


ISSN: 0973-7510
E-ISSN: 2581-690X
HIV, HBV, and HCV can form a pretty challenging trio when they coexist. Managing co-infection is crucial for the overall health of the individual, especially considering the potential impact on the liver. Regular monitoring and appropriate medical care can make a significant difference in the outcome for co-infected patients. To ascertain the seroprevalence of HBV and HCV in individuals with HIV attending the Anti-Retroviral Therapy (ART) center affiliated with a tertiary care hospital in Eluru, Andhra Pradesh. Over an 8-month duration, blood samples were obtained from all the individuals visiting the ART Centre. These samples underwent screening for surface antigen of HBV (HBsAg) and antibodies against HCV (anti HCV) by using rapid card tests. Positive samples were subsequently validated through ELISA testing. Baseline CD4 counts, CD4 count after receiving ART were assessed in individuals with HIV alone and those with coinfection of HBV. HIV viral load tests were conducted in individuals with HIV infection and those with coinfection of HBV, assessing their response to ART. Statistical analysis was applied to examine the obtained results. Among the 4382 participants, the seroprevalence of HBV & HCV was 0.02%. The baseline CD4 values averaged 310 for HIV mono-infection cases and 223 for HIV/HBV co-infection cases, indicating a statistically significant distinction with a P value of 0.03. Likewise, the mean values of the CD4 counts after taking ART in individuals with HIV alone and those with coinfection of HBV were 675 and 599, respectively, with a statistically significant P value of 0.05. The study revealed a substantial enhancement in the effectiveness of ART, as indicated by HIV-1 viral load values, in both mono-infection and co-infection cases. Considering the similarity in the main transmission routes of HIV, HBV, and HCV, it is anticipated that hepatotropic viruses would be present in individuals with HIV infection.
Hepatitis B Virus, Hepatitis C Virus, Human Immunodeficiency Virus, Co-infection, Hepatotropic Viruses
Individuals carrying the Human Immunodeficiency Virus (HIV) are at an increased risk of susceptibility to co-infection with Hepatitis B virus (HBV) and Hepatitis C virus (HCV) due to the similarity in transmission routes.1,2 As per the 2021 Global Progress Report on HIV, Viral Hepatitis, and Sexually Transmitted Infections by the World Health Organization (WHO), only 10% of individuals with chronic hepatitis B virus infection receive a diagnosis, and merely 22% of them undergo treatment. In the case of hepatitis C infection, 21% of individuals are diagnosed, and out of those diagnosed, 62% receive treatment.3 HIV infection-induced compromise in cell-mediated immunity (CMI) results in heightened replication of hepatotropic viruses, expediting the clinical progression of both HBV and HCV infections in individuals living with HIV (PLHIV).4 This has the potential to significantly influence the epidemiology of HBV infection within groups characterized by high HIV seroprevalence.5 Additionally, HIV-reactive patients displayed an increased prevalence of cirrhosis.6 The comprehension of co-infections involving HBV and HCV with HIV holds particular significance in Asian countries, given the heightened baseline prevalence of HBV and HCV.7
In 2019, India fell into the intermediate endemicity zone for HBV infection, with an average prevalence of 4%. The occurrence of HBsAg positivity in the general population ranged from 1.1% to 12.2%, averaging around 3-4%. The estimated prevalence of Anti-HCV antibodies varied from 0.09% to 15%. India bears a substantial portion of the global HBV burden, hosting 10-15% of the world’s carriers, approximately 40 million individuals.8
India has an estimated 2.5 million PLHIV9 majority of whom reside in four southern states of Maharashtra, Andhra Pradesh, Karnataka, and Tamil Nadu.10,11 With 3,21,000 PLHIV, Andhra Pradesh was the second highest prevalence state next to Maharashtra.10 India is home to the world’s second-largest population of chronic hepatitis infection, with an HBsAg prevalence ranging from 2 to 7%.12
The occurrence of HBV and HCV in individuals living with HIV (PLHIV) varies across different geographical areas. Deepinder Chhina conducted a study in North India and reported a prevalence rate of 2.8% of HBV co-infection and 10.6% of HCV co-infection in North India.13 In a study conducted in the south India, Kumarasamy found that HBV co-infection prevalence rate was 6%, while that of HCV co-infection was 4.8%.14 The risk groups and type of exposure involved are other determinants of prevalence.15,16
STIs increase the risk of acquiring HIV which in turn aggravates the risk of HBV and HCV. MSM cases have more incidence of HCV infection. Individuals co-infected with HIV and HBV exhibit elevated HBV viral load, raising the risk of liver cirrhosis and hepatocellular carcinoma.12,17 In individuals with co-infections, the mortality rate related to liver issues was most pronounced in those with lower CD4+ cell counts. Additionally, it doubled after 1996, following the introduction of highly active antiretroviral therapy (HAART).18,19 HIV1 status is assessed and monitored by CD4 lymphocyte count and quantification of HIV1 RNA levels.20
According to WHO recommendation and NACO treatment guidelines the preferred first line drug regimen is TLD – Tenofovir (300 mg) + Lamivudine (300 mg) + Dolutegravir (50 mg) as fixed drug combination (FDC) in a single pill once a day. Tenofovir is known for its nephrotoxicity. Creatinine clearance should be monitored regularly. If the creatinine clearance is >30 ml/min then Abacavir (600 mg), lamivudine (300 mg) and Dolutegravir (50 mg) or Zidovudine lamivudine (300 mg) and Dolutegravir (50 mg) should be given as a substitute for Tenofovir in Patients. Patient should be switched to Second line (Ritonavir boosted Atazanavir + Dolutegravir) and third line (Ritonavir boosted Darunavir + Dolutegravir) drug regimen if treatment failure occurs with the first line drugs.21
Effective introduction of anti-retroviral therapy (ART) has reduced the deaths due to HIV-related illnesses but hepatic failure has become the major cause of mortality.22 HIV infection disrupts the usual course of chronic Hepatitis C acquired through parenteral means, resulting in an accelerated progression towards cirrhosis, hepatocellular carcinoma, and liver failure.23
This cross-sectional study aims to characterize and assess the seroprevalence of HBV and HCV in individuals living with HIV (PLHIV) attending ART centers over an 8-month period at Government General Hospital, Eluru with relation to their CD4 counts and HIV viral loads.
The study was conducted among HIV patients attending the ART center at Government General Hospital, Eluru, spanning from January 2023 to August 2023. The study encompassed a total of 4382 individuals living with HIV (PLHIV). Details of patients like Age, sex, risk factors, baseline CD4 counts before starting ART, and treatment status were recorded. Blood samples were collected for the latest CD4 counts by flow cytometry and HIV 1 viral levels by RNA PCR assay. Rapid testing for screening for hepatitis B surface antigen (HBsAg – OZOTEST) and anti-HCV antibodies (STANDARD Q HCV Ab) was done and positive tests were confirmed by ELISA test (HEPALISA KIT).
The study comprised 4382 participants, with 94.5% (4142) categorized as adults and 5.4% (240) belonging to the pediatric age group (0-15 years) at the time of registration. In the current study, 93 adults (2.12%) were identified with co-infection of HIV and HBV, while 2 cases (0.04%) of HIV and HCV co-infection were observed. Females were more compared to males with M:F ratio of 0.7:1. Transgenders constitute 0.2% of all the participants and the majority of them belong to the 21 to 30 years age group (58.3%) followed by 31 to 40 years age group (28.6%) (Figure 1).
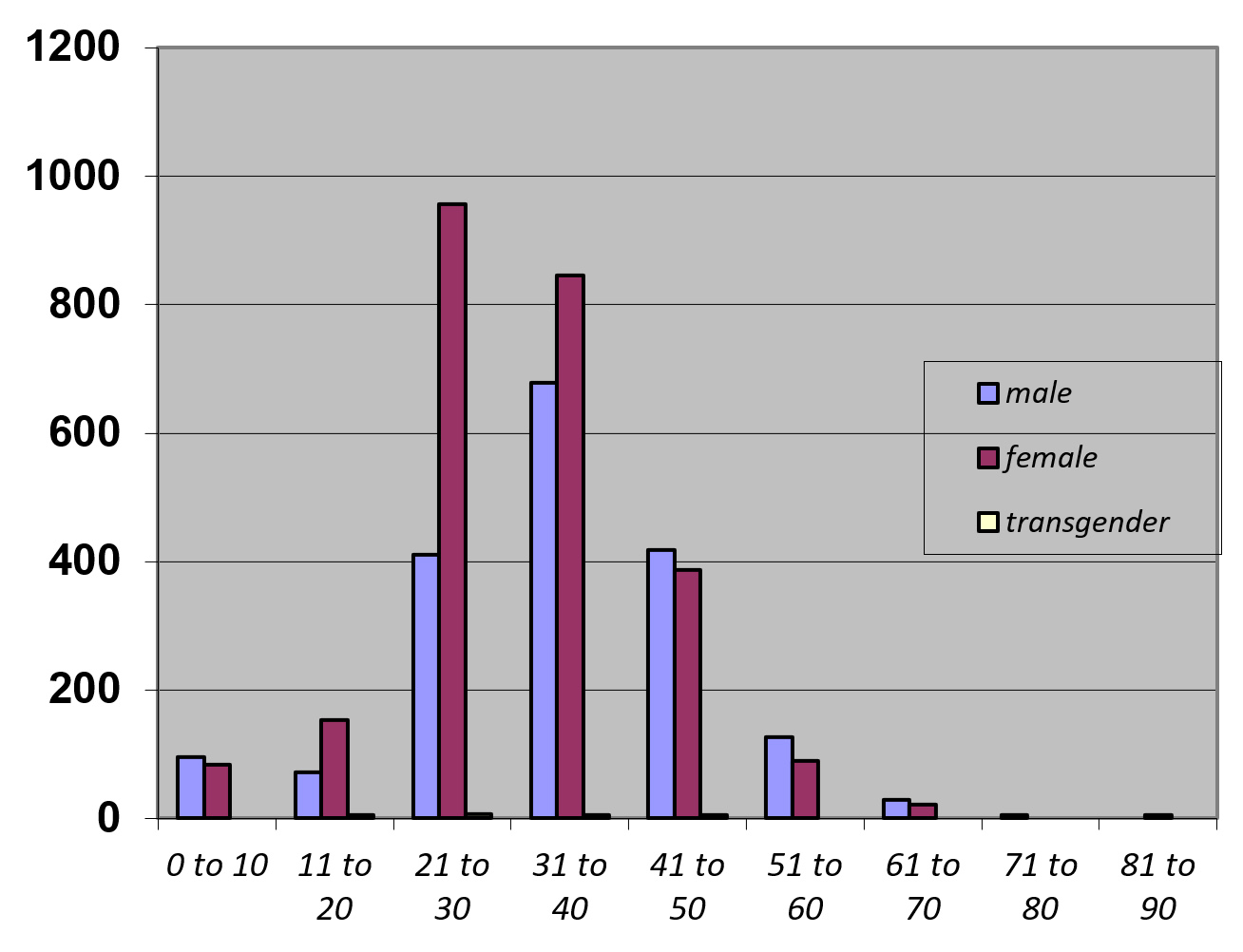
Figure 1. Age-wise distribution of study participants (n = 4382)
Heterosexual transmission (93.2%) was observed as the major risk factor for HIV transmission, followed by mother-to-child transmission (6.1%). other risk factors include female sex workers, homosexuals, unsafe injection practices, and blood transfusions (Table 1).
Table (1):
Risk factors associated with HIV transmission
No. |
Risk factors |
Males |
Females |
Total |
|---|---|---|---|---|
1 |
Mother to child |
137 |
131 |
268 (6.1%) |
2 |
Heterosexual |
1687 |
2398 |
4085 (93.2%) |
3 |
Blood transfusion |
0 |
1 |
1 (
|
4 |
Female sex workers |
0 |
7 |
7 (0.1%) |
5 |
Homosexuals |
5 |
0 |
5 (0.1%) |
6 |
Unsafe injection practices |
2 |
– |
2 (
|
7 |
Transgenders |
– |
– |
12 (0.2%) |
8 |
Unknown |
1 |
1 |
2 (0.1%) |
Total |
1832 |
2538 |
4382 |
A history of blood transfusion was given as a risk factor in a 39-year female patient with a baseline CD4 count of 132 and was started on ART in March 2023. Among the seven female sex workers, the majority belong to the 21 to 30 years age group (57.1%) followed by the 31 to 40 age group (28.6%) (Figure 2).
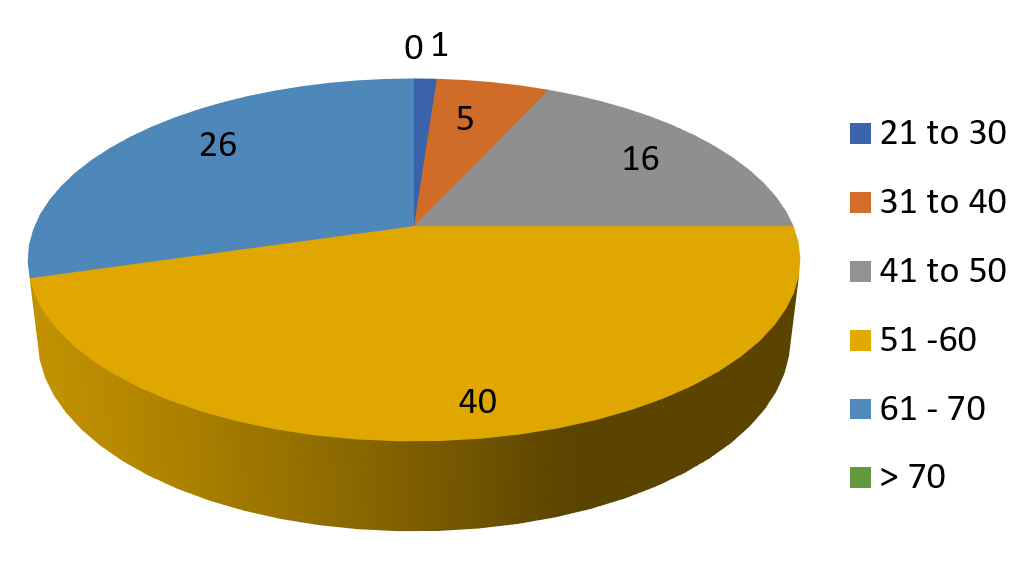
Figure 2. Agewise distribution of HIV & HBV coinfection cases
Maximum cases of HIV & HBV co-infection were observed in the age group of 51 to 60 years age group (43%) followed by 61 to 70 years age group (27%).
4171 (95%) patients were receiving first line drugs. Due to elevated serum creatinine levels 52 (1%) receiving ALD based drugs and 147 (3%) receiving ZLD drugs. 24 patients developed CKD due to tenofovir toxicity. 4 patients were on dialysis. 10 patients were on secondline drugs and 2 were on thirdline drugs. HBV infected and HCV infected people are showing good clinical progression with the drugs. There were no treatment failures as well as cirrhosis.
Among the HIV mono-infection cases, baseline CD4 T-lymphocyte counts done at the beginning of ART compared with the latest CD4 T-lymphocyte counts after the treatment showed a good response to ART. Similar improvement in CD4 counts was observed in all 93 adult individuals having HIV and HBV co-infection (Table 2).
Table (2):
Baseline and latest CD4 counts among adult and pediatric participants in HIV mono-infection and HIV & HBV co-infection
| CD4 counts | HIV mono-infection | HIV & HBV co-infection | ||||
|---|---|---|---|---|---|---|
| Adults | Pediatric | Adults | ||||
| Baseline | Latest | Baseline | Latest | Baseline | Latest | |
| 0 to 200 | 1481 | 132 | 44 | 13 | 38 | 4 |
| 200 to 400 | 1672 | 573 | 69 | 31 | 39 | 21 |
| 400 to 600 | 565 | 1066 | 49 | 57 | 9 | 24 |
| 600 to 800 | 172 | 1062 | 26 | 53 | 4 | 17 |
| 800 to 1000 | 103 | 689 | 20 | 48 | 3 | 17 |
| Above 1000 | 56 | 527 | 32 | 38 | 0 | 10 |
| Total | 4049 | – | 240 | – | 93 | – |
The mean of baseline CD4 values in HIV mono-infection cases is 310 whereas the mean of baseline CD4 counts in HIV/HBV co-infection is 223. This is statistically significant with a P value of 0.03.
The mean of the latest CD4 values in HIV mono-infection cases and HIV/ HBV co-infection was 675 and 599, respectively, and the P value is 0.06 which is statistically significant.
The efficacy of ART, as assessed through HIV-1 viral load values, demonstrated notable enhancement in both mono-infection and co-infection cases in the current study (Figure 3).
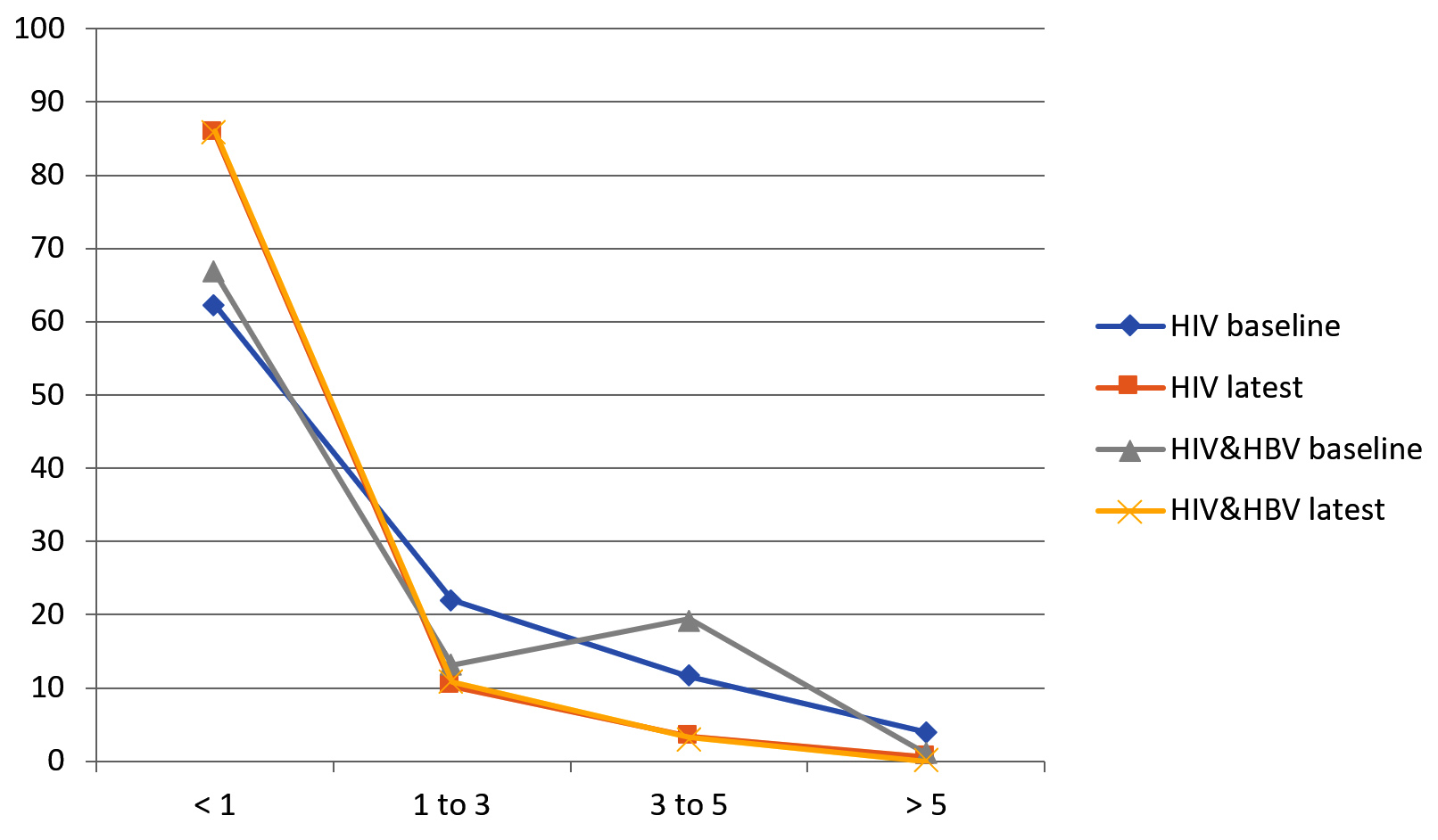
Figure 3. Baseline and latest viral load levels in HIV alone and along with HBV
The goal of the National Viral Hepatitis Control Programme is to combat hepatitis and work towards the nationwide elimination of Hepatitis C by 2030. The program aims for a substantial decrease in the infected population, as well as a reduction in morbidity and mortality related to Hepatitis B and C, including conditions like cirrhosis and Hepatocellular carcinoma (liver cancer).8 The rates of co-infection with HBV and HCV among HIV patients exhibit variability worldwide, contingent on geographic regions and the specific type of exposure.24
According to India’s National AIDS Control Organization (NACO), the estimated HIV prevalence in 2019 was 0.24% among adult males and 0.20% among adult females.9 In the present study on HIV reactive cases, females were significantly higher than males with a ratio of M:F=0.7:1. In the previous study by Saravanan et al., males were more affected than females.25
Among the 4382 PLHIV, the prevalence of HBV co-infection was 2.12% while HCV co-infection was 0.04%. According to India’s 2019 National Action Plan on Viral Hepatitis, the global seroprevalence of HBV and HCV among PLHIV was estimated at 7.35% and 6.26%, respectively. Chakravarty et al. indicated that HBsAg prevalence within the HIV-infected population in India could be estimated to range from 2% to 14%.8 Notably, sexual contact emerged as the predominant transmission route for HIV-HBV co-infection in the country.12 Nearly 99% HBV negative PLHIV were included in the Hep B vaccination at the ART center as per the NHM guidelines. The prevalence of HBV and HCV has exhibited variations across various studies, with potential dependence on both the geographic location and the distinct risk factors prevalent within the study groups (Table 3).
Table (3):
The HBV and HCV prevalence in HIV cases among various studies
No. |
Study |
% of HBV co-infection |
% of HCV co-infection |
|---|---|---|---|
1 |
Saravanan et al.25 |
9 |
2.2 |
2 |
Tripathi et al.26 |
2.25 |
1.61 |
3 |
Mohammedi et al.24 |
14.5 |
72 |
4 |
Anwar et al.27 |
2.13 |
9.19 |
5 |
Jayeetasarkar et al.28 |
8.3 |
– |
6 |
Deepinderchhina et al.13 |
3 |
11 |
7 |
Team et al.29 |
10 |
3.6 |
8 |
Present Study |
2.12 |
0.04 |
Solomon. S noted a substantial occurrence of HIV and HCV co-infection within the population of intravenous drug users (IDU).11 In the present study, only 2 cases of HIV/HCV co-infection were observed as the study group predominantly comprised heterosexually acquired HIV infections than another mode of transmission and correlated with a previous study by Tripathi et al.26
In the present study, 240 pediatric patients were registered for ART. Co-infection was not observed in the pediatric age group which may be due to the effective implementation of the universal immunization program.
Maximum cases of HIV mono-infection were observed in the age group of 31 to 40 followed by 21 to 30 this correlates with the majority of the studies. In the 51-60 age group, HBV/HIV co-infection was predominantly observed, accounting for 43% of the cases. This might be due to the lack of implementation of Hep B vaccination in adults, the chronic nature of HBV infection, and prolonged survival of PLHIV due to effective ART. In contrast, Saravanan et al. found a higher incidence of HIV/HBV co-infection specifically among individuals aged 31 to 40 in their study.
In the current study, there was a disparity of 87 in the mean values of baseline CD4 counts between HIV mono-infection and HIV/HBV co-infection, with a corresponding P value of 0.03. This aligns with the results reported by Saravanan et al.25 In contrast, Paul et al. observed a difference of 100 in their study.20
The current study noted a substantial reduction in HIV viral load values following
ART treatment in individuals with HIV alone and those with coinfection of HBV. Chronic Kidney Disease due to Tenofovir could be prevented by regular monitoring of serum creatinine levels and increasing the awareness in patients by giving counselling.
Understanding co-infection patterns in HIV-reactive patients across different geographical regions is crucial, particularly as they undergo prolonged antiretroviral treatment and require management for co-infections with HBV and HCV. Implementing continuous surveillance, adherence to treatment, health education, and vaccination initiatives for the adolescent age group can contribute to decreasing the incidence of these viral infections. Initiating studies to promptly identify the actual prevalence of HIV and hepatotropic viral infections in specific geographic areas is essential for effective control and management of the situation.
ACKNOWLEDGMENTS
The authors would like to thank Dr. U.V.N. Sastry, MBBS, DA, Medical Officer, ART Centre, Government General Hospital, and Dr. K.V.V. Vijayakumar, ADME Principal, Government Medical College, Eluru for their support.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Government Medical College, Eluru, India, with reference number IEC/2024/001/GMC.ELR.
- Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol. 2006;44(1):S6-9.
Crossref - Thio CL. Hepatitis B and human immunodeficiency virus co-infection. Hepatology. 2009;49(S5):S138-145.
Crossref - World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021: Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact. World Health Organization; 2021. ISBN 978-92-4-003098-5.”Accessed on Febraury 6th ,2023”.
- Ganesan M, Poluektova LY, Kharbanda KK, Osna NA. Human immunodeficiency virus and hepatotropic viruses co-morbidities as the inducers of liver injury progression. World J Gastroenterol. 2019;25(4):398-410.
Crossref - Gilson RJ, Hawkins AE, Beecham MR, et al. Interactions between HIV and hepatitis B virus in homosexual men: effects on the natural history of infection. AIDS. 1997;11(5):597-606.
- Colin JF, Cazals-Hatem D, Loriot MA, et al. Influence of human immunodeficiency virus infection on chronic hepatitis B in homosexual men. Hepatology. 1999;29(4):1306-1310.
Crossref - World Health Organization. Global Hepatitis Report. 2017.
- Ministry of Health and Family Welfare, Government of India. National Action Plan Combating Viral Hepatitis in India; 2019.”Accessed on Febraury 10th ,2023.
- National AIDS Control Organization (NACO), India. HIV Facts & Figures: HIV Estimations 2019. National AIDS Control Organization; 2019. Accessed on Febraury 10th, 2023.
- UNAIDS. Global HIV & AIDS Statistics — Fact Sheet; 2021. UNAIDS; 2021. “Accessed on Febraury 6th ,2023.
- Solomon SS, Srikrishnan AK, Mehta SH, et al. High Prevalence of HIV, HIV/Hepatitis C Virus Coinfection, and Risk Behaviors Among Injection Drug Users in Chennai, India: A Cause for Concern. J Acquir Immune Defic Syndr. 2008;49(3):327-332.
Crossref - Chakravarty R, Pal A. Insights into human immunodeficiency virus-hepatitis B virus co-infection in India. World J Virol. 2015;4(3):255-264.
Crossref - Chhina D, Garg S, Chinna R, Dhiman P, Gupta D. Study of Prevalence of Hepatitis B, Hepatitis C and Other Opportunistic Coinfections in HIV-infected Patients in a Tertiary Care Hospital of North India. Journal of Gastrointestinal Infections. 2020;10(1): 7-10.
Crossref - Kumarasamy N, Solomon S, Flanigan TP, Hemalatha R, Thyagarajan SP, Mayer KH. Natural history of human immunodeficiency virus disease in southern India. Clin Infect Dis. 2003;36(1):79-85.
Crossref - Bhattacharya S, Badrinath S, Hamide A, Sujatha S. Co-infection with hepatitis C virus and human immunodeficiency virus among patients with sexually transmitted diseases in Pondicherry, South India. Indian J Pathol Microbiol. 2003;46(3):495-497. PMID: 15025322.
- Hussain T, Kulshreshtha KK, Sinha S, Yadav VS, Katoch VM., HIV, HBV, HCV and syphilis co-infections among patients attending the STD clinics of district hospitals in Northern India. Int J Infect Dis. 2006;10(5):358-363.
Crossref - Di Bisceglie AM. Hepatitis B and hepatocellular carcinoma. Hepatology. 2009;49(5S):S56-S60.
Crossref - Thio CL, Seaberg EC, Skolasky R Jr, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the multicenter cohort study (MACS). Lancet. 2002;360(9349):1921-1926.
Crossref - Vallet-Pichard A, Pol S. Hepatitis viruses and human immunodeficiency virus co-infection: Pathogenesis and treatment. J Hepatology. 2004;41(1):156-166.
Crossref - Demosthenes JP, Sachithanandham J, Fletcher GJ, et al., Characteristics of Treatment-naïve HBV-Infected Individuals with HIV-1 Coinfection: A Cross-sectional Study from South India. Indian J Med Microbiol. 2019;37(2): 219-224.
Crossref - Ministry of Health and Family Welfare, India. National Guidelines for HIV Care and Treatment 2021. Ministry of Health and Family Welfare; 2021. Accessed on Febraury 20th, 2023.
- Helbert M, Breuer J. Monitoring patients with HIV disease. J ClinPathol. 2000;53:266-272.
Crossref - Soto B, Sanchez Quijano A, Rodrigo L, et al. Human immunodeficiency virus infection modifies the natural history of chronic parentally acquired hepatitis C with an unusually rapid progression to cirrhosis. J Hepatol. 1997;26(1):1-5.
Crossref - Mohammadi M, Talei G, Sheikhian A, et al. Survey of both hepatitis B virus (HBsAg) and hepatitis C virus (HCV-Ab) co-infection among HIV positive patients. Virol J. 2009;6:202.
Crossref - Saravanan S, Velu V, Kumarasamy N, et al. Coinfection of hepatitis B and hepatitis C virus in HIV-infected patients in south India. World J Gastroenterol. 2007;13(37):5015-5020.
Crossref - Tripathi AK, Khanna M, Gupta N, Chandra M. Low Prevalence of Hepatitis B Virus and Hepatitis C Virus Co-infection in Patients with Human Immunodeficiency Virus in Northern India. J Assoc Physicians India. 2007;55:429-431. PMID: 17879496.
- Anwar MS, Nafees M, Nabi U. Sero-prevalence of HCV and associated infections with HIV and HBV among prisoners in Lahore. Biomedica. 2011;27:119-122.
- Sarkar J, Bandyopadhyay B, Chakrabarty R, et al. HIV-HBV Coinfection among Individuals Attending the ICTC of a Tertiary Care Hospital in West Bengal, India. International Scholarly Research Notices. 2013:180150.
Crossref - Teame G, Gebreyesus A, Tsegay E, Gebretsadik M, Adane K. Hepatitis B and C viral coinfections and their association with HIV viral load suppression among HIV-1 infected patients on ART at Mekelle hospital, northern Ethiopia. AIDS Res Ther. 2022;19:57.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.