


ISSN: 0973-7510
E-ISSN: 2581-690X
The presence of ESBLs and CRE in E. coli and Klebsiella pneumoniae poses a significant challenge in healthcare and community settings. These enzymes can confer resistance to multiple antibiotics, limiting treatment options for infections caused by these strains. This resistance complicates infection management, leading to prolonged illness, increased healthcare costs, and higher mortality. This cross-sectional study, conducted from 2021 to 2022 at three hospitals in the northern border region of Saudi Arabia, involved collecting 541 samples from various wards and units. Samples were inoculated on blood-agar and MacConkey’s media, incubated overnight at 37°C, and analyzed for growth. Antibiotic susceptibility was tested using the “MicroScan WalkAway-96 SI-automated system. A total of 541 positive cases were collected from three major cities in the northern border territory of Saudi Arabia. Observations show that E. coli (18.66%, n = 101) was the most prominent pathogen, compared to Klebsiella pneumoniae (9.9%, n = 54). Females were more prone to ESBL-producing E. coli infections, with 67% having a urinary tract infection, whereas male patients were more predisposed to respiratory K. pneumoniae infections (54% compared to females at 46%). Out of 155 samples, 49.01% were ESBL-producing E. coli, and 20.38% were ESBL+CRE. Furthermore, 15.68% of K. pneumoniae were ESBL producers. E. coli showed resistance to 92% of ampicillin, 90% of oxacillin, 79% of ceftazidime, 76% of cefepime, 57% of aztreonam, and 53% of cephalothin, while amikacin (85%), imipenem, and meropenem were effective. Klebsiella pneumoniae showed 74% resistance to ampicillin, 67% to ceftazidime, 63% to co-trimoxazole, 57% to amoxicillin-clavulanate, and 42% to aztreonam. The sensitive antibiotics were imipenem (46%), aztreonam (42%), and amikacin (44%). The results are both intriguing and alarming. It is crucial to address the spread of ESBL and CRE-producing organisms.
Carbapenem-resistant Enterobacteriaceae, Prevalence, Infection, ESBL, CRE
Multidrug resistance (MDR) refers to the ability of microorganisms to withstand multiple structurally and functionally distinct drugs, often due to the overexpression of efflux pumps and other resistance mechanisms.1 The emergence and spread of antibiotic resistance among pathogenic bacteria, particularly Escherichia coli and Klebsiella pneumoniae, pose a significant global challenge in healthcare settings. Notably, Extended-Spectrum Beta-Lactamase (ESBL) and Carbapenem-Resistant Enterobacteriaceae (CRE) production in these bacterial species have garnered substantial attention due to their impact on treatment efficacy and patient outcomes.2,3
In urinary tract and respiratory tract infections, MDR occurs when pathogens develop resistance to multiple commonly used antibiotics, complicating therapy and increasing the risk of treatment failure and recurrence. ESBLs, enzymes capable of hydrolyzing a wide range of beta-lactam antibiotics including penicillin and cephalosporin, are increasingly prevalent among clinical isolates of E. coli and K. pneumoniae, conferring resistance and complicating infection management.4-6
Conversely, CRE strains, characterized by their resistance to carbapenem antibiotics, represent a more alarming scenario. Klebsiella pneumoniae and, to a lesser extent, Escherichia coli, produce carbapenemases such as Klebsiella pneumoniae carbapenemases (KPC) and New Delhi metallo-beta-lactamase (NDM), leading to high-level resistance to this critical class of antibiotics.7 The presence of ESBL and CRE-producing E. coli and K. pneumoniae significantly limits treatment options, resulting in prolonged illnesses, increased mortality rates, and elevated healthcare costs. Furthermore, these multidrug-resistant strains present significant challenges to infection control practices in healthcare settings. The raises concerns about their potential threats, underscoring the urgent need to investigate new drugs that could be effective against multidrug-resistant microorganisms.8-10
The alarming increase in ESBL prevalence is being reported worldwide, including in Saudi Arabia, which has a large expatriate population from South Asia where antimicrobial resistance is common. The annual Hajj pilgrimage also poses a risk for infectious illness transmission, further contributing to the rising prevalence of drug-resistant bacteria in the kingdom.11,12
Current study aims to comprehensively analyze the epidemiology, clinical implications, and recent trends associated with ESBL and CRE production in Escherichia coli and Klebsiella pneumonia in Saudi Arabia, highlighting the urgent need for effective strategies to combat these resistant pathogens. Specifically, we investigated the prevalence of infections caused by CRE and ESBL-producing bacteria in the Northern Border region of Saudi Arabia.
Study design
This cross-sectional study was performed from 2021 to 2022 at the microbiology departments of three hospitals in the northern border region of Saudi Arabia: Prince Abdulaziz bin Musaed Hospital, Arar; Turaif General Hospital, Turaif; and Rafha Central Hospital, Rafha.
Sample collection
Overall, 541 samples, including wound, blood, sputum, pus, urine, tracheal secretion, catheters, high vaginal discharge, breast discharge, femoral and tracheal tips, diabetic foot, ear swab, eye swab, mouth swab, bronchoalveolar lavage, and pleural fluid, were collected from patients at these three hospitals as part of routine patient care. The sample collection began in 2021 and lasted through the end of 2022. Data were gathered from eight medical and surgical wards, including the outpatient department, emergency room, intensive care unit, surgical intensive care unit, maternity and childcare, artificial kidney unit, female medical ward, male medical and surgical ward, and pediatric ward. The samples were then immediately sent to the laboratory for additional analysis.
Sample procedures
For colony formation, samples were inoculated on blood-agar and MacConkey’s media and incubated overnight at 37°C. Brain heart infusion broth was used to inoculate blood samples. After incubation, a drop was inoculated on media and cultured for 7 days at 37°C. A negative result indicates the absence of growth on the blood sample from the clinical specimens. The isolates were observed as pure colonies, and growth was evaluated for further testing. Mixed growing cultures were excluded during the observation of the media.
Laboratory analysis for antibiotic susceptibility
For laboratory identification, the “MicroScan WalkAway-96 SI-automated system” was used. The Neg/BP/Combo 30-B1017-306E group panels were used for antimicrobial susceptibility testing. All operations were carried out as directed by the manufacturer.
Tests for ESBL confirmatory (Phenotypic Confirmatory Disc Diffusion Test PCDDT)
PCDDT was used to confirm if the isolate was positive for ESBL or not. Ceftazidime (CAZ-30 g), ceftazidime with clavulanic acid (CAC-30/10 g), cefotaxime (CTX-30 g), and cefotaxime-clavulanic acid (CTX/C-30/10 g) discs were distributed at a minimum distance of 24 mm on Mueller Hinton Agar (MHA) inoculated with isolates screened for ESBL production. The isolates were confirmed to be ESBL producers if the zone size increased by more than 5 mm when using ceftazidime/clavulanic acid and cefotaxime-clavulanic acid compared to ceftazidime or cefotaxime alone.13
Confirmation test
The CLSI breakpoints are used to interpret the MIC (minimum inhibitory concentration) obtained for aztreonam, cefotaxime, and ceftriaxone with or without clavulanic acid. The MIC data was used as a major indicator for ESBL formation in a confirmatory test addressed by the CLSI guideline.14
Statistical analysis
Descriptive statistics were examined, and all the findings were represented as percentages and frequencies. Data were cross tabulated to express outcomes in relation to various age categories. SPSS version 20 was used to conduct the statistical analysis.
Demographic studies and prevalence of pathogens in northern borders
Overall, 541 positive samples were collected from three major cities in the northern border region of Saudi Arabia. Most of the samples were from males (n = 305, 55%), with the highest age group being over 56 (n = 175, 28%). The collected samples included sputum (n = 168, 30%), wound site (n = 142, 26%), and urine (n = 76, 14%) cases. The prevalence of ESBL was found to be 0.76%, with E. coli accounting for 18.66% (n = 101) and Klebsiella pneumoniae for 9.9% (n = 54) as shown in Table 1. Male patients were more predisposed to K. pneumoniae infection (54%) compared to females (46%), primarily in sputum samples from those suffering from respiratory infections.
Table (1):
Gender, age, type of sample, type of microorganisms isolated from different clinical samples (n = 566)
| Variable | Categories | Frequency | Percentage |
|---|---|---|---|
| Gender | Male | 305 | 55% |
| Female | 252 | 45% | |
| Age (years) |
>1 | 42 | 7% |
| 1-5 | 35 | 6% | |
| 6-15 | 41 | 7% | |
| 16-25 | 58 | 10% | |
| 26-35 | 45 | 8% | |
| 36-45 | 40 | 7% | |
| 46-55 | 73 | 13% | |
| 56-65 | 57 | 10% | |
| <56 | 175 | 28% | |
| Sample vaginal discharge |
Sputum | 168 | 30% |
| Blood | 24 | 4% | |
| Urine | 76 | 14% | |
| Wound | 142 | 26% | |
| Pus | 43 | 7% | |
| Tracheal secretions | 45 | 7% | |
| Catheters | 14 | 3% | |
| High | 9 | 2% | |
| Breast discharge | 9 | 1% | |
| Femoral & tracheal tip | 3 | 0.5% | |
| Diabetic foot | 3 | 0.5% | |
| Ear swab | 6 | 1% | |
| Eye swab | 6 | 1% | |
| Mouth swab | 3 | 0.5% | |
| Bronchoalveolar lavage | 13 | 2% | |
| Pleural fluid | 2 | 0.5% | |
| Type of isolate |
E. coli | 107 | 19% |
| P. stuartii | 6 | 1% | |
| K. pneumoniae | 54 | 10% | |
| P. mirabilis | 64 | 11% | |
| P. aeruginosa | 67 | 11% | |
| S. aureus | 36 | 6% | |
| S. marcescens | 4 | 1% | |
| Actinobacteria | 37 | 6% | |
| Gram-positive cocci | 31 | 5% | |
| Gram-negative bacilli | 45 | 8% | |
| Gram-negative cocci | 7 | 1% | |
| Bacteroides | 21 | 4% | |
| S. pyogenes | 4 | 1% | |
| S. epidermidis | 2 | 1% | |
| Beta-Haemolyticus streptococcus | 45 | 8% | |
| Alpha-Haemolyticus streptococcus | 20 | 4% | |
| Staphylococcus | 17 | 3% | |
| coagulase-negative |
A variety of clinical samples were observed (Figure 1 and Table 1). Although different pathogens were isolated, the highest percentage of E. coli infection (19%) was observed, followed by other organisms: P. mirabilis (11%), P. aeruginosa (11%), and K. pneumoniae (10%), with the rest as shown in Figure 1. These included P. stuartii, S. aureus, S. marcescens, Actinobacteria, Gram-positive cocci, Gram-negative bacilli, Gram-negative cocci, Bacteroids, S. pyogenes, S. epidermidis, Beta-haemolytic Streptococcus, Alpha-haemolytic Streptococcus, and coagulase-negative Staphylococcus.
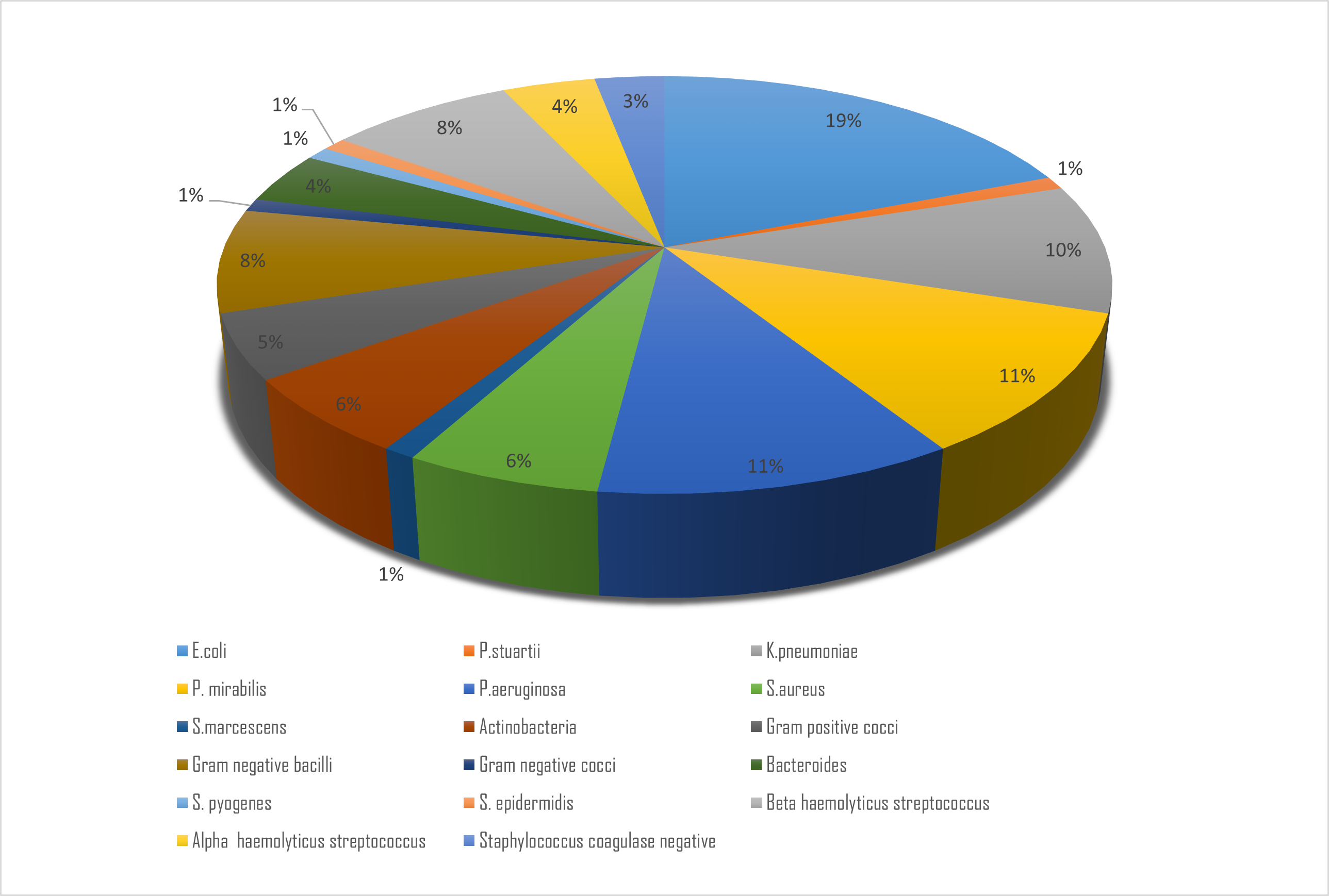
Figure 1. This pie chart illustrates the distribution of different types of microorganisms isolated from various clinical samples. Each slice represents a specific microorganism, showing the proportion of the total 566 isolates that each microorganism comprises represented as percentage
Susceptibility profile E. coli
Female patients were found to be more susceptible to E. coli infections, with 67% of cases among 101 samples, particularly suffering from urinary tract infections. The antibiotic susceptibility profile indicated that E. coli was resistant to the following drugs: 92% to ampicillin, 90% to oxacillin, 79% to ceftazidime, 76% to cefepime, 57% to aztreonam, and 53% to cephalothin. The drugs to which E. coli was most susceptible were amikacin (85%), followed by imipenem and meropenem, both with 78% susceptibility, as depicted in Table 2 and Figure 2.
Table (2):
Susceptibility profile E. coli (n = 101)
| Variable | Categories | Frequency | Percentage | |
|---|---|---|---|---|
| Gender of patient | Male | 34 | 34% | |
| Female | 67 | 67% | ||
| Sample | pus | 9 | 9% | |
| Wound | 7 | 7% | ||
| Urine | 59 | 59% | ||
| Blood | 11 | 11% | ||
| Bronchioalveolar lavage | 1 | 1% | ||
| Ear swab | 2 | 2% | ||
| High vaginal swab | 4 | 4% | ||
| Sputum | 6 | 6% | ||
| Catheters | 2 | 2% | ||
| Susceptibility profile | Amikacin | Resistant | 7 | 7% |
| Susceptible | 85 | 85% | ||
| Imipenem | Resistant | 5 | 5% | |
| Susceptible | 78 | 78% | ||
| Ertapenem | Resistant | 15 | 15% | |
| Susceptible | 4 | 4% | ||
| Meropenem | Resistant | 10 | 10% | |
| Susceptible | 78 | 78% | ||
| Cefoxitin | Resistant | 14 | 14% | |
| Susceptible | 49 | 49% | ||
| Piperacillin- tazobactam | Resistant | 26 | 26% | |
| Susceptible | 62 | 62% | ||
| Cephalothin | Resistant | 53 | 53% | |
| Susceptible | 0 | 0% | ||
| Cefuroxime | Resistant | 51 | 51% | |
| Susceptible | 1 | 1% | ||
| Ceftazidime | Resistant | 79 | 79% | |
| Susceptible | 2 | 2% | ||
| Ceftriaxone | Resistant | 37 | 37% | |
| Susceptible | 1 | 1% | ||
| Cefepime | Resistant | 76 | 76% | |
| Susceptible | 2 | 2% | ||
| Cephazolin | Resistant | 4 | 4% | |
| Susceptible | 0 | 0% | ||
| Aztreonam | Resistant | 57 | 57% | |
| Susceptible | 2 | 2% | ||
| Ampicillin | Resistant | 92 | 92% | |
| Susceptible | 6 | 6% | ||
| Amoxicillin –clavulanate | Resistant | 39 | 39% | |
| Susceptible | 32 | 32% | ||
| Co-trimoxazole | Resistant | 70 | 70% | |
| Susceptible | 30 | 30% | ||
| Oxacillin | Resistant | 90 | 90% | |
| Susceptible | 1 | 1% | ||
| Methicillin | Resistant | 9 | 9% | |
| Susceptible | 1 | 1% | ||
| Cefotaxime | Resistant | 48 | 48% | |
| Susceptible | 0 | 0% | ||
| Tobramycin | Resistant | 16 | 16% | |
| Susceptible | 19 | 19% | ||
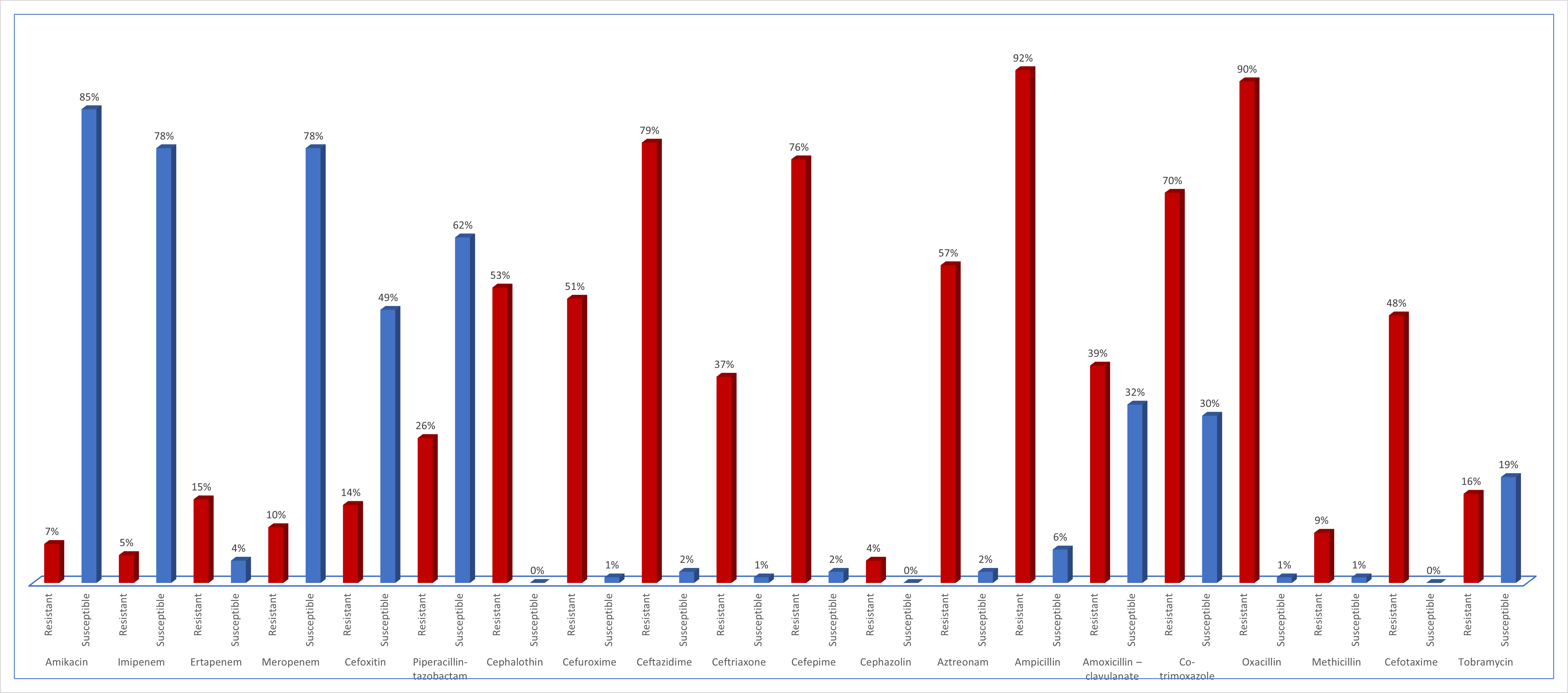
Figure 2. This bar graph illustrates the antimicrobial susceptibility of Escherichia coli isolates to various antibiotics. Each bar represents the percentage of isolates that are susceptible, or resistant to a specific antibiotic, providing a clear visualization of the effectiveness of each antimicrobial agent against E. coli
Susceptibility profile of K. pneumoniae
In addition, Klebsiella pneumoniae exhibited varying degrees of resistance to antibiotics according to its susceptibility profile. Ampicillin was found to be the most resistant medication (74%), followed by ceftazidime (67%), co-trimoxazole (63%), amoxicillin-clavulanate (57%), and aztreonam (42%). However, certain antibiotics showed sensitivity against K. pneumoniae, with imipenem (46%), aztreonam (42%), and amikacin (44%) being identified as effective options. Regarding Gram-negative cocci, the antibiotic susceptibility profile (n=7) revealed notable resistance to co-trimoxazole (57%), while amikacin demonstrated susceptibility (71%). Conversely, Gram-positive cocci exhibited resistance to cefoxitin (57%) and ampicillin (70%), with a susceptibility of 60% to imipenem, as depicted in Figure 3 and Table 3.
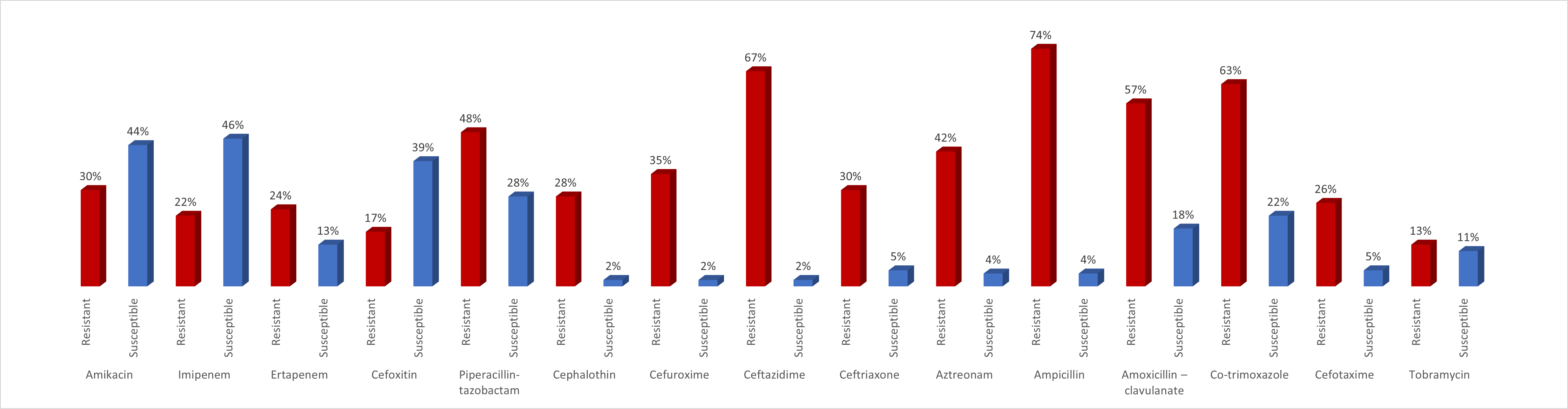
Figure 3. This bar graph illustrates the antimicrobial susceptibility of Klebsiella pneumoniae isolates to various antibiotics. Each bar represents the percentage of isolates that are susceptible, intermediate, or resistant to a specific antibiotic, providing a clear visualization of the effectiveness of each antimicrobial agent against K. pneumonia
Table (3):
Susceptibility profile of K. pneumoniae (n = 54)
| Variable | Categories | Frequency | Percentage | |
|---|---|---|---|---|
| Gender of patient | Male | 29 | 54% | |
| Female | 25 | 46% | ||
| Sample | Blood | 10 | 18% | |
| Bronchoalveolar lavage | 5 | 9% | ||
| Urine | 10 | 18% | ||
| Pus | 5 | 9% | ||
| Sputum | 18 | 33% | ||
| Tracheal secretions | 3 | 5% | ||
| Vaginal swab | 2 | 4% | ||
| Susceptibility profile | Amikacin | Resistant | 16 | 30% |
| Susceptible | 24 | 44% | ||
| Imipenem | Resistant | 12 | 22% | |
| Susceptible | 25 | 46% | ||
| Ertapenem | Resistant | 13 | 24% | |
| Susceptible | 7 | 13% | ||
| Cefoxitin | Resistant | 9 | 17% | |
| Susceptible | 21 | 39% | ||
| Piperacillin- tazobactam | Resistant | 26 | 48% | |
| Susceptible | 15 | 28% | ||
| Cephalothin | Resistant | 15 | 28% | |
| Susceptible | 1 | 2% | ||
| Cefuroxime | Resistant | 19 | 35% | |
| Susceptible | 1 | 2% | ||
| Ceftazidime | Resistant | 36 | 67% | |
| Susceptible | 1 | 2% | ||
| Ceftriaxone | Resistant | 16 | 30% | |
| Susceptible | 3 | 5% | ||
| Aztreonam | Resistant | 23 | 42% | |
| Susceptible | 2 | 4% | ||
| Ampicillin | Resistant | 40 | 74% | |
| Susceptible | 2 | 4% | ||
| Amoxicillin –clavulanate | Resistant | 31 | 57% | |
| Susceptible | 10 | 18% | ||
| Co-trimoxazole | Resistant | 34 | 63% | |
| Susceptible | 12 | 22% | ||
| Cefotaxime | Resistant | 14 | 26% | |
| Susceptible | 3 | 5% | ||
| Tobramycin | Resistant | 7 | 13% | |
| Susceptible | 6 | 11% | ||
Multidrug resistance, ESBL and CRE producing E. coli and K. pneumoniae
For the total isolates of E. coli and K. pneumoniae (n = 155), initial screening for ESBL production was performed using the Phenotypic Confirmatory Disc Diffusion Test (PCDDT). This test involves placing antibiotic disks, such as cefotaxime and ceftazidime, alone and in combination with a beta-lactamase inhibitor like clavulanic acid, on an agar plate inoculated with the bacteria. The presence of ESBLs is indicated by an enhanced zone of inhibition around the disc containing the inhibitor compared to those without it.15
If the initial screening test is positive or equivocal, a confirmatory test is necessary. This often involves more specific methods like the E-test or broth microdilution method, following standardized protocols.16 These methods measure the minimum inhibitory concentrations (MICs) of certain antibiotics both with and without beta-lactamase inhibitors to confirm ESBL production. CRE bacteria are a subset of Enterobacteriaceae that have acquired resistance to carbapenems, potent antibiotics often considered the last line of defense against multidrug-resistant bacterial infections. These bacteria produce enzymes known as carbapenemases, which can break down and render carbapenem antibiotics ineffective.17
Interestingly, out of 155 samples, 49.01% were ESBL-producing E. coli, and 20.38% were ESBL+CRE E. coli. Furthermore, 15.68% were ESBL-producing K. pneumoniae, 5.88% were K. pneumoniae resistant to aminoglycosides, 1.96% were multidrug-resistant (MDR) K. pneumoniae, and 3.92% were ESBL+CRE K. pneumoniae (Figure 4).
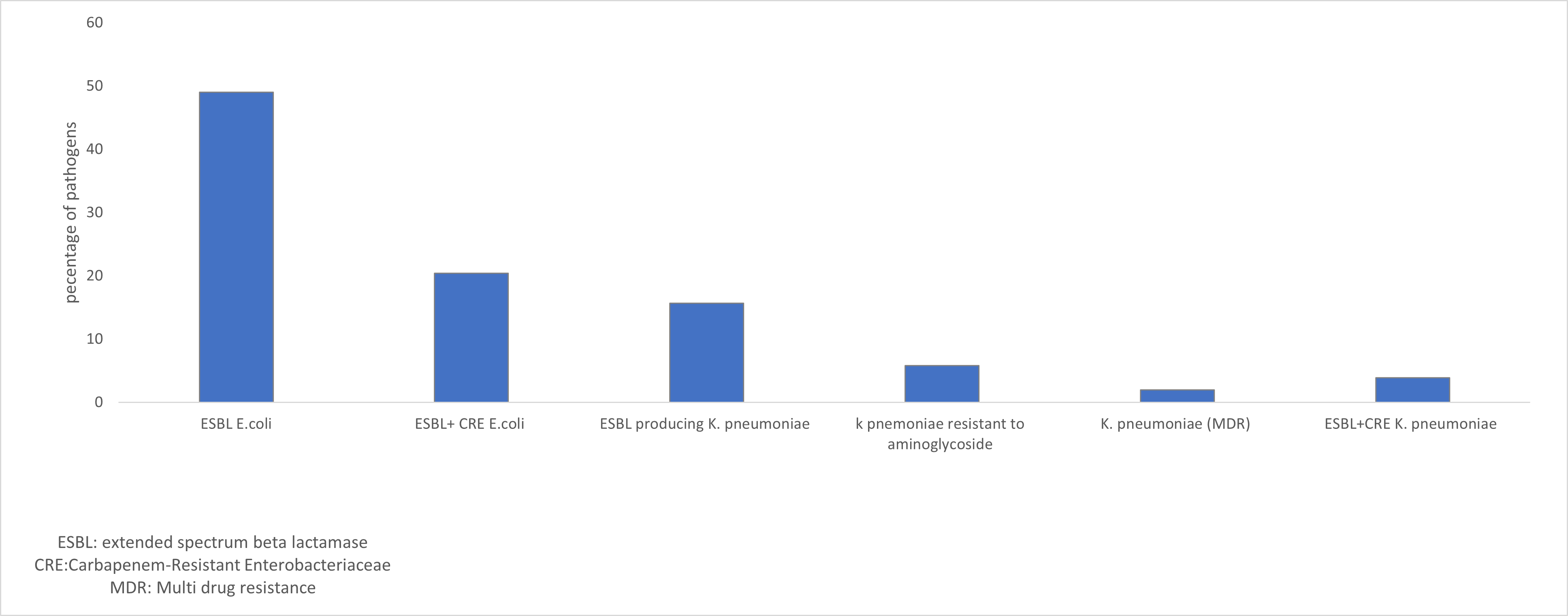
Figure 4. Bar graph depicts the prevalence of multidrug resistance (MDR), extended-spectrum beta-lactamase (ESBL) production, and carbapenem-resistant Enterobacteriaceae (CRE) among Escherichia coli and Klebsiella pneumoniae isolates. Each set of bars represents the percentage of isolates exhibiting MDR, ESBL production, and CRE production for both bacterial species
The emergence of Extended-Spectrum Beta-Lactamase (ESBL) producing Escherichia coli (E. coli) represents a major global public health concern due to its increasing prevalence and the ensuing challenges within healthcare settings. ESBLs, enzymes that provide resistance to a wide range of beta-lactam antibiotics like penicillin and cephalosporin, render these drugs ineffective against ESBL-producing bacteria.18
The prevalence of ESBL-producing E. coli in healthcare settings such as hospitals, clinics, and long-term care facilities, poses a significant threat, leading to prolonged hospital stays, increased healthcare costs, and higher mortality rates.19 Concurrently, the emergence of ESBL E. coli in community-acquired infections presents a challenge in outpatient management and contributes to the spread of antibiotic resistance beyond healthcare environments.18,19
Prevalence rates of ESBL-producing
E. coli vary across regions and settings, influenced by factors like geographic location, antimicrobial usage patterns, infection control practices, and population demographics.20 In our study, female candidates were more susceptible to UTI-related E. coli infection, with 18.66%, consistent with other studies.21 Beta-lactamases were found to be present in 49.01% of ESBL-producing E. coli and 15.68% in ESBL+ CRE, consistent with other studies.22 Understanding the epidemiology and prevalence trends of ESBL E. coli is crucial for developing effective strategies for infection control, antibiotic stewardship, and patient management.
The results of the current study offer valuable insights into the prevalence and antibiotic susceptibility patterns of ESBL-producing E. coli and K. pneumoniae in the northern border territory of Saudi Arabia. The study, which collected 541 positive cases from three major cities, highlights E. coli as the most prominent pathogen, accounting for 18.66% of cases, followed by Klebsiella pneumoniae at 9.9%.
Gender-based analysis revealed intriguing trends in infection susceptibility. Females exhibited a higher susceptibility to ESBL-producing E. coli, with 67% experiencing urinary tract infections. Conversely, male patients showed a higher predisposition to respiratory infections caused by K. pneumoniae, with 54% of cases compared to 46% in females. These gender-specific variations in infection sites may be attributed to anatomical and physiological differences, and further investigations could shed light on the underlying factors.23
The study also assessed the prevalence of ESBL production among the collected samples. Out of 155 samples, ESBL-producing E. coli accounted for 49.01%, while ESBL+ CRE was present in 20.38% of cases. Among K. pneumoniae isolates, 15.68% were found to produce ESBL. These findings underscore the significance of ESBLs in the studied region, emphasizing the need for continued surveillance and effective infection control measures.24
Antibiotic susceptibility profiles revealed concerning levels of resistance among E. coli and K. pneumoniae isolates. ESBL-producing E. coli demonstrated high resistance rates to ampicillin (92%), oxacillin (90%), ceftazidime (79%), cefepime (76%), aztreonam (57%), and cephalothin (53%). However, some antibiotics, such as amikacin (85%), imipenem, and meropenem, remained effective against E. coli, indicating potential treatment options. Other studies have reported similar findings regarding the resistance profiles of ESBL-producing Escherichia coli and Klebsiella pneumoniae. One study found that ESBL-producing E. coli and K. pneumoniae showed high resistance rates to cefotaxime (100%) and significant resistance to other beta-lactam antibiotics.25 Another analysis reported that the average resistance rates of ESBL-producing E. coli and K. pneumoniae to cefpodoxime, cefixime, cefazolin, and ceftriaxone were above 98%.26 High resistance to penicillin and beta-lactam was observed in ESBL-positive isolates, with reported resistance rates reaching 100% for certain antibiotics. These studies corroborate the observed high resistance rates to multiple antibiotics among ESBL-producing E. coli and K. pneumoniae isolates, emphasizing the continued effectiveness of antibiotics like amikacin, imipenem, and meropenem.27,28
K. pneumoniae isolates, as indicated by their antibiotic susceptibility profiles, demonstrated significant resistance rates to ampicillin (74%), ceftazidime (67%), co-trimoxazole (63%), amoxicillin-clavulanate (57%), and aztreonam (42%). Noteworthy, imipenem (46%), aztreonam (42%), and amikacin (44%) were identified as effective antibiotics against K. pneumoniae.
Current findings emphasize the importance of careful antibiotic usage and the continual monitoring of resistance patterns.29 The observed resistance to commonly prescribed antibiotics highlights the dire need for the development and implementation of robust antimicrobial stewardship programs and antimicrobial policies to promote better use of these drugs in the hospital setting coupled with infection control programs.30 Furthermore, the susceptibility profiles identified in this study can assist clinicians in choosing appropriate antibiotics for treating infections caused by ESBL-producing E. coli and K. pneumoniae in the Northern border region of Saudi Arabia.
In conclusion, the study in three major cities of Saudi Arabia’s northern border region focused on infections caused by E. coli and Klebsiella pneumoniae. E. coli emerged as the predominant pathogen, while K. pneumoniae also contributed to the overall cases. Gender-specific trends were observed, with females more prone to ESBL-producing E. coli infections associated with urinary tract infections, and males showing a higher predisposition to respiratory infections caused by K. pneumoniae. Antibiotic susceptibility profiles highlighted the significance of emerging resistant pathogens, particularly ESBL-producing E. coli. Therefore, New antimicrobials, rapid diagnostic and antimicrobial susceptibility testing should be included for future antimicrobial stewardship interventions.
ACKNOWLEDGMENTS
The authors would like to thank the Department of Pharmaceutics, Faculty of Pharmacy Northern Border University, Rafha, Saudi Arabia, Prince Abdullah Bin Abdulaziz, Hospital Arar, Rafha Central Hospital and Turaif General Hospital Saudi Arabia.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
This study was funded by the Deanship of Scientific Research, Northern Border University, Arar, Saudi Arabia, with project number NBU-FFR-2615-2024-03
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Microbiology Laboratory of Prince Abdulaziz bin Musaed Hospital, Arar; Turaif General Hospital, Turaif; and Rafha Central Hospital, Rafha.
- Alanazi M, Alqahtani HM, Alshammari MK, et al. Infection Prevalence at a Tertiary Hospital in Hail, Saudi Arabia: A Single-Center Study to Identify Strategies to Improve Antibiotic Usage. Infect Drug Resist. 2023;16:3719-3728.
Crossref - Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657-686.
Crossref - Logan LK, Weinstein RA. The epidemiology of carbapenem-resistant Enterobacteriaceae: the impact and evolution of a global menace. J Infect Dis. 2017;215(Suppl 1):S28-S36.
Crossref - Bhatta DR, Hamal D, Shrestha R, et al. Burden of multidrug resistant respiratory pathogens in intensive care units of tertiary care hospital. Asian J Med Sci. 2019;10(2):14-19.
Crossref - Alzahrani MA, Sadoma HHM, Mathew S, Alghamdi S, Malik JA, Anwar S. Retrospective Analysis of Antimicrobial Susceptibility of Uropathogens Isolated from Pediatric Patients in Tertiary Hospital at Al-Baha Region, Saudi Arabia. Healthcare. 2021;9(11):1564.
Crossref - Shaikh S, Fatima J, Shakil S, et al. Antibiotic resistance and extended spectrum beta-lactamases: Types, epidemiology and treatment. Saudi journal of biological sciences. 2015;22(1):90-101.
- Peri AM, Doi Y, Potoski BA, et al. Antimicrobial treatment challenges in the era of carbapenem resistance. Diagnostic microbiology and infectious disease, 2019;94(4): 413-425.
- Kanj SS, Zeina AK. Current concepts in antimicrobial therapy against resistant gram-negative organisms: extended-spectrum β-lactamase–producing enterobacteriaceae, carbapenem-resistant enterobacteriaceae, and multidrug-resistant Pseudomonas aeruginosa. Mayo Clinic Proceedings. 2011; 86(3).
- Soomro S, Chidrawar VR, Imran M, Alshammari HO. Immunomodulating, anti-bacterial and anti-cancer potential of Za’atar (Thymus vulgaris) and its combination with essential oil (Olive and Balsam Oil). Int J Pharm Sci. 2019;10(8):3721-3726.
Crossref - Trecarichi EM, Tumbarello M. Antimicrobial-resistant gram-negative bacteria in febrile neutropenic patients with cancer: current epidemiology and clinical impact. Curr Opin Infect Dis. 2019;32(6):561-568.
- Soomro S, Alshammari HO, Alabbas YA. Awareness and knowledge about antibiotic use and resistance among students of Northern Border University Saudi Arabia. J Trop Dis. 2017;5(5):1000247.
Crossref - Saleh A-GA, Mohammed A-GS, Mahmoud GM. Epidemiology of Extended-Spectrum Beta-Lactamases (ESBLs)-Producing Bacteria in Different Regions in Saudi Arabia: A Systematic Review. Annu Res Rev Biol. 2018;26(5):1-11.
Crossref - Naseer F, Iqbal R, Ikram N, et al. Phenotypic cofirmatory disc diffusion test (PCDDT), double disc synergy test (DDST), E-test OS diagnostic tool for detection of extended spectrum beta lactamase (ESBL) producing Uropathogens. J Appl Biotechnol Bioeng. 2017;3(3): 344-349.
Crossref - Bostanoglu E, Demirbilek M, Aliskan HE, Colakoglu S, Gocmen JS. Interpretation of minimal inhibitory concentrations of extended spectrum beta lactamase producing Escherichia coli and Klebsiella spp. strains according to new Clinical Laboratory and Standards Institute (CLSI) criteria. Afr J Microbiol Res. 2013;7(6):498-503.
- Kumar D, Singh AK, Ali MR, et al. Antimicrobial susceptibility profile of extended spectrum β-lactamase (ESBL) producing Escherichia coli from various clinical samples. Infectious Diseases: Research and Treatment. 2014;7: IDRT-S13820
- Lalitha MK. Manual on antimicrobial susceptibility testing. Performance standards for antimicrobial testing: Twelfth Informational Supplement 56238; 2004: 454-456.
- Kardos N. CRE (Carbapenem Resistant Enterobacteriaceae) and the Globalization of Antimicrobial Resistance: Problems and Solutions. Sun Text Rev Biotechnol. 2020;1(1).
Crossref - Sivakumar M, Abass G, Vivekanandhan R, et al. Extended-spectrum beta-lactamase (ESBL) producing and multidrug-resistant Escherichia coli in street foods: a public health concern. J Food Sci Technol. 2021;58:1247-1261.
Crossref - Bezabih YM, Bezabih A, Dion M, et al. Comparison of the global prevalence and trend of human intestinal carriage of ESBL-producing Escherichia coli between healthcare and community settings: a systematic review and meta-analysis. JAC-Antimicrob Resist. 2022;4(3):dlac048.
Crossref - Canton R, Coque TM. The CTX-M b-lactamase pandemic. Curr Opin Microbiol. 2006;9(5):466-475.
Crossref - Huttner A, Hatz C, van den Dobbelsteen G, et al. Safety, immunogenicity, and preliminary clinical efficacy of a vaccine against extraintestinal pathogenic Escherichia coli in women with a history of recurrent urinary tract infection: a randomised, single-blind, placebo-controlled phase 1b trial. Lancet Infect Dis. 2017;17(5):528-537.
Crossref - Liu H, Wang Y, Wang G, et al. The prevalence of Escherichia coli strains with extended spectrum beta-lactamases isolated in China. Front Microbiol. 2015;6:133081.
Crossref - Szadvari I, Ostatnikova D, Durdiakova JB. Sex differences matter: Males and females are equal but not the same. Physiol Behav. 2023;259:114038.
Crossref - Aldrazi FA, Rabaan AA, Alsuliman SA, et al. ESBL expression and antibiotic resistance patterns in a hospital in Saudi Arabia: do healthcare staff have the whole picture?. J Infect Public Health. 2020;13(5):759-766.
Crossref - Mofolorunsho KC, Ocheni HO, Aminu RF, Omatola CA, Olowonibi OO. Prevalence and antimicrobial susceptibility of extended-spectrum beta lactamases-producing Escherichia coli and Klebsiella pneumoniae isolated in selected hospitals of Anyigba, Nigeria. Afr Health Sci. 2021;21(2):505-512.
Crossref - Keshi L, Weiwei X, Shoulin L, et al. Analysis of drug resistance of extended-spectrum beta-lactamases-producing Escherichia coli and Klebsiella pneumoniae in children with urinary tract infection. Saudi Med J. 2019;40(11):1111-1115.
Crossref - Santella B, Boccella M, Folliero V, et al. Antimicrobial Susceptibility Profiles of Klebsiella pneumoniae Strains Collected from Clinical Samples in a Hospital in Southern Italy. Can J Infect Dis Med Microbiol. 2024;2024:5548434.
Crossref - Najjuka CF, Kateete DP, Kajumbula HM, Joloba ML, Essack SY. Antimicrobial susceptibility profiles of Escherichia coli and Klebsiella pneumoniae isolated from outpatients in urban and rural districts of Uganda. BMC Res Notes. 2016;9:235.
Crossref - Bezabih YM, Bezabih A, Dion M, et al. Comparison of the global prevalence and trend of human intestinal carriage of ESBL-producing Escherichia coli between healthcare and community settings: a systematic review and meta-analysis. JAC-Antimicrob Resist. 2022;4(3):dlac048.
Crossref - Abayneh M, Tesfaw G, Abdissa A. Isolation of extended-spectrum b-lactamase-(ESBL-) producing Escherichia coli and Klebsiella pneumoniae from patients with community-onset urinary tract infections in Jimma University Specialized Hospital, Southwest Ethiopia. Can J Infect Dis Med Microbiol. 2018;2018:4846159.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.