1999 to 2002 and description of two tet (M)-positive isolates of M. hominis susceptible to tetracyclines. Antimicrobial agents and chemotherapy, 2008; 52(2): pp.742-744.
- Brill, J.R. Diagnosis and treatment of urethritis in men. American family physician, 2010; 81(7): pp.873-878.
- Budía, A., Luis Palmero, J., Broseta, E., Tejadillos, S., Benedicto, A., Queipo, J.A., Gobernado, M. and Fernando Jiménez Cruz, J. Value of semen culture in the diagnosis of chronic bacterial prostatitis: a simplified method. Scandinavian journal of urology and nephrology, 2006; 40(4): pp.326-331.
- Murray, P. Manual of clinical microbiology. 9th ed. Washington D.C.: ASM Press 2007.
- McKechnie, M.L., Hillman, R.J., Jones, R., Lowe, P.C., Couldwell, D.L., Davies, S.C., King, F., Kong, F. and Gilbert, G.L. The prevalence of urogenital micro-organisms detected by a multiplex PCR–reverse line blot assay in women attending three sexual health clinics in Sydney, Australia. Journal of medical microbiology, 2011; 60(7): pp.1010-1016.
- Song, T., Ye, A., Xie, X., Huang, J., Ruan, Z., Kong, Y., Song, J., Wang, Y., Chen, J. and Zhang, J. Epidemiological investigation and antimicrobial susceptibility analysis of ureaplasma species and Mycoplasma hominis in outpatients with genital manifestations. Journal of clinical pathology, 2014; 67(9): pp.817-820.
- Farkas, B., Ostorházi, E., Pónyai, K., Tóth, B., Adlan, E., Párducz, L., Marschalkó, M., Kárpáti, S. and Rozgonyi, F. Frequency and antibiotic resistance of Ureaplasma urealyticum and Mycoplasma hominis in genital samples of sexually active individuals. Orvosi hetilap, 2011; 152(42): pp.1698-1702.
- Al-Dahmoshi, H.O.M. Rapid Detection of Microbial Profile among Women with Vaginitis in Hilla City, Iraq. Journal of Applied Pharmaceutical Science, 2017; 7(02): pp.228-232.
- Zdrodowska-Stefanow, B., Klosowska, W.M., Ostaszewska-Puchalska, I., Bulhak-Koziol, V. and Kotowicz, B. Mycoplasma hominis and Ureaplasma urealyticum infections in male urethritis and its complications. Adv Med Sci, 2006; 51: pp.254-257.
- Kenny, G.E. and Cartwright, F.D. 2. Susceptibilities of Mycoplasma hominis, M. pneumoniae, and Ureaplasma urealyticum to GAR-936, dalfopristin, dirithromycin, evernimicin, gatifloxacin, linezolid, moxifloxacin, quinupristin-dalfopristin, and telithromycin compared to their susceptibilities to reference macrolides, tetracyclines, and quinolones. Antimicrobial agents and chemotherapy, 2001; 45(9): pp.2604-2608.
- Bayraktar, M.R., Ozerol, I.H., Gucluer, N. and Celik, O. Prevalence and antibiotic susceptibility of Mycoplasma hominis and Ureaplasma urealyticum in pregnant women. International Journal of Infectious Diseases, 2010; 14(2): pp.e90-e95.
- Lee, M.Y., Kim, M.H., Lee, W.I., Kang, S.Y. and Jeon, Y.L. Prevalence and Antibiotic Susceptibility of Mycoplasma hominis and Ureaplasma urealyticum in Pregnant Women. Yonsei medical journal, 2016; 57(5): pp.1271-1275.
- Koh, E., Kim, S., Kim, I.S., Maeng, K.Y. and Lee, S. Antimicrobial susceptibilities of Ureaplasma urealyticum and Mycoplasma hominis in pregnant women. Korean Journal of Clinical Microbiology, 2009; 12(4): pp.159-162.
- Taylor-Robinson, D. The role of mycoplasmas in pregnancy outcome. Best Practice & Research Clinical Obstetrics & Gynaecology, 2007; 21(3): pp.425-438.
- Pararas, M.V., Skevaki, C.L. and Kafetzis, D.A. Preterm birth due to maternal infection: causative pathogens and modes of prevention. European Journal of Clinical Microbiology and Infectious Diseases, 2006; 25(9): pp.562-569.
- Samra, Z., Rosenberg, S. and Soffer, Y. In vitro susceptibility of Mycoplasma hominis clinical isolates to tetracyclines, quinolones and macrolides. Diagnostic microbiology and infectious disease, 2002; 44(4): pp.359-361.
© The Author(s) 2017. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.