


ISSN: 0973-7510
E-ISSN: 2581-690X
Healthcare associated infections are the potential cause of morbidity and mortality amongst paediatric population. Widespread antimicrobial use amongst paediatric population leads to the antimicrobial resistance. Bloodstream infections amongst the paediatric population are the leading cause of death. The objective of the study was to determine the general trend of antimicrobial susceptibility pattern in the paediatric and neonatal age group in the ICU setting. Retrospective analysis was done of all the patients of paediatric and neonatal age group who were admitted in ICU including patients on ventilators, and whose blood samples were sent to the lab for culture and sensitivity testing. The sample profile from PICU and NICU shows the total numbers of 3056 samples (including blood, ET secretion, pus, urine, pleural fluid, etc.) were received in the laboratory from paediatric and Neonatal ICU during the study period. Total blood samples received from PICU and NICU were 1310 (sample size). Out of these, blood samples received from PICU were 618 (33.76%), of which 173 (28%) were positive, whereas, 692 (56.52%) blood samples were received from NICU, of which 242 (35%) were positive. The blood samples showed that in PICU, CONS (20.75%), and Staphylococcus aureus (16.98%) were found in maximum numbers. In NICU, Klebsiella pneumoniae were obtained in maximum numbers (30.77%), followed by Acinetobacter baumannii (21.98%). CONS (Methicillin resistant) were found 100% susceptible against Linezolid, followed by Vancomycin and Clindamycin (83% each). Staphylococcus aureus showed 100% sensitivity for Teicoplanin. Klebsiella pneumoniae, were found to be most susceptible to Tigecycline (74.07%) and Colistin (70.37%). Acinetobacter in blood of PICU patients showed high level of resistance with only 37.5% sensitivity for Colistin and Minocycline each, 12.5% sensitivity for Amikacin. To our conclusion, Linezolid was found to be the best Antimicrobial agent against MRCONS, whereas, Linezolid, Teicoplanin, Tetracyclines were found to have good efficacy against Staphylococcus aureus. The best antimicrobial agents against Klebsiella pneumonia and E. coli were Colistin and Tigecycline.
Multidrug-resistant Organisms, Klebsiella pneumoniae, MR CONS, Health Care Associated Infections, PICU, NICU
Health care associated infections are emerging as a global threat in hospital settings, especially in intensive care units. The incidence of these infections in paediatric and neonatal ICU ranges from 6 to 12% and 10 to 25% respectively.1 The common cause of morbidity and mortality in neonates is sepsis, the predisposing factors for which are premature birth, low birth weight and prolonged hospital stay. Besides these factors, the widespread use of antimicrobials adds to the burden, which leads to early colonization of the virulent strains resulting in increased rate of morbidity and mortality amongst neonates.2 As Antimicrobial resistance is on the rise worldwide, it is gradually sneaking up into paediatric population because of injudicious use of antibiotics.3
One of the major health issue in low-middle income countries including India is Neonatal death, which shares the major burden of infant and under-5 mortality.4 Approximately one million deaths occurring a year in the neonatal period (0-28 days) are caused by infection. These account for over 25% of global neonatal deaths and 99% of these deaths occur in developing countries.5 Bloodstream infections remains the leading cause of death with mortality rate of 12.7% in paediatric population.6
Because of developing antibiotic resistance, the antibiotics commonly used for treatment are not so effective. The spectrum hospital acquired infections of paediatrics patients is quite different from the adult patients.7
It is advisable to the clinical microbiologists and clinicians to keep track on the susceptibility pattern for the better management of patients. Therefore, the present study was planned to know the burden and antimicrobial susceptibility pattern of multidrug-resistant organisms in blood stream infections amongst the paediatric patients in PICU.
This is retrospective study from January 2023 to December 2023 done in the Department of Microbiology at a tertiary care hospital, in North India. Data was collected from Laboratory information system. Ethical clearance was taken from institutional ethical clearance committee under Ref. No. SGRR/IEC/02/24.
This paper aims to determine the general trend of antimicrobial susceptibility pattern in the paediatric and neonatal age group in the ICU setting of our hospital. All the patients of paediatric and neonatal age group who were admitted in ICU including patients on ventilators, and whose blood samples were sent to the lab for culture and sensitivity testing were included in the study. Total blood samples received from PICU and NICU were 1310. The samples other than blood and samples from wards and ICUs other than PICU (Paediatric ICU) and NICU (Neonatal ICU) were excluded from the study.
1-2 ml of paired blood samples were collected in BACTEC BD (Becton, Dickinson and company) blood culture vials from the patients in ICU and sent to the microbiology lab for the culture and sensitivity testing. Once in the clinical microbiology laboratory, were directly incubated aerobically at 35 ± 1°C into the BACTEC fluorescent series instrument. The blood culture bottles which beeped positive were subjected to preliminary microscopic examination of Gram-stain. Subcultures were also performed from these bottles on blood and MacConkey agar plates at 48 hrs and 72 hrs which were incubated aerobically at 37°C overnight. The plates were kept incubated in BACT/ALERT upto day 5, before reporting it negative (In case there was no beep). Antibiotic susceptibility testing of bacterial isolates was performed using Vitek 2 compact automated machine, the results of which were interpreted as per Clinical and Laboratory Standards Institute guidelines. American Type Culture Collection control strains were used to ensure the quality of each procedure.
Total blood samples received from PICU and NICU were 1310. Out of these, blood samples received from PICU were 618 (33.76%), of which 173 (28%) were positive, whereas, 692 (56.52%) blood samples were received from NICU, of which 242 (35%) were positive (Table).
Table:
Culture positive blood samples from PICU & NICU (%)
PICU (n = 618) |
173 (28%) |
NICU (n = 692) |
242 (35%) |
The bacterial profile of blood samples shows that in PICU, CONS (20.75%) and Staphylococcus aureus (16.98%) were found in maximum numbers, followed by E. coli, Acinetobacter and Pseudomonas aeruginosa (15.09% each), whereas, in NICU, Klebsiella pneumoniae were obtained in maximum numbers (30.77%), followed by Acinetobacter baumannii (21.98%). CONS (10.99%) and Staphylococcus aureus (1.10%) were found in low numbers in NICU (Figure 1).
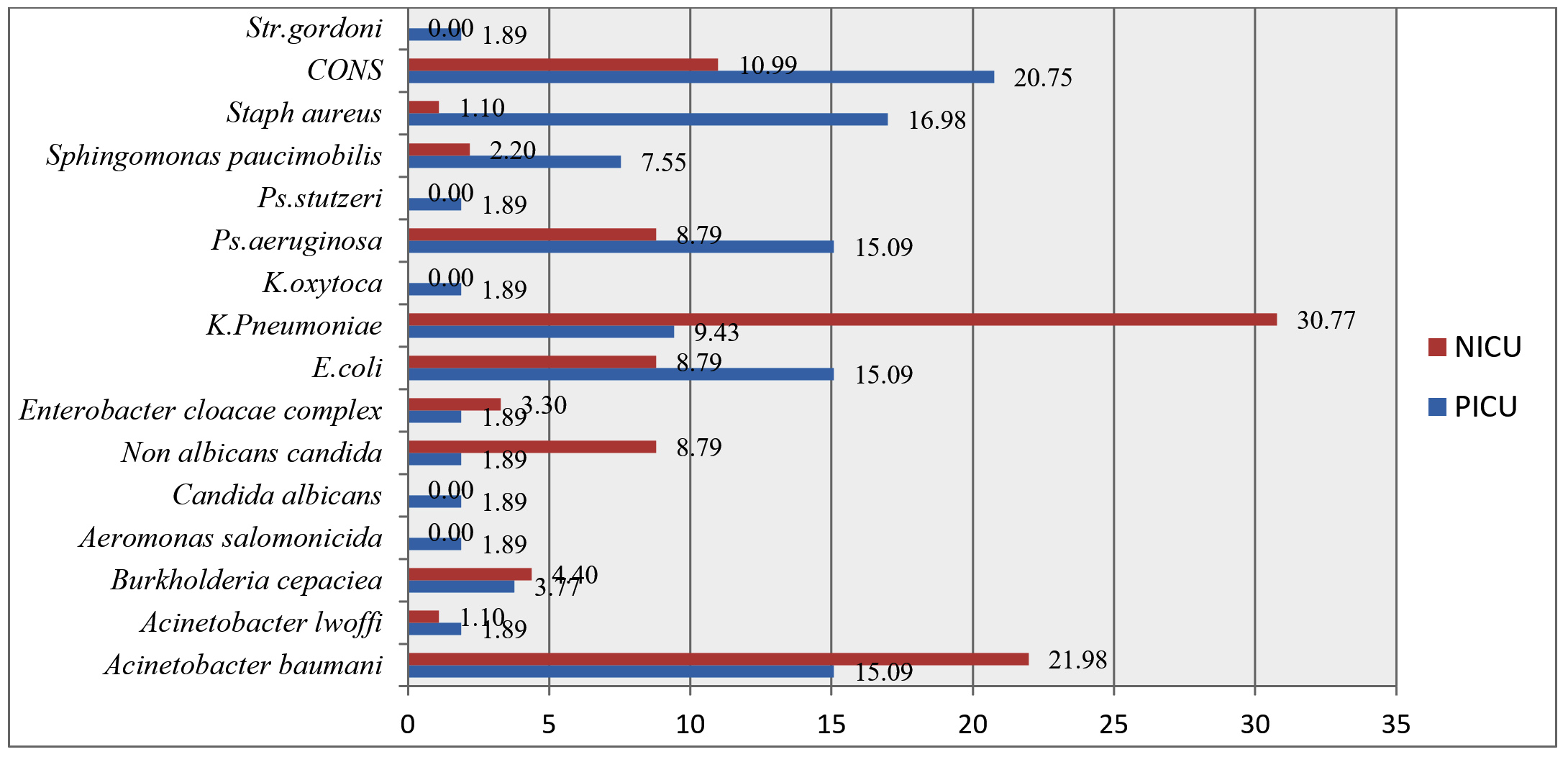
Figure 1. Bacterial profile in blood samples (PICU & NICU)
Antimicrobial profile of blood samples from PICU
Escherichia coli have shown very good sensitivity for Ciprofloxacin, Tigecycline with 100% sensitivity each, Gentamicin, Colistin, Amikacin, Imipenem and Meropenem (87.5% sensitivity each). Acinetobacter in blood of PICU patients showed high level of resistance with only 37.5% sensitivity for Colistin and Minocycline each, 12.5% sensitivity for Amikacin. All other antibiotics were resistant against Acinetobacter. Pseudomonas aeruginosa showed maximum susceptibility against Meropenem (66.6%), followed by Ciprofloxacin (44.4%), Ceftazidime, Amikacin, Imipenem (33.3%) and Only 22.2% against Pip-Taz (Figure 2).
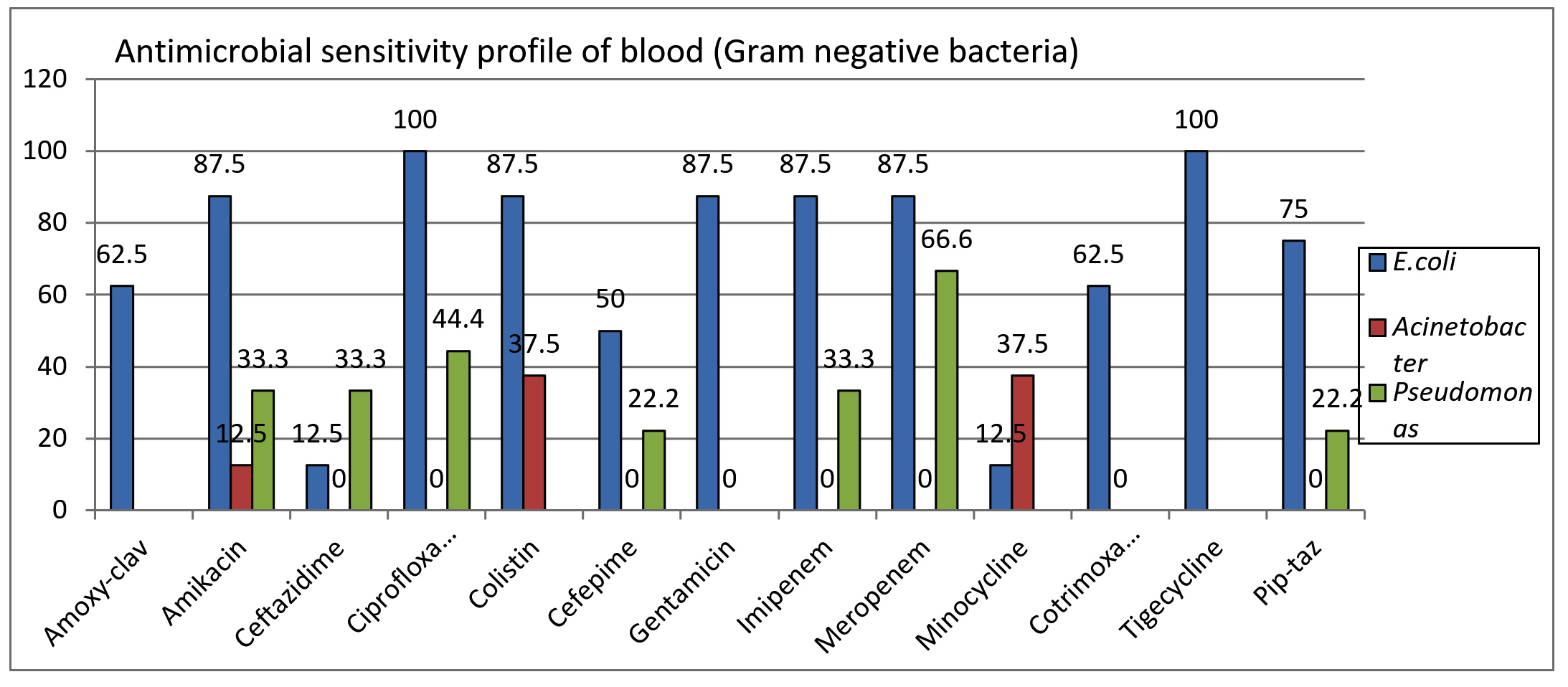
Figure 2. Antimicrobial susceptibility profile of predominant Gram-negative bacteria in blood (PICU)
Staphylococcus aureus have 100% sensitivity for Teicoplanin. Rifampicin, Linezolid and Tetracycline group of antibiotics were found to have good sensitivity (75%) against Staphylococcus aureus (Figure 3).
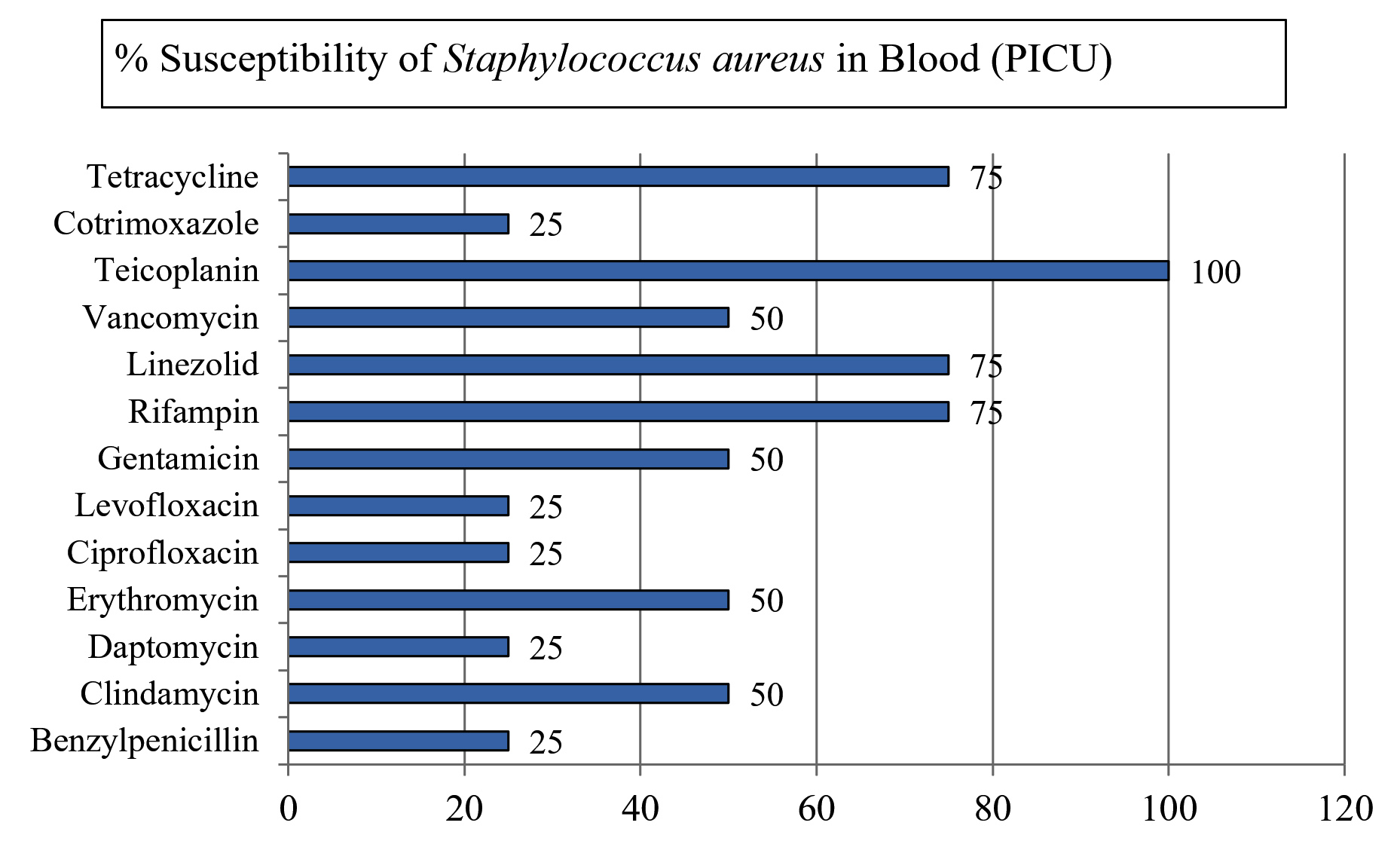
Figure 3. Antimicrobial susceptibility profile of Staphylococcus aureus in blood (PICU)
Methicillin-resistant CONS were found in large numbers (66%) amongst all the Coagulase negative Staphylococcus aureus isolated from blood samples. Figure 4 shows the susceptibility pattern of methicillin-resistant CONS isolated from blood samples. It was found 100% susceptible against Linezolid, followed by Vancomycin and Clindamycin (83% each).
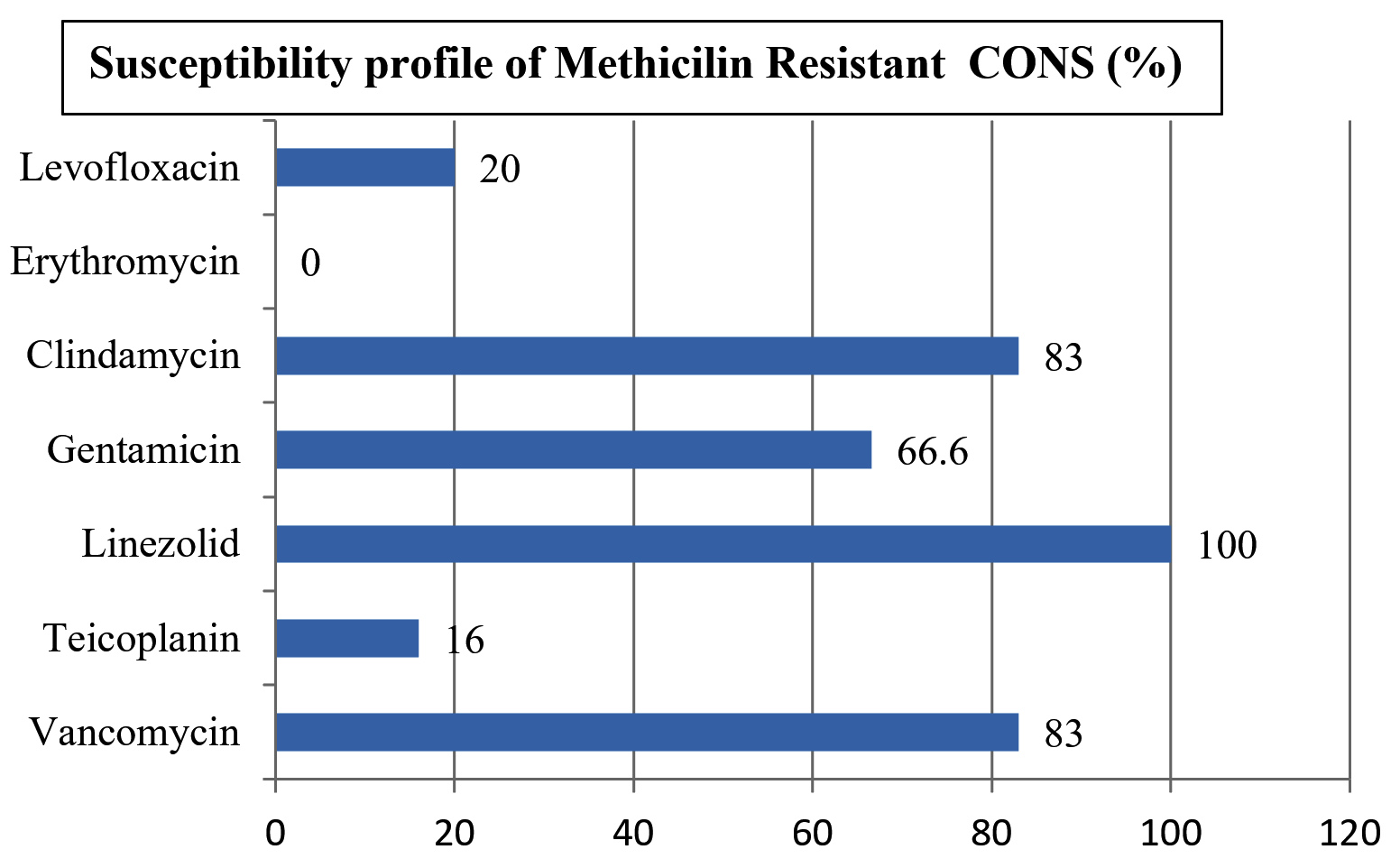
Figure 4. Antimicrobial susceptibility profile of MR-CONS (PICU)
Antimicrobial profile of blood samples from NICU
As shown in Figure 5, the predominant bacteria isolated in the cultures from NICU, Klebsiella pneumoniae, were found to be most susceptible to Tigecycline (74.07%) and Colistin (70.37%). All other antimicrobial agents showed very low susceptible rates against Klebsiella pneumoniae.
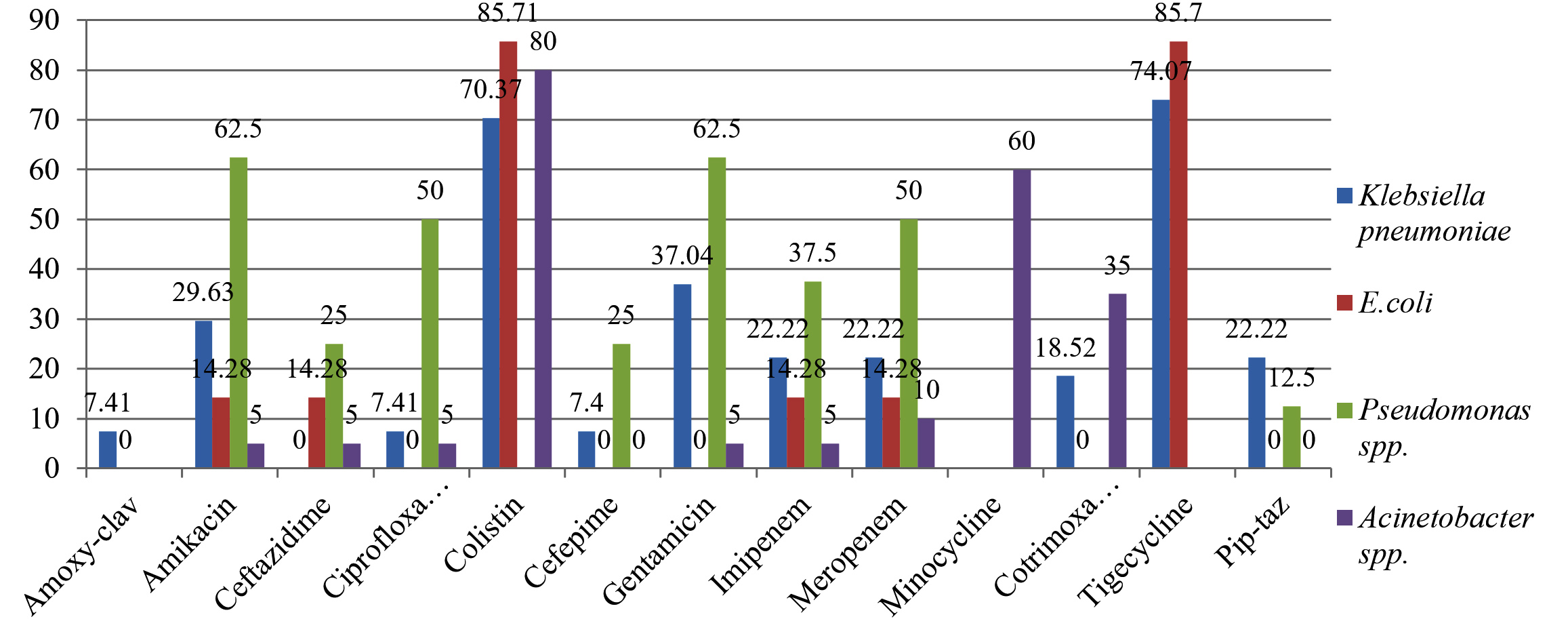
Figure 5. Antimicrobial susceptibility profile of Gram-negative bacteria in Blood (NICU)
Antimicrobial susceptibility for E. coli showed the similar pattern with high susceptibility against Colistin and Tigecycline (85.7%), and all other antimicrobial agents showed very low susceptibility rates. Whereas, in case of Pseudomonas aeruginosa, maximum susceptibility was seen against aminoglycosides, Amikacin and Gentamicin (62.5% each).
Acinetobacter spp. Shows maximum susceptibility against Colistin (80%) and Minocycline (60%).
Nosocomial infections in the paediatric age group constitute a major health problem as they are associated with high morbidity and mortality. This is one of the reasons of increased health care costs and burden on the patients as well as health care workers.8 Multidrug-resistant organisms require more expensive therapies, thus treatment cost is correspondingly increased.9 The prevalence of infections by MDR organisms vary across the world.
In this study, it is seen that 33.76% of the total samples were blood sample, out of which 28% were positive blood cultures, whereas, 35% of the samples were positive blood cultures from NICU. This higher rate of positivity of blood cultures from NICU may be due to the more number of samples received from NICU.
The bacterial profile of PICU is different from that of NICU. In PICU, it is seen that CONS and Staphylococcus aureus were isolated in maximum numbers (20.75% and 16.98%) respectively. Singh et al. also observed CONS as emerging primary pathogen amongst gram positive bacteria in blood stream infections.10 A study done in a tertiary care centre, Punjab, India, also reported very high amount, i.e. 38.7% of CONS from Paediatric department.11 Similarly, a study from Brazil also reported that around 25% to 57% of BSI were caused by CONS.12 Besides CONS, Staphylococcus aureus also remains the major cause of Blood stream infections in the hospital settings. In this study, Staphylococcus aureus were isolated in high amount (16.98%). Similar results were achieved by Tak et al., in their study done in Indian Trauma centre, where they achieved 53% Staphylococcus aureus from Blood samples followed by CONS (47%).13 A Chinese study also reported the higher amount of Gram-positive bacteria as compared to Gram-negative bacteria in ICUs.14 Followed by CONS and Staphylococcus aureus, which comprised of major culprit amongst PICU patients, Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter species were found 15.09% each. The rates were comparable to the study Singhi S, et al., where the majorly was Klebsiella pneumoniae and Acinetobacter species were isaolated but Pseudomonas aeruginosa were found only in 3%.15
Whereas, in NICU, Gram-negative Bacteria (GNB) predominated with Klebsiella pneumoniae in maximum numbers (30.77%), followed by Acinetobacter baumannii (21.98%). The results of NICU were similar to that of the study done by Putra et al., where they received 66.01% of GNB from blood samples, showing GNB as the predominant cause of bloodstream infection in ICU. Whereas, in contrary to our study, the predominant isolate in a study conducted by Putra et al., was Burkholderia cepacia.16 Similar to our study, Singhi et al., and Maham et al. also reported Klebsiella pneumoniae as predominant gram-negative bacteria causing blood stream infections.17
Silago et al. reported the predominant bacterium as Acinetobacter species in PICU.18 This difference may be due to the distinct social, economic, and environmental factors in these regions.
The predominant gram-positive bacteria which was responsible for bacteremia in PICU was Coagulase-negative Staphylococcus aureus (CONS) with the rate of 20.75%. Amongst these, around 50% of the strains were contaminant as the differential time to positivity is >120 mins in them. The remaining 50% were found to be significant. The reason of MR CONS may be due to the prolonged stay of the patients in ICU settings and exposure to numerous antibiotics. In this study, MR CONS were 100% susceptible to Linezolid, followed by Vancomycin and Clindamycin with 83% each. Whereas, study done in Indonesia by Putra et al., susceptibility rates for Staphylococcus haemolyticus were reported in blood, in which it has shown similar pattern of 94% susceptibility against Vancomycin, 96% susceptibility against Linezolid, and a slightly lower susceptibility for Clindamycin (38%).16
In our study, 62.5% of Staphylococcus aureus bacteremia were due to methicillin-resistant Staphylococcus aureus (MRSA). These rates were comparable to the study conducted by Tak et al. and Wyllie et al. who reported 59% and 50% bacteremia by MRSA strain respectively.19 Contrary to this, the rates of MRSA were seen zero % in a study done by Duan et al.14 This difference may be due to different infection cleaning practices.
Staphylococcus aureus isolated in blood samples were 100% susceptible for Teicoplanin, followed by Tetracycline and Linezolid (75%) and susceptibility to Vancomycin, Gentamicin, Clindamycin and Erythromycin was 50% each in our study. Whereas, in a study conducted by Tak et al. and Wyllie et al. Staphylococcal isolates were 100% susceptible to Vancomycin, Teicoplanin and Linezolid.19 The reason of reduced susceptibility in our study may be due to prolonged use of the antimicrobials during the immunocompromised state of patients in ICU stay.
From the samples received from PICU, Escherichia coli, Acinetobacter spp. and Pseudomonas species were predominantly isolated amongst Gram-negative bacteria. The susceptibility pattern of Escherichia coli were found good against Fluoroquinolones and Tigecycline with 100% susceptibility, followed by Colistin, Aminoglycosides and Carbapenems (87.5%). In contrast to our study, only 0.7% of E. coli were found in a study done by Rezk et al., which were non-MDR.20
Acinetobacter species was found 100% resistant to majority of the antibiotics, except Minocycline, Colistin and Amikacin which showed very low level of susceptibility. Similar pattern was seen in a study done by Rezk et al. in Egypt, in which all Acinetobacter species were resistant to ampicillin/sulbactam, cefoxitin, ceftazidime, cefpodoxime, cefotaxime, ceftriaxone, imipenem, meropenem, amikacin, gentamicin, tobramicin, ciprofloxacin, levofloxacin, and norfloxacin. But low level of sensitivity was seen against Tetracycline and Doxycycline. The susceptibility for Pseudomonas aeruginosa in our study was maximum for Meropenem and minimum for Piperacillin-tazobactam. In a study by Rezk et al., Meropenem was 100% resistant, may be due to injudicious use of higher antimicrobials in their set up, whereas susceptibility for Pip-taz was 30%, which was almost similar to our study.20 A similar observation has been reported in a Palestinian study which reported that meropenam and amikacin were the most effective antibiotics against Pseudomonas aeruginosa.21 In another study in Pakistan, nearly two-third Pseudomonas aeruginosa were resistant to ceftazidime, imipenam, aztreonam and ofloxacin; while the majority of isolates demonstrated resistance to four or more antibiotics.22 This multidrug resistance indicates that even a combination of antibiotics may be ineffective in settings where Pseudomonas is a major cause of nosocomial infection.
In NICU, predominant bacteria were Klebsiella pneumoniae and Acinetobacter baumannii. In our study, >70% of Klebsiella pneumoniae were susceptible to Colistin and Tigecycline. Whereas, susceptibility to carbapenems, cephalosporins and other antimicrobials were very low. This is in contrast to the study done by Duan et al., where the susceptibility to carbapenems and other antimicrobials were high. K. pneumoniae is a common cause of healthcare-acquired infections, and one of the key pathogens in BSIs.23 Increased use of carbapenems has contributed significantly to the emergence of carbapenem-resistant K. pneumoniae (CRKP) strains.24,25 Acinetobacter baumannii was the second most predominant bacteria isolated from NICU settings. It showed good sensitivity for Minocycline and colistin. Whereas, all other antimicrobials like aminoglycosides, cephalosporins, carbapenems, fluoroquinolones, etc. showed very high resistance against Acinetobacter baumannii. The reason may be due to the prolonged ICU stay of the patients and injudicious use of antimicrobial. Susceptibility for Minocycline was moderate and was very low against all other antimicrobials in a study done by Duan et al. Similarly, the low level of susceptibility against Minocycline was seen in a study done by Rezk. et al. Multidrug-resistant bacteria such as carbapenem resistant Enterobacteriaceae (CRE) and carbapenem resistant Acinetobacter baumannii (CRAB) have been increasing constantly in recent years.
Summary
Increasing emergence of MDR organisms represents a global threat to the patients admitted in ICU, especially in paediatric age group. The prevalence of Staphylococcus aureus and CONS were high in PICU, whereas, in NICU, Klebsiella pneumoniae and Acinetobacter baumannii were predominantly seen. Methicillin-resistant CONS were found in 66% isolates of CONS in blood samples. 50% of these were found significant. These were found to be highly susceptible for Linezolid, Vancomycin and Clindamycin.
Staphylococcus aureus showed good sensitivity against Teicoplanin, Linezolid, Rifampin and suscepibility tetracyclines. Whereas, it showed moderate susceptibility against Vancomycin.
In NICU, the predominant bacteria were Klebsiella pneumoniae and Acinetobacter baumannii.
Majority of Klebsiella pneumoniae were susceptible to Colistin and Tigecycline. Whereas, they showed moderate susceptibility and resistance to other antimicrobials. This showed the MDR pattern of this organism.
Acinetobacter baumannii was the second most predominant bacteria isolated from NICU settings. It showed good sensitivity for Minocycline and colistin. Whereas, all other antimicrobials like aminoglycosides, cephalosporins, carbapenems, fluoroquinolones, etc. showed very high resistance against Acinetobacter baumannii.
The distribution of prevalent microorganisms and their antibiotic susceptibility revealed a high divergence among BSIs in PICU & NICU from a tertiary care hospital. Therefore, different antibiotic therapies for various wards and distinct age groups are recommended, for strengthening the
Infection prevention and control strategies for preventing the emergence and spread of highly antibiotic-resistant bacteria.
Gram-positive bacteria were predominant as compared to Gram-negative bacteria in PICU settings. CONS were predominantly isolated. Majority of them were Methicillin resistant CONS. Linezolid was found to be the best Antimicrobial agent against MRCONS.
In NICU, Gram-negative bacteria were more common. Klebsiella pneumoniae was the predominant bacteria. The best antimicrobial agents against Klebsiella pneumoniae were Colistin and Tigecycline.
The other predominant microorganism in NICU was Acinetobacter baumannii. It showed good sensitivity for Colistin and Minocycline.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Shri Guru Ram Rai Institute of Medical & Health Sciences, Dehradun, India, under Ref. No. SGRR/IEC/02/24.
- Halim MMA, Eyada IK, Tongun RM. Prevalence of multidrug drug resistant organisms and hand hygiene compliance in surgical NICU in Cairo University Specialized Pediatric Hospital. Egyptian Pediatric Association Gazette. 2018;66(4):103-111.
Crossref - Gajul SV, Mohite ST, Mangalgi SS, Wavare SM, Kakade SV. Klebsiella pneumoniae in septicemic neonates with special reference to extended spectrum β-lactamase, AmpC, metallo β-lactamase production and multiple drug resistance in tertiary care hospital. J Lab Physicians. 2015;7(1):32-37.
Crossref - Malini A, Banaji N, Shanthi AK. Profile of Multidrug Resistant Isolates from Paediatric Patients in a Tertiary Care Hospital, Puducherry. J Clin Diagn Res. 2017;11(12):DC06-DC10).
Crossref - Knippenberg R, Lawn JE, Darmstadt GL, et al. Systematic scaling up of neonatal care in countries. Lancet. 2005;365(9464):1087-1098.
Crossref - Waters D, Jawad I, Ahmad A, et al. Aetiology of community-acquired neonatal sepsis in low- and middle-income countries. J Glob Health. 2011;1:154-70.
- Droz N, Hsia Y, Ellis S, Dramowski A, Sharland M, Basmaci R. Bacterial pathogens and resistance causing community acquired paediatric bloodstream infections in low- and middle-income countries: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2019;8:207.
Crossref - Akinkugbe O, Cooke FJ, Pathan N. Healthcare-associated bacterial infections in the paediatric ICU. JAC Antimicrob Resist. 2020;2(3):dlaa066.
Crossref - Malagi NAN, Sushma U, Thangavelu S, et al. Study of incidence, microbiological profile of nosocomial infections in pediatric intensive care unit of tertiary care center. Int J Contemp Pediatr. 2023;10(8):1258-1261.
Crossref - Ibrahim HMA, Taha GEMM, Ibrahim NH, El Malah WM, Anwar MM. Prevalence of multidrug resistant organisms in neonatal and pediatric intensive care Units of Beni-Suef University Hospital. Egypt J Med Microbiol. 2019;28(2):27-35.
Crossref - Singh S, Dhawan B, Kapil A, et al. Coagulase-negative staphylococci causing blood stream infection at an Indian tertiary care hospital: Prevalence, antimicrobial resistance and molecular characterisation. Indian J Med Microbiol. 2016;34(4):500-505.
Crossref - Siddhu SK, Malhotra S, Devi P, Tuli AK. Significance of coagulase negative Staphylococcus from blood cultures: persisting problems and partial progress in resource constrained settings. Iran J Microbiol. 2016;8(6):366-371.
- Keim LS, Torres-Filho SR, Silva PV, Teixeira LA. Prevalence, aetiology and antibiotic resistance profiles of coagulase negative staphylococci isolated in a teaching hospital. Braz J Microbiol. 2011;42(1):248-255.
Crossref - Tak V, Mathur P, Lalwani S, Misra MC. Staphylococcal blood stream infections: Epidemiology, resistance pattern and outcome at a level 1 Indian trauma care center. J Lab Physicians. 2013;5(1):46-50.
Crossref - Duan N, Sun L, Huang C, Li H, Cheng B. Microbial Distribution and Antibiotic Susceptibility of Bloodstream Infections in Different Intensive Care Units. Front Microbiol. 2021;12:792282.
Crossref - Singhi S, Ray P, Mathew JL, Jayashree M, Dhanalakshmi. Nosocomial Bloodstream Infection in a Pediatric Intensive Care Unit. Indian J Paediatrics. 2008;75:25-30.
Crossref - Putra IW, Dharamwati I, Setyaningtyas A, et al. Microbial pattern and antibiotic susceptibility in pediatric intensive care unit Dr. Soetomo hospital, Surabaya. Indonesian Journal of Tropical and Infectious Disease. 2019;7(5):122-130.
Crossref - Maham diS, Fallah F, Gholinejad Z, Seifi A, Hoseini-Alfatemi SM. Bacterial etiology and antibiotic resistance pattern of pediatric bloodstream infections: a multicenter based study in Tehran, Iran. Ann Ig. 2018;30(4):337-345.
Crossref - Silago V, Mruma EC, Msemwa B, et al. Predominance of Acinetobacter spp., Harboring the blaIMP Gene, Contaminating the Hospital Environment in a Tertiary Hospital in Mwanza, Tanzania: A Cross-Sectional Laboratory-Based Study.Pathogens. 2022;11(1):63.
Crossref - Wyllie DH, Crook DW, Peto TEA. Mortality after Staphylococcus aureus bacteremia in two hospitals in Oxfordshire, 1997-2003: Cohort study. BMJ. 2006;333(7562):281.
Crossref - Rezk AR, Bawady SA, Omar NN, et al. Incidence of emerging multidrug-resistant organisms and its impact on the outcome in the pediatric intensive care. Egyptian Pediatric Association Gazette. 2021;69:25.
Crossref - Astal Z. Susceptibility patterns in Pseudomonas aeruginosa causing nosocomial infections. J Chemother. 2004;16(3):264-268.
Crossref - Sarwari A, Hasan R, Lim CB, Ng Y, Ng C, Zaman S. PCR identification and automated ribotyping of Pseudomonas aeruginosa clinical isolates from intensive care patients. Scand J Infect Dis. 2004;36(5):342-349.
Crossref - Kern WV, Rieg S. Burden of bacterial bloodstream infection-a brief update on epidemiology and significance of multidrug-resistant pathogens. Clin Microbiol Infect. 2020;26(2):151-157.
Crossref - Landman D, Bratu S, Kochar S, et al. Evolution of antimicrobial resistance among Pseudomonas aeruginosa, Acinetobacter baumannii and Klebsiella pneumoniae in Brooklyn, NY. J Antimicrob Chemother. 2007;60(1):78-82.
Crossref - Girometti N, Lewis RE, Giannella M, et al. Klebsiella pneumoniae bloodstream infection: epidemiology and impact of inappropriate empirical therapy. Medicine. 2014;93(17):298-309.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.