


ISSN: 0973-7510
E-ISSN: 2581-690X
The traditional systems of medicine have significantly become more accepted in the developed and developing countries due to their curative property, less toxicity and minimal side effects. However, several studies have shown that they are associated with microbial contaminants. This study aimed at identifying fungi in nine polyherbal medicines used for the treatment of tuberculosis in Eastern Cape Province, South Africa. Sequences of fungi DNA that encodes internal transcribed spacer (ITS) region were retrieved from the remedies. The ITS region of the fungal rRNA operon was amplified using ITS1 and ITS4 primers. The amplicons were visualized on agarose gel electrophoresis, followed by end repair and adaptor ligation. They were further purified and quantified using Library Preparation kit NEBNext® UltraT DNA Library Prep Kit for Illumina and run on Illumina’s MiSeq platform. The study revealed that the polyherbal medicines are contaminated with fungi species. The predominant mycoflora obtained belongs to different genera or species of fungi. They include Aspergillus, Penicillium, Alternaria, Candida, Ramularia, Cladosporium and Malassezia among others. Some of these organisms are capable of causing infections in immunocompromised patients. Thus, the study identified various fungal contaminants in polyherbal remedies sold to tuberculosis patients in five communities in the Eastern Cape Province of South Africa.
Fungi, ITS region, Polyherbal medicines, Public health, Tuberculosis
The use of polyherbal formulations for therapeutic purposes has significantly increased in the developed and developing countries because of their curative property, less toxicity and minimal side effects1,2. These benefits have made the usage of herbal medicines to be intertwined with that of modern medicine, thus, increasing the global market by 7% annually3. Traditional healers, especially those in low-income countries make use of various herbal preparations for the treatment and management of ailments such as wound infection, skin diseases, diabetes, diarrhoea, urinary tract infections, stomach illnesses and tuberculosis4,5.
Tuberculosis (TB), caused by a bacterium called Mycobacterium tuberculosis is the major killer among the infectious diseases and it is the ninth-leading cause of death worldwide. An estimate of 10.4 million new TB cases was reported in 2016, of this population, 1.7 million deaths including human immunodeficiency virus-TB co-infected individual were recorded6. Seven countries have been implicated to have the highest burden of TB cases, thus responsible for 64% of the world TB burden. These countries include India, Indonesia, China, Philippines, Pakistan, Nigeria and South Africa6. According to the Statistics for South Africa, TB is a significant public health challenge accounting for 7.2% of all death in 2016 followed by diabetes mellitus7. The report of WHO (2016) gave an estimated incidence of 454,000 cases of active TB in South Africa; this implies that, about 0.8% of the 54 million South Africa populations develop active TB diseases8.
In South Africa, about three million people make use of herbal remedies for their health care purposes especially for the treatment of infection disease such as TB4,9. Despite the increasing use of herbal preparations and the global expansion of the market, safety is of great concern. Some studies have revealed that due to unscientific mode of harvesting, drying, transportation, cleaning and handling of these herbal preparations, the raw plants prone to infestations and exposed them to different kinds of microbial contaminants10. The dominating contaminants are the bacterial endospores and fungal spores while the remaining are heavy metals and viruses originating from the soil11,12,13,14.
A few surveillance studies15,16,17,18 have been conducted and have shown the presence of microbial contaminants in herbal preparations. Walther et al19 investigated 109 traditional liquid herbal medicinal products in Mwanza city, the findings revealed that 81.7% of the samples were contaminated with fecal coliforms. The microbial quality of some oral liquid herbal medicines marketed in Ile-Ife conducted showed that 90% of the samples carried microbial loads beyond officially permissible limits20. Also, the quality control of hypoglycemic herbal preparations in Nairobi investigated have shown that the preparations are contaminated with both bacterial and fungal contaminants21.
Siakrwar et al22 isolated and identified a wide spectrum of fungi including Aspergillus, Penicillium, Alternaria, Rhizopus and Syncephalastrum species in 15 medicinal plants. Toma and Abdulla,23 found that most of the fungal species detected in different types of spices and medicinal plants were Aspergillus spp. and Penicillium spp. while Stachybotrys sp., Syncephalastrum racemocum, Uocladium botrytis, Alternaria alternata, Cladosporium lignicolum and Gliocladium catenulatum were less frequently detected. Quality assessment of aqueous herbal/medicinal products has shown that the most abundant fungi were from Cladosporium herbarum. This was then followed by Aspergillus spp., Saccharomyces kluyverii, Rhodotorulla minuta, Candida membranifasciens and Sporobolomyces salmonicolor24.
The presence of numerous fungal species in herbal preparations can be harmful to consumers. Thus, in other to safe guard the health of the consumers, this study aimed at identifying the presence of different fungi in polyherbal medicines used for the treatment of tuberculosis in Amathole District Municipality, Eastern Cape Province, South Africa.
Sample collection
This study is a secondary data analysis of the first authors’ research project “Ethno-medicinal documentation of polyherbal medicines used for the treatment of tuberculosis in Amathole District Municipality of the Eastern Cape Province, South Africa” where information about the herbs used for the preparation of these remedies are revealed (25). A total of nine different polyherbal medicines were purchased from the traditional herbal healers in five different communities namely; East London (EL), King Williams Town (KWT), Hogsback (HB), Alice (AL) and Fort Beaufort (FB) as shown in Figure 1 26. These remedies were liquid preparations and each of them was already homogenized and packaged in a 2 liters container by the herbal healers. Each remedy was labeled and coded according to the place of collection. The number of remedies obtained in this study was due to the fact that only a few traditional healers treat and sell the remedies for the treatment of tuberculosis. They claim to have acquired the knowledge from their ancestors, and this knowledge is being transferred from one generation to another. The samples were transported to Medicinal Plants and Economic Development (MPED) Research Centre Microbiology Laboratory for analysis.

Fig. 1. Map of Amathole District Municipality (26)
DNA extraction
A modified method of Dei-Tutuwa et al27 was used for the fungal DNA extraction. One ml of each sample was pipetted into Eppendorf tubes and centrifuged at 12500 rpm for 10 mins, the supernatant was discarded and the cell pellets was collected. The total fungal DNA was extracted using ZR Fungal/Bacterial DNA MiniPrepTM Kit (Zymo Research, USA) according to the manufacturer instructions.
Amplification of fungal DNA using polymerase chain reaction (PCR)
The assay was conducted using the internal transcribed spacer (ITS) region of the fungal genome which is highly variable among species or even populations of the same species28. This region lies between the 18S small subunit (SSU) and 28S large subunit (LSU) ribosomal RNA (rRNA) genes, which also contains two non-coding spacer regions (ITS-A and ITS-B) separated by the 5.8S rRNA gene. The total genomic fungal DNA was amplified using forward ITS1 (5’-TCCGTAGGTGAACCTGCGG-3’) and reverse primers ITS4 (5’-TCCTCCGCTTATTGATATGC-3’)29. PCR reaction was carried out in a final volume of 25 µL consisting England Biolabs, USA 5 µL template DNA, 12.5 µL of Q5 ® Hot start High-Fidelity 2X PCR Master Mix (New), 1 µL of 10 pmol each of the oligonucleotide primers (Inqaba Biotech, SA) and 5.5 µL of nuclease free water). Reactions were performed in the thermocycler (Bio-Rad Mycycler, USA) under the following conditions: initial denaturation at 95 °C for 2 min, followed by 30 cycles at 95 °C for 20 sec, 55 °C for 30 sec, and 72 °C for 30 sec, and a final elongation at 72 °C for 5 min (30). In order to confirm the PCR products size, 5 µl of the amplicons was analyzed by gel electrophoresis in 1% agarose (Merck, SA) stained with 3 µl ethidium bromide (Sigma-Aldrich, USA). A 100 bp DNA ladder (Thermo Scientific, (EU) Lithuania was included for band size estimation purposes. All gels were run in 0.5X TBE buffer at 95 V for 1 h and visualized by UV trans-illumination (Alliance 4.7, France).
Purification of amplicons and sequencing
The amplicons were purified using the Agencourt® Ampure® XP bead protocol (Beckman Coulter, USA). The amplicon libraries were purified using the Agencourt® Ampure® XP bead protocol (Beckman Coulter, USA). Library concentration was measured using Nebnext Library quant kit (New England Biolabs, USA) and quality validated using Agilent 2100 Bioanalyser (Agilent Technologies, USA). The samples were pooled in equimolar concentrations and diluted to 4nM based on library concentrations and calculated amplicon sizes. The library pool was sequenced on a MiSeqTM (Illumina, USA) using a MiSeqTM Reagent kit V3 600 cycles PE (Illumina, USA). The final pooled library was at 10pM with 20% PhiX as control amplicon sequencing protocol. Each sample was sequenced in the sense and antisense directions using ITS1 and ITS4 primers29,31.
Data analysis
The relative frequency of different fungal phylum in each of the remedy, percentage occurrence of each fungal family and the abundance of fungal families was calculated according to Girridher and Ready32.
% of frequency = [Number of observation in which a species appeared/ Total number of observation ] ×100
Distribution of different fungal phylum in each of the polyherbal remedies
The mycological analysis of the nine polyherbal remedies revealed that all the herbal preparations are contaminated with different fungal phylum and species. The predominant fungal phylum identified in all the herbal remedies was Ascomycota followed by Basidiomycota. The presence of 5% Glomeromycota was identified in KWTb and HBss remedies while 5% Zygomycota was found in KWTc remedy (Figure 2).
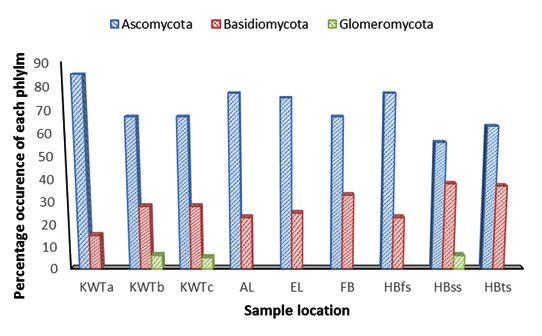
Fig. 2. Relative frequencies of contaminating organisms in each of the polyherbal remedy
Distribution of different fungal families in all the polyherbal remedies
A total of 43 different fungal families were identified in all the nine polyherbal remedies. Members of the families Davidiellaceae, Mycosphaerellaceae, Trichocomaceae, Pleosporaceae and Saccharomycetaceae were identified in all the remedies (Figure 3). This was followed by Debaryomycetaceae, Malasseziaceae, Dothioraceae, Herpotrichiellaceae and Tremellaceae.

Fig. 3. Percentage occurrence of each fungal family identified in the polyherbal remedy
The abundance of each fungal family in all the remedies is represented in Figure 4 below. Members of the family Trichocomaceae were the most abundant followed by Mycosphaerellaceae, Pleosporaceae, Saccharomycetaceae, Tremellaceae, Davidiellaceae, Malasseziaceae and Sporidiobolaceae.
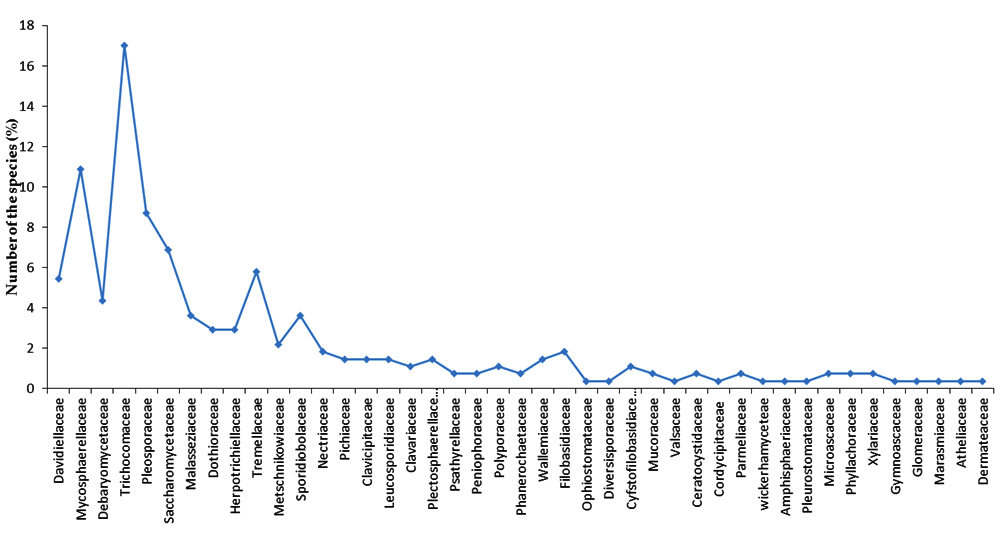
Fig. 4. The abundance of fungal families in all the polyherbal remedies
Distribution of different fungal genera and species in each of the polyherbal remedies
By analyzing each of the herbal preparation (supplementary material), KWTa remedy was mainly contaminated with species of Debaryomyces, Penicillium and Ramularia. However, Rhodotorula, Cladosporium, Ramularia, Candida and Malassezia species were found in KWTb remedy. The remedy from KWTc was contaminated with Ramularia, Candida, Cryptococcus, Rhodotorula, Cystofilobasidium and Mucor species.
While AL remedy was mostly dominated with Ramularia, Aspergillus, Penicillium, Candida, Rhinocladiella and Parmotrema species; Cladosporium, Ramularia, Alternaria, Candida and Malassezia were identified in EL remedy. The presence of Cladosporium, Ramularia, Aspergillus, Penicillium, Alternaria and Candida were detected in FB remedy.
While species of Cladosporium, Ramularia, Aspergillus and Penicillium dominated the mycofloral of HBfs remedy, HBss remedy was contaminated with Cladosporium, Ramularia and Aspergillus. However, Cladosporium, Ramularia, Aspergillus, Penicillium, Alternaria and Wallemia species were detected in HBts remedy.
Across all the herbal remedies, the most predominant mycoflora obtained was distributed in four different genera which comprised of Candida, Cladosporium, Ramularia and Alternaria. This was followed by Aspergillus and Penicillium which were found in seven and eight remedies, respectively (supplementary material).
The use of polyherbal medicines for the treatment and management of various illnesses is part of the health-care culture in South Africa. These remedies are prepared locally by traditional healers by combining two or more parts of medicinal plants such as the root, leaf, stem, flower and seed. The results obtained in the present study revealed the presence of different fungi contaminants particularly moulds and yeast in the polyherbal remedies, which are used for the treatment of TB. The presences of these organisms may pose potential health risks to tuberculosis patients considering their immunocompromised status. The high fungal population in each of the remedies is an indication of low environmental sanitation and unhygienic standard of processing these herbal medicines. All the remedies were stored at room temperature in the shops and there were no expiry date written on them, thus, the storage condition could have encouraged the growth of these fungal species.
Many of the fungal species identified are naturally inhabitant of the soil and some are plant pathogens. According to Sharma33, fungal contamination of herbal preparations mainly occurs during a slow drying process. Inadequate drying or postharvest storage of the herbs under a high relative humidity and favourable temperature promotes the growth of these microbes33. Also, the unscientific methods of collection, unsuitable transportation and prolonged storage of the plants and inadequate hygiene of the handler could trigger the growth of organisms in herbal medicines34; 10.
The presence mould such as Aspergillus and Penicillium species in seven and eight polyherbal remedies, respectively, could be attributed to the growth of these organisms in the herbs before the medicinal plants were completely dried10. Both species of Aspergillus and Penicillium have been associated with food poisoning and may cause infections in an immunosuppressed individuals35,36. The results of this study were in well agreement with those found by Tournas and Katsoudas37. The study examined the microbiological quality of various medicinal herbal teas. The findings revealed that the most common fungal contaminants in the herbal teas were Aspergillus niger, Penicillium spp., Eurotium rubrum, E. chevalieri, A. flavus, Fusarium spp., Alternaria alternata and yeasts. Also, a South African study has reported contamination of herbal products with bacteria as well as fungi such as Penicillium and Aspergillus38. Examination of pathogenic microorganisms in medicinal herbal drugs has equally shown that the most abundant fungi species were from Fusarium, Aspergillus and Alternaria according to Stevic et al10. In addition, the fungal contamination of powdered herbal medicinal preparations sold in some parts of Nigeria was evaluated, the results showed that all of the herbal preparations had the presence of fungal contaminants with predominance of Aspergillus spp. and Penicillium spp., while Mucor spp., Candida spp. and Trichosporium spp., were also present39. Similar to this study, is the findings of Zheng et al40 which revealed that the surface of medicinal herbs are predominantly contaminated with species of Aspergillus and Penicillium.
Aspergillus is a group of moulds found in natural environment, it is an airborne fungus capable of causing Aspergillosis. Species of this genus are highly aerobic, possesses the ability to grow where high osmotic pressure exist and are found in oxygen rich environment. They are capable of growing at low water content; thus, to avoid their growth, quick drying of the herbs are highly important10. There species are detectable in the ground, air and in plants. Aspergillus does not normally cause infection except in an immunocompromised individuals such as leukaemia, asthma, HIV/AIDS and in people with damaged lungs due to TB infection, thus causing severe pulmonary disease41. According to WHO Bulleting, about one-third of TB patients develop cavities in their lungs, thus making them vulnerable to the infection41. The presence of this Aspergillus in the remedies could be detrimental to the health of TB-patients considering their immunosuppressed status.
Species of Fusarium were also detected in four of the remedies. In a study carried out by Stevic et al10, Fusarium was observed as the most dominant genus in most of the herbal drugs tested. The spores of this organism can survive drying conditions and remain dormant for several months. They are found abundantly in the soil and many of them are important plant pathogens causing various diseases such as crown rot, head blight and scab on cereal grains42. Some strains such as Fusarium fumonisins and F. trichothecenes are toxins producers; however, they were not identified in these remedies. Several species of Fusarium have emerged as important opportunistic pathogens in humans causing a broad spectrum of infections such as hyalohyphomycosis, mycotic keratitis, onychomycosis, pneumonia, disseminated infections and sinusitis mostly in immunocompromised patients43,44. Species of Fusarium identified in this study are F. oxysporum, F. verticillioides and F. delphinoides. Many studies have reported cases of Fusariosis in patients with acute myeloid and lymphoblastic leukemia45 however; there is dearth information on Fusarium infections associated with tuberculosis patients. Considering the immune-deficiency of the patients, the consumption of these remedies over a long period and prolong storage should be avoided in order to prevent the production of mycotoxins in the remedies.
Alternaria, Candida and Ramularia species were also found in all the tested remedies. Alternaria species are plant pathogens and field mycotoxin-producing moulds10. They are capable of producing tenuazonic acid and other toxic metabolites which may be associated with diseases in humans or animals. These organisms have been reported as causative agents of subcutaneous phaeohyphomycosis, mycotic keratitis, hypersensitivity pneumonitis and extrinsic asthma46. They equally cause infections such as allergic bronchopulmonary mycosis and pheohyphomycotic lumbar spondylodiscitis in immunocompromised individuals. Therefore, it is important to maintain these remedies at the temperature or condition that would not support the growth this organism.
Candida species are yeasts and the most common cause of global fungal infections called Candidiasis47. They are commensals that colonize the skin, gastrointestinal and reproductive tracts. The species of Candida identified in this study are non-pathogenic strains but are capable of causing infections in immunocompromised patients. Species of these organisms have been reported as emerging pathogenic fungal in patients with pulmonary tuberculosis48,49. Since Candida species can be found on the skin, coupled with the unsterile mode of preparation of these remedies, it could be said that this organism was introduced into the remedies by the handler during the process of preparation. The presence of these fungal contaminants in the polyherbal remedies can reduce or inactivate the therapeutic activity of the remedies and possess the potential to adversely affect the tuberculosis patients.
The findings of this study indicated that polyherbal medicines marketed in the study area are contaminated with fungi contaminants. Some of these organisms are capable of causing infections in immunocompromised patients while others are plant pathogens. The contamination of these polyherbal preparations could have resulted from contaminated soil, plants, inadequate drying, unhygienic mode of preparation and possibly prolonged storage. This could probably be a potential health risk to consumers. It is therefore suggested that quality-control measures and safe handling practices be established for medicinal herbs in the Province.
ACKNOWLEDGMENTS
The work was supported by National Research Foundation of South Africa. The authors also acknowledge the traditional healers for selling the polyherbal remedies to us.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
- Binu S. Uses of pteridophytes among the tribals in pathanamthitta district, Kerala, India. J Non Timber Forest Products, 2008; 5(2): 129-131.
- Devi V M, Prasad P N, Kalirajan K. Infrared spectral studies on Siddha drug-Pavala parpam. Inter J pharma and Bio Sci, 2010; 1(4): 474-483.
- Dubey N K, Kumar A, Singh P, Shukla R. Microbial contamination of raw materials: A major reason for the decline of India’s share in the global herbal market. Curr Sci (00113891), 2008; 95: 717-718.
- Louw C A M, Regnier T J C, Korsten L (). Medicinal bulbous plants of South Africa and their traditional relevance in the control of infectious diseases. J Ethnopharmacol, 2002; 82(2): 147-154.
- Buwa L V, Afolayan A J. Antimicrobial activity of some medicinal plants used for the treatment of tuberculosis in the Eastern Cape Province, South Africa. Afr J Biotechnol, 2009; 8(23): 6683-6687.
- World Health Organization. Bending the curve – ending TB: Annual report 2017. India: World Health Organization, Regional Office for South-East Asia; 2017. apps.who.int/iris/bitstream/10665/254762/1/978929022584-eng.pdf
- Statistics South Africa. TB Statistics for South Africa – National & provincial 2017. TBFACTS.ORG | Information about Tuberculosis, 2017. https://www.tbfacts.org/tb-statistics-south-africa/ Accessed 2rd November, 2017.
- World Health Organization. Global Tuberculosis Control. Geneva, 2016 www.who.int/tb/en. Accessed 2rd November, 2017.
- Elujoba A A, Odeleye O M, Ogunyemi C M. Traditional medicine development for medical and dental primary health care delivery system in Africa. Afr J Trad Complement Alter Med, 2005; 2: 46-61.
- Steviæ T, Pavloviæ S, Stankoviæ S, Šavikin K. Pathogenic microorganisms of medicinal herbal drugs. Arch Biol Sci, 2012; 64(1): 49-58.
- Adeleye I A, Okogi G, Ojo E O. Microbial contamination of herbal preparations in Lagos, Nigeria. J Health Popul Nutr, 2005; 23(3): 296-297.
- Kaume L, Foote J C, Gbur E E. Microbial contamination of herbs marketed to HIV-infected people in Nairobi (Kenya). South Afr J Sci, 2012; 108 (9-10): 1-4.
- Ting A, Chow Y, Tan W. Microbial and heavy metal contamination in commonly consumed traditional Chinese herbal medicines. J Trad Chin Med, 2013; 33(1): 119-124.
- Noor R, Huda N, Rahman F, Bashar T, Munshi S K. Microbial contamination in herbal medicines available in Bangladesh. Bangladesh Med Res Coun Bull, 2014; 39(3):124-129.
- Czech E, Kneifel W, Kopp B. Microbiological status of commercially available medicinal herbal drugs-A screening study. Planta Medica, 2001; 67: 263-269. doi: 10.1055/s-2001-12007.
- Tassaneeyakul W, Razzazi-Fazeli E, Porasuphatana S, Bohm J. Contamination of aflatoxins in herbal medicinal products in Thailand. Mycopathologia, 2004; 158(2): 239-244.
- Okunlola A, Adewoyin B A, Odeku AO. Evaluation of pharmaceutical and microbial qualities of some herbal medicinal products in South Western Nigeria. Trop J Pharm Res, 2007; 6: 661-670.
- Kulshrestha R, Gupta C P, Shukla G, Kundu M G, Bhatnagar S P, Katiyar C K. The effect of water activity and storage temperature on the growth of Aspergillus flavus in medicinal herbs. Planta Medica, 2008; 74:1308-1315.
- Walther C, Marwa K J, Seni J, Hamis P, Silago V, Mshana S E, Jande M (). Microbial contamination of traditional liquid herbal medicinal products marketed in Mwanza city: magnitude and risk factors. Pan Afr Med J, 2016; 23(1).
- Igbeneghu O A, Lamikanra A. Assessment of the microbial quality of some oral liquid herbal medicines marketed in Ile-Ife, South-western Nigeria. Afr J Microbiol Res, 2016; 10 (38): 1618-24.
- Chege I N, Okalebo F A, Guantai A N, Karanja S. A Quality Control of Hypoglycemic Herbal Preparations in Nairobi, Kenya. J Pharm Phytochem, 2015; 3 (4): 16-21.
- Siakrwar P, Mahajan S, Gupta A, Asthana M, Sharma R. Isolation and Identification of Fungal Contamination in Stored Medicinal Plants. Am J Pharm Pharmacotherapeutics, 2014; 1 (2): 052-058.
- Toma F M, Abdulla N F. Isolation and identification of fungi from spices and medicinal plants. Res J Environ Earth Sci, 2013; 5 (3): 131-138.
- Osei-Adjei G, Hackman H K, Mills-Robertson F C, Tay S C K (). Quality assessment of aqueous herbal/medicinal products sold on the Ghanaian market. Food Sci Qual Manage, 2013; 20: 13-8.
- Famewo E B, Clarke A M, Afolayan A J. Ethno-medicinal documentation of polyherbal medicines used for the treatment of tuberculosis in Amathole District Municipality of the Eastern Cape Province, South Africa. Pharm Bio, 2017; 55 (1): 696-700.
- Famewo E B, Clarke A M, Afolayan A J. Identification of bacterial contaminants in polyherbal medicines used for the treatment of tuberculosis in Amatole District of the Eastern Cape Province, South Africa, using rapid 16S rRNA technique. J Health Popul Nutr, 2016; 35 (1): 27. doi: 10.1186/s41043-016-0064-y.
- Dei-Tutuwa D, Amuna P, Rahman M A. Rapid Detection of Microbial Contamination in Ghanaian Herbal Medicines by PCR Analysis. Ghana Med J, 2014; 48 (2): 106-111.
- Schoch C L, Seifert K A, Huhndorf S, Robert V, Spouge J L, Levesque C A, Miller A N. Nuclear ribosomal internal transcribed spacer (ITS) region as a universal DNA barcode marker for Fungi. Proc Natl Acad Sci, 2012; 109 (16): 6241-6246.
- White T J, Bruns T, Lee S J W T, Taylor J W. Amplification and direct sequencing of fungal ribosomal RNA genes for phylogenetics. PCR protocols: a guide to methods and applications. 1990, 18 (1): 315-322.
- Kuo H C, Su Y L, Yang H L, Chen T Y. Identification of Chinese medicinal fungus Cordyceps sinensis by PCR-single-stranded conformation polymorphism and phylogenetic relationship. J Agric Food Chem, 2005; 53 (10): 3963-3968.
- Kozich J J, Westcott S L, Baxter N T, Highlander S K, Schloss P D. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Appl Environ Microbiol, 2013; 79 (17): 5112-5120.
- Giridhar P, Ready S M. Incidence of mycotoxin producers on spices from Andhra Pradesh. J Indian Bot Soc, 1997; 76: 161-164.
- Sharma A. 2001. Irradiation to decontaminate herbs and spices, pp. 60-73. In Peter K V (eds.), Handbook of herbs and spices. Cambridge, UK: Woodhead Publishing.
- Sagoo S K, Little C L, Greenwood M, Mithani V, Grant K A, McLauchlin J, de-Pinna E, Threlfall E J. Assessment of the microbiological safety of dried spices and herbs from production and retail premises in the United Kingdom. Food Microbiol, 2009; 26 (1): 39-43.
- Lin S J, Schranz J, Teutsch S M. Aspergillosis case fatality rate: systematic review of the literature. Clinic Infect Dis, 2001; 32 (3): 358-366.
- Bateman A C, Jones G R, O’Connell S, Clark F J, Plummeridge. Massive hepatosplenomegaly caused by Penicillium marneffei associated with human immunodeficiency virus infection in a Thai patient. J Clin Path, 2002; 55 (2): 143-144.
- Tournas V H, Katsoudas E J. Microbiological quality of various medicinal herbal teas and coffee substitutes. Microbiol insights, 2008; 1: MBI-S943.
- Govender S, Du Plessis-Stoman D, Downing T G, Van de Venter M. Traditional herbal medicines: Microbial contamination, consumer safety and the need for standards. S Afr J Sci, 2006; 102 (5): 253-255.
- Anyanwu C U. Fungal contaminants of powdered herbal drugs sold in parts of Enugu State, Southeast, Nigeria. Plant Product Res J, 2010; 14 (1):46-50.
- Zheng R S, Wang W L, Tan J, Xu H, Zhan R T, Chen W W. An investigation of fungal contamination on the surface of medicinal herbs in China. Chin Med, 2017; 12 (1): 2.
- World Health Organization/Bulletin. 2011. Tuberculosis survivors at risk of fungal infection. http://www.who.int/bulletin/releases/NFM1211EN.pdf?ua=1, Accessed 08th November, 2017.
- Nelson P E, Dignani M C, Anaissie E J. Taxonomy, biology, and clinical aspects of Fusarium species. Clin Microbiol Rev, 1994; 7 (4): 479-504.
- Makowsky M J, Warkentin D I, Savoie M L. Caspofungin and amphotericin B for disseminated Fusarium verticillioides in leukemia. Ann Pharmacother, 2005; 39: 1365-1366.
- Guarro J. Fusariosis, a complex infection caused by a high diversity of fungal species refractory to treatment. Eur J Clin Microbiol Infect Dis, 2013; 32: 1491-1500.
- Jossi M, Ambrosioni J, Macedo-Vinas M, Garbino J. Invasive fusariosis with prolonged fungemia in a patient with acute lymphoblastic leukemia: case report and review of the literature. Intern J Infect Dis, 2010; 14 (4): 354-356.
- Crissey J T, Parish L C, Lang H. 1995. Manual of medical mycology, pp. 263. Blackwell Scientific, Cambridge, Massachusettes.
- Manolakaki D, Velmahos G, Kourkoumpetis T, Chang Y, Alam H B, De Moya M M, Mylonakis E (). Candida infection and colonization among trauma patients. Virulence, 2010; 1 (5): 367–375. doi:10.4161/viru.1.5.12796.
- Kali A, Charles M P, Noyal M J, Sivaraman U, Kumar S, Easow J M. Prevalence of Candida co-infection in patients with pulmonary tuberculosis. The Australasian Med J, 2013; 6 (8): 387.
- Ndukwu C B, Mbakwem-Aniebo C, Frank-Peterside N. Prevalence of Candida Co-Infections among Patients with Pulmonary Tuberculosis in Emuoha, Rivers State, Nigeria. IOSR J Pharmacy and Biol Sci, 2016; 11 (5): 60-63.
© The Author(s) 2018. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.