

ISSN: 0973-7510
E-ISSN: 2581-690X
Dengue fever represents an increasing arboviral public health concern in a significant endemic population situated in tropical and subtropical regions globally, exhibiting different levels of clinical manifestation. This research focused on examining the clinical and laboratory dynamics associated with the four dengue serotypes. This cross-sectional study was conducted in the Department of Microbiology Laboratory, Adesh Institute of Medical Sciences and Research, Adesh University, Bathinda, Punjab, India. Blood samples from all clinically dengue suspected patients were received from various Department of AIMSR hospital, between the period of August 2024 to July 2025. Samples were tested for NS1Ag, IgM and IgG by ELISA method. Dengue serotypes were detected by using RT-PCR at BSL-III laboratory of AIMSR hospital. During the study period, 378 samples were tested among which 39 were positive for one or more dengue parameters by ELISA method. 15 (38.46%) samples were positive for NS1Ag and 3 (7.69%) were positive for IgM only. Prevalence of Dengue was found to be (39) 10.30%. Among the 39 ELISA positive samples, prevalence of dengue serotypes amplified by RT-PCR. DENV-2 (51.28%) was most predominant serotypes. Other serotypes were significantly less common, with DENV-1 and DENV-3 identified in 7.69% each, and DENV-4 in 2.56%. 10.25% of cases showed co-infection with DENV-2 + DENV-3 serotypes, whereas 5.12% of cases exhibited co-infection with DENV-1 + DENV-2 and DENV-1 + DENV-3 serotypes each, DENV-3 + DENV-4 and all four-serotype identified in a single case accounting for 2.56% each. Most of the dengue patients in our study were residents of Punjab. Our study revealed that DENV-2 is the most common serotype with maximum severity. Dengue was more frequently diagnosed in females than males.
Dengue, Dengue Fever, Dengue Shock Syndrome, Platelet
The dengue virus is a member of the genus Flavivirus of the family Flaviviridae. These vector-borne diseases have drawn great concern worldwide particularly in tropical and subtropical regions because of their recurring outbreaks.1,2 Dengue fever, also known as breakbone fever, is an infectious tropical disease transmitted by Aedes mosquitoes, particularly A. aegypti and A. albopictus.3 There are four serotypes of the virus and referred to as DENV-1, DENV-2, DENV-3, and DENV-4, All four serotypes can cause the complete spectrum of disease. Dengue hemorrhagic fever (DHF) occurs when a person previously infected with one type of dengue serotype gets reinfected with different strain of Dengue virus.4
The World Health Organization (WHO) consider dengue as a major global public health challenge in the tropic and subtropic nations. In 2024, the World Health Organization documented 7.6 million instances of dengue, with 3.4 million being verified cases, over 16,000 severe cases, and over 3,000 deaths. At present, there are 90 nations experiencing ongoing dengue spread in 2024, although not all cases have been recorded officially.5,6 In India, in the year 2025, a total of 113,450 cases were reported, out of which 95 deaths were documented. Maximum morbidity and mortality documented from Kerala and Tamil Nadu.7 The first reported case of dengue like illness was reported from Madras (India) in 1780 and the first virologically proved epidemic of dengue shock syndrome (DSS) or dengue fever (DF) in India occurred in Kolkata and Eastern Coast of India in 1963-1964.8
Aims and objectives
The aim and objective of this study was to find the prevalence of Dengue serotypes and severity of dengue infections among various serotypes and to correlate the serotype with the degree of thrombocytopenia and total leucocytes count.
Study location
The study was conducted in the Laboratory, Department of Microbiology, Adesh Institute of Medical Science and Research (AIMSR), Adesh University (AU), Punjab.
Molecular testing: Reverse Transcription – Polymerase Chain Reaction (RT-PCR) was done at Biosafety Level 3 (BSL-III) laboratory of AIMSR hospital. The study was carried out after getting the approval letter from AIMSR Research Committee with Ref. No. AIMSR/MC/Estt/620 and Ethics Committee for Biomedical and Health Research, Adesh University, Bathinda with Ref. No. AU/EC_BHR/2k24/66.
Study design and duration of study
A cross-sectional study was conducted on 39 patients with dengue, confirmed by Enzyme-Linked Immunosorbent Assay (ELISA) against dengue-specific non-structural protein 1 (NS1Ag) antigen, Immunoglobulin M (IgM), and Immunoglobulin G (IgG). The study was conducted from August 2024 to July 2025 in AIMSR.
Selection of patients
All dengue suspected patients, blood samples were collected from people of all ages. ELISA test was performed and those found to be positive for any parameter of dengue (NS1Ag/IgM/IgG) were further tested by RT-PCR for detection of dengue serotypes. Those samples were negative by ELISA, considered as dengue negative. Clinical history, Complete Blood Cell (CBC), Liver Function Test (LFT) and Renal Function Test (RFT) parameters of patient was taken and recorded on a performa.
Inclusion criteria
All age groups, freshly collected, proper labelled, received from various inpatient/outpatient departments with patient consent agreement, blood samples were included in the study.
Exclusion criteria
Those blood samples were inadequate, leaked, without patient consent agreement were excluded. Patients suffering with leukemia or other hematologic disorders also excluded. All ELISA negative samples excluded for further detection of dengue serotypes by RT-PCR.
Methodology
All dengue suspected patients, blood samples were received in yellow colour Serum Separation Tube (SST). The samples were properly checked and those sample falling in inclusion criteria were included in the study. Then samples were allowed to clotted after which they were centrifuged at 3,000 RPM for 10 minutes to obtain the serum for Dengue ELISA (NS1Ag, IgM and IgG). Serum samples found positive by ELISA were stored and RT-PCR was done to detect dengue serotypes. Complete Blood Count (CBC) and biochemical analysis was done at Hematology and Biochemistry Department of Central Laboratory AIMSR Hospital.
Laboratory evaluation required
Total Leucocyte Count (TLC), Differential Leucocyte Count (DLC), platelet count, blood urea, serum creatinine, Aspartate Aminotransferase/Serum Glutamic-Oxaloacetic Transaminase (AST/SGOT), Alanine Aminotransferase/Serum Glutamate Pyruvate Transaminase (ALT/SGPT), Total protein and serum albumin were obtained at admission. The dengue serotype was confirmed by RT-PCR for which RNA was extraction by QIAGEN kit and amplification was done with Bio-Rad RT-PCR thermocycler by Genes2Me Pvt. Ltd., RT-PCR kit.
Hematological and biochemical profiling
To keep track of how the illness developed, hematological and biochemical tests were conducted multiple times during the hospital stay. These evaluations took place 3-4 days after symptoms began and were carried out again as needed based on clinical assessments. Hematological assessments were performed using Beckman Coulter analysis system (unicel DxH 800). Standard quality control procedures were followed as per manufacturer guidelines. Biochemical tests were conducted on fresh serum samples using a fully automated biochemistry analyzer. The comprehensive metabolic panel included Liver Function Test (LFT) Such as ALT, AST, total protein levels, and bilirubin levels. Renal Function Tests were (RFT) such as serum creatinine, blood urea, and Uric acid.
Statistical analysis
Statistical analyses were conducted using IBM SPSS Statistics Software version 30.0.0.0 (172) and Microsoft Excel. Descriptive statistics like means, Standard Deviation (SD), Ranges were calculated for demographic variables, clinical characteristics, hematological and biochemical parameters stratified by dengue serotype. Pearson test was used to analyze laboratory parameters between dengue-positive and dengue-negative groups, P-value 0.05 was considered significant. In the study, dengue negative patients selected as control group. They matched same age and sex groups (individual matching).
Characteristics and demographics of the study population
During the study period from August 2024 to July 2025 a total of 378 dengue suspected samples were received from various departments of AIMSR Hospital. 214 (56.62%) samples were received from males and 164 (43.38%) from female patients. Out of these 378, 39 (10.30%) were dengue positive by ELISA and 304 (89.69%) were dengue negative by ELISA. Among 39 dengue-positive patients, 15 (38.46%) were positive only for NS1Ag, (02) 5.12% were positive for IgM only, 01 (2.56%) was positive only for IgG, 06 (15.38%) were positive for both NS1Ag + IgM, 04 (10.25%) were IgM + IgG positive and 07 (17.94%) were NS1Ag + IgM + IgG positive. Out of 39 Dengue positive samples by ELISA, 19 (48.71%) were of male patients and 20 (51.28%) were of female patients. In the study, highest prevalence was observed in age group 10-20 (23.07%) years followed by other age groups patients shown in Figure.
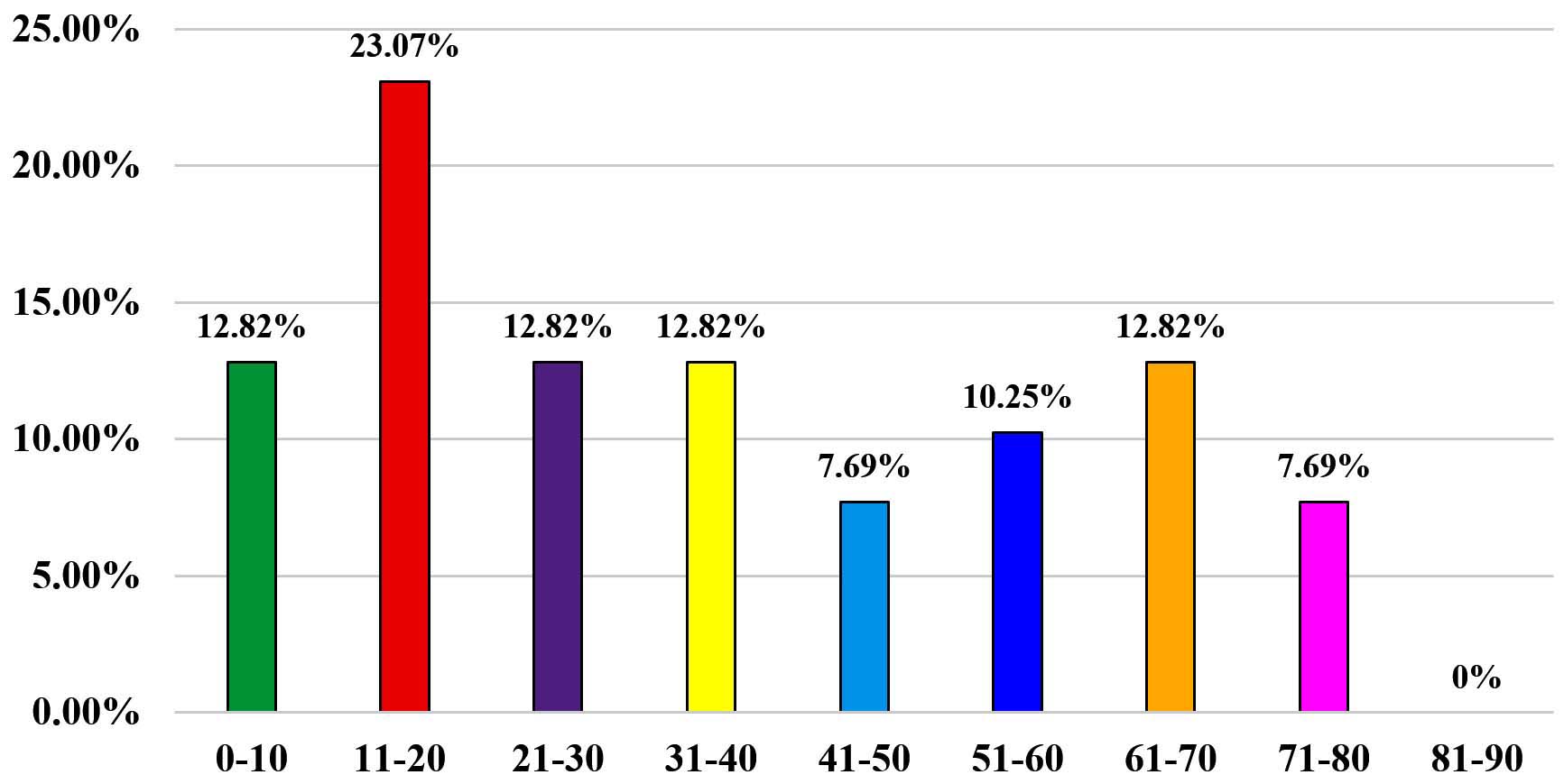
Figure. Age-wise distribution of dengue prevalence
In the present study, among 39 dengue confirmed positive samples by ELISA, association of dengue infection, negative relationship seen in TLC and PLT (<0.001), PLT, SGOT/AST (0.105), SGPT/ALT (0.078), Total protein (<0.05), blood urea (0.141), creatinine (0.103), and uric acid (-0.097). The overall association of laboratory findings between the dengue positive and negative groups is shown in Table 1.
Table (1):
Hematological and biochemical findings in study participants
Parameters |
Case, dengue positive (n = 39) Median (Q3-Q1) |
Control, dengue negative (n = 39) Median (Q3-Q1) |
P-value |
|---|---|---|---|
Age |
31 (57-15) |
40 (60-24) |
0.330 |
RBC (x106 Cells/µL) |
4.49 (4.87-3.81) |
4.17 (4.87-3.7) |
0.310 |
TLC (x103 /µL) |
5.80 (1.10-3.40) |
8.80 (1.09-6.50) |
|
Neutrophil (%) |
61.8 (72.5-52.6) |
71.8 (80.1-56.6) |
0.241 |
Lymphocyte (%) |
27.5 (35-18.3) |
19 (33-11.2) |
0.060 |
Monocyte (%) |
8 (9.2-6.2) |
7.1 (9.4-4.9) |
0.072 |
Eosinophil (%) |
0.7 (1.6-0) |
0.4 (1.3-0.1) |
0.104 |
Basophils (%) |
0.4 (0.8-0) |
0.4 (0.5-0.1) |
0.063 |
Platelets (x103 /µL) |
100 (150-36) |
142 (244-525) |
|
Urea (mg/dl) |
28.5 (45-21) |
26 (58-19) |
0.141 |
Creatinine (mg/dl) |
0.92 (1.17-0.76) |
0.7 (1.7-0.5) |
0.103 |
Uric acid (mg/dl) |
4.65 (6.7-3.6) |
3.9 (7.7-3.4) |
0.097 |
Total bilirubin (mg/dl) |
0.6 (1.4-0.4) |
0.6 (0.9-0.4) |
0.017 |
Total protein (gm/dl) |
6.2 (7.2-5.5) |
6.3 (6.9-5.8) |
|
AST (U/L) |
104 (231-48) |
49 (137-24) |
0.105 |
ALT (U/L) |
75 (292-34) |
45 (75-21) |
0.078 |
RBC: Red Blood Cell, TLC: Total Leukocyte Count, AST: Aspartate Aminotransferase, ALT: Alanine Aminotransferase
Clinical features
This study analyzed the clinical characteristics of 39 dengue-positive patients. Fever was the most common symptom in all 38 cases (97.43%) followed by headache 32 (82.05%), myalgia 28 (71.79%), chills 26 (66.66%), and nausea and vomiting 22 (56.41%). Abdominal pain was reported in 18 (46.1%) of the cases, whereas diarrhea was observed in 10 (25.64%) of the patients. Mucosal bleeding was present in 05 (12.80%) cases. Less frequent symptoms included rash 05 (12.870%) and eye pain 03 (7.69%).
Hematological profiling
Hematological analysis indicated prevalent anemia, with 42.2% of men and 33.33% of females showing low hemoglobin levels. A WBC count below the lower limit was observed in 14.61% of the patient’s suggesting leukopenia. Elevated hematocrit was observed in 29.36% of men and 18.84% of females, suggesting possible polycythemia or dehydration. Thrombocytopenia was observed, in 67.98% of the patients having platelet counts below the normal threshold. Neutropenia was identified in 21.91% of the patients, while most lymphocyte counts were normal or low, with only 8.43% showing possible lymphocytosis. Table 2 shown hematological parameters in dengue patients.
Table (2):
Hematological Parameters in Dengue Patients
Parameter |
Mean ± SD (Q3-Q1) |
Range |
|---|---|---|
Platelet Count (x103 /µL) |
105 ± 077 (1.50-0.36) |
0.28-1.82 |
White Blood Cell Count (x103 /µL) |
8.40 ± 7.08 (0.111-0.340) |
1.32-15.48 |
Hemoglobin (g/dL) |
12.26 ± 2.65 (14-10.6) |
9.61-14.91 |
Neutrophil (%) |
61 ± 14 (72.5-52.6) |
47-75 |
Lymphocyte (%) |
28.11 ± 13.69 (35-18.3) |
14.4-41.8 |
Monocyte (%) |
7.67 ± 2.86 (9.2-6.2) |
4.81-10.53 |
Eosinophil (%) |
1.24 ± 1.79 (1.6-0) |
0-3 |
Biochemical profiling
In our study, biochemical analysis revealed that 84.83% of the patients maintained normal total serum bilirubin levels, whereas 15.16% exceeded the upper limit. Elevated ALT levels were observed in 75.84% of patients, exceeding the normal threshold of 42 IU/L, and AST levels were above the normal range in 60.11% of patients. In contrast, serum creatinine and blood urea nitrogen remained within normal limits for most patients with 10.11% and 20.22%, respectively, exceeding these values. 74.71% of patients had total protein levels at or above the standard lower limit of 6.4 mg/dl. Table 3 shown comparison of hematological and biochemical findings in dengue positive patients.
Table (3):
Comparison of hematological and biochemical findings in NS1Ag, IgM, and NS1Ag + IgM & NS1Ag + IgM + IgG positive dengue patients
Parameters |
NS1Ag only (n = 15) Median (Q3-Q1) |
Both NS1Ag + IgM (n = 6) Median (Q3-Q1) |
NS1Ag + IgM + IgG (n = 7) Median (Q3-Q1) |
|---|---|---|---|
Age |
27 (50-17) |
17 (31-9) |
50 (61-30) |
Hemoglobin (g/dL) |
12.9 (14.1-8.0) |
12.95 (14.1-12.0) |
14.0 (16.1-12.1) |
RBC (x106 Cells/µL) |
4.45 (4.78-3.77) |
4.72 (5.01-4.46) |
4.76 (5.02-4.18) |
TLC (x103/µL) |
4.50 (7.40-3.20) |
4.60 (3.40-1.70) |
9.70 (2.2-6.10) |
Neutrophil (%) |
62 (72-52) |
63.2 (82.2-42.9) |
59.3 (68-37) |
Lymphocyte (%) |
27.9 (29.4-16.6) |
28.95 (50.5-9.5) |
30 (53-22) |
Monocyte (%) |
9.2 (9.6-6.9) |
6.45 (7.4-5.0) |
8 (9-6.7) |
Eosinophil (%) |
0 (0.5-0) |
0.85 (1.6-0.5) |
1.2 (2-0.2) |
Platelets (x103 /µL) |
140 (176-500) |
112 (150-360) |
350 (700-220) |
Urea (mg/dL) |
22 (30-18) |
29 (55.5-21.9) |
33.5 (58-26) |
Creatinine (mg/dL) |
0.7 (0.85-0.55) |
0.8 (0.95-0.45) |
1.15 (1.6-0.9) |
Uric acid |
5.6 (7.15-3.15) |
6.1 (7.1-5.1) |
5 (7.6-4) |
Total bilirubin (mg/dL) |
0.6 (0.9-0.5) |
0.45 (1.2-0.4) |
1.1 (2.0-0.5) |
Total protein (gm/dL) |
6.5 (7.65-5.7) |
7.24 (7.56-6.89) |
6.3 (6.8-5.6) |
AST (U/L) |
90.5 (190-44.5) |
170 (2000-129) |
543.5 (1687-73) |
ALT (U/L) |
50 (123-29.5) |
151.5 (977-103) |
708 (934-197) |
In this study, the Mean ± SD platelet count was 105 ± 077, with a range from 028-1.82 × 10³/µL. Mean ± SD Hemoglobin was 12.26 ± 2.65 g/dL, range from 9.61-14.91 g/dL, and Mean ± SD White Blood Cell (WBC) count was 8.40 ± 7.08 × 10³/µL, with a range from 1.32-15.48 × 10³/µL, as shown in Table 3
In the present study, 20 (51.27%) patients were positive for Dengue IgM antibodies (single + multiple) indicating recent infections. The presence of NS1Ag antigen in 15 (38.46%) of patients supports the acute phase of dengue and dengue IgG antibodies indicating past infections. The mean values of these markers suggest a predominance of recent dengue infections shown in Table 4.
Table (4):
Serological Markers in Dengue Patients
Marker |
Total Positive (%) |
Mean ± SD (Q3-Q1) |
Range |
|---|---|---|---|
NS1 Antigen (single) |
15 (38.46%) |
4.38 ± 2.04 (5.251-0.597) |
2.34-6.42 |
Dengue IgM Antibody (single + multiple) |
20 (51.20%) |
2.45 ± 1.33 (2.536-0.33) |
1.12-3.78 |
Dengue IgG Antibody (single + multiple) |
12 (30.76%) |
2.59 ± 1.40 (1.567-0.12) |
1.19-3.99 |
Distribution of dengue serotype
The prevalence of dengue virus serotypes among the positively tested individuals showed a significant dominance of DENV-2, accounting for 20 (51.28%) of the total cases (Table 5). The other serotypes were significantly less common, with DENV-1 and DENV-3 identified in 3 cases (7.69%) each, and DENV-4 in 1 case (2.56%). Co-infections with multiple dengue virus serotypes were observed in a small proportion of confirmed cases. Specifically, 4 (10.25%) of cases showed co-infection with DENV-2 + DENV-3 serotypes, whereas 02 (5.12%) of cases exhibited co-infection with DENV-1 + DENV-2 and DENV-1 + DENV-3 serotypes each, DENV-3 + DENV-4 and all four-serotype identified in a single case 1 (2.56%) each. These findings indicate that although co-infections are relatively rare, they do occur, with DENV-3 being involved in both types of co-infections detected in this study. In the study among 02 cases of dengue positive none of the four serotypes detected.
Table (5):
Prevalence of dengue serotypes
No. |
Types of serotypes |
Total detected |
Percentage (%) |
|---|---|---|---|
1 |
DENV-1 |
03 |
7.69% |
2 |
DENV-2 |
20 |
51.28% |
3 |
DENV-3 |
03 |
7.69% |
4 |
DENV-4 |
01 |
2.56% |
5 |
DENV-1+2 |
02 |
5.12% |
6 |
DENV-2+3 |
04 |
10.25% |
7 |
DENV-1+3 |
02 |
5.12% |
8 |
DENV-3+4 |
01 |
2.56% |
9 |
DENV-1+2+3+4 |
01 |
2.56% |
Comparison of dengue serotypes with hematological parameters
The present study noted less significant difference in the mean platelet count and WBC among the serotype’s groups. whereas recorded no significant difference in the mean of other blood cells shown in Table 6.
Table (6):
Comparison of mean with hematological parameters based on dengue serotypes
Serotype |
Platelets (Mean ± SD) |
TLC (x103 /µL) (Mean ± SD) |
Neutrophils (%) (Mean ± SD) |
Lymphocytes (%) (Mean ± SD) |
Monocyte (%) (Mean ± SD) |
Eosinophils (%) (Mean ± SD) |
|---|---|---|---|---|---|---|
DENV-1 |
105 ± 166 |
8.70 ± 7.0 |
67.4 ± 12.40 |
22.9 ± 11.66 |
8.1 ± 1.66 |
0.9 ± 0.25 |
DENV-2 |
107 ± 0.77 |
6.5 ± 5.0 |
57.43 ± 16.49 |
29.96 ± 16.79 |
7.26 ± 3.63 |
1.88 ± 2.31 |
DENV-3 |
103 ± 0.89 |
9.1 ± 5.0 |
57.8 ± 13.11 |
32.7 ± 12.85 |
9.2 ± 1.05 |
0.7 ± 1.1 |
DENV-1+2 |
0.90 ± 1.1 |
10.6 ± 4.5 |
64.6 ± 10.32 |
24.75 ± 9.82 |
9.55 ± 0.35 |
0.65 ± 0.35 |
DENV-2+3 |
100 ± 046 |
9.8 ± 8.5 |
67.7 ± 6.03 |
23.75 ± 4.15 |
7.52 ± 2.12 |
0.57 ± 0.43 |
DENV-1+3 |
0.87 ± 0.83 |
11.8 ± 8.3 |
63.2 ± 5.5 |
27.05 ± 5.8 |
8.95 ± 0.63 |
0.1 ± 0.1 |
Dengue is a significant mosquito-borne virus that has undergone considerable changes in its spread over the past quarter-century, posing a serious health issue globally, particularly in tropical and subtropical countries.9
In the present study, out of 343 dengue suspected cases, 39 cases were positive for dengue by ELISA method. Prevalence of dengue recorded 10.30%. Higher seroprevalence (62.26%) was reported by Pachori et al.,10 whereas Deshkar et al. reported 24.49% prevalence,11 31.3% prevalence was reported by Ukey et al., in central India,12 Saini et al. reported 30.6% prevalence in western Maharashtra,13 Sood S reported 18.99% in Rajasthan, India,14 and 17.7% prevalence was reported by Rao et al., in Andhra Pradesh, India.15 Singh et al., reported less prevalence of dengue (3.25%).16 On the basis of previous studies, we observed that the prevalence of dengue varies across different geographical areas, which depends on study inclusion criteria and environmental factors.
In the present study, out of 39 dengue positive cases, 23.07% cases were from the age group of 11-20 years, followed by 12.82% cases in the age groups of 0-10, 21-30, 31-40 & 61-70 years. Srinivas et al. in Andhra Pradesh, India, reported maximum seropositivity (35.84%) in the age group of 0-10 years, followed by age group of 11-20 years (22.66%).15 Ukey et al. in central India reported highest seropositivity of 43.90% in children 0-10 years followed by 31.71% in age group of 15-30 years.12 Deshkar et al. in central India, reported 40.50% cases were from the age group of 0-10 years, followed by 26.71% cases in the age group of 11-20 years.11 In general, dengue infections occur in people of all age groups, but youngsters are more likely to contract them than adults. Children and adults are thought to be more vulnerable to dengue infections because of their intrinsically more permeable vascular endothelium and relatively weaker immune systems.
Our study revealed almost equal number of affected females 20 (51.28%) and males 19 (48.71%). Deshkar et al. reported 2,325 (60.83%) male patient and 1,497 (39.17%) females.11 Karoli et al. reported 58% male patients and 42% females.17 However, approximately equal number of affected females 550 (50.70%) and males 535 (49.30%) were reported by Murugananthan et al. in Sri Lanka.18
The most common clinical feature in suspected dengue cases was fever in most cases (97.43%) followed by headache (82.05%), myalgia (71.79%), chills (66.66%), and nausea and vomiting 22 (56.41%). Abdominal pain was reported in 46.1% of the cases, whereas diarrhea was observed in 25.64% of the patients. Mucosal bleeding were present in 12.80%. Less frequent symptoms included rash 12.87% and eye pain in 7.69% cases. Deshkar et al. reported fever (100%), followed by myalgia in 74.64%, arthralgia in 65.76% and headache in 60.92% cases.11 Other Similar findings were reported by Turbadkar et al., who observed that fever was the major presenting complaint followed by icterus in 26%, myalgia in 26% and headache in 14% in the suspected cases of dengue19 Mandal et al. also reported fever in all cases followed by headache (62.16%), rash (37.84%) and bleeding (13.51%).20 Dengue infection symptoms were depended on immunity of patients.
In our study, mean TLC (Table 1) was within the normal limits in all serotypes of infection. But the mean neutrophil and lymphocyte percentages were significantly different between the groups. Thrombocytopenia and platelet dysfunction was frequently seen in dengue; both strongly associated to the result of the treatment. The WHO recommendations in 2009 were reaffirmed that there is a sudden drop or that the platelet count is less than 150,000. Clinical dengue is indicated by several signs, one of which is blood discharge deteriorating.
The NS1Ag was the only component studied by Kulkarni et al.21 IgM was positively correlated with thrombocytopenia. The present study showed a link between dengue and thrombocytopenia and Sero-markers. This could be attributed to the following factors. The amount of NS1Ag is determined by the viral burden, because the duration of illness rises, as the quantity of NS1Ag lowers. When antibodies begin to develop. The NS1Ag antigen is sequestered into immune cells when it appears complicated.22
Among these 39 individuals, the largest group, accounting for 51.28%, was infected with the second serotype of the dengue virus (DENV-2), as shown in Table 5. There were also 7.69% of patients each infected with DENV-1 and DENV-3, while 2.56% had DENV-4. These findings align with earlier research by Afreen et al., Mishra et al., and Shastri et al. conducted in Delhi, Uttar Pradesh, and Mumbai, respectively.23-25
In the present study, 8 patients (n = 39) were identified as having co-infections with
DENV-2 serotype, 4 patients (10.25%) had co-infections with serotypes 2 and 3, while 2 patients (5.12%) were found to possess both serotype 1 and 2, and one patient with each of serotypes 1 and 3. A prior study by Afreen et al, from Delhi highlighted the first observed cases of simultaneous infections by varying dengue serotypes.23 Our findings are similar with the work of Saxena. The highest incidence of severe dengue cases was seen with DENV-2 (20.6%) and DENV-4 (20%). Racherla et al. determined that DENV-2 was the most common serotype, while DENV-3 and DENV-4 had increased rates of infection.26,27
This research offers important insights into the demographic profiles, circulating serotypes of the dengue virus, and how clinical characteristics relate to laboratory results among patients with dengue at a specialized hospital in Bathinda, Punjab, India. The outcomes of this research highlight the essential importance of public health initiatives in areas where DENV-2 infection rates are high. Our findings reveal the significance of clinical indicators, including alterations in blood and chemical markers, which are vital for the management and forecasting of dengue fever’s progression. As the intensity of dengue fever increased, significant shifts in these indicators were noted, including lower levels of hemoglobin and platelet counts, in addition to higher levels of liver enzymes, bilirubin, and kidney function indicators. These findings can inform treatment strategies and public health actions, ultimately aiming to alleviate the impact of the disease in the affected areas. Initial serotyping in patients with dengue can help monitor the epidemiological trends and help estimate the clinical and laboratory trends of the different serotypes of dengue infection. In addition to this, the prompt diagnosis and treatment of dengue cases, continuous case surveillance and vector control efforts are important to contain the disease in Punjab.
Limitations
This research has few constraints, the most significant being that the samples tested negative by ELISA and were not subsequently verified by RT-PCR because of budget constraints. Because of insufficient patient information, we were unable to conduct follow-up assessment of the patients. We recommend additional studies to recognize the virus serotypes during the outbreak period to connect them with dengue-related complications and to carry out follow-ups on the patients.
ACKNOWLEDGMENTS
The authors are thankful to all the participants who voluntarily agreed to participate in this research work and to the staff of Adesh Hospital Bathinda, for their support.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the AIMSR Research Committee (Ref. No. AIMSR/MC/Estt/620) and Ethics Committee for Biomedical and Health Research, Adesh University, Bathinda (Ref. No AU/EC_BHR/2k24/66).
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Kilpatrick AM, Randolph SE. Drivers, dynamics, and control of emerging vector-borne zoonotic diseases. Lancet. 2012;380(9857):1946-1955.
Crossref - Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature. 2013;496(7446):504-507.
Crossref - Halstead SB. Pathogenesis of dengue: challenges to molecular biology. Science. 1988;239(4839):476-81.
Crossref - Kurane I. Dengue hemorrhagic fever with special emphasis on immunopathogenesis. Comp Immunol Microbiol Infect Dis. 2007;30(5-6):329-340.
Crossref - Gubler DJ. Dengue and dengue hemorrhagic fever. Clin Microbiol Rev. 1998;11(3):480-496.
Crossref - World Health Organization (WHO). Dengue – Global situation. New ed. Geneva, Switzerland: World Health Organization. 2024. https://www.who.int/emergencies/disease-outbreak-news/item/2024-DON518
- National Center for Vector Borne Diseases Control (NCVBDC). Dengue Situation In India; Dengue Cases and Deaths in the Country. 2025. https://ncvbdc.mohfw.gov.in/index4.php?lang=1&level=0&linkid=431&lid=3715
- Gupta N, Srivastava S, Jain A, Chaturvedi UC. Dengue in India. Indian J Med Res. 2012;136(3):373-90.
- Schaefer TJ, Panda PK, Wolford RW. Dengue Fever. [Updated 2024 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2026.
- Pachori P, Sharma GK, Pachori S, Pachori G. A Study of Correlation Between Dengue Serological Markers and Platelet Count in Ajmer Region. Ann of Pathol and Lab Med. 2022;9(2):50-53.
Crossref - Deshkar ST, Raut SS, Khadse RK. Dengue infection in central India: a 5 years study at a tertiary care hospital. Int J Res Med Sci. 2017;5(6):2483-2489.
Crossref - Ukey P, Bondade S, Paunipagar P, Powar R, Akulwar S. Study of seroprevalence of dengue Fever in central India. Indian J Community Med. 2010;35(4):517-519.
Crossref - Saini S, Kinikar AG, Deorukhkar S, Bhalerao D, Roushani SB. Epidemiology and seropositivity of dengue fever cases in a rural tertiary care hospital of western Maharashtra, India. International Journal of Biomedical and Advanced Research. 2013;4(7):473-447.
- Sood S. A hospital based serosurveillance study of dengue infection in jaipur (rajasthan), India. J Clin Diagn Res. 2013;7(9):1917-1920.
Crossref - Srinivas RMS, Pavani K, Manick D, Kareem MA, Vinayaraj EV. Seroprevalence of dengue virus in a tertiary care hospital, Andhra Pradesh, South India. Int J Res Med Sci. 2017;1(4):448-450. https://www.msjonline.org/index.php/ijrms/article/view/2647
- Singh N, Singh AK, Kumar A. Dengue outbreak update in India: 2022. Indian J Public Health. 2023;67(1):181-183.
Crossref - Karoli R, Fatima J, Siddiqi Z, Kazmi KI, Sultania AR. Clinical profile of dengue infection at a teaching hospital in North India. J Infect Dev Ctries. 2012;6(7):551-554.
Crossref - Murugananthan K, Kandasamy M, Rajeshkannan N, Noordeen F. Demographic and clinical features of suspected dengue and dengue haemorrhagic fever in the Northern Province of Sri Lanka, a region afflicted by an internal conflict for more than 30 years-a retrospective analysis. Int J Infect Dis. 2014;27:32-36.
Crossref - Turbadkar D, Ramchandran A, Mathur M, Gaikwad S. Laboratory and clinical profile of dengue: A study from Mumbai. Ann Trop Med Public Health. 2012;5(1):20-23.
Crossref - Mandal SK, Ganuly J, Sil K, et al. Clinical profiles of dengue fever in a teaching hospital of Eastern India. Natl J Med Res. 2013;3(02):173-176.
- Kulkarni RD, Patil SS, Ajantha GS, et al. Association of platelet count and serological markers of dengue infection- importance of NS1 antigen. Indian J Med Microbiol. 2011;29(4):359-362.
Crossref - Hang VT, Nguyet NM, Trung DT, et al. Diagnostic accuracy of NS1 ELISA and lateral flow rapid tests for dengue sensitivity, specificity and relationship to viraemia and antibody responses. PLoS Negl Trop Dis. 2009;3(1):e360.
Crossref - Afreen N, Deeba F, Naqvi I, et al. Molecular investigation of 2013 dengue Fever outbreak from delhi, India. PLoS Curr. 2014;6:
Crossref - Mishra G, Jain A, Prakash O, et al. Molecular characterization of dengue viruses circulating during 2009-2012 in Uttar Pradesh, India. J Med Virol. 2015;87(1):68-75.
Crossref - Shastri J, Williamson M, Vaidya N, Agrawal S, Shrivastav O. Nine year trends of dengue virus infection in Mumbai, Western India. J Lab Physicians. 2017;9(4):296-302.
Crossref - Saxena S. The Laboratory Profile and The Prevalence of Dengue Serotypes at A Tertiary Care Hospital. Eur J Cardiovasc Med. 2024;4(3):1159-1164.
- Racherla RG, Pamireddy ML, Mohan A, et al. Co-circulation of four dengue serotypes at South Eastern Andhra Pradesh, India: A prospective study. Indian J Med Microbiol. 2018;36(2):236-240.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.