


ISSN: 0973-7510
E-ISSN: 2581-690X
Sowmya G.S
Klebsiella pneumoniae (K. pneumoniae) is a high-priority antibiotic-resistant pathogen contributing significantly to the global burden of antimicrobial resistance (AMR). Extended-spectrum β-lactamases (ESBLs) and AmpC β-lactamases are major resistance mechanisms commonly observed in K. pneumoniae. The present study aimed to determine the prevalence and distribution of ESBL and AmpC β-lactamase production and to evaluate associated antimicrobial resistance patterns among clinical isolates. A prospective laboratory study was conducted over one year (January-December 2020) in a tertiary care hospital, South India. Total of 100 clinical isolates of K. pneumoniae were included. Identification and antimicrobial susceptibility testing (AST) were performed using the VITEK 2 compact system, while ESBL and AmpC production were detected using standard phenotypic methods. AST demonstrated markedly high resistance rates to carbapenems (meropenem, ertapenem and imipenem), fluoroquinolones (ciprofloxacin), cephalosporins (cefuroxime, ceftriaxone, and cefepime), and β-lactamase inhibitors. Overall, 53% (n = 53) of isolates were ESBL producers, 48% (n = 48) were AmpC producers, while 24% (n = 24) exhibited co-production of both enzymes. The proportion of co-producers represents a considerable subset, suggesting a clinically relevant association with multidrug-resistance. The association between ESBL and AmpC β-lactamase production was found to be statistically not significant (P-value = 0.49). The co-existence of ESBL and AmpC enzymes was associated with a higher resistance burden across multiple antibiotic classes, underscoring its potential impact on therapeutic outcomes. These findings highlight a substantial prevalence of β-lactamase-mediated resistance and emphasize the need for continuous surveillance, implementation of robust antimicrobial stewardship programs, and proper infection control strategies to limit the spread of multidrug-resistant K. pneumoniae.
Klebsiella pneumoniae, Antimicrobial Resistance, AmpC β-lactamase, Extended-Spectrum β-Lactamase, Multidrug-resistance
Antimicrobial resistance (AMR) has emerged as a major global health concern, driven by the rapid evolution of resistance mechanisms and the diminishing effectiveness of available therapeutic agents.1 In healthcare settings, AMR contributes to increased morbidity, mortality, prolonged hospital stays, and escalating treatment costs.2 In 2018, the World Health Organization (WHO) classified Klebsiella pneumoniae as a high-priority pathogen due to its critical role in antibiotic resistance and the urgent need for new therapeutic strategies.3,4 K. pneumoniae, a Gram-negative bacterium belonging to the Enterobacterales family, is a leading cause of nosocomial infections including, surgical site infections, urinary tract infections, ventilator-associated pneumonia, skin & soft tissue infections, intra-abdominal infections, and bloodstream infections.5 K. pneumoniae is also found to be associated with outbreaks in intensive care units (ICUs), leading to further complications in infection control approaches.6
The increased prevalence of antibiotic resistance mechanisms that significantly restrict therapeutic options is one of the major worrying aspects of K. pneumoniae.7 Among these, production of extended spectrum β-lactamases (ESBLs) and AmpC β-lactamases represent a major contributor to β-lactam resistance in K. pneumoniae.8,9 ESBLs, such as TEM, SHV, and CTX-M enzymes, hydrolyze a wide range of β-lactam antibiotics, including cephalosporins (1st-3rd generation), aztreonam, and penicillins and are susceptible to tazobactam and clavulanic acid (β-lactamase inhibitors).10,11 In contrast, AmpC β-lactamases, namely DHA, CMY, and CIT confer resistance to cephalosporins, penicillins, monobactams, and cephamycins and are typically not inhibited by β-lactamase inhibitors.7,12 The co-existence of ESBL and AmpC enzymes further complicates detection and limit therapeutic options, often resulting in multidrug-resistant (MDR) phenotypes and potential treatment failure.13,14 Although, horizontal transfer of ESBL and AmpC β-lactamase genes among Enterobacterales, including K. pneumoniae, Escherichia coli, Proteus spp., and Salmonella spp., facilitates the spread of resistance, potentially leading to poor treatment outcomes and diagnostic failures, particularly in cases of severe infections.13
Virulence factors such as Lipopolysaccharides, capsules, fimbriae, efflux pumps, porins and iron-acquisition systems enhance the pathogenicity of K. pneumoniae, their clinical impact is significantly magnified when combined with β-lactamase-mediated resistance.15 Additionally, overuse of antimicrobial agents, improper infection control measures, and poor sanitation especially in resource-limited settings, encourages the proliferation of β-lactamase-producing K. pneumoniae.16 To address this dilemma, proper surveillance is needed to know the distribution and prevalence of β-lactamase-mediated resistance in local settings.17
Despite increasing reports of ESBL and AmpC production worldwide, there is limited region-specific data on their distribution, co-occurrence, and associated antimicrobial resistance patterns in clinical isolates of K. pneumoniae, particularly in tertiary care settings in India. Furthermore, the clinical implications of co-production remain inadequately explored, creating a significant evidence gap that hinders the development of effective empirical therapy and infection control strategies. In this context, the present study was designed to evaluate the prevalence and distribution of ESBL and AmpC β-lactamases among clinical isolates of K. pneumoniae and to analyze their antimicrobial susceptibility patterns. By focusing on co-occurrence and resistance trends, this study aims to provide clinically relevant insights that may support improved antimicrobial stewardship and infection control practices.
Study design and setting
This was a prospective laboratory investigation conducted in the Microbiology Laboratory of a tertiary care hospital, Mysuru, India, from January 2020 to December 2020. The study was approved by the Institutional Ethical Committee, JSS Medical College, with the approval number JSSMC/PG/6929/2019-20 dated 27-01-2020. The study comprised of 100 K. pneumoniae isolates obtained from multiple clinical samples by convenience sampling technique due to financial constraints.
Isolation and identification of Klebsiella pneumoniae
Clinical samples received in the Microbiology laboratory for routine culture and antimicrobial sensitivity testing were processed as per the laboratory standard protocol. Urine samples were cultured on urichrome agar, while other clinical samples were inoculated onto Blood agar and MacConkey agar. After incubation at 37 °C for 18-24 hours, isolates were preliminarily identified based on colony morphology and Gram staining characteristics. Confirmation of Klebsiella pneumoniae identification and antimicrobial susceptibility testing were performed using the VITEK 2 Compact system according to the manufacturer’s instructions. The confirmed isolates were further screened for extended-spectrum β-lactamase (ESBL) and AmpC β-lactamase production.
ESBL detection by combination disc diffusion method
ESBL production was evaluated in accordance with Clinical and Laboratory Standards Institute-2019 (CLSI) guidelines by using cefotaxime (30 µg) and cefotaxime-clavulanate (30 µg/10 µg) antibiotic discs. K. pneumoniae isolates were first lawn cultured on a Mueller-Hinton agar, then cefotaxime (30 µg) and cefotaxime-clavulanate (30 µg/10 µg) antibiotic discs were placed centre to centre. After overnight incubation at 37 °C, a ≥ 5 mm increase in a cefotaxime-clavulanate zone size against the zone diameter of the cefotaxime disc was considered as positive for the ESBL production.13,18
AmpC screening by cefoxitin disc test
AmpC β-lactamase production was screened using the cefoxitin disc-based method with Escherichia coli ATCC 25922 as the indicator strain. A lawn culture of the indicator strain was prepared on Mueller–Hinton agar, and discs inoculated with the test organism were placed adjacent to a cefoxitin (30 µg) disc. After overnight incubation at 37 °C, distortion or flattening of the cefoxitin inhibition zone toward the test organism disc was considered indicative of AmpC production.19 Although this method is commonly used for AmpC screening, it may have limited sensitivity in detecting low-level AmpC producers.
Data analysis
All the results obtained from the study were entered into Microsoft Excel. Descriptive statistics were primarily used to summarize the results. Categorical variables, including gender-wise distribution, age-wise distribution, sample-wise distribution, antimicrobial susceptibility testing pattern, and prevalence of ESBL and AmpC β-lactamase production, were described as frequencies (numbers) and percentages (%). McNemar test was used to know the association between ESBL vs AmpC β-lactamase production. A P-value of <0.05 was interpreted as statistically significant value.
Demographic Characteristics and Distribution of Klebsiella pneumoniae isolates
A total of 100 non-duplicate K. pneumoniae isolates recovered from various clinical specimens were included in the study. Preliminary identification was based on colony morphology and Gram staining characteristics, followed by confirmation using the VITEK 2 Compact system. Among the isolates analyzed, 74% (n = 74) were obtained from male patients, while 26% (n = 26) were from female patients. The highest proportion of isolates was observed in the 21-30 years and 41-50 years age groups, with 30% (n = 30) isolates each. This was followed by the 61-70 years age group accounting for 29% (n = 29), the 11-20 years age group with 8% (n = 8), and patients aged ≥81 years with 3% (n = 3) isolates. Analysis of clinical specimen distribution showed that urine samples accounted for the highest number of K. pneumoniae isolates [39% (n = 39)], followed by sputum [27% (n = 27)], endotracheal aspirates [19% (n = 19)], blood [9% (n = 9)], and pus samples [6% (n = 6)].
Antimicrobial susceptibility testing (AST) pattern
The AST of 100 K. pneumoniae isolates showed 100% resistant to piperacillin-tazobactam, cefuroxime, cefuroxime axetil, and ceftriaxone. Sensitivity was observed for fosfomycin 78% (n = 78), tigecycline 73% (n = 73), and 25% (n = 25) for both trimethoprim sulfamethoxazole and amikacin. Interestingly, 15% (n = 15) of the isolates were found to be resistant to colistin. Among the 27 K. pneumoniae isolates from urine samples, 12 isolates were susceptible and 15 isolates were non-susceptible to nitrofurantoin. The detailed antimicrobial susceptibility pattern was depicted in Table.
Table: Antimicrobial Susceptibility Testing pattern of 100 clinical Klebsiella pneumoniae isolates
Antimicrobial agents |
Resistant |
Intermediate |
Susceptible |
|---|---|---|---|
Nitrofurantoin |
15 (15%) |
0 |
12 (12%) |
Trimethoprim sulfamethoxazole |
75 (75%) |
0 |
25 (25%) |
Colistin |
15 (15%) |
85 (85%) |
0 |
Fosfomycin |
9 (9%) |
13 (13%) |
78 (78%) |
Tigecycline |
9 (9%) |
18 (18%) |
73 (73%) |
Ciprofloxacin |
92 (92%) |
3 (3%) |
5 (5%) |
Gentamicin |
81 (81%) |
4 (4%) |
15 (15%) |
Amikacin |
25 (25%) |
50 (50%) |
25 (25%) |
Meropenem |
97 (97%) |
0 |
3 (3%) |
Imipenem |
93 (93%) |
7 (7%) |
0 |
Ertapenem |
90 (90%) |
5 (5%) |
5 (5%) |
Cefepime |
98 (98%) |
1 (1%) |
1 (1%) |
Cefoperazone sulbactam |
86 (86%) |
5 (5%) |
9 (9%) |
Ceftriaxone |
100 (100%) |
0 |
0 |
Cefuroxime axetil |
100 (100%) |
0 |
0 |
Cefuroxime |
100 (100%) |
0 |
0 |
Piperacillin tazobactam |
100 (100%) |
0 |
0 |
Amoxicillin clavulanate |
98 (98%) |
2 (2%) |
0 |
Distribution of Extended spectrum-β-lactamases (ESBLs) and AmpC β-lactamases among Klebsiella pneumoniae isolates
Among the 100 K. pneumoniae clinical isolates, 29 (29%) were identified as ESBL producers alone, 24 (24%) as AmpC producers alone, and 24 (24%) exhibited co-production of both ESBL and AmpC β-lactamases. In total, 53 (53%) of isolates produced ESBLs (Figure 1) and 48 (48%) produced AmpC β-lactamases (Figure 2). For association between ESBL vs AmpC β-lactamase production among the isolates, McNemar test showed Chi-square (χ²) value of 0.47 and P-value 0.49. Hence, no significant association was observed between ESBL vs AmpC β-lactamase production, suggesting that both resistance mechanisms occur at similar frequencies in the study population.
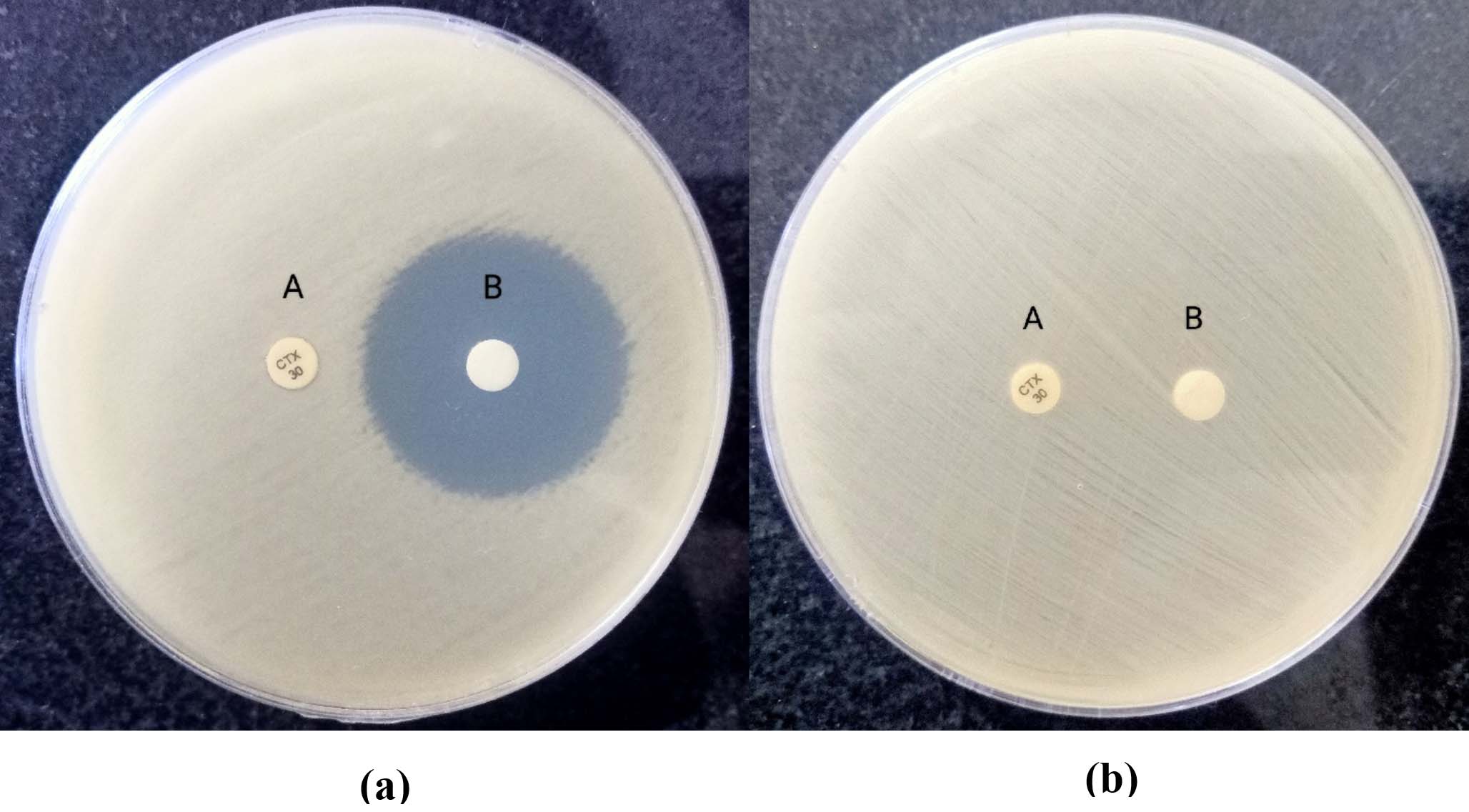
Figure 1. ESBL positive isolate (a) with Cefotaxime (A) zone diameter ≤6 mm and Cefotaxime-clavulanate (B) zone diameter 28 mm. ESBL negative isolate (b) with Cefotaxime (A) zone diameter ≤6 mm and Cefotaxime-clavulanate (B) zone diameter ≤6 mm
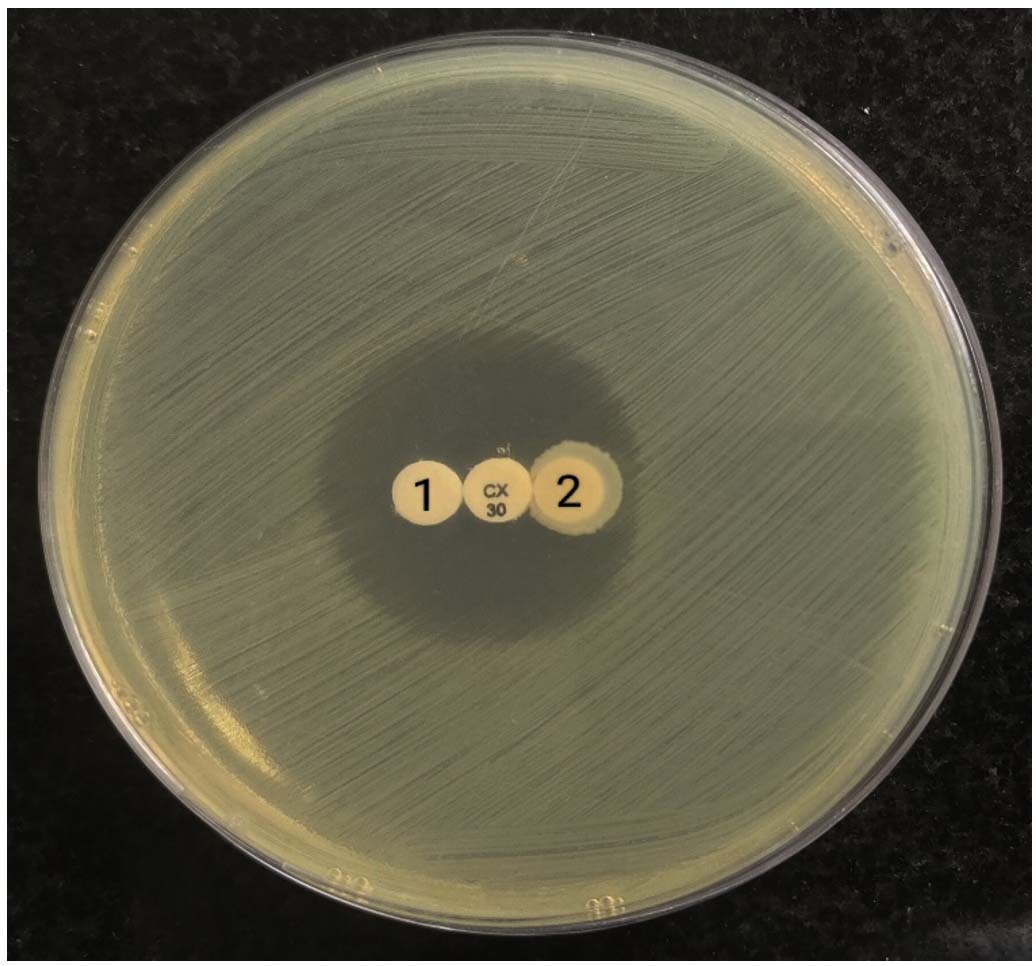
Figure 2. Isolate-2 showed AmpC production (distortion in Cefoxitin zone size) and Isolate-1 was negative for AmpC production (no distortion in Cefoxitin zone size)
Antimicrobial resistance has emerged as a major global public health concern in the 21st century.20 Among Gram-negative pathogens, K. pneumoniae has gained particular importance because of its ability to acquire and disseminate multiple resistance determinants. According to the Antimicrobial Resistance Collaborators group, K. pneumoniae was identified as the third most significant pathogen associated with AMR-related mortality in 2019, contributing to more than 250,000 deaths worldwide.21 The increasing prevalence of extended-spectrum β-lactamase and AmpC β-lactamase-producing strains has further complicated the management of healthcare-associated infections, as these enzymes confer resistance to a broad range of β-lactam antibiotics and are frequently associated with multidrug resistance.22,23
In the present study, a higher proportion of K. pneumoniae isolates were recovered from male patients compared to females, which is consistent with the findings reported by Nirwati et al.24 This predominance may be attributed to greater occupational and community exposure among males, increased healthcare-seeking behavior, and a higher likelihood of hospitalization and associated risk factors, all of which may contribute to increased acquisition and transmission of resistant pathogens. Urine samples constituted the predominant source of isolates, similar to the observations made by Mohsen et al.,25 and Nepal et al.26 The predominance of urinary isolates may be associated with the organism’s ability to colonize the urinary tract, particularly in catheterized patients and individuals with recurrent urinary tract infections.
The antimicrobial susceptibility demonstrated high resistance rates to cephalosporins, β-lactam/β-lactamase inhibitor combinations, carbapenems, and fluoroquinolones. Similar resistance trends have been documented by Helmi et al.,27 and Chethankumar et al.5 The emergence of such resistance patterns may be associated with excessive and inappropriate use of broad-spectrum antibiotics, prolonged hospital stay, empirical antimicrobial therapy, and inadequate infection control practices. In addition, plasmid-mediated transfer of resistance genes among Gram-negative bacteria facilitates the rapid dissemination of resistant strains within healthcare settings. The high resistance observed against carbapenems is particularly concerning, as these agents are often considered last-resort drugs for severe infections caused by MDR organisms. Increasing carbapenem resistance may indicate the possible coexistence of carbapenemase enzymes such as metallo-β-lactamases (MBLs), which further restrict available therapeutic options.14,28
The present study identified a considerable proportion of ESBL (53%) and AmpC (48%) β-lactamase-producing isolates, including strains co-producing both enzymes (24%). Studies conducted by Hou et al.,29 (ESBL 89.5%, AmpC 36.8% and coproduction 31.5%), Bhandari et al.,28 (35.6% AmpC and 28.9% ESBL) and Perera et al.17 (50% ESBL and 19% AmpC) have also reported significant proportion of ESBL and AmpC β-lactamases among K. pneumoniae. However, variations in prevalence rates among studies may result from differences in geographical location, hospital antibiotic policies, infection control practices, sample size, patient population, and distribution of resistance genes. The co-production of ESBL and AmpC enzymes is clinically significant because it not only broadens the resistance profile of the organism but also complicates phenotypic detection. AmpC β-lactamase production may mask ESBL activity, resulting in false-negative detection and inappropriate antimicrobial therapy.30 Furthermore, these enzymes are commonly encoded on plasmids and other mobile genetic elements, enabling horizontal transfer between bacterial species and contributing to the rapid spread of MDR pathogens. This highlights the urgent need for continuous surveillance of antimicrobial resistance patterns, early laboratory detection of β-lactamase-producing organisms, and implementation of effective antimicrobial stewardship programs. Rational antibiotic prescribing, strict adherence to infection prevention and control measures, hand hygiene practices, and diagnostic stewardship are essential strategies to reduce the spread of resistant organisms within healthcare facilities.
Overall, the findings of the present study emphasize the significant contribution of K. pneumoniae to the growing burden of antimicrobial resistance, particularly through the production of ESBL and AmpC β-lactamases. The high prevalence of resistant isolates observed in this study underscores the importance of routine screening for β-lactamase production and continuous monitoring of resistance trends to support appropriate therapeutic decisions and improve patient outcomes.
The present study demonstrated a high prevalence of antimicrobial resistance among K. pneumoniae clinical isolates, with substantial production of ESBL and AmpC β-lactamases, including co-production of both enzymes. The occurrence of these resistance mechanisms was associated with reduced susceptibility to multiple commonly used antimicrobial agents, thereby limiting available therapeutic options and increasing the risk of treatment failure. The detection of ESBL and AmpC co-producing isolates in a significant proportion of strains highlights the emerging challenge of multidrug-resistant K. pneumoniae in clinical settings and emphasizes the importance of routine phenotypic screening for β-lactamase production in microbiology laboratories.
The findings of this study contribute valuable regional data on the prevalence and resistance patterns of ESBL and AmpC-producing K. pneumoniae, which may aid clinicians in selecting appropriate empirical therapy and support hospital infection control policies. Strengthening antimicrobial stewardship programs, enforcing strict infection prevention and control measures, and promoting rational antibiotic usage are essential to limit the dissemination of resistant strains. In addition, continuous surveillance and early detection of resistant isolates are necessary to monitor evolving resistance trends and improve patient management. Future studies involving larger sample sizes and molecular characterization of resistance genes are recommended to better understand the genetic mechanisms responsible for ESBL and AmpC production and their transmission dynamics among healthcare-associated pathogens.
ACKNOWLEDGMENTS
The authors would like to acknowledge the Department of Microbiology, JSS Medical College and the management of JSS Academy of Higher Education and Research for permitting us to conduct this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
VBC, MRR RSG, SGS, RPM, and NSM conceptualized and designed the study. WAHA performed experiments. VBC, PC, MRR, WAHA, RSG, SGS, RPM, and NSM performed result analysis. VBC, MRR and RSG performed project administration. SGS, RPM, MRR, NSM, VBC and RSG supervised the study. PC performed data curation, interpretation and wrote the manuscript. PC, MRR, WAHA, VBC, RSG, SGS, RPM, and NSM reviewed the manuscript. MRR and PC revised the manuscript. All authors read and approved the final manuscript for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
The study was approved by the Institutional Ethical Committee, JSS Medical College, with the approval number JSS/MC/PG/6929/2019-20, dated 27/01/2020.
- Subramanya SH, Bairy I, Metok Y, Baral BP, Gautam D, Nayak N. Detection and characterization of ESBL-producing Enterobacteriaceae from the gut of subsistence farmers, their livestock, and the surrounding environment in rural Nepal. Sci Rep. 2021;11(1):2091.
Crossref - Desta K, Woldeamanuel Y, Azazh A, et al. High Gastrointestinal Colonization Rate with Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae in Hospitalized Patients: Emergence of Carbapenemase-Producing K. pneumoniae in Ethiopia. PLoS ONE. 2016;11(8):e0161685.
Crossref - Taraghian A, Esfahani BN, Moghim S, Fazeli H. Characterization of Hypervirulent Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae Among Urinary Tract Infections: The First Report from Iran Infection and Drug Resistance. 2020;;13:3103-3111.
Crossref - Ejaz H. Analysis of diverse β-lactamases presenting high-level resistance in association with OmpK35 and OmpK36 porins in ESBL-producing Klebsiella pneumoniae. Saudi J Biol Sci. 2022;29(5):3440-3447.
Crossref - Chethankumar P, Tejashree A, Murthy NS, Rao MR. In Vitro Synergistic Effect of Colistin with Fosfomycin Against Carbapenem-Resistant Klebsiella pneumoniae. Cureus. 202416(8):e66295.
Crossref - Guo X, Cao Z, Dai Z, et al. Antimicrobial Susceptibility and Molecular Epidemiology of Multidrug-Resistant Klebsiella pneumoniae in Central China. Jpn J Infect Dis. 2016;70(3):229-234.
Crossref - Realegeno S, Ward K, Garner OB, Yang S. Deceiving Phenotypic Susceptibility Results on a Klebsiella pneumoniae Blood Isolate Carrying Plasmid-Mediated AmpC Gene blaDHA-1. Front Cell Infect Microbiol. 2021;11:561880.
Crossref - Azimi L, Erajiyan G, Talebi M, et al. Phenotypic and Molecular Characterization of Plasmid Mediated AmpC among Clinical Isolates of Klebsiella pneumoniae Isolated from Different Hospitals in Tehran.J Clin Diagn Res. 2015;9(4):DC01-3.
Crossref - Hertz FB, Jansaker F, Okon KO, et al. ESBL production in Escherichia coli and Klebsiella pneumoniae isolates from Nigeria. MicrobiologyOpen. 2019;8(9):mbo3.816.
Crossref - Cheddie P, Dziva F, Akpaka PE. Detection of a CTX-M group 2 beta-lactamase gene in a Klebsiella pneumoniae isolate from a tertiary care hospital, Trinidad and Tobago. Ann Clin Microbiol Antimicrob. 2017;16(1):33.
Crossref - Aila NAE, Laham NAA, Ayesh BM, Naas T. Fecal carriage of extended-spectrum β-lactamase-producing enterobacterales from hospitals and community settings in Gaza Strip, Palestine. BMC Microbiol. 2023;23(1):376.
Crossref - Santiago GS, Goncalves D, Da Silva Coelho I, De Mattos De Oliveira Coelho S, Ferreira HN. Conjugative plasmidic AmpC detected in Escherichia coli, Proteus mirabilis and Klebsiella pneumoniae human clinical isolates from Portugal. Braz J Microbiol. 2020;51(4):1807-1812.
Crossref - Rizi KS, Mosavat A, Youssefi M, et al. High prevalence of blaCMY AmpC beta-lactamase in ESBL co-producing Escherichia coli and Klebsiella spp. clinical isolates in the northeast of Iran. J Glob Antimicrob Resist. 2020;22:477-482.
Crossref - Salvia T, Dolma KG, Dhakal OP, Khandelwal B, Singh LS. Phenotypic Detection of ESBL, AmpC, MBL, and Their Co-occurrence among MDR Enterobacteriaceae Isolates. J Lab Physicians. 2022;14(03):329-335.
Crossref - Lee MMY, Kuan NL, Li ZY, Yeh KS. Occurrence and characteristics of extended-spectrum β-lactamase- and pAmpC-producing Klebsiella pneumoniae isolated from companion animals with urinary tract infections. PLoS ONE. 2024;19(1):e0296709. Crossref
- Diriba K, Awulachew E, Tekele L, Ashuro Z. Fecal Carriage Rate of Extended-Spectrum Beta-Lactamase-Producing Escherichia coli and Klebsiella pneumoniae Among Apparently Health Food Handlers in Dilla University Student Cafeteria. Infect Drug Resist. 2020;13:3791-3800.
Crossref - Perera PDVM, Gamage S, De Silva HSM, et al. Phenotypic and genotypic distribution of ESBL, AmpC β-lactamase and carbapenemase-producing Enterobacteriaceae in community-acquired and hospital-acquired urinary tract infections in Sri Lanka. J Glob Antimicrob Resist. 2022;30:115-122.
Crossref - Kazemian H, Heidari H, Ghanavati R, et al. Phenotypic and Genotypic Characterization of ESBL-, AmpC-, and Carbapenemase-Producing Klebsiella pneumoniae and Escherichia coli Isolates. Med Princ Pract. 2019;28(6):547-551.
Crossref - Ashok AK, Jaryal SC, Thakur K, Sood A, Gupta PK, Thakur S. Detection of Inducible and Non-inducible (constitutive) AmpC β-lactamase-producing Gram-Negative Bacteria among Family Enterobacteriaceae by Two Phenotypic Methods-Disk Antagonism Test (DAT) and AmpC disk Test at a Tertiary Care Hospital, Himachal Pradesh, India. Int J Curr Microbiol Appl Sci. 2016;5(4):133-139.
Crossref - El-Hariri SA, Saleh F, Moghnieh W, Sokhn ES. Phenotypic and molecular characterization of ESBL producing Escherichia coli and Klebsiella pneumoniae among Lebanese patients. JAC-Antimicrobial Resistance. 2023;5(3).
Crossref - Araujo L, Papa-Ezdra R, Avila P, et al. Great Plasticity in a Great Pathogen: Capsular Types, Virulence Factors and Biofilm Formation in ESBL-Producing Klebsiella pneumoniae from Pediatric Infections in Uruguay. Antibiotics. 2024;13(2):170.
Crossref - Palmieri M, Schicklin S, Pelegrin AC, et al. Phenotypic and Genomic Characterization of AmpC-Producing Klebsiella pneumoniae From Korea. Ann Lab Med. 2018;38(4):367-370.
Crossref - Seo KW. Development of a Method for the Fast Detection of Extended-Spectrum β-Lactamase- and Plasmid-Mediated AmpC β-Lactamase-Producing Escherichia coli and Klebsiella pneumoniae from Dogs and Cats in the USA. Animals. 2023;13(4):649.
Crossref - Nirwati H, Sinanjung K, Fahrunissa F, et al. Biofilm formation and antibiotic resistance of Klebsiella pneumoniae isolated from clinical samples in a tertiary care hospital, Klaten, Indonesia. BMC Proceedings. 2019;13(S11):20.
Crossref - Mohsen SMY, Hamzah HA, Al-Deen MMI, Baharudin R. Antimicrobial Susceptibility of Klebsiella pneumoniae and Escherichia coli with Extended-Spectrum β-lactamase-associated Genes in Hospital Tengku Ampuan Afzan, Kuantan, Pahang. Malays J Med Sci. 2016;23(2):14-20.
- Nepal K, Pant ND, Neupane B, et al. Extended spectrum beta-lactamase and metallo beta-lactamase production among Escherichia coli and Klebsiella pneumoniae isolated from different clinical samples in a tertiary care hospital in Kathmandu, Nepal. Ann Clin Microbiol Antimicrob. 2017;16(1):62.
Crossref - Helmi UM, Desa MNM, Taib NM, Jamaluddin TZMT, Masri SN. Multiple ambler class A ESBL genes among Klebsiella pneumoniae isolates in a Malaysian district hospital. Trop Biomed. 2016;33(1):109-119
- Bhandari A, Khatiwada S, Sharma A, et al. Prevalence of drug resistant Enterobacteriaceae in a Nepalese tertiary care hospital. PLOS Global Public Health. 2024;4(1):e0000858.
Crossref - Hou XH, Song XY, Ma XB, Zhang SY, Zhang JQ. Molecular characterization of multidrug-resistant Klebsiella pneumoniae isolates. Braz J Microbiol. 2015;46(3):759-768.
Crossref - Oberoi L, Singh N, Sharma P, Aggarwal A. ESBL, MBL and AMPC lactamases producing superbugs – havoc in the intensive care units of Punjab India. J Clin Diagn Res. 2013;7(1):70-73.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.