


ISSN: 0973-7510
E-ISSN: 2581-690X
The global tuberculosis (TB) epidemic is becoming progressively more complex due to the increasing prevalence of multidrug-resistant TB (MDR-TB), particularly with resistance to fluoroquinolones (FQs). This study focuses on identifying genetic mutations in the gyrA and gyrB genes of Mycobacterium tuberculosis that drive FQ resistance. Sputum samples from suspected pulmonary TB patients were analyzed using PCR and sequencing to detect mutations within the quinolone resistance-determining regions (QRDR). The analysis revealed that mutations in gyrA, especially S95T, are prevalent and play a key role in FQ resistance. Additionally, less frequent mutations in gyrB, such as E501D and A533P, were also detected. These findings shed light on the molecular mechanisms contributing to FQ resistance in MDR-TB strains and underscore the need for enhanced diagnostic methods to identify resistance patterns more accurately. The insights gained from this research offer a foundation for improving TB treatment approaches and addressing the growing challenge of drug-resistant TB worldwide.
MDR-TB, Fluoroquinolone Resistance, gyrA Mutations, gyrB Mutations, Diagnosis, Sequence Analysis
Tuberculosis (TB) continues to pose a significant global health challenge, with approximately 8.8 million new cases and 1.45 million deaths reported each year1,2 complications, and higher rates of morbidity and mortality. Emergence of drug-resistant forms. Multidrug-resistant TB (MDR-TB), caused by Mycobacterium tuberculosis strains resistant to both isoniazid and rifampin, represents a critical threat to global TB management efforts.3,4
Fluoroquinolones (FQs) are critical second-line drugs in TB treatment5,6 whole-genome sequencing (WGS). These broad-spectrum antibacterial agents Inhibit mycobacterial DNA gyrase, resulting in bactericidal effects, thereby preventing bacterial DNA replication7-9 with moxifloxacin, levofloxacin, or gatifloxacin being prescribed to MDR-TB patients. Recently, several clinical trials of “universal” drug regimens, aiming to treat drug-susceptible and drug-resistant TB, have included a fluoroquinolone. In the absence of clinical data comparing their side-by-side efficacies in controlled MDR-TB trials, a pharmacological rationale is needed to guide the selection of the most efficacious fluoroquinolone. The present studies were designed to test the hypothesis that fluoroquinolone concentrations pharmacokinetics. Moxifloxacin (MFX), a fourth-generation fluoroquinolone, exhibits enhanced efficacy against Mycobacterium tuberculosis relative to ofloxacin (OFX). Consequently, WHO advocates for its inclusion in the treatment regimen for MDR-TB10-12 treatment regimens for multidrug-resistant TB (MDR-TB). The extensive use of fluoroquinolones to treat bacterial infections has contributed to the rise of fluoroquinolone-resistant strains of multidrug-resistant tuberculosis (MDR-TB) and extensively drug-resistant tuberculosis (XDR-TB). XDR-TB, which is resistant to fluoroquinolones and at least one second-line injectable drug, poses serious challenges in managing the treatment of patients affected by this condition.13,14
Tuberculosis resistance to fluoro-quinolones is mainly driven by mutations in the gyrA and gyrB genes, which code for the DNA gyrase subunits.15-17 The gyrA gene’s conserved region (codons 74 to 113) serves as the main locus for resistance mutations, whereas mutations in the gyrB gene (codons 461 to 499) are less common, both genes are integral to the QRDR16-18 its rapid diagnosis is crucial. The present study aimed to characterize mutations conferring resistance to second line drugs (SLDs). Despite these associations, up to 60% of fluoroquinolone-resistant M. tuberculosis isolates have been reported to lack known mutations in the QRDR of the gyrA or gyrB genes, compromising the sensitivity and specificity of molecular testing methods14,19 called multidrug-resistant (MDR). It is still uncertain whether mutations linked to resistance outside the QRDR of gyrA and gyrB play a role in FQ resistance.
India is classified among the nations with the highest burden of MDR-TB, making a substantial contribution to the global prevalence of this disease.20 TB was the leading cause of death due to a single infectious agent, ranking well above HIV/AIDS. Almost one-fourth of the world’s population is infected with M. tuberculosis. TB is curable and preventable. About 85% of people who develop TB can be successfully treated with drug regimens of 6 months. Universal health coverage (UHC. Data from national drug resistance surveys indicate that a substantial proportion of newly diagnosed and previously treated TB cases in India are MDR-TB. Fluoroquinolones, highly effective antimicrobial agents plays a crucial role in the treatment regimen for MDR-TB, have been extensively employed for over two decades in India in the management of undiagnosed respiratory bacterial infections.21 The indiscriminate administration of fluoroquinolones has been implicated in fostering fluoroquinolone resistance in Mycobacterium tuberculosis, potentially affecting clinical outcomes for MDR-TB patients22,23 knowledge about the prevalence and molecular characterization of FQ-resistant Mycobacterium tuberculosis isolates from this region remains scant. In this study, 138 M. tuberculosis isolates determined by the agar proportion susceptibility method to be resistant to ofloxacin (OFX). Assessing the prevalence of fluoroquinolone resistance in India is crucial for formulating appropriate treatment strategies for MDR-TB patients.
Given the critical role of fluoroquinolones in TB treatment and the increasing incidence of fluoroquinolone-resistant TB, there is a critical need to deepen our understanding of the genetic mechanisms that contribute to this resistance. This study focuses on the detection and characterization of gyrA and gyrB gene mutations in FQ-resistant M. tuberculosis using molecular methods. By isolating, identifying, and biochemically characterizing M. tuberculosis isolates, assessing their anti-mycobacterial susceptibility patterns, evaluating the prevalence of XDR-TB in India, and assessing the efficacy of the Line Probe Assay (LPA) for the prompt identification of extensively drug-resistant M. tuberculosis, this research aims to provide crucial insights to inform more effective TB control strategies and treatment regimens.
Ethical considerations
The research adhered to the ethical guidelines sanctioned by the Ethical Committee of the Department of Microbiology at Aligarh Muslim University, Aligarh. Consent was obtained from all participants after informing them about the study.
Sample collection
Sputum specimens were obtained from patients presenting with clinical indications of pulmonary tuberculosis at the Culture and Drug Susceptibility Testing (DST) Laboratory, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh. The inclusion criteria were based on clinical symptoms like persistent cough, chest pain, and hemoptysis, combined with radiological findings indicative of TB. A total of 865 samples were collected between June 2019 and November 2022, following strict ethical guidelines.
Controls and quality assurance
To ensure the reliability of our results, each set of experiments included negative controls (no DNA templates) to monitor for contamination, and positive controls using known FQ-resistant and FQ-sensitive M. tuberculosis strains to validate the results of mutation detection and susceptibility testing. Additionally, each batch of PCR amplifications included a control sample with a known mutation profile to verify the accuracy and consistency of the amplification process.
DNA extraction and PCR amplification
DNA extraction was performed using the GenoLyse® kit, following manufacturer instructions, to standardize the extraction process and enhance reproducibility. PCR amplification targeted the gyrA and gyrB gene regions, crucial for determining fluoroquinolone susceptibility. The selection of these specific regions was based on their known association with FQ resistance, ensuring the study’s focus on clinically relevant mutations.
Innovative techniques
The study employed a dual approach combining conventional Sanger sequencing with real-time PCR to enhance mutation detection sensitivity. This innovative method allowed for the rapid detection of mutations within the QRDR of gyrA and gyrB genes and the assessment of their frequency across different samples. This dual methodology is particularly advantageous in settings with a high burden of MDR-TB, facilitating quicker and more accurate diagnostics.
Sequence analysis
Sequencing data were analyzed using UGENE, aligned against Mycobacterium tuberculosis reference sequences using ClustalW in MEGA X to ensure accurate mutation identification. Special attention was given to novel mutations outside the traditional QRDR, which could suggest alternative mechanisms of resistance.
Data submission
High-quality sequences obtained from this study were submitted to GenBank, providing a valuable resource for future research and enabling comparisons with other strains globally. This transparency in data sharing underscores the study’s contribution to the broader scientific community.
GyrA region mutations
Mutations within the gyrA gene contribute to fluoroquinolone resistance were identified, including S91P (serine to proline at position 91), D94N (aspartic acid to asparagine at position 94), D94A (aspartic acid to alanine at position 94), D94G (aspartic acid to glycine at position 94), and S95T (serine to threonine at position 95). These mutations were observed across various samples, with the most prevalent being S95T, found in all analyzed samples. In contrast, the D94G mutation was detected only in sample AN-10, and the S91P mutation was found exclusively in sample AN-03. The mutations D94N and D94A were present in multiple samples, further highlighting their role in resistance mechanisms. The distribution of these mutations is detailed in Table 1. Nucleotide mutations within QRDR of the gyrA gene, along with amino acid translations, are illustrated in Figure 1 and 2, respectively, showcasing the specific alterations that contribute to fluoroquinolone resistance.
Table (1):
Distribution of GyrA Mutations in Mycobacterium tuberculosis Samples
| Sample Name | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mutation | AN-01 | AN-02 | AN-03 | AN-04 | AN-05 | AN-07 | AN-08 | AN-09 | AN-10 |
| S91P | – | – | Found | – | – | Found | – | – | – |
| D94N | Found | Found | – | – | Found | – | – | – | – |
| D94A | – | – | – | Found | – | – | Found | – | – |
| D94G | – | – | – | – | – | – | – | – | Found |
| S95T | Found | Found | Found | Found | Found | Found | Found | Found | Found |
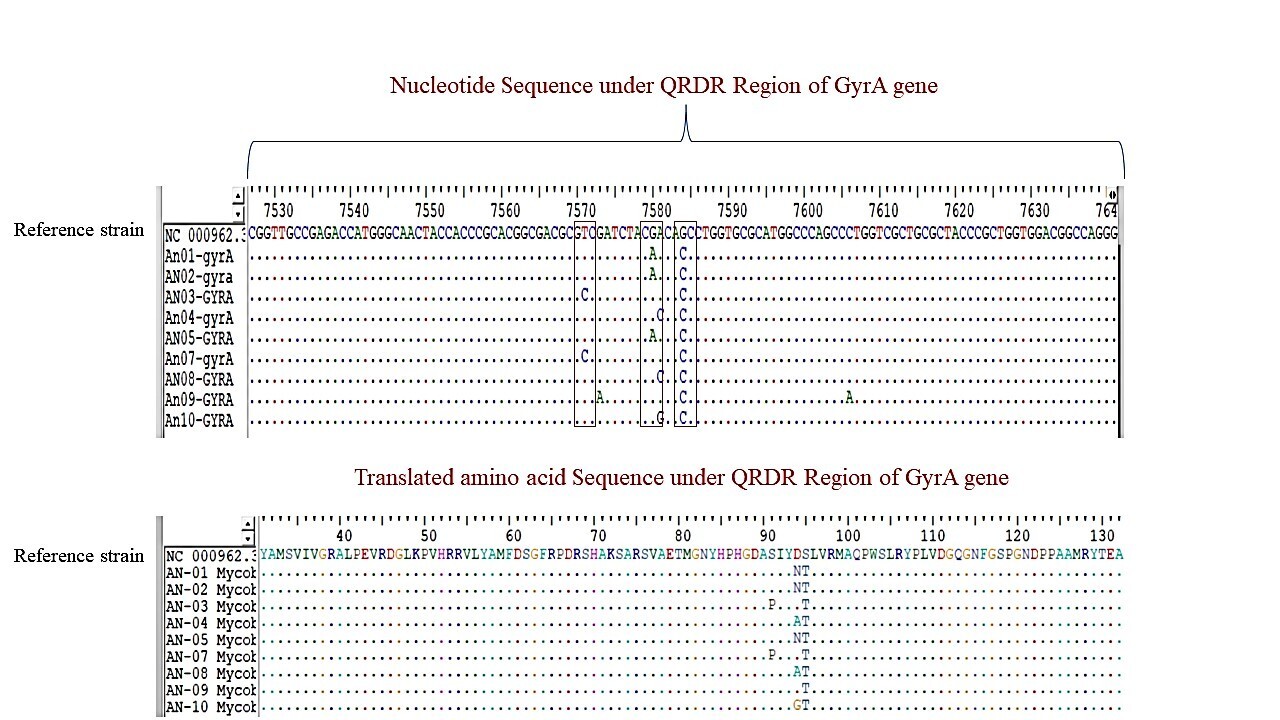
Figure 1. The chromatograms of the GyrA region for a representative sample, showing nucleotide sequences with mutations at positions S91P, D94N, D94A, D94G, and S95T
![]()
Figure 2. Sequence alignment of the QRDR region of the GyrA gene, highlighting the mutations in comparison to the reference strain. Dots indicate similarity with the reference, while variations represent the detected mutations
GyrB region mutations
Although less common, mutations in the gyrB gene also contribute to fluoroquinolone resistance. The identified mutations include E501D (glutamic acid to aspartic acid at position 501) and A533P (alanine to proline at position 533). These mutations were exclusively detected in sample AN-09, as shown in Table 2. The nucleotide sequences and amino acid translations for the gyrB region, presented in Figure 3 and 4, respectively, further delineate the genetic changes that may influence resistance to fluoroquinolones.
Table (2):
Distribution of GyrB Mutations in Mycobacterium tuberculosis Samples
| Sample Name | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mutation | AN-01 | AN-02 | AN-03 | AN-04 | AN-05 | AN-07 | AN-08 | AN-09 | AN-10 |
| E501D | – | – | – | – | – | – | – | Found | – |
| A533P | – | – | – | – | – | – | – | Found | – |
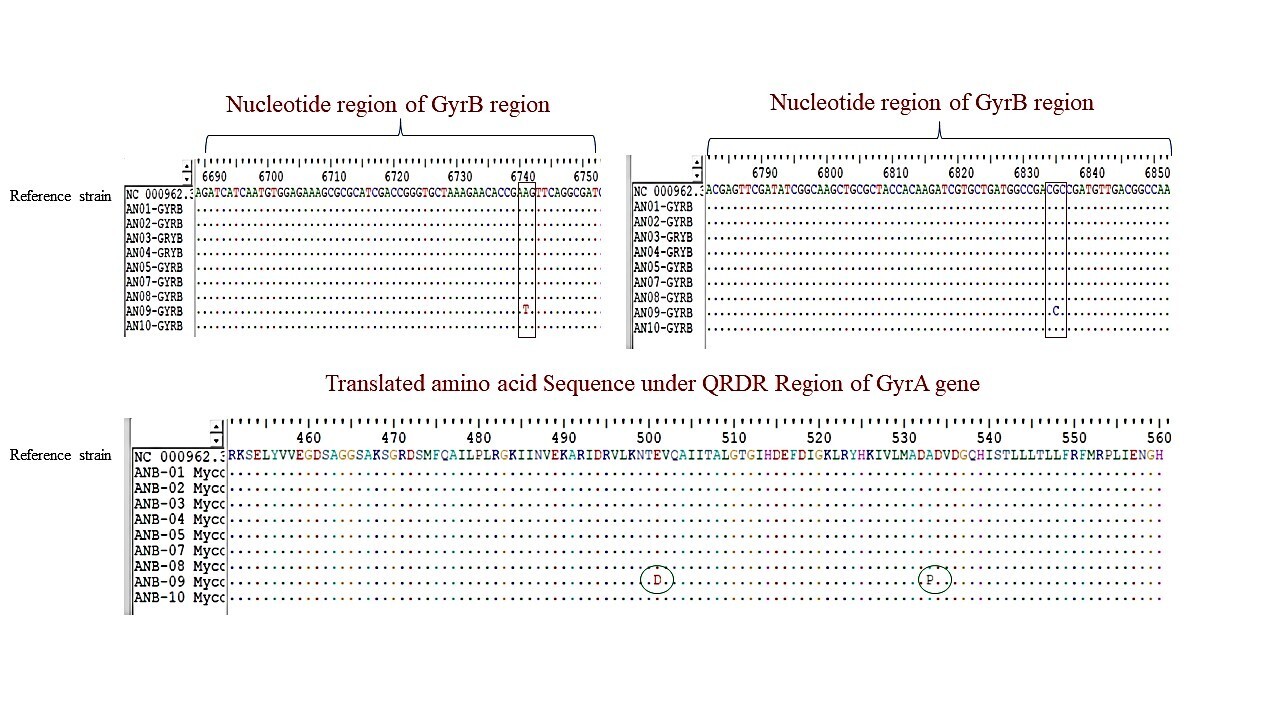
Figure 3. The chromatograms of the GyrB region for sample AN-09, displaying nucleotide sequences with mutations at positions E501D and A533P
![]()
Figure 4. Sequence alignment of the GyrB region, demonstrating the mutations E501D and A533P relative to the reference strain
GenBank accession numbers
The gyrA and gyrB nucleotide sequences were successfully entered into GenBank, receiving accession numbers PP738939 to PP738947 for GyrA sequences and PP738948 to PP738956 for GyrB sequences (Table 3). These entries are crucial for future research, providing a reference for comparative studies on fluoroquinolone resistance and helping advance new diagnostic and therapeutic methods. The data have also been shared with the DNA Data Bank of Japan (DDBJ) and the European Nucleotide Archive (ENA) to maximize accessibility for the scientific community.
Table (3):
GenBank Accession Numbers for GyrA and GyrB Sequences
Sample |
GyrA Accession Number |
GyrB Accession Number |
|---|---|---|
AN-01 |
PP738939 |
PP738948 |
AN-02 |
PP738940 |
PP738949 |
AN-03 |
PP738941 |
PP738950 |
AN-04 |
PP738942 |
PP738951 |
AN-05 |
PP738943 |
PP738952 |
AN-07 |
PP738944 |
PP738953 |
AN-08 |
PP738945 |
PP738954 |
AN-09 |
PP738946 |
PP738955 |
AN-10 |
PP738947 |
PP738956 |
The availability of these sequences in public databases facilitates future research efforts and enables the tracking of resistance patterns in global M. tuberculosis strains.
The high prevalence of specific mutations, particularly the S95T polymorphism in the GyrA gene and the rare but significant mutations like D94G, highlights a critical challenge in the global management of tuberculosis.24 The persistence and the spread of these mutations highlights the need for robust surveillance systems to monitor the emergence of drug resistance in Mycobacterium tuberculosis. Our findings suggest that current diagnostic assays need to be continually updated to include these mutations for accurate resistance detection and effective treatment planning. The widespread occurrence of the S95T mutation across various geographical regions, as shown in our study and supported by similar research, points towards its potential as a biomarker for specific TB strains25,26 katG and the ribosomal binding site of inhA (isoniazid). This could have substantial implications for developing targeted therapies and vaccines, particularly in regions with high MDR-TB and XDR-TB burdens. Our study’s identification of less common but clinically significant mutations in the gyrB gene, such as E501D and A533P, provides crucial insights for clinicians. Recognizing these mutations in clinical isolates can directly influence treatment choices, promoting the use of alternative second-line drugs when typical fluoroquinolones are likely to be ineffective. This precision in treatment strategy could lead to better patient outcomes, reduced transmission rates, and ultimately, a decline in the occurrence of drug-resistant tuberculosis.
While our study provides valuable insights into the mutation spectrum of FQ-resistant TB, several limitations must be acknowledged. First, the sample size, though substantial, is limited to one geographical area, which may not fully represent the global diversity of Mycobacterium tuberculosis. Future studies should aim to include a broader geographic sample to validate our findings and explore regional differences in mutation prevalence. Secondly, our analysis was restricted to known mutations within the QRDR of gyrA and gyrB genes. There may be other genetic factors outside these regions contributing to resistance that were not detected in this study. Future research should employ whole-genome sequencing to uncover these potential unknown mutations and their roles in drug resistance.
This research offers significant insights into the mutational profiles of the GyrA and GyrB regions in clinical isolates of Mycobacterium tuberculosis. The identification of known resistance-associated mutations, as well as less common variants, contributes to our understanding of the molecular mechanisms underlying FQ resistance. These findings may inform the development of improved molecular rapid detection tools for identifying fluoroquinolone resistance and guide personalized treatment strategies for TB patients. Future studies should focus on correlating these genetic mutations with phenotypic resistance profiles and investigating their impact on treatment outcomes. Additionally, exploring potential compensatory mutations and their role in maintaining bacterial fitness in the presence of resistance-conferring mutations could provide further insights into the evolution of FQ resistance in M. tuberculosis.
Future scope
Future research on fluoroquinolone resistance in M. tuberculosis should expand to include diverse geographic samples and employ whole-genome sequencing to identify novel mutations beyond known resistance regions. Correlating these genetic markers with clinical outcomes will be key to developing targeted treatments and improving diagnostic tools, ultimately enhancing global TB control efforts.
ACKNOWLEDGMENTS
The authors are grateful to the Department of Microbiology and the Tuberculosis Laboratory for providing the necessary facilities to carry out this research. Authors are also thankful to the laboratory staff for their technical assistance and support throughout the study.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
AS conceptualized and visualized the study. HMK and AS conducted the investigation. MS, NF, and MAK, along with AS, performed data curation. MS, NF, and AS applied the methodology. AS, MS, NF, HMK, and MAK conducted formal analysis. HMK, AS and MAK performed validation. AS wrote the original draft. AS, MAK and HMK reviewed and edited the manuscript. HMK supervised and managed the project. All authors read and approved the final manuscript for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed throughout this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics and Research Advisory Committee of the Department of Microbiology at Aligarh Muslim University, Aligarh, India.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Amin MA, Ahmed SM, Shahzadi I, Sultana R, Hanif A. Frequency and Determinants of Delay in Diagnosis of Pulmonary Tuberculosis. Pak J Health Sci. 2023:154-159.
Crossref - Chakaya J, Khan M, Ntoumi F, et al. Global Tuberculosis Report 2020 – Reflections on the Global TB burden, treatment and prevention efforts. Int J Infect Dis. 2021;113(Suppl 1):S7-S12.
Crossref - Prasad R, Gupta N, Banka A. Multidrug-resistant tuberculosis/rifampicin-resistant tuberculosis: Principles of management. Lung India. 2018;35(1):78-81.
Crossref - Mancuso G, Midiri A, De Gaetano S, Ponzo E, Biondo C. Tackling Drug-Resistant Tuberculosis: New Challenges from the Old Pathogen Mycobacterium tuberculosis. Microorganisms. 2023;11(9):2277.
Crossref - Che Y, Lu Y, Zhu Y, et al. Surveillance of fluoroquinolones resistance in rifampicin-susceptible tuberculosis in eastern China with whole-genome sequencing-based approach. Front Microbiol. 2024;15:1413618.
Crossref - Sterling TR. Fluoroquinolones for the treatment and prevention of multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2016;20(12):S42-S47.
Crossref - Sarathy J, Blanc L, Alvarez-Cabrera N, et al. Fluoroquinolone efficacy against tuberculosis is driven by penetration into lesions and activity against resident bacterial populations. Antimicrob Agents Chemother. 2019;63(5):e02516.
Crossref - Millanao AR, Mora AY, Villagra NA, Bucarey SA, Hidalgo AA. Biological effects of quinolones: A family of broad-spectrum antimicrobial agents. Molecules. 2021;26(23):7153.
Crossref - Asif M. Antimicrobial and Anti-tubercular Activity of Quinolone Analogues. Sci Int. 2013;1(10):336-349.
Crossref - Falzon D, Jaramillo E, Schünemann HJ, et al. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur Respir J. 2011;38(3):516-528.
Crossref - Sirgel FA, Warren RM, Streicher EM, Victor TC, Van helden PD, Bottger EC. gyrA mutations and phenotypic susceptibility levels to ofloxacin and moxifloxacin in clinical isolates of Mycobacterium tuberculosis. J Antimicrob Chemother. 2012;67(5):1088-1093.
Crossref - Chien JY, Chien ST, Chiu WY, Yu CJ, Hsueh PR. Moxifloxacin improves treatment outcomes in patients with ofloxacin-resistant multidrug-resistant tuberculosis. Antimicrob Agents Chemother. 2016;60(8):4708-4716.
Crossref - Lai CC, Tan CK, Huang YT, et al. Extensively drug-resistant Mycobacterium tuberculosis during a trend of decreasing drug resistance from 2000 through 2006 at a Medical Center in Taiwan. Clin Infect Dis. 2008;47(7):e57-63.
Crossref - Seung KJ, Keshavjee S, Rich ML. Multidrug-resistant tuberculosis and extensively drug-resistant tuberculosis. Cold Spring Harb Perspect Med. 2015;5(9):a017863.
Crossref - Maruri F, Sterling TR, Kaiga AW, et al. A systematic review of gyrase mutations associated with fluoroquinolone-resistant Mycobacterium tuberculosis and a proposed gyrase numbering system. J Antimicrob Chemother. 2012;67(4):819-831.
Crossref - Mayer C, Takiff H. The Molecular Genetics of Fluoroquinolone Resistance in Mycobacterium tuberculosis . Microbiol Spectr. 2014;2(4):MGM2-0009-2013.
Crossref - Chien JY, Chiu WY, Chien ST, Chiang CJ, Yu CJ, Hsueh PR. Mutations in gyrA and gyrB among fluoroquinolone-and multidrug-resistant Mycobacterium tuberculosis isolates. Antimicrob Agents Chemother. 2016;60(4):2090-2096.
Crossref - Momen G, Achraf A, Abdelmajid L, et al. Molecular characterization of mutations associated with resistance to second line drugs in Mycobacterium tuberculosis patients from casablanca, morocco. Rev Inst Med TropSao Paulo. 2021;63:E19.
Crossref - Devasia R, Blackman A, Eden S, et al. High proportion of fluoroquinolone-resistant Mycobacterium tuberculosis isolates with novel gyrase polymorphisms and a gyrA region associated with fluoroquinolone susceptibility. J Clin Microbiol. 2012;50(4):1390-1396.
Crossref - Khanna A, Saha R, Ahmad N. National TB elimination programme – What has changed. Indian J Med Microbiol. 2023;42:103-107.
Crossref - Kumar K, McHugh TD, Lipman M. Fluoroquinolones for treating tuberculosis. Clinical Pharmacist. 2017;9(5).
Crossref - Zhang Z, Lu J, Wang Y, Pang Y, Zhao Y. Prevalence and molecular characterization of fluoroquinolone- Resistant Mycobacterium tuberculosis isolates in China. Antimicrob Agents Chemother. 2014;58(1):364-369.
Crossref - Zhu C, Zhang Y, Shen Y, et al. Molecular characterization of fluoroquinolone-resistant Mycobacterium tuberculosis clinical isolates from Shanghai, China. Diagn Microbiol Infect Dis. 2012;73(3):260-263.
Crossref - Disratthakit A, Prammananan T, Tribuddharat C, et al. Role of gyrB mutations in pre-extensively and extensively drug-resistant tuberculosis in Thai clinical isolates. Antimicrob Agents Chemother. 2016;60(9):5189-5197.
Crossref - Siddiqi N, Shamim M, Hussain S, et al. Molecular characterization of multidrug-resistant isolates of Mycobacterium tuberculosis from patients in North India. Antimicrob Agents Chemother. 2002;46(2):443-450.
Crossref - Daum LT, Rodriguez JD, Worthy SA, et al. Next-generation ion torrent sequencing of drug resistance mutations in Mycobacterium tuberculosis strains. J Clin Microbiol. 2012;50(12):3831-3837.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.