


ISSN: 0973-7510
E-ISSN: 2581-690X
Insufficient vitamin D levels in the bloodstream, together with the presence of specific genetic variations known as single nucleotide polymorphisms (SNPs) within the VDR gene, have consistently been linked to a higher likelihood of contracting and experiencing more severe forms of various diseases such as the ongoing COVID-19 pandemic. We aimed to explore the potential relationship between vitamin D levels, Bsml and FOKI polymorphisms, and COVID-19 infection outcomes. A case-control study was conducted with COVID-19 patients and a control group of non-COVID-19 patients (n = 107 each). The associations between vitamin D status, polymorphisms, and COVID susceptibility were investigated. Participants diagnosed with COVID-19 exhibited an average age of 48.84 ± 12.18, while non-COVID-19 patients had an average age of 46.82 ± 9.903. Disease severity, assessed by the CT severity score, showed a negative correlation with the Vitamin D levels. Among participants with COVID-19, the mean level of vitamin D was 35.25 ± 9.40 ng/mL while non-COVID-19 patients showed 38.85 ± 9.40 ng/mL with a significant difference (p = 0.004**) although among COVID-19 cases, 87 (81.3%) individuals had sufficient vitamin D levels and non-severity of disease was more common i.e. 54 (50.5%) among the COVID patients who had sufficient level of Vitamin D. The study found no significant association between Vitamin D levels and rs1544410 Bsml polymorphism (p = 0.429). However, it is important to highlight a weak significant association observed between with Fok1 polymorphism (p = 0.049). These findings underscore the weak influence of genetic factors, particularly VDR Fok1 gene variants, in shaping an individual’s susceptibility to COVID-19. A significant difference in vitamin D status was observed between the COVID-19 and non-COVID-19 groups and lower level was observed in the COVID-19 infected patients. Furthermore, a weak significant association was observed between Fok1 rs2228570 genotype and COVID-19 susceptibility. Larger sample sizes are required to comprehensively understand the association between different genotypes and COVID-19 outcomes.
Vitamin D, COVID-19, rs2228750, Fok1, rs1544410, Bsm1, Genotyping Frequency, Alleles Frequency, Genetic Polymorphisms
Despite the large pandemic, the Coronavirus Disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), many aspects related to its occurrence and associated risk still lack.1 COVID-19 has significantly impacted numerous facets of society, including health, interpersonal connections, healthcare systems, sustainable development, psychological well-being, and everyday routines.2-8 COVID-19 has brought about extensive repercussions, manifesting as a spectrum of symptoms ranging from mild to severe respiratory illness. Typical indications include fever, cough, difficulty breathing, fatigue, bodily discomfort, and loss of taste or smell.9 Specific populations, such as older populations and individuals with existing health conditions, face an increased risk of severe complications.1 SARS-CoV-2 enters the host cells by interacting with Angiotensin-converting enzyme 2 (ACE2) receptors, primarily found in alveolar type-II pneumocytes, kidney epithelial cells, and enterocytes in the small intestine.10 Inadequate vitamin D levels are a significant health issue, affecting one billion people worldwide. Vitamin D is vital in maintaining optimal bone metabolism and mineral balance. It acts as an essential nutrient and functions as a fat-soluble secosteroid prohormone. The biologically active form of Vitamin D3, known as calcitriol, exerts its effects by binding to vitamin VDRs in the gastrointestinal tract, lungs, bones, and immune cells.11 Despite the abundance of VDRs in lung tissue, the exact role of vitamin D-VDR signaling in lung related are not fully understood. Gromova et al.12 conducted a study that revealed vitamin D deficiency in six distinct regions of Kazakhstan. Inadequate vitamin D levels are associated with weakened immune defences against diseases and increased susceptibility.13 Supplementation with Vitamin D has been shown to reduce the likelihood of respiratory infections, particularly during the winter season when influenza is more prevalent.14,15 Furthermore, research has indicated that maintaining optimal vitamin D reduces the risk of viral infections, such as human immunodeficiency virus (HIV), hepatitis B, and C.16
Since the beginning of COVID-19, there has been a significant increase in studies focused on analysing the impact of vitamin D. This disease is a contagious respiratory illness with a robust inflammatory response.16,17 A thorough investigation involving 25 randomized controlled trials (RCTs) determined that regular vitamin D supplementation generally offers protection against lower respiratory tract infections. Insufficient vitamin D levels have also been identified as a risk factor for pneumonia and Acute respiratory distress syndrome (ARDS).18,19 Several studies have explored the relationship between vitamin D levels and the occurrence of coronavirus infections. Some researchers have observed a higher likelihood of COVID-19 in individuals with low vitamin D levels,20-26 whereas others have reported no noticeable impact of vitamin D on COVID-19 susceptibility.24,25 Notably, there is an apparent correlation among populations from Asian countries, but no similar pattern has been observed in European countries.24 Another study also reported comparable findings in which participants were categorized into three groups based on the duration of infection. The acute infection group displayed low vitamin D levels followed by slightly high levels in recovered individuals. In contrast, the highest levels were observed in uninfected patients.25
The VDR gene harbors over 470 single nucleotide polymorphisms (SNPs), although only a small subset of these SNPs affects vitamin D absorption. Among them, four significant variants within the VDR gene were found to enhance the stability, activity, and expression of VDR mRNA.27 Numerous studies have explored the possible influence of genetic variations in the VDR gene on the severity of and susceptibility to COVID-19. However, it is crucial to acknowledge that existing studies in this field are limited, and their findings are inconsistent.28-31 The impact of genetic factors, particularly SNPs of the VDR gene, such as rs1544410, and rs2228570, on vitamin D levels has been explored in several studies like.31-34 It is important to highlight that various studies have presented contradictory findings, for example, two studies from India and one from Greece found no significant correlation between genetic variations in rs2228570 and 25(OH)D levels.34,35 Investigations carried out in China and Russia established an association between decreased levels of 25(OH)D and the FF genotype of rs2228570.36,37 These contrasting results highlight the complexity and variability in how genetic factors, particularly SNPs of the VDR gene like rs1544410 and rs2228570, influence vitamin D levels and potentially modulate immune responses. Given this background, the aim of our study is to investigate the association between vitamin D levels, VDR rs1544410 BsmI, and rs2228570 FokI polymorphisms with the severity and susceptibility of COVID-19.
This study was conducted at the Faculty of Medicine, Tanta University Hospital, from August 2021 to February 2022. The research protocol was approved by the medical ethics committees of the Faculty of Medicine, Tanta University, Egypt (approval number 34830/8/21). The research study adhered to the guidelines of the Declaration of Helsinki, and written informed consent was obtained from all study participants. The study included 107 patients aged ≥25 years who had COVID-19 treated at Tanta University hospitals. To confirm the presence of SARS-CoV-2 infection, all participants underwent laboratory testing using a Cobas® 6800 autoanalyzer (Roche Cobas, Germany) on samples taken from the back of their nose and throat (nasopharyngeal swabs). Around 5-10 mL of blood were dripped from all participants for the serological and molecular experiments. In addition, a control group of 107 patients who were treated in the same institutions during the proposed research period and met the same criteria but tested negative for COVID-19 was included in the study.
Exclusion criteria
Participants with certain medical conditions, such as immunodeficiency, malnutrition, obesity, inherited heart disease, autoimmune and metabolic disorders, malignancy, or any chronic illness, were considered ineligible for inclusion in the study. Additionally, individuals who had received vitamin D, calcium, multivitamins, or supplementation during the last six months of the study were also not included.
Clinical assessments
Full clinical history and laboratory and chest computed tomography (CT) were performed for every participant in this study. Laboratory assessments (ferritin), cardiac biomarkers (D-dimer and lactate dehydrogenase (LDH)), blood urea nitrogen, and liver enzymes (aspartate aminotransferase (AST) and alanine aminotransferase (ALT), were performed for every participant using a Beckman CX4 clinical biochemistry auto analyser. In addition, complete blood count (CBC), inflammatory biomarkers(C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), serum procalcitonin).
Estimation of serum [25(OH)] D levels
The ELISA Kit (K2110 Immunodiagnostic [Dutch Company], Holland) was used to quantify the level of serum 25(OH) D, according to the manufacturer’s instructions. Vitamin D status was classified into different categories using the following thresholds: serum 25(OH) D levels >30 ng/mL were categorized as sufficient, 21-30 ng/mL indicated insufficient levels, levels less than 20 ng/mL were classified as low, and levels less than 12 ng/mL were considered extremely deficient.38
Genotyping for VDR Fok1 polymorphism
From the whole dropped blood sample, 200 microliters were subjected to whole DNA genomic extraction using the QIAamp Blood Mini Kit (Qiagen). The extracted DNA was stored at -20°C for future genotyping analysis. Genotyping for the VDR Fok1 (rs2228570, 27823 C/T) polymorphism was performed using Real-Time PCR (RT-PCR) in combination with TaqMan® Universal PCR Master Mix (Applied Biosystems). The analysis focused on the rs2228570/Fok1 (C/T) single nucleotide polymorphism (SNP) within exon 2. To explore this SNP, allelic discrimination RT-PCR was employed using TaqMan® probes supplied by Applied Biosystems. The analysis entailed the use of specific primers, including a short primer (5-2 CGCACAGACAGGCCTGCA-32), long primer (5-2 TGCCGCCTGCCTGCGCAGACAGGCCTGCG-32), and constant primer (5-2 GCCCAGTTCAC GCAAGAG-32).32
Genotyping for VDR BsmI (rs1544410), polymorphism
Genotype rs1544410 was extracted using standard genotyping techniques. Blood samples were collected from the study participants, and DNA was isolated from these samples using established laboratory protocols. The genotyping assay used in this study involved a PCR-based method. Allele-specific PCR was used to determine the genotype of the rs1544410 locus. This technique uses primers specific to each allele variant, allowing amplification of the target DNA region. The PCR products were then analyzed by gel electrophoresis to visualize the presence or absence of specific DNA fragments corresponding to each allele variant. The resulting data were carefully examined, and the genotype of VDR BsmI rs1544410 was determined for each study participant based on the observed DNA fragment patterns.
CT severity score
The term “CT severity score” typically refers to a scoring system used in medical imaging, specifically in the context of computed tomography (CT) scans. CT severity scores are often used to assess the extent and severity of certain medical conditions, particularly those affecting organs or structures that can be visualized through CT imaging. One common example is the CT severity score used in assessing lung involvement in patients with conditions like COVID-19 or other respiratory diseases. In the case of COVID-19, for instance, a CT severity score may be used to quantify the extent of lung damage or involvement based on the findings in the CT images.
Each lung is anatomically divided into three zones delineated by the carina and lower pulmonary veins. These zones were further categorized into four groups based on the percentage of lung involvement: less than 25%, 25-49%, 50-74%, and greater than 75%. The total score for the combined zones was 24.
Score 1
This is classified as non-severe unless the oxygen saturation falls below 93. In other words, if a patient has a CT severity score of 1, it’s generally considered non-severe unless their oxygen saturation levels drop below 93%, at which point it may be reclassified as severe.
Score 2
Similar to score 1, score 2 is typically classified as non-severe unless the oxygen saturation falls below 93%.
Score 3
This is automatically classified as severe, regardless of the oxygen saturation levels. Even if the oxygen saturation is above 93%, a CT severity score of 3 is considered severe.
Score 4
Similar to score 3, a CT severity score of 4 is automatically considered severe, irrespective of the oxygen saturation levels.
In terms of Oxygen Saturation (O2), there are two classifications:
- Oxygen Saturation (O2) ≤93%:
If the oxygen saturation is less than or equal to 93%, regardless of the CT severity score, the case is classified as severe. This means that even if the CT score is as low as 1 or 2, with an oxygen saturation of 93% or lower, it is still considered a severe case.
- Oxygen Saturation (O2) >93%:
If the oxygen saturation is above 93%, the classification as severe or non-severe depends on the CT severity score.
If the CT score is 1 or 2, and oxygen saturation is above 93%, it is classified as non-severe.
However, if the CT score is 3 or 4, it is classified as severe, even if the oxygen saturation is above 93%. In this case, the severity is determined more by the CT findings than the oxygen saturation level.
Statistical analysis
Statistical analyses were performed using SPSS software version 27.0, and data visualization was performed using JASP. Descriptive statistics, such as means with standard deviations, were used to analyse continuous variables. Categorical variables were presented as frequencies with percentages. The Mann-Whitney U test was used to compare continuous variables between the two groups. Multiple comparisons were performed using the KS test. A rank correlation was used to investigate the association between continuous data and their significance. Differences in genotypes and allele frequencies between different groups and control subjects were presented as odds ratios (OR) computed by binary logistic regression, along with their respective 95% confidence intervals (CI) and p-values. The results were declared significant if the calculated p-value was less than the predetermined significance threshold level of 0.05, indicating that the observed outcomes were unlikely to be attributed to chance.
This study involved 107 individuals confirmed to have COVID-19, and another 107 individuals were chosen as a comparison group with no COVID-19. The mean age of COVID-19 participants was 48.84 ± 12.18 years, and that of the non-COVID-19 group was 46.82 ± 9.903 years. The mean BMI of COVID-19 participants was 29.71 ± 4.81, whereas the non-COVID-19 group had a mean BMI of 29.62 ± 4.62. Regarding sex distribution, 40.2% (n = 86) of the patients were female, and 59.8% (n = 128) were male. The mean age of male participants was 48.02 ± 11.47 years, while the female participants had a mean age of 47.55 ± 10.62 years with no significant difference (p = 0.759). Among all the patients, 82.7% (n = 177) had no history of COVID-19 infection. The demographic and clinical variables for both groups are presented in Table 1.
Table (1):
Demographic and clinical attributes of COVID-19 and non-COVID-19 groups
Variables of the Study |
COVID-19 (N = 107) |
Non-COVID (N = 107) |
p-value |
|---|---|---|---|
Age (years) (Mean ± SD) |
48.84 ± 12.18 |
46.82 ± 9.90 |
0.022* |
BMI (Mean ± SD) |
29.71 ± 4.81 |
29.62 ± 4.62 |
0.926 |
HB (Mean ± SD) |
11.23 ± 1.50 |
11.37 ± 1.91 |
0.926 |
RBC (Mean ± S.D) |
3.85 ± 0.47 |
3.97 ± 0.42 |
0.097 |
WBC (Mean ± S.D) |
3.64 ± 2.36 |
7.33 ± 4.41 |
|
Hematocrit (Mean ± SD) |
34.28 ± 3.89 |
42.95 ± 8.65 |
|
Platelet Count (Mean ± S.D) |
279691.59 ± 81900.12 |
227.07 ± 57.76 |
|
Mean Corpuscular volume (Mean ± S.D) |
67.75 ± 3.21 |
67.70 ± 1.99 |
0.097 |
Mean Corpuscular Hemoglobin (Mean ± S.D) |
30.55 ± 3.29 |
31.21 ± 2.16 |
0.511 |
Mean Corpuscular haemoglobin level (Mean ± SD) |
30.94 ± 2.52 |
29.93 ± 2.41 |
|
Neutrophil (Mean ± S.D) |
68.91 ± 3.64 |
56.80 ± 6.33 |
|
Lymphocyte (Mean ± S.D) |
23.99 ± 4.21 |
36.72 ± 6.83 |
|
Monocyte (Mean ± SD) |
7.22 ± 2.69 |
6.45 ± 2.69 |
0.032* |
Ferritin (Mean ± S.D) |
230.59 ± 198.27 |
112.35 ± 34.45 |
|
D Dimer (Mean ± S.D) |
1.24 ± 0.54 |
0.30 ± 0.21 |
|
Procalcitonin (Mean ± S.D) |
1.98 ± 2.29 |
0.35 ± 1.04 |
|
C-reactive protein (Mean ± S.D) |
15.82 ± 13.73 |
5.15 ± 3.27 |
|
Glutamicpyruvictransaminase (Mean ± S.D) |
30.49 ± 6.32 |
23.35 ± 6.53 |
|
Glutamicoxaloacetictransaminase (Mean ± S.D) |
33.14 ± 8.82 |
23.25 ± 4.55 |
|
Lactatede hydrogenase (Mean ± SD) |
191.03 ± 25.36 |
183.01 ± 32.42 |
0.319 |
Urea (Mean ± SD) |
34.77 ± 10.44 |
29.23 ± 8.39 |
|
Vitamin D (Mean ± S.D) |
35.25 ± 9.40 |
38.85 ± 9.40 |
0.004* |
Smoking Yes No |
23 (21.5%) 84 (78.5%) |
27 (25.2%) 80 (74.8) |
0.518 |
Smell and Taste Yes No |
91 (85%) 16 (15%) |
197 (100) – |
|
History of Asthma Yes No |
27 (25.2%) 80 (74.8%) |
– 107 (100%) |
|
Neurological Yes No |
8 (7.5%) 99 (92.5%) |
1 (0.9%) 106 (99.1%) |
0.017* |
COVID-19 previous infection Yes No |
37 (34.6%) 70 (65.4%) |
– 107 (100%) |
|
Severity Severe Non-severe |
41 (19.2%) 66 (30.8%) |
2 (0.9%) 105 (49.1%) |
|
Mortality Yes No |
2 (0.9%) 105 (49.1%) |
– 107 (50%) |
0.155 |
*Statistically significant.
Regarding BMI, the COVID-19 group had a slightly higher mean (29.71 ± 4.81) than the non-COVID-19 group, with no significant difference (p = 0.962). The analysis of haematological parameters showed that differences in mean hemoglobin (Hb) were not significantly different (p = 0.926) and red blood cell (RBC) count between the COVID-19 and non-COVID-19 groups (p = 0.097). However, the WBC count was significantly lower (p < 0.001) in the COVID-19 group (3.85 ± 0.47 ng/mL) than in the comparison to the non-COVID-19 group (7.33 ± 4.41 ng/mL). Similarly, the mean hematocrit (HMC) was significantly lower in the COVID-19 group (34.28 ± 3.89 ng/mL) than in the non-COVID participants (42.95 ± 8.65 ng/mL) (p < 0.001). In terms of urea levels, the COVID-19 group had a higher average (34.77 ± 10.44 ng/mL) than the non-COVID-19 group (29.23 ± 8.39 ng/mL), and the difference observed was notably significant (p < 0.001). Additionally, the average vitamin D level was significantly lower in the COVID-19 group (35.25 ± 9.40 ng/mL) than in the non-COVID-19 group (38.85 ± 9.40 ng/mL) (p = 0.004). Regarding qualitative attributes, no significant association was observed between smoking and COVID-19 (p = 0.518). However, an association was found between participants experiencing smell and taste issues and those who had COVID-19 with significance (p < 0.001), and 91 (85%) of them reported smell and taste issues.
The other group did not have a family history of asthma (p < 0.001). Of the COVID-19 participants, 37 (43.6%) reported having a previous infection, whereas 70 (65.4%) had no prior infection of COVID-19 (p < 0.001). Considering the severity of the disease measured by O2 saturation, 66 (30.8%) of participants were non-severe in the COVID-19 group, which was lower in the non-COVID-19 group (105 (49.1%)). A significant association was observed between severity and the presence of COVID-19. However, no association was noted between mortality and COVID among the participants as the study observed 105 (49.1%) non-mortality in the COVID-19 group and 107(50%) non-mortality cases in the non-COVID-19 group ( p = 0.155).
Vitamin D 25(OH)D level
Vitamin D 25(OH)D levels were evaluated in the COVID-19 and non-COVID-19 groups. Among participants with COVID-19, the mean level was 35.25 ± 9.40 ng/mL, and in the non-COVID-19 group, it was 38.85 ± 9.40 ng/mL with a significant difference (p = 0.004). Figure 1 shows a graphical representation of the serum 25(OH)D level distribution in both groups.
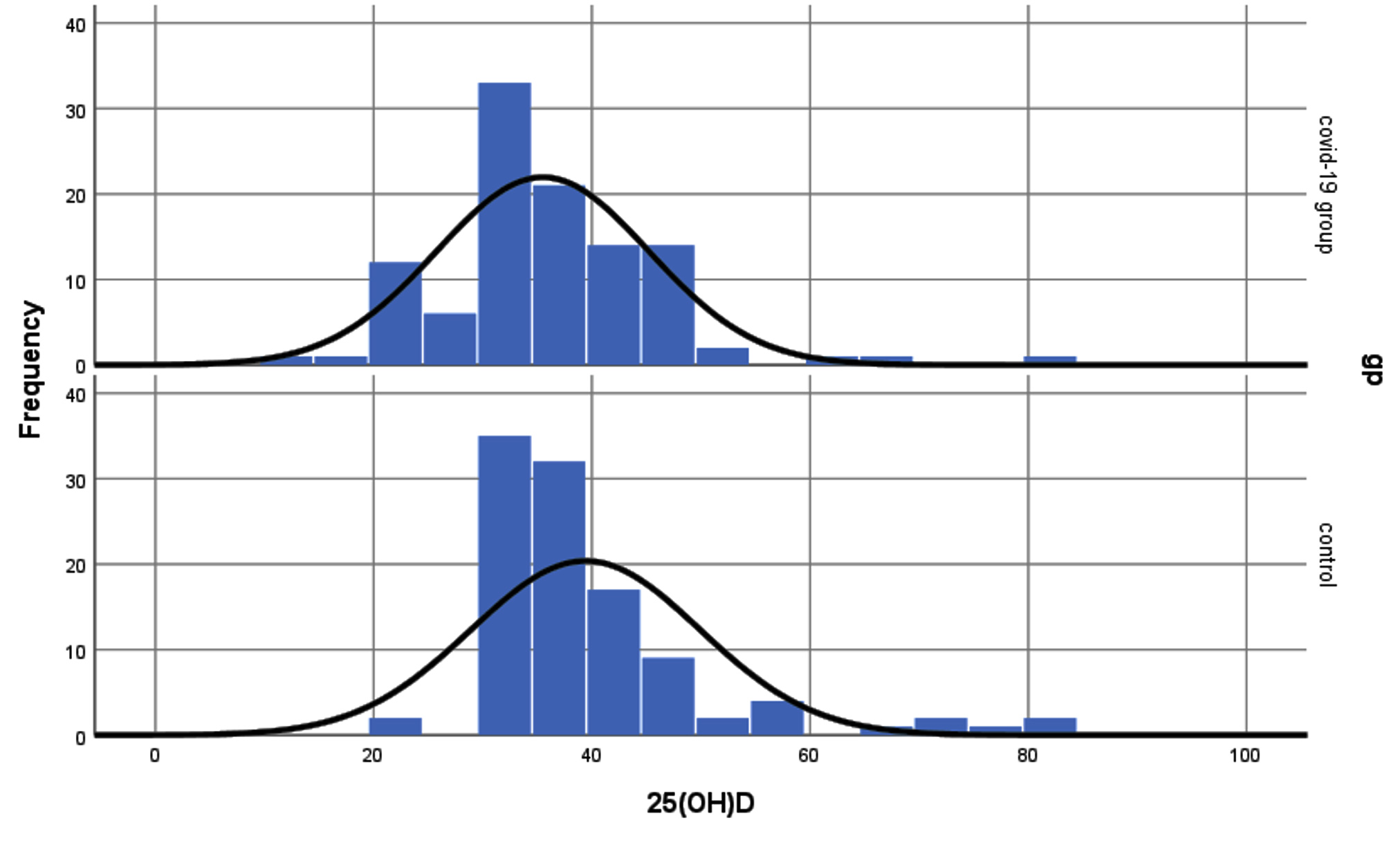
Figure 1. Serum 25-hydroxyvitamin D (25(OH)D) level among COVID-19 and Non-COVID-19 groups
Both groups exhibited a deficiency in 25(OH)D levels; however, this was more evident in COVID-19 than in uninfected participants. Among COVID-19 cases, 87 (81.3%) individuals had sufficient vitamin D levels; 105 (98.1%) individuals in the uninfected group had adequate levels greater than the previous group. Notably, 15 (14%) individuals in the COVID-19 group displayed insufficient vitamin D levels, higher than the unaffected group, where only 2 (1.9%) individuals had inadequate levels. Furthermore, 5 (4.7%) patients in the COVID-19 group exhibited vitamin D deficiency, while no such deficiency was observed in the unaffected group.
The association between the group (COVID-19 vs. non-COVID) and Vitamin D level was statistically significant (c2 = 16.629, p < 0.001), indicating a strong relationship between the occurrence of COVID and vitamin D level. On the other hand, when examining the association between Vitamin D levels and sex, no association was observed (c2 = 3.913, p = 0.141). Furthermore, the mean vitamin D level among females (36.81 ± 9.589 ng/mL) was nearly identical to that of males (37.89 ± 10.716 ng/mL). Figure 2 shows the distribution of Vitamin D level with respect to COVID and non-COVID groups.
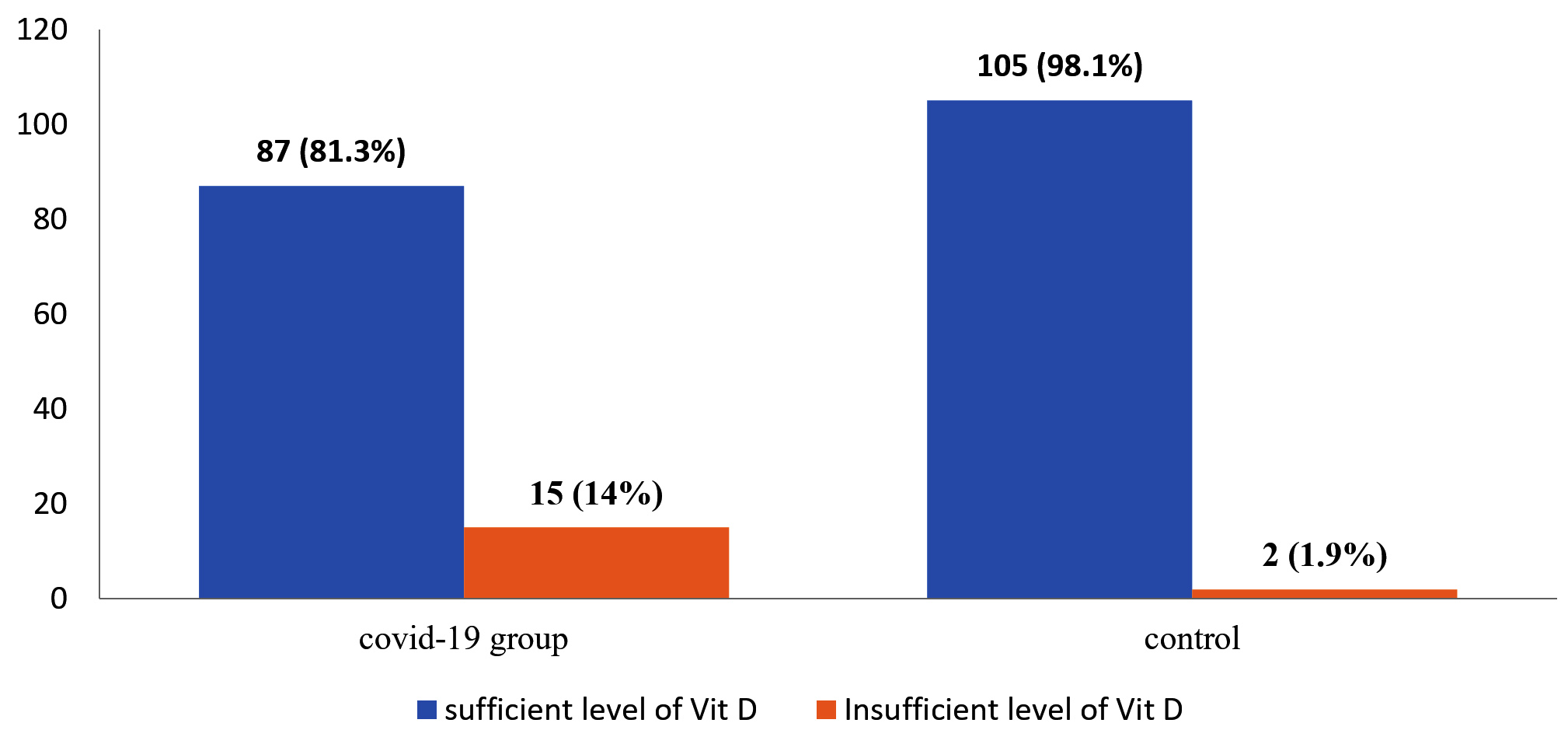
Figure 2. Percentage Distribution of Vitamin D levels among COVID and non-COVID
Participants were categorized into two age groups based on the median age (45 years) as the threshold point for comparison purposes. Participants above 45 were classified as “old,” while those below the median age were considered “younger.” A vitamin D level mean among younger participants was 37.75 ± 10.543 ng/mL, while older participants had a vitamin D level mean of 37.16 ± 10.02 ng/mL with an insignificant difference (KS = 0.419, p = 0.676). The BMI of COVID-19 participants was slightly higher (29.71 ± 4.81 Kg/m2) than that of the uninfected group (29.62 ± 4.62 Kg/m2), suggesting that the participants’ diets provided sufficient nutrient intake. Moreover, no correlation was noted between BMI and Vitamin D levels (r = 0.091, p = 0.186). Hemoglobin (Hb) and red blood cell count (RBC) showed weak positive correlations with Vitamin D levels (r = 0.139, p = 0.042) and (r = 0.138, p = 0.044, respectively). However, the white blood cell count (WBC) was also not observed correlated with Vitamin D levels (r = 0.075, p = 0.275) (Figure 3).
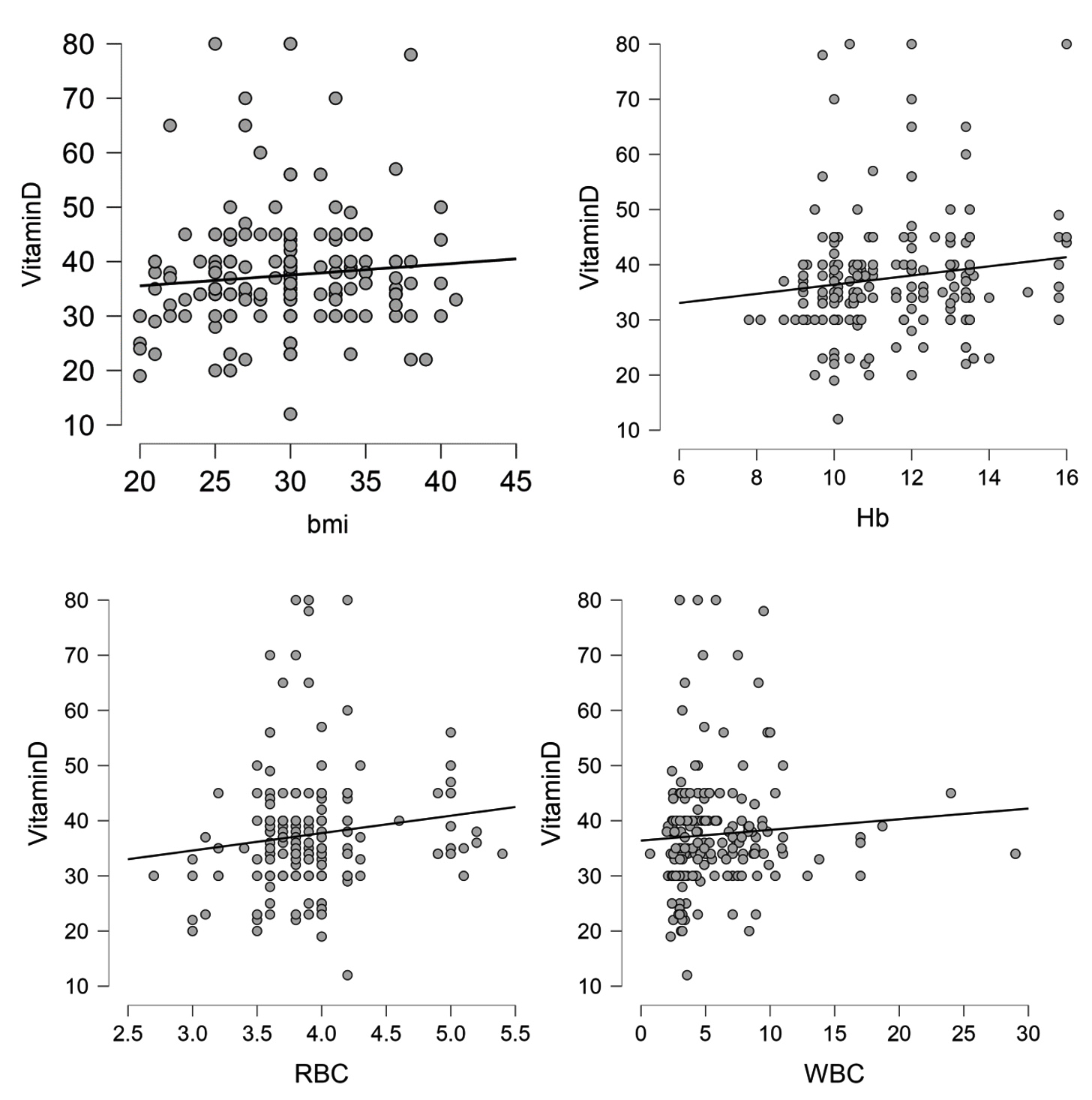
Figure 3. Correlation between Vitamin D and Clinical Variables
Interestingly, our study revealed a significant difference (KS = 2.208, p = 0.028) in the mean 25(OH) D level between smokers (40.24 ± 10.856ng/mL) and non-smokers (36.61 ± 9.963 ng/mL). Considering the mortality and severity of the body’s vitamin D level, the study noted a negative correlation between vitamin D level and disease severity (r = -0.131, p = 0.031) but no correlation was observed with mortality (r = 0.031, p = 0.653).
Vitamin D receptors rs1544410 BsmI and rs2228750 Fok1 polymorphism
The study observed the AA genotype in 22 individuals (12.6%) in the COVID-19 participant group and 42 individuals (19.6%) in the uninfected group. Among the COVID-19 participants, the AG genotype was observed at a frequency of 15.9%, whereas it was noted that 24.8% of the non-COVID-19 group (c2 = 19.216, OR = 5.963, 95% CI: 2.684-13.249) (Table 2). Similarly, the GG genotype was present in 21.5% of the COVID-19 participants, while only 5.6% of the uninfected participants exhibited this genotype (c2 = 20.839, OR = 5.975, 95% CI: 2.774-12.874) (Table 2). The findings highlight a notable difference in AG and GG genotypes between COVID-19 uninfected participants (p < 0.001). In this specific population, the AG and GG genotypes were associated with an increased likelihood of COVID-19 occurrence (OR = 5.963, c2 = 19.216) and (OR = 5.975, c2 = 20.839, respectively).
Table (2):
VDR rs1544410 Bsml and Fok1 genotypes associated with the susceptibility of COVID-19 and Non-COVID-19 patients
| VDR rs15444410 BsmI genotypes and alleles polymorphisms | COVID-19 (n=107) |
Non-COVID (n = 107) |
OR(C.I) | Test-statistic | p-value |
|---|---|---|---|---|---|
| AA | 27 (12.6%) | 42 (19.6%) | 0.334 (0.022-0.245) | 8.445 | Reference category (1) |
| AG | 34 (15.9%) | 53 (24.8%) | 5.963 (2.684-13.249) | 19.216 | <0.001* |
| GG | 46 (21.5%) | 12 (5.6%) | 5.975 (2.774-12.874) | 20.839 | <0.001* |
| ALLELES | |||||
| A | 88 (20.6%) | 137 (32%) | 0.393 (0.266-0.580) | 22.49 | <0.001* |
| G | 126 (29.4%) | 77 (18%) | 2.584 (1.725-3.762) | 22.090 | 0.001* |
| CC | 48 (22.5%) | 6(2.8%) | – | – | Reference category (1) |
| TC | 31 (14.6%) | 57 (26.8%) | 0.077 (0.029-0.203) | 26.66 | 0.027* |
| TT | 27 (12.7%) | 44 (20.7%) | 1.128 (0.590-2.159) | 0.133 | 0.715 |
| ALLELES | |||||
| C | 124(29.2%) | 68 (16%) | 0.3117 (2.049-4.640) | 31.369 | <0.001* |
| T | 86 (20.2%) | 147 (34.6) | 0.321 (0.216-0.478) | 32.249 | <0.001* |
Furthermore, when considering the VDR FOK1 gene, the TC genotype significantly differed between the COVID-19 and non-COVID-19 groups (p = 0.027) (Table 2). This significant association was linked to a decreased susceptibility to COVID-19 (OR = 0.077, c2 = 26.66). The GG genotype of rs1544410 was significantly more common among COVID-19 participants (n = 46, 21.5%, OR = 5.975, 95% CI: 2.774-12.874) than among uninfected participants (n = 12, 5.6%, OR = 0.077, 95% CI: 0.029-0.203) (Table 2). Conversely, the TC genotype of VDR Fok1 was more frequent among COVID-19 participants (n = 57, 26.8%) than in the uninfected group (Table 2). The findings from the genotyping and allele analysis of VDR rs1544410 and Fok1 are presented in Table 2. All allele frequencies of A, C, G, and T were statistically associated with susceptibility to COVID-19
(p < 0.001). Frequencies of C (n = 124, 29.2%) and G (126, 29.4%) in COVID-19 participants dominated the frequencies of uninfected group (n = 68,16%) and for the G allele (n = 77;18%). The A, C, and T alleles were associated with a reduced risk of infection.
This study noted an insignificant association between Vitamin D levels and VDR BsmI rs1544410 (p = 0.429) (Table 3). The analysis indicated sufficient levels of vitamin D across all rs1544410 genotypes. Among the 214 participants, 192 individuals with different rs1544410 genotypes displayed adequate 25 (OH)D levels. No association was found between rs1544410 and 25(OH)D levels. However, it is worth noting that a weak significant association was observed between 25 (OH)D levels and genotypes of the rs2228570 VDR Fok1 polymorphism (p = 0.049) (Table 3). It can also be observed from the study that GG genotype 38 (35.3%) of rs1544410 has sufficient level of vitamin D among COVID patients
(Table 4) while the non-severity of disease was more i.e. 54 (50.5%) among the COVID patients who had sufficient level of Vitamin D (Table 5).
Table (3):
The association between 25(OH)D level with VDR rs1544410 Bsml and rs2228570 Fok1 genotypes
| Vitamin D level | Statistic test | p-value | ||||
|---|---|---|---|---|---|---|
| sufficient | insufficient levels | low | ||||
| VDR rs1544410 BsmI polymorphism | AA | 64 (29.9%) | 5 (2.3%) | 0 (0%) | 3.837 | 0.429 |
| AG | 78 (36.4%) | 7 (3.3%) | 2 (0.9%) | |||
| GG | 50 (26.0%) | 5 (2.3%) | 3 (1.4%) | |||
| VDR rs2228570 Fok1 polymorphism | CC | 44 (23.4%) | 6 (2.8%) | 4 (1.9%) | 9.541 | 0.049* |
| TC | 81 (38%) | 6 (2.8%) | 1 (0.5%) | |||
| TT | 66 (31%) | 5 (2.3%) | 0 (0%) | |||
* Statistically significant
Table (4):
The association between 25(OH)D level with VDR rs1544410 Bsml of COVID-19 patients
| Vitamin D level among COVID-19 Patients | VDR rs1544410 BsmI polymorphism | P-value | |||
|---|---|---|---|---|---|
| AA | AG | GG | |||
| Vitamin D level | Sufficient | 23 (21.5%) | 26 (24.3%) | 38 (35.5%) | 2.519 (0.641) |
| Insufficient levels | 4 (3.7%) | 6 (5.6%) | 5 (4.7%) | ||
| Low | 0 (0.0%) | 2 (1.9%) | 3 (2.8%) | ||
Table (5):
The association between 25(OH)D level with VDR rs1544410 Bsml of COVID-19 patients
| Vitamin D level and Severity of disease among COVID-19 Patients | Severity | P-value | ||
|---|---|---|---|---|
| Severe | Non-severe | |||
| Vitamin D level | Sufficient | 33 (30.8%) | 54 (50.5%) | 0.029 (0.985) |
| Insufficient levels | 6 (5.6%) | 9 (8.4%) | ||
| Low | 2 (1.9%) | 3 (2.8%) | ||
When considering severity as measured by O2 saturation, it was observed that the frequencies of non-severity in each genotype and allele predominated over the frequencies in the severe group. The study suggested the association between VDR rs1544410 BsmI genotypes and allele polymorphisms with the severity of COVID-19. Among the genotypes, the AA genotype was found in 4.7% of severe cases and 27.6% of non-severe cases, with an odds ratio (OR) of 3.112 (95% CI: 1.342-6.650, p = 0.006). The AG genotype was present in 6.1% of severe cases and 34.6% of non-severe cases, showing an OR of 3.105 (95% CI: 1.322-7.350, p = 0.010). The GG genotype appeared in 9.3% of severe cases and 17.8% of non-severe cases, with an OR of 2.996 (95% CI: 1.346-6.670, p = 0.007). For allele frequencies, the A allele was found in 14% of severe cases and 27.1% of non-severe cases, yielding an OR of 1.503 (95% CI: 0.779-2.227, p = 0.001). The G allele was observed in 6.1% of severe cases and 52.8% of non-severe cases, with an OR of 1.188 (95% CI: 0.488-1.889, p < 0.001) (Table 6). The presence of alleles C and T was observed associated with a reduced risk of severity [c2 = 16.572, OR=0.222, 95% CI: 0.108-0.459, p < 0.001] and [c2 = 11.050, OR = 0.305, 95% CI: 0.151-0.641) (Table 6), respectively. Moreover, individuals with the CC genotype were significantly associated with a reduced risk of experiencing severity [c2 = 7.845, OR = 0.212, 95% CI: 0.13-0.674, p < 0.001]
(Table 6).
Table (6):
VDR rs1544410 Bsml and Fok1 genotypes associated with severity of COVID-19 and Non-COVID-19 patients
| VDR rs1544410 BsmI genotypes and alleles polymorphisms | Severe N=43 | Non-severe N=171 | OR (C.I) | Test-statistic | p-value |
|---|---|---|---|---|---|
| AA | 10 (4.7%) | 59 (27.6%) | 3.112 (1.342-6.650) | 7.665 | 0.006* |
| AG | 13 (6.1%) | 74 (34.6%) | 3.105 (1.322-7.350) | 6.643 | 0.010* |
| GG | 20 (9.3%) | 38 (17.8%) | 2.996(1.346-6.670) | 7.220 | 0.007* |
| ALLELES | |||||
| A | 30 (14%) | 58 (27.1%) | 1.503 (0.779-2.227) | 18.238 | 0.001* |
| G | 13 (6.1%) | 113 (52.8%) | 1.188 (0.488-1.889) | 11.743 | <0.001* |
| CC | 22 (10.3%) | 32 (15%) | 0.212 (0.130-0.674) | 7.845 | 0.001* |
| TC | 11 (5.2%) | 77 (36.2%) | 0.238 (0.10-0.564) | 10.643 | <0.001* |
| TT | 10 (4.7%) | 61 (28.6%) | 1.148 (0.457-2.879) | 0.086 | 0.796 |
| ALLELES | |||||
| C | 15 (7%) | 109 (50.9%) | 0.222 (0.108-0.459) | 16.572 | <0.001* |
| T | 28 (13.1%) | 62 (29%) | 0.305 (0.151-0.641) | 11.050 | 0.001* |
*Statistically significant.
1st category of each genotype=Reference Category
These findings indicate a potential association between specific genotypes and susceptibility to severe COVID-19. The AG and GG genotypes of VDR rs1544410 BsmI may contribute to an increased likelihood of COVID-19 occurrence, whereas the TC genotype of VDR rs2228750 Fok1 were found associated with a decreased susceptibility to the disease. However, owing to the limited number of mortality cases (n = 2), it may be challenging to generalize the data regarding mortality outcomes.
The nature of vitamin D involves a wide range of functions, spanning from its participation in immune responses to anti-inflammatory properties and antimicrobial capabilities,13,16,39 As such, our objective was to explore the potential influence of vitamin D on susceptibility to COVID-19, achieved through an examination of the serum level of 25-hydroxyvitamin D (25(OH)D) in individuals who tested positive or negative for the virus. Our investigation revealed a noteworthy reduction in vitamin D levels in the COVID-19 group compared with the uninfected/control group. These observations align with earlier research conducted by other researchers.13,21,40-43 Gallelli et al. also reported comparable findings in their study, where participants were categorized into three groups based on the duration of infection. The acute infection group displayed low vitamin D levels (9.63 ± 8.70 ng/mL), followed by slightly high levels in recovered individuals (11.52 ± 4.90 ng/mL). In contrast, the highest levels were observed in uninfected patients (15.96 ± 5.99 ng/mL).25 In further validating the relationship between low vitamin D levels and increased susceptibility to COVID-19, a meta-analysis conducted by Mukherjee et al. attributed this association predominantly to seasonal UV exposure.44
Sex has been investigated in various studies exploring its influence on vitamin D levels.45 However, our study yielded different results, as an insignificant relationship was found between sex and with the mean 25(OH)D level among females being nearly equivalent to that among males.46-49 Zhumina et al. performed a study in the Kazakhstan region, analyzing vitamin D levels among healthy volunteers and reported similar findings when comparing individuals based on gender.46 The study found a significant negative correlation with vitamin D levels. These findings are consistent with those of a previous study.41
Additionally, the impact of genetic factors, particularly SNPs of the VDR gene, such as rs1544410, and rs2228570, on vitamin D levels has been explored in several studies.31-34 Our investigation examined the association between vitamin D levels of rs1544410 and FOK1 genotypes and their respective alleles. However, the study observed no association between vitamin D levels and rs1544410 but a slight association with Fok1 genotypes. It is worth noting that different studies have reported conflicting results. For instance, research conducted in China and Russia demonstrated a relationship between reduced levels of 25(OH)D and the ff genotype rs2228570 (FokI T > C) of rs2228570.36,37 Conversely, two studies from India reported no significant correlation between genetic variations in rs2228570 and 25(OH)D levels.35,47 In the study conducted by Al Anouti et al., various specific genotypes within these genes were identified as being associated with severe cases of COVID-19. Notably, the AA genotype in the SNP rs59241277, the CC genotype in the SNP rs113574864, the GG genotype in the SNP rs182901986, the TT genotype in the SNP rs60349934, and the GG genotype in the SNP rs113876500 within the GC gene were all found to be linked to a higher risk of experiencing critical COVID-19.48
Laplana et al. conducted a comprehensive meta-analysis that revealed a noteworthy association between rs2228570 and COVID-19 infection. This intriguing finding has stimulated additional research to explore the possible correlation between this particular SNP and its influence on susceptibility to COVID-19. In particular, allele T and TT genotypes were identified as risk factors for respiratory syncytial virus (RSV) infection.50 Our study observed significant allele frequencies for A, C, G, and T associated with COVID-19 susceptibility. Alleles C and T of the rs228570 FOK1 genotype significantly reduced the likelihood of COVID-19, However, alleles A and T were observed more frequently in the non-infected group than in the COVID-19 group, whereas C and G were observed less frequently in the COVID-19 group. Notably, only the VDR BsmaI rs2228750 genotype TT was found to be insignificant concerning COVID susceptibility but showed an increased likelihood.
In conclusion, our case-control study investigated the relationship between vitamin D status, genetic polymorphisms, and COVID-19 susceptibility has yielded valuable insights. There was a notable difference in the levels of vitamin D between individuals with COVID-19 and those without the infection, with COVID-19 patients exhibiting lower levels of vitamin D which indicates correlation between vitamin D status and the susceptibility of COVID-19. The study found no significant association between Vitamin D levels and VDR rs1544410 Bsml Polymorphism while slight significant correlation was observed with VDR rs2228750 Fok1 polymorphism. However, it is imperative to perform additional studies and research involving larger sample sizes to obtain a more comprehensive understanding of the association between different genotypes and COVID-19 within this region.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Medical Ethics Committee of the Faculty of Medicine, Tanta University (approval number 34830/8/21).
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Fong SJ, Dey N, Chaki J. An introduction to COVID-19. Artificial intelligence for coronavirus outbreak. 2021:1-22.
Crossref - Haileamlak A. The impact of COVID-19 on health and health systems. Ethiopian Journal of Health Sciences. 2021;31(6):1073.
Crossref - Sethi BA, Sethi A, Ali S, Aamir HS. Impact of Coronavirus disease (COVID-19) pandemic on health professionals. Pak J Med Sci. 2020;36(COVID19-S4):S6.
Crossref - Poudel AN, Zhu S, Cooper N, et al. Impact of Covid-19 on health-related quality of life of patients: A structured review. Plos one. 2021;16(10):e0259164.
Crossref - Khetrapal S, Bhatia R. Impact of COVID-19 pandemic on health system & Sustainable Development Goal 3. Indian J Med Res. 2020;151(5):395-399.
Crossref - Sabetkish N, Rahmani A. The overall impact of COVID-19 on healthcare during the pandemic: A multidisciplinary point of view. Health Sci Rep. 2021;4(4):e386.
Crossref - Long E, Patterson S, Maxwell K, et al. COVID-19 pandemic and its impact on social relationships and health. J Epidemiol Community Health. 2022;76(2):128-132.
Crossref - Haleem A, Javaid M, Vaishya R. Effects of COVID-19 pandemic in daily life. Curr Med Res Pract. 2020;10(2):78-79.
Crossref - Lei S, Jiang F, Su W, et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. E Clinical Medicine. 2020;21.
Crossref - Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2- 2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271-280.
Crossref - Pike JW, Meyer MB. The vitamin D receptor: new paradigms for the regulation of gene expression by 1, 25-dihydroxyvitamin D3. Rheum Dis Clin North Am. 2012;38(1):13-27.
Crossref - Gromova O, Doschanova A, Lokshin V, et al. Vitamin D Deficiency in Kazakhstan: Cross-Sectional Study. J Steroid Biochem Mol Biol. 2020;199:105565.
Crossref - Jayawardena R, Jeyakumar DT, Francis TV, Misra A. Impact of the Vitamin D Deficiency on COVID-19 Infection and Mortality in Asian Countries. Diabetes Metab Syndr Clin Res Rev. 2021;15(3):757-764.
Crossref - Bergman P, Lindh AU, Bjorkhem-Bergman L, Lindh JD. Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE. 2013;8(6):e65835.
Crossref - Urashima M, Segawa T, Okazaki M, Kurihara M, Wada Y, Ida H. Randomised Trial of VitaminD Supplementation to Prevent Seasonal Influenza A in Schoolchildren. Am J Clin Nutr. 2010;91(5):1255-1260.
Crossref - Nimavat N, Singh S, Singh P, Singh SK, Sinha N. Vitamin D Deficiency and COVID-19: A Case-Control Study at a Tertiary Care Hospital in India. Ann Med Surg. 2021;68:102661.
Crossref - Ali N. Role of Vitamin D in Preventing of COVID-19 Infection, Progression and Severity. J Infect Public Health. 2020;13(10):1373-1380.
Crossref - Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. bmj. 2017;356:i6583.
Crossref - Dancer RC, Parekh D, Lax S, et al. Vitamin D deficiency contributes directly to the acute respiratory distress syndrome (ARDS). Thorax. 2015;70(7):617-624.
Crossref - Merzon E, Tworowski D, Gorohovski A, et al. Low Plasma 25(OH) Vitamin D Level Is Associated with Increased Risk of COVID-19 Infection: An Israeli Population-based Study. FEBS J. 2020;287(17):3693-3702.
Crossref - Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 Positivity Rates Associated with Circulating 25-Hydroxyvitamin D Levels. PLoS ONE. 2020;15(9):e0239252.
Crossref - Singh S, Kaur R, Singh RK. Revisiting the role of vitamin D levels in the prevention of COVID-19 infection and mortality in European countries post infections peak. Aging Clin Exp Res. 2020;32(8):1609-12.
Crossref - Padhi S, Suvankar S, Panda VK, Pati A, Panda AK. Lower levels of vitamin D are associated with SARS-CoV-2 infection and mortality in the Indian population: An observational study. Int Immunopharmacol. 2020;88:107001.
Crossref - Bakaloudi DR, Chourdakis M. A Critical Update on the Role of Mild and Serious Vitamin D Deficiency Prevalence and the COVID-19 Epidemic in Europe. Nutrition. 2022;93:111441.
Crossref - Gallelli L, Mannino GC, Luciani F, et al. Vitamin D Serum Levels in Subjects Tested for SARS CoV-2: What Are the Differences among Acute, Healed, and Negative COVID-19 Patients? A Multicenter Real-Practice Study. Nutrients. 2021;13(11):3932.
Crossref - Hastie CE, Mackay DF, Ho F, et al. Vitamin D concentrations and COVID-19 infection in UK Biobank. Diabetes Metab Syndr. 2020;14(4):561-565.
Crossref - Wang Q, Xi B, Reilly KH, Liu M, Fu M. Quantitative assessment of the associations between four polymorphisms (Fok I, Apa I, Bsm I, Taq I) of vitamin D receptor gene and risk of diabetes mellitus. Mol Biol Rep. 2012;39(10):9405-9414.
Crossref - Abdollahzadeh R, Shushizadeh MH, Barazandehrokh M, et al. Association of Vitamin D receptor gene polymorphisms and clinical/severe outcomes of COVID-19 patients. Infect Genet Evol. 2021;96:105098.
Crossref - Jafarpoor A, Jazayeri SM, Bokharaei-Salim F, et al. VDR gene polymorphisms are associated with the increased susceptibility to COVID-19 among iranian population: A case control study. Int J Immunogenet. 2022;49(4):243-253.
Crossref - Kotur N, Skakic A, Klaassen K, et al. Association of vitamin D, zinc and selenium related genetic variants with COVID-19 disease severity. Front Nutr. 2021;8:689419.
Crossref - Apaydin T, Polat H, Yazan CD, et al. Effects of vitamin D receptor gene polymorphisms on the prognosis of COVID-19. Clin Endocrinol. 2022;96(6):819-830.
Crossref - Fiaz H, Khan AR, Abbas S, et al. Association of vitamin D receptor polymorphisms with cardiometabolic conditions in Pakistani population. Int J Vitam Nutr Res. 2024;94(1):45-53.
Crossref - Ju F, Zhu R. Association of vitamin D levels and VDR variant (rs2228570) with allergic rhinitis: A meta-analysis and trial sequential analysis. Heliyon. 2023;9(6):e17283.
Crossref - Divanoglou N, Komninou D, Stea EA, et al. Association of vitamin D receptor gene polymorphisms with serum vitamin D levels in a Greek rural population (Velestino Study). Lifestyle Genom. 2021;14(3):81-90.
Crossref - Bhanushali AA, Lajpal NA, Kulkarni SS, Chavan SS, Baghadi SS, Das BR. Frequency of FokI and TaqI Polymorphism of Vitamin D Receptor Gene in Indian Population and Its Association with 25-Hydroxyvitamin D Levels. Indian J Hum Genet. 2009;15(3):108-113.
Crossref - Li K, Shi Q, Yang L, et al. The Association of Vitamin D Receptor Gene Polymorphisms and Serum 25- Hydroxyvitamin D Levels with Generalized Vitiligo: Association of VDR Polymorphisms and Vitiligo Risk. Br J Dermatol. 2012;167(4):815-821.
Crossref - Baturin AK, Sorokina EY, Vrzhesinskaya OA, et al. The study of the association between rs2228570 polymorphism of VDR gene and vitamin D blood serum concentration in the inhabitants of the Russian Arctic. Vopr Pitan. 2017;86(4):77-84.
Crossref - Holick MF. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. 2017;18(2):153-65.
Crossref - Levine AJ, Harper JM, Ervin CM, Chen YH, Harmon E, Xue S, et al. Serum 25-hydroxyvitamin D, dietary calcium intake, and distal colorectal adenoma risk. Nutr Cancer. 2001;39:35–41.
Crossref - Soltani-Zangbar MS, Mahmoodpoor A, Dolati S, et al. Serum Levels of Vitamin D and Immune System Function in Patients with COVID-19 Admitted to Intensive Care Unit. Gene Rep. 2022;26:101509.
Crossref - Sooriyaarachchi P, Jeyakumar DT, King N, Jayawardena R. Impact of Vitamin D Deficiency on COVID-19. Clin Nutr ESPEN. 2021;44:372-378.
Crossref - Alpcan A, Tursun S, Kandur Y. Vitamin D levels in children with COVID-19: a report from Turkey. Epidemiol Infect. 2021;149:e180.
Crossref - Hammam NH, Aziz MRA, Soliman AMM, et al. Relation between vitamin D and COVID-19 in Egyptian patients. Egypt J Intern Med. 2024; 36(84).
Crossref - Mukherjee SB, Gorohovski A, Merzon E, Levy E, Mukherjee S, Frenkel-Morgenstern M. Seasonal UV Exposure and Vitamin D: Association with the Dynamics of COVID-19 Transmission in Europe. FEBS Open Biol. 2021;12(1):106-117.
Crossref - Wierzbicka, A, Oczkowicz, M. Sex Differences in Vitamin D Metabolism, Serum Levels and Action. Br J Nutr. 2022;128(11):2115-2130.
Crossref - Zhumina AG, Li K, Konovalova AA, et al. Plasma 25-Hydroxyvitamin D Levels and VDR Gene Expression in Peripheral Blood Mononuclear Cells of Leukemia Patients and Healthy Subjects in Central Kazakhstan. Nutrients. 2020;12(5):1229.
Crossref - Hassan I, Bhat YJ, Sabhiya M, et al. Association of Vitamin D Receptor Gene Polymorphisms and Serum 25-Hydroxy Vitamin D Levels in Vitiligo-A Case-Control Study. Indian Dermatol Online J. 2019;10(2):131-138.
Crossref - Al-Anouti F, Mousa M, Karras SN, et al. Associations between Genetic Variants in the Vitamin D Metabolism Pathway and Severity of COVID-19 among UAE Residents. Nutrients. 2021;13(11):3680.
Crossref - Abbas AH, Salloom DF, Misha’al KI, Taqi EA. Vitamin D receptor rs2228570 and rs1544410 genetic polymorphisms frequency in Iraqi thalassemia patients compared to other ethnic populations. Gene Reports. 2021;23:101131.
Crossref - Laplana M, Royo JL, Fibla J. Vitamin D Receptor Polymorphisms and Risk of Enveloped Virus Infection: A Meta-Analysis. Gene. 2018;678:384-394.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.