


ISSN: 0973-7510
E-ISSN: 2581-690X
Chlamydia trachomatis is one among the sexually transmitted diseases causing genital tract infection frequently associated with complications of infertility. The aim of our study is to detect the presence of C. trachomatis infection (CTI) in female infertility by nested Polymerase Chain Reaction (PCR) in a tertiary care center. A cross-sectional study was done with 230 infertile women attending the OPD of Reproductive Medicine and Surgery. CTI was detected among the study participants by screening for momp and cryptic plasmid gene using nested PCR. Based on the history and clinical presentation, the enrolled patients categorized as primary and secondary infertility. The results of the nested PCR for the primary and secondary infertile women were tabulated and compared for the statistical significance using Epi info version 7 and Chi-square test. A p-value of < 0.05 considered significant. In the study, participants 1 (20%) was primary and 4 (80%) belonged to secondary infertility. Of the 230 infertile women screened 2.2% of them had PCR positive for either momp or cryptic plasmid gene. CTI was seen more (80%) in secondary infertile than in primary infertile women. CTI was seen more in the age group 26-30 years (60%) followed by 21-25 years and 31-35 years (20%). The results of our study showed CTI is associated with infertility and recurrent spontaneous abortion. It’s imperative to screen for CTI by molecular method in young females which necessitates early therapy and prevention of long term complications like infertility.
Sexually Transmitted Pathogens, Nested PCR, Cryptic Plasmid, Recurrent Spontaneous Abortion
Globally Sexually transmitted infections (STI’s) are a serious public health concern. The most common bacterial STI pathogen are C. trachomatis. It is an obligate intracellular bacteria, currently recognized as one of the most prevalent bacterial sexually transmitted pathogens.1,2 According to estimates from the World Health Organization (WHO), 129 million individuals worldwide had C. trachomatis in 2020.1,3 According to the Sexually Transmitted Disease (STD) surveillance data from the US Centre for Disease Control and prevention (CDC), there were about 4 million cases of C. trachomatis infection was recorded in 2018.4,5 Based on the disease it caused C. trachomatis was divided into two strains or biovar – LGV (Lympho Granuloma Venereum) and TRIC (Trachoma Inclusion Conjunctivitis).6 Genital infections of C. trachomatis belonging the serovar D-K clinically manifest in females as cervicitis, salpingitis, acute urethral syndrome and endometritis whereas in males it manifest as urethritis, proctitis, epididymitis.7 These infections can be managed if promptly and appropriate medical care is provided. In women they tend to cause Pelvic Inflammatory Disease (PID), which could lead chronic consequences like infertility if left untreated.
According to several studies, 70 to 80 percent of female genital C. trachomatis patients are asymptomatic.8 Infertility can be classified as primary and secondary. Primary is defined as couples who never conceived, while secondary is defined as a couple who are unable to conceive after a prior successful conception but not necessarily having a live birth9, ectopic pregnancy and chronic pelvic pain.7,10,11 Infertility has a substantial socio psychological effect.12 It is estimated that 8–12% of couples are affected globally, however prevalence varies in different part of the globe.13 In India, incidence of primary infertility varies between 3.9% and 16.8%.12 One of the most prevalent preventable causes of Tubal Factor Infertility (TFI) and bad pregnancy outcomes is Chlamydial PID. The clinical signs or sequelae linked to recent C. trachomatis infection are not yet considered as a significant health issue in India. Screening for C. trachomatis testing is not often done as part of the evaluation of infertility.14 This large range could result from various detection methods of Chlamydia is being employed, as well as various population types.15 Rarely the prevalence of genital CTI and its consequences are studied in the underdeveloped countries. Accurate tests for the screening of C. trachomatis are very expensive and complex.9 Though it is theoretically possible to isolate the bacteria but it is technically challenging, and the need and maintenance of cell lines to acquire the living organism is another constraint of the culture. The majority of the commercially available serological test kits are expensive and have poor sensitivity and specificity.16 Hence, we aimed in the present study to detect the presence of CTI among infertile women with the use of sensitive molecular techniques like nested PCR and also the association of C. trachomatis infection in primary and secondary infertility was also assessed.
Study participants
A cross-sectional study was conducted with infertile women (n=230) who attended the Out Patient Department (OPD) of Reproductive Medicine and Surgery, Sri Ramachandra Hospital, SRIHER, a tertiary care hospital in Chennai. Sample size was determined by the odds ratio of 2.5% with power of 90% and α error of 5%. Infertile women in the reproductive age ranging from 18 years to 42 years of age of both primary and secondary cause, having no history of genital tuberculosis, and patients willing to give consent were included in the study. Patients with antibiotics treatment in the previous two months, history of recently treated for genital tuberculosis, repetitive specimen from the same patients and patients who are not willing to give consent were excluded from the study. This study is cleared by Institutional Ethics Committee with the enrollment number IEC-NI/20/FEB/74/11. A detailed clinical history was taken in the proforma.
Extraction of DNA
Endocervical swabs were collected using sterile pure viscose swab (PW041-100, Hi Media Laboratories). DNA was extracted from endocervical specimen using commercially available DNA extraction kit (QIAGEN, GERMANY) as per the standard protocol and eluted the DNA. The load of DNA was estimated by spectrophotometer (Nano drop tech). beta globin gene was included as internal control for identifying PCR inhibitors if any.
PCR for diagnosis of CTI
Nested PCR for detecting the presence of C. trachomatis with new primers targeted to find momp and cryptic plasmid genes. The assay was performed with 20µl extracted DNA using the primers designed from the conserved region of momp gene and cryptic plasmid gene of C.trachomatis with forward and reverse primer (Table 1). Positive and negative control were also run in each experiments. Test was performed in a thermo cycler (Thermofisher Veriti) following standard protocol. The amplification product (10µl) was analysed by gel electrophoresis in a 2% agarose gel (Hi media) and observed under UV transilluminator. The presence of 438bp for momp gene and 368bp for cryptic plasmid gene in clinical specimens indicated presence of C. trachomatis infections. Sanger sequencing was done for the amplified product for further confirmation. All the DNA sequences obtained were verified by BLAST analysis and deposited at NCBI (National Centre for Biotechnology Information, USA – http://www.ncbi.nlm.nih.gov) GenBank online database and provided with sequence accession numbers. Human beta globin was included as an internal control. Presence of 92bp of human beta globin gene indicates the presence of required amplifiable DNA and also PCR inhibitory were absent in the extracted DNA.
Table (1):
Primers for PCR
Primers for first round of nested PCR:
| Target organism | Target gene | Primer sequence | Tm (c) | Amplicon size |
|---|---|---|---|---|
| C. trachomatis | momp gene | Forward 5’-TGACGCTATCAGCATGCG-3’ Reverse 5’-CTCCAATGTAGGAGTGAACAT-3’ |
57.98 57.51 |
707 |
| cryptic plasmid gene | Forward 5’-GGGATTCCTGTAACAACAAGTC-3’ Reverse 5’-ATCAATGCCCGGGATTGG-3’ |
56.97 57.39 |
773 | |
| IC | beta globin gene | Forward 5’-CAACTTCATCCACGTTCACC-3’ Reverse 5’-GAAGAGCCAAGGACAGGTAC-3’ |
55.1 55.6 |
268 |
Primers for second round of nested PCR:
| Target organism | Target gene | Primer sequence | Tm (c) | Amplicon size |
|---|---|---|---|---|
| C. trachomatis | momp gene | Forward 5’-GGGATCGYTTTGATGTATTYTG-3’ Reverse 5’-AACTTGCTTGCCAYTCATGG-3’ |
55.26 57.25 |
438 |
| cryptic plasmid gene | Forward 5’-TTCTTATTGTTCTGGGGAAGAG-3’ Reverse 5’-TCTTCGTAACTCGCTCCG-3’ |
55.44 56.52 |
368 | |
| IC | beta globin gene | Forward 5’-TGGTGTCTGTTTGAGGTTGC-3’ Reverse 5’-AGGGCTGGGCATAAAAGTC-3’ |
56.6 55.6 |
92 |
Study participants
About 230 infertile women were enrolled and tested for recent CTI by nested PCR. The age of the study participants included in the study ranged from 18-42 years old. The median age of the study participants was 28 year with an Inter Quartile Range (IQR) of 6. The age and infection rate with detailed clinical histories of infertility is mentioned in table 2 & 3.
Table (2):
Distribution of age among the study population
Age (years) |
Total number of participants (n=230) |
Total no. of positive (n=5) |
Mean |
SD |
|---|---|---|---|---|
Less than 20 yrs |
7 |
0 (0%) |
0 |
0 |
21-25 |
61 |
1 (20%) |
||
26-30 |
99 |
3 (60%) |
28.6 |
1.154 |
31-35 |
42 |
1 (20%) |
||
36-40 |
15 |
0 (0%) |
0 |
0 |
41-45 |
6 |
0 (0%) |
0 |
0 |
Table (3):
Defined group of participants and CTI rate
| Clinical group | Participants (n=230) | Age in years (Range) | C. trachomatis | ||
|---|---|---|---|---|---|
| N | % | Positive | Negative | ||
| Recurrent spontaneous abortion | 44 | 19.1% | 20-33 | 2 (4.5%) | 45 (95.4%) |
| Infertility | 186 | 80.8% | 21-35 | 3 (1.6%) | 183 (98.3%) |
Among the 2 female with history of frequent spontaneous abortion. One had 2 pregnancy loses and the other had ectopic pregnancy along with 2 pregnancy loses. There are 5 (2.2%) female patients harboring CTI in the study group. In this, 40% of the patients had recurrent spontaneous abortion and 60% of them had infertility. CTI rate was high in women with secondary infertility when compared to primary infertility (80%, 4 out of 5) (Table 4)
Table (4):
CTI among primary & secondary infertility
| Women | Positive(n= 5) | Negative (n= 225) | Odds ratio | P value | ||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Primary | 1 | 20 | 138 | 61.3 | 6.34 | 0.0814 |
| Secondary | 4 | 80 | 87 | 38.6 | ||
Duration of infertility associated with current CTI
The duration of infertility among the enrolled participants is shown in Table 5.
Table (5):
Duration of infertility
Duration |
Total number of participants (n=230) |
Number of positive(n=5) |
Number of negative(n=225) |
|---|---|---|---|
˂ 5 years |
141 |
2 |
139 |
5-9 years |
46 |
3 |
43 |
˃10 years |
43 |
0 |
43 |
Risk factors
Of the 230 samples, 5 (2.2%) were positive for C. trachomatis momp and C. trachomatis cryptic plasmid and both (momp & cryptic pasmid). Of these 5 patients 1 (20%) primary infertility and 4 (80%) were secondary infertility. Association of risk factors among the positive patients and their statistical significance are shown in Table 6.
Table (6):
Risk factors associated with CTI
Risk factors |
P value |
|---|---|
Young age |
0.688317 |
Multiple partner |
0.000676 |
Use of IUD |
0.00001 |
Symptoms of PID |
0.000146 |
Nulliparous |
0.060443 |
lack of use of contraceptive device |
0.002821 |
P value <0.05 are considered as significant. Multiple partner, Use of IUD, Symptoms of PID and lack of use of contraceptive device are the significant risk factors associated with the study
Nested PCR analysis
In our study, the nested Polymerase Chain Reaction result was considered positive if it was able to yield amplicons specific for either of the 2 genes namely, momp (438bp) or cryptic plasmid (368bp) of C. trachomatis. Of the 230 samples, 5 were PCR positive for C. trachomatis momp gene (figure 1) whereas, 3 samples positive for cryptic plasmid gene (figure 2). Totally 3 samples positive for specific amplicons of both momp and cryptic plasmid genes. Genbank accession number was obtained for all the positive samples and the ID’s are OR492623- OR492625, PP068739, PP068740, OR270824, OR270825, PP068741.
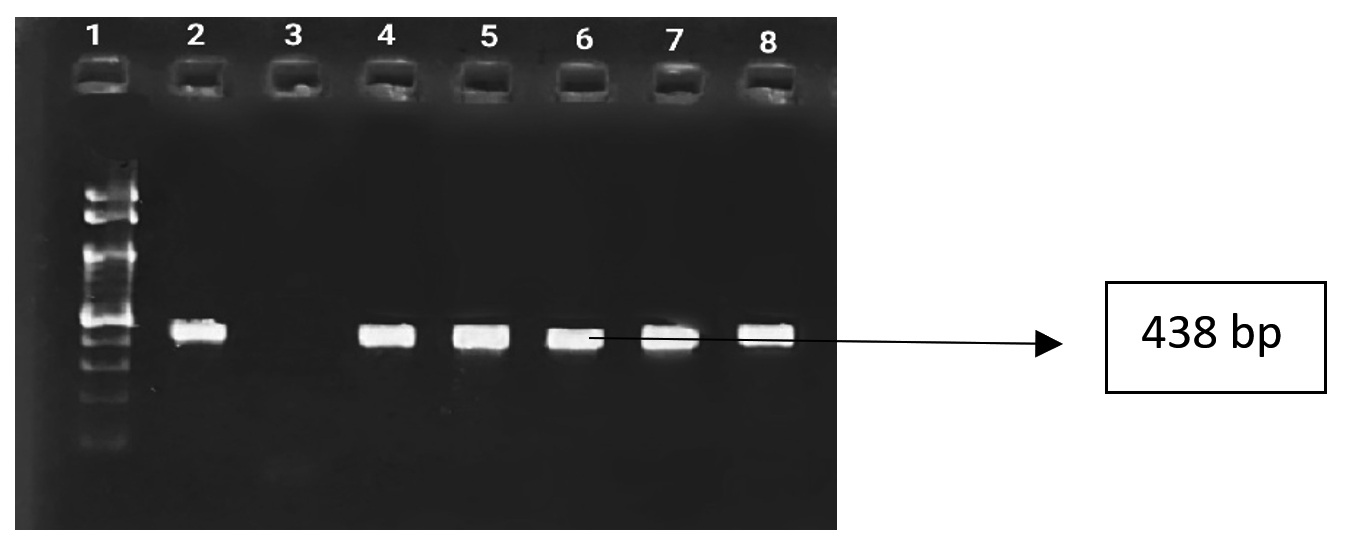
Figure 1. Lane 1- 100bp DNA marker, Lane 2- Positive control, Lane 3- Negative control, Lane 4 to 8- Chlamydia trachomatis (momp) Positive sample

Figure 2. Lane 1- 100bp DNA marker, Lane 2 to 4- Chlamydia trachomatis (cryptic plasmid) positive sample, Lane 5- Positive control, Lane 6- Negative control
In this study, majority of the cases (n=4, 80%) are secondary infertility. While (n=1, 20%) had primary infertility. Among the secondary infertility patients 1 (20%) had ruptured ectopic mass leading to TFI determined by Hysterosalpingogram (HSG). The overall Chlamydial positivity in the infertile women was found to be 5 (2.2%) (M=118.5, 95% CI: 109.7% – 127.2%) who were positive for one or both genes.
The sensitivity and specificity is increased by doing nested PCR targeting one or two genes at the same time may reduce the chance of false negativity. It was found that multiplex nested PCR targeting different genes for identification of N. gonorrhoeae and C. trachomatis improved the sensitivity of C. trachomatis detection in an earlier investigation.17 In addition, nesting the PCR technique has improved the sensitivity, specificity when comparing with the traditional single-target PCR as it minimizes the inhibitors in the clinical sample which prevents nonspecific DNA amplification.18 Numerous researchers and studies have evaluated and discussed the advantages of targeting the major outer membrane protein gene (momp) and the cryptic plasmid gene for the molecular detection,19,20 and hence used in the present study. Endocervical swab is the sample of choice for culture and Nucleic Acid Amplification Technique (NAAT) in females for better PCR positivity.21,22 Genital infections caused by C.trachomatis are often asymptomatic.4,8,23 Usually, cervix is the initial site of the infection however urethra and rectum may also be infected.24 Some individual’s experiences vaginal discharge, burning micturition, lower abdomen pain, dysuria, pelvic pain, post coital bleeding, nausea and fever.25 Even in our study the most frequent complaints were abdominal pain, back pain, foul smelling white discharge, post coital bleeding and bleeding per vaginum among the positive patients. Pelvic Inflammatory Disease (PID), urethritis, cervicitis, and cervical dysplasia are the conditions clinically linked to genital C. trachomatis.4,8,23 According to the studies by Subramanian AV et al. and Meenakshi Malhotra et al. C. trachomatis is thought to be a important cause of PID and female infertility worldwide.8,26 The risk of TFI and ectopic pregnancy increases with each episode of PID. According to Ray et al. infertility caused by C. trachomatis can be preventable.27 In 15–40% of women with cervical Chlamydial infection, PID is present.28 About 20% of PID patients may have tubal scarring, which will make them infertile; 18% will have chronic pelvic pain and 9% will experience an ectopic pregnancy.29 In our study 40% of the individual was diagnosed to have PID and ectopic pregnancy. Chlamydial DNA tends to survive in human fallopian tube tissues; this suggests that the infection may still be present and continue to cause immune-mediated tissue destruction that results in TFI.30 In our study, 20% women had TFI. According to various research, the risk factors for C. trachomatis infections are young age, oral contraceptive usage, Intrauterine Device (IUD), inconsistent condom, multiple sex partners, and prior history of STI.25,31 In our study, 80% of them were young age and lack of contraceptive device (p=0.002821), 40% of them had symptoms of PID (p=0.000146), 20% were nulliparous, multiple partner (p=0.000676) and inconsistent IUD use (p=0.0001) respectively and 20% had previous history of STI. C. trachomatis is one of the common cause of bacterial STI in World.3 In 2016, 127 million new cases of C. trachomatis was reported according to global STI surveillance.32 C. trachomatis genital infections are the most common STI in Europe and the United States. They largely have an impact on younger people. In our study, 80% of the women belonged to young age group. In the United States, the CDC received reports of more than 1.3 million CTI in 2010.33 In 2017, approximately 4,09,646 cases of C. trachomatis were reported to the European Centre for Disease Prevention and Control from 26 different European countries.34 The estimated worldwide prevalence of C. trachomatis in 2016 was 2.7% in males and 3.8% in females.35 In rural and urban women, the prevalence of CTI was found in 5.9% and 1.8%, respectively.36 In our study also, the infection rate of C. trachomatis was 2.2%. In Assam, primary and secondary infertile women had a seropositivity of 25% for C. trachomatis, whereas the control group had only 7.5% but in our study, the prevalence of C. trachomatis is only 2.2% possibly as a result of increased awareness,37 hygienic condition associated and also majority of the study participants belongs to urban areas. Based on ELISA and PCR results by Mallika Ghosh et al. the prevalence of CTI was 8.75% among the women with infertility.9 Bajpai and his colleagues in their study found, 4.5% tested positive and 6.5% tested borderline positive for IgG ELISA among infertile women.38 In Alligarh, using ELISA and cell culture from endocervical and blood samples the seropositivity was found to be 55% and 5.5% in the secondary infertile women and control group.39 Patients with PID had an overall C. trachomatis positive rate of 33% from cervical samples by Enzyme Immuno Assay.40 Using the multiplex amplicor CT/NG kit, men and women were shown to have a relatively low prevalence of C. trachomatis (0.88%) in Karnataka.41 This molecular study showed as rate of positivity as 2.2% for C. trachomatis among female with infertility has been observed. In Puducherry, there was a very low incidence 0.38% of C. trachomatis was observed among pregnant women.25 So, the reason for prevalence varying in different parts of the country is may be due to the personal hygiene, literacy, cultural, social behavior, population under study and methodology of the assay. Our results are comparable to Alexandar et al. and Linden et al. (1.8% & 2.2%). History of previous infection of Chlamydia has been observed in secondary infertile women’s has been reported in various studies. Recurrent spontaneous abortions and infertility have both been linked to C. trachomatis.39,42 A similar correlation was seen in the current investigation, however the number of sample included in the study is small to draw any firm conclusions, and the women who were included were not followed up on. The enrolled women were unable to be contacted due to frequent change of their mobile numbers and difficult to obtain information from the patients. The importance of C. trachomatis diagnosis is highlighted by the absence of signs, and symptoms in a substantial proportion of currently infected women as well as high rate of infection in the younger age group. Current C. trachomatis infections may contribute to the cause of infertility and their treatment will improve the chances of successful pregnancy outcomes.
Molecular diagnosis of CTI should be encouraged; the study findings suggest the nested PCR method used in the current study may be used to diagnose and treat at the early C. trachomatis infections in both symptomatic and asymptomatic patients, particularly in females with infertility. The detection of C. trachomatis was enhanced by the incorporation of two different genes. The results of the study indicate a strong correlation between current CTI and infertility. The lack of signs and symptoms associated with the illness emphasizes the need to investigate women with a history of infertility for better management.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Sri Ramachandra, Institute of Higher Education and Research (Deemed to be University), Chennai, India, with reference number IEC-NI/20/FEB/74/11.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Mohseni M, Sung S, Takov V. Chlamydia. [Updated 2023 Aug 8]. In: StatPearls. Treasure Island (FL): StatPearls https://www.ncbi.nlm.nih.gov/books/NBK537286/
- Murray SM, McKay PF. Chlamydia trachomatis: Cell biology, immunology and vaccination. Vaccine. 2021;39(22):2965-2975.
Crossref - Rodrigues R, Sousa C, Vale N. Chlamydia trachomatis as a Current Health Problem: Challenges and Opportunities. Diagnostics. 2022;12(8):1795.
Crossref - Chlamydia – CDC Detailed Fact Sheet. https://www.cdc.gov/std/chlamydia/stdfact-chlamydia-detailed.htm#print
- Kreisel KM, Spicknall IH, Gargano JW, et al. Sexually Transmitted Infections Among US Women and Men: Prevalence and Incidence Estimates, 2018. Sex Transm Dis. 2021;48(4):208-214.
Crossref - Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Elsevier Inc., 2014;3697.
- Hocking JS, Geisler WM, Kong FYS. Update on the Epidemiology, Screening, and Management of Chlamydia trachomatis Infection. Infect Dis Clin North Am. 2023;37(2):267-288.
Crossref - Vaikundam Subramanian A, Nagarajan S, Santhana Kumarasamy P. Aftermath of Chlamydia Trachomatis – The Tip of an Iceberg in Female Reproductive Health. J Mother Child. 2023;27(1):102-106.
- Ghosh M, Choudhuri S, Ray RG, et al. Association of Genital Chlamydia trachomatis Infection with Female Infer-tility, Study in a Tertiary Care Hospital in Eastern India. Open Microbiol J. 2015;9:110-116.
Crossref - Charlotte GA, Thomas QC. Chlamydial Infections. In: Dan LL, Anthony FS, Dennis KL, Stephen HL, Jameson JL, Joseph L. Eds. Harrison’s Principles of Internal Medicine. McGraw Hill 2012: 1421-1431.
- Zumla A. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Lancet Infect Dis. 2010;10(5):303-304.
Crossref - Rutstein SO, Shah IH. Infecundity, infertility, and childlessness in developing conuntries. InInfecundity, infertility, and childlessness in developing conuntries 2004:56-56.
- Adamson PC, Krupp K, Freeman AH, et al. Prevalence & correlates of primary infertility among young women in Mysore, India. Indian J Med Res. 2011;134(4):440-446.
- Mania-Pramanik J, Kerkar S, Sonawane S, Mehta P, Salvi V. Current Chlamydia trachomatis Infection, A Major Cause of Infertility. J Reprod Infertil. 2012;13(4):204-210.
- Rawre J, Dhawan B, Malhotra N, et al. Prevalence and distribution of Chlamydia trachomatis genovars in Indian infertile patients: a pilot study. APMIS. 2016;124(12):1109-1115.
Crossref - Rastogi S, Das B, Salhan S, et al. Effect of treatment for Chlamydia trachomatis during pregnancy. Int J Gynaecol Obstet. 2003;80(2):129-137.
Crossref - Priyadarshi K, Prakash P, Rani A, et al. Multiplex nested polymerase chain reaction targeting multiple genes for the detection of Neisseria gonorrhoeae and Chlamydia trachomatis in genitourinary specimens. Indian J Sex Transm Dis AIDS. 2019;40(2):152-158.
Crossref - Sandin RL. Polymerase chain reaction and other amplification techniques in mycobacteriology. Clin Lab Med. 1996;16(3):617-639.
Crossref - Mahony JB, Luinstra KE, Sellors JW, et al. Comparison of plasmid- and chromosome-based polymerase chain reaction assays for detecting Chlamydia trachomatis nucleic acids. J Clin Microbiol. 1993;31(7):1753-1758.
Crossref - Seth-Smith HM, Harris SR, Persson K, et al. Co-evolution of genomes and plasmids within Chlamydia trachomatis and the emergence in Sweden of a new variant strain. BMC Genomics. 2009;10:239.
Crossref - Malhotra M, Bala M, Muralidhar S, et al. Prevalence of Chlamydia trachomatis and its association with other sexually transmitted infections in a tertiary care center in North India. Indian J Sex Transm Dis AIDS. 2008;29(2):82-85.
Crossref - Patel AL, Sachdev D, Nagpal P, et al. Prevalence of Chlamydia infection among women visiting a gynaecology outpatient department: evaluation of an in-house PCR assay for detection of Chlamydia trachomatis. Ann Clin Microbiol Antimicrob. 2010;9:24.
Crossref - Shetty S, Kouskouti C, Schoen U, et al. Diagnosis of Chlamydia trachomatis genital infections in the era of genomic medicine. Braz J Microbiol. 2021;52(3):1327-1339.
Crossref - Black CM. Current methods of laboratory diagnosis of Chlamydia trachomatis infections. Clin Microbiol Rev. 1997;10(1):160-184.
Crossref - Stephen S, Ghose S, Anitharaj V, Pradeep J. Seroprevalence of Chlamydia trachomatis in Healthy Pregnant Women of Puducherry. Indian J Microbiol Res. 2017;4(3):295-297.
- Malhotra M, Sood S, Mukherjee A, Muralidhar S, Bala M. Genital Chlamydia trachomatis: an update. Indian J Med Res. 2013;138(3):303-316.
- Ray K. Chlamydia trachomatis & infertility. Indian J Med Res. 2006;123(6):730-734.
- Hillis S, Black C, Newhall J, et al. New opportunities for Chlamydia prevention: applications of science to public health practice. Sex Transm Dis. 1995;22(3):197-202.
Crossref - Miller KE. Diagnosis and treatment of Chlamydia trachomatis infection [published correction appears in Am Fam Physician. 2008;77(7):920]. Am Fam Physician. 2006;73(8):1411-1416.
- Patton DL, Askienazy-Elbhar M, Henry-Suchet J, et al. Detection of Chlamydia trachomatis in fallopian tube tissue in women with postinfectious tubal infertility. Am J Obstet Gynecol. 1994;171(1):95-101.
Crossref - Leon SR, Konda KA, Klausner JD, et al. Chlamydia trachomatis infection and associated risk factors in a low-income marginalized urban population in coastal Peru. Rev Panam Salud Publica. 2009;26(1):39-45.
Crossref - World Health Organization. Report on global sexually transmitted infection surveillance 2018.
- Centers for Disease Control and Prevention. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae-2014. MMWR Recomm Rep. 2014;63(RR-02):1-19.
- European Centre for Disease Prevention. Annual Epidemiological Report. ECDC, European Centre for Disease Prevention and Control; 2012.
- Rowley J, Hoorn SV, Korenromp E, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. 2019;97(8):548-562.
Crossref - Alexander R, Mathai E, Nayyar V, Mathew M, Jasper P. Low prevalence of chlamydial endocervical infection in antenatal south Indian women. Genitourin Med. 1993;69(3):240-241.
Crossref - Mohan DG, Borthakur AK. Seroprevalence of Chlamydia trachomatis in infertile women in a tertiary care hospital: a pilot study. Indian J Med Microbiol. 2015;33(2):331-332.
Crossref - Bajpai T, Ganesh BS, Neelesh G. Prevalence of Chlamydia trachomatis immunoglobulin G antibodies in infertile women attending an in vitro fertility center. Indian J Sex Transm Dis AIDS. 2015;36(2):215-216.
Crossref - Malik A, Jain S, Rizvi M, Shukla I, Hakim S. Chlamydia trachomatis infection in women with secondary infertility. Fertil Steril. 2009;91(1):91-95.
Crossref - Shrikhande SN, Joshi SG, Zodpey SP, Saoji AM. Chlamydia trachomatis in pelvic inflammatory disease. Indian J Pathol Microbiol. 1995;38(2):181-184.
- Sowmya B, Rajendran P, Krishnan S, et al. Prevalence of Chlamydia trachomatis and Neisseria gonorrhoeae genital infections in the apparently healthy population of Sringeri (Karnataka) by a coamplification PCR assay. Indian J Med Microbiol. 2001;19(4):228-229.
- Malik A, Jain S, Hakim S, Shukla I, Rizvi M. Chlamydia trachomatis infection & female infertility. Indian J Med Res. 2006;123(6):770-775.
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.