


ISSN: 0973-7510
E-ISSN: 2581-690X
Antimicrobial Resistance (AMR) among different microorganisms has become a serious issue and contributing to cause severe diseases. Proper monitoring measures should be taken to improve the current scenario of antimicrobial resistance. The present study focuses on identification, antimicrobial resistance profiling and virulence factors of bacterial isolates recovered from various human clinical cases. Total 350 clinical samples were collected from a public hospital in Shimla (Himachal Pradesh) and a private diagnostic centre in Mohali (Punjab). K. pneumoniae (51.42%) and E. coli (44.57%) were recovered from all the sample sources while S. aureus (3.15%) and Bacillus spp. (0.86%) were isolated from urine samples only. Overall maximum resistance was observed against ampicillin (94.28%), amoxicillin + clavulanic acid (90.5%), cefepime (88%) and ceftriaxone (80.18%) while it was minimum for cefoperazone (0.85%), kanamycin (1.14%), lomefloxacin and norfloxacin (1.42% each) and cefixime (1.71%). 52.28% isolates were multidrug-resistant (MDR) and 13.42% were extensive drug resistant (XDR). Drug resistant phenotypes were prominently observed in isolates recovered from tracheal fluid and cerebrospinal fluid (CSF). The expression of selective virulence factors like motility, lipase, protease and capsule production was evenly associated with drug-resistant and drug-sensitive bacterial phenotypes; however, siderophore and biofilm production was only seen among isolates with drug resistant phenotype. A significant relation between both the variables was statistically confirmed using chi-square test and the probability value (p < 0.05) for calculated c2 of 43.28 with degree of freedom 10. Occurrence of MDR and XDR bacterial strains among clinical samples bring on economic burden on health system as well as on patient in terms of longer hospital stays and treatment delays.
Antimicrobial Resistance, Multidrug-resistant, Extensive Drug-resistant, Virulence, Antibiotics
Antimicrobial Resistance (AMR) has emerged as the global public health problem of the 21st century and can be defined as the ability of microorganisms to neutralize the action of drugs designed to inhibit or kill them. It is a major threat to public health and poses a huge challenge to treat different ailments. It occurs when microbes develop different mechanisms to withstand the effect of antimicrobials which include enzymatic degradation of antibiotics, modification of the antibiotic target sites, overproduction of the target, replacement of the target, efflux and reduced permeability of the membrane. Antimicrobial selection pressure is the main contributing factor for the development of drug resistance and the propagation of resistant organisms. Other drivers of AMR are unsystematic use of antibiotics, ease in purchase without medical prescription and unreasonable use as growth promoters by animal and agricultural sector. Naturally developed genetic modifications are the mainstay of developing AMR or it can be acquired through horizontal gene transfer between microorganisms.1 Antibiotics have historically been grouped into two broad categories based on their spectrum of activity; broad spectrum and narrow spectrum. Broad spectrum antibiotics have a wider range of activity and are usually considered when the disease etiology is not known whereas narrow spectrum antibiotics are useful in treatment when the causative pathogen is known.2 Based on chemical or molecular structures, antibiotics are mainly categorized into eight classes including beta-lactams, macrolides, tetracyclines, quinolones, aminoglycosides, sulphonamides, glycopeptides and oxazolidinones. Generally, multidrug-resistance (MDR) is defined as acquired resistance to at least one agent in three or more antimicrobial classes tested while extensively
drug-resistance (XDR) as non-susceptibility to at least one agent in all but two or fewer antimicrobial classes. Pan-drug resistance (PDR) is defined as non-susceptibility to all agents in all antimicrobial categories tested. Moreover, misuse and overuse of antibiotics can also disturb the natural microbiome of the planet and due to this practice; even environmental isolates are becoming resistance of antibiotics. It was estimated that 4.95 million deaths were reported in Sub-Saharan Africa and Australasia in the year 2019 and were associated with bacterial AMR. The principal pathogens associated with resistance were Acinetobacter baumannii, Escherichia coli, Klebsiella pneumoniae, Streptococcus pneumoniae, Staphylococcus aureus and Pseudomonas aeruginosa.3 AMR creates a significant financial burden on health systems as well as on national economies overall. Prolonged hospital stays and expensive treatment regimens impose catastrophic costs and affect the overall productivity of patients and their caregivers. Microbial virulence factors are the molecules that contribute in rising pathogenicity of the microorganism. This study aimed in identification, antimicrobial susceptibility testing and expression of selective virulence factors among bacterial isolates recovered from various human clinical cases. This study would help in understanding the local resistance pattern for different antibiotics among clinical isolates and the association of virulence factors with disease severity.
Study site and sampling
Total 350 samples were collected during the three months period (June-August 2022) recovered from various clinical cases at public hospital in Shimla (Himachal Pradesh, India) and a private diagnostic center in Mohali (Punjab, India). This diagnostic centre was providing various phenotypic and molecular diagnostic services to referred samples from adjoining states like Himachal Pradesh, Punjab, Chandigarh and Haryana. Samples collected from the local hospital were immediately shifted to the research laboratory, Department of Microbiology, Himachal Pradesh University (Shimla) in sterile and cool conditions and processed further within 24 hours of collection. Clinical samples received at private diagnostic center were processed there for further isolation and identification of bacteria. Sample sources were urine (n = 120), blood (n = 22), sputum (n = 57), swabs (n = 36), and others (n = 115).
Reference strains used
The standard microbial type culture collection (MTCC) strains previously obtained from CSIR-Institute of Microbial Technology (IMTech) Chandigarh and regularly sub-cultured were used as standard controls in this study. The reference strains used were: Escherichia coli MTCC1687, Salmonella typhi MTCC-98, Staphylococcus aureus MTCC-96 and Pseudomonas aeruginosa MTCC-1688. American type culture collection (ATCC) bacterial strains: Escherichia coli/ATCC 25992/ATCC 35218, Staphylococcus aureus/ATCC 25923 and Pseudomonas aeruginosa/ATCC 27853 were also used as quality control strains in this study.
Isolation and identification of bacteria
Different sample types were processed following standard methodology. Urine samples were streaked on Nutrient agar and MacConkey agar plates. Blood cultures were obtained from aerobic blood culture vials and streaked further to obtain pure cultures. Sputum and pus swabs were serially diluted using 10-fold physiological saline. Appropriate dilutions within the range of 10-2-10-6 were selected and 1 ml inoculums from each tube dilution were inoculated in nutrient broth tubes for enrichment purpose and incubated at 37°C overnight. 0.1 ml volume from 10-2, 10-3 and 10-4 dilutions were poured and spread on nutrient agar plates and incubate at 37°C for 48-72 hours. Cultural characteristics like shape, size, color, elevation and appearance were recorded and purified colonies were obtained by streaking on freshly prepared nutrient agar slants.4 Gram staining was done to evaluate the morphological features and standard biochemical tests were performed to further identify the microorganisms.5 Biochemical characteristics of each organism were interpreted as per Bergey’s Manual of Determinative Bacteriology.6 Culture isolates were maintained in 10% glycerol stocks at -20°C for further use.
In vitro antibiotic cultural sensitivity assay
Antimicrobial susceptibility profiles of the isolates were determined using standard Kirby-Bauer disc diffusion method.7 Freshly grown bacterial colonies were suspended in 4-5 ml normal saline to make bacterial inoculums and the optical density (OD) was adjusted to 0.08 to 0.10 at 625 nm which is equivalent to the 0.5 McFarland’s reference standard. A lawn culture of each bacterial inoculums were prepared on Mueller-Hinton agar plates and antibiotic discs were placed and incubated at 37°C for overnight. Antimicrobial susceptibility pattern was recorded in the form of zone of inhibition around the antibiotic discs. The diameter of zones of inhibition were interpreted as sensitive, intermediate and resistant as per the clinical laboratory standard institute (CLSI) guidelines mentioned in the instructions manual and the technical datasheet with the antibiotic discs.8 The commercially available antibiotic discs used in this study were as follows:
For Urine culture isolates
HiMedia Dodeca UTI-IV (DE011-1PK) antibiotic rings were used containing 12 different antibiotics: Amikacin (AK-30 µg), Cefalexin (CN-30 µg), Ceftriaxone (CTR-30 µg), Cefixime (CFM-5 µg), Cefoperazone (CPZ-75 µg), Nalidixic acid (NA-30 µg), Kanamycin (K-30 µg), Nitrofurantoin (NIT-300 µg), Lomefloxacin (LOM-30 µg), Ofloxacin (OF-5 µg), Norfloxacin (NX-10 µg), Gentamicin (GEN-10 µg).
For other culture isolates
Ampicillin (AMP-10 µg), Amoxicillin-clavulanate (A/CL-20/10 µg), Cefuroxime (CFR-30 µg), Ceftriaxone (CTR-30 µg), Cefotaxime (CFO-30 µg), Ceftazidime (CFZ-30 µg), Meropenem (MRP-30 µg), Trimethoprim/sulfamethoxazole (TRM/SUL-1.25/23.75 µg), Chloramphenicol (CHL-30 µg), Gentamicin (GEN-10 µg), Ciprofloxacin (CPR-5 µg), Nitrofurantoin (NIT-300 µg), Cefepime (CFP 30 µg), Piperacillin/tazobactam (P/-TZ-100-10 µg) and Cefoxitin (CFX-30 µg).
Screening of virulence factors among uropathogens
Standard methodology was followed to determine the expression of virulence factors among uropathogens.9 Additionally, the correlation of drug resistant phenotype (MDR & XDR) with the expression of different virulence factors was also determined using chi-square test (c2).
Motility test
Bacterial isolates were inoculated in a semisolid motility test medium with the help of a straight inoculation needle about 8-10 mm deep into the medium only once and incubated at 37°C for 24 hours. The positive motility test result was indicated by the diffused growth that extends as a zone of turbidity from the stab line and negative results show growth restricted to the stab line.
Lipase production
A sterile egg yolk was mixed in the ratio 1:1 with physiological saline solution. 10% egg yolk was mixed with autoclaved nutrient agar enriched with 1% NaCl. Egg yolk agar medium petri plates were prepared and the test organism inoculums (30 µl each) were placed in the wells and incubated at 37°C for 1-4 days. Production of lipase enzyme by the test organism was indicated by the clear zones around the colonies.
Protease production
2% skimmed milk was added to nutrient agar (Himedia, Mumbai) to prepare the protease test medium. Test organism inoculums in a 30 µl volume were loaded in each well and incubated for 24-72 hours at 37°C. Protease enzyme production was indicated by clear halos around bacterial colonies.
Siderophore production
Siderophores are high-affinity chelating compounds that help bacteria in accumulation of iron. The principal indicator media used for this test were chrome azurol S (CAS) and hexadecyl trimethyl ammonium bromide (HDTMA). Solution-I: 60.5 mg of CAS dye was mixed in 50 ml of double distilled water. Solution-II: 10 ml of Fe (III) solution was made by mixing 27 mg of Ferric chloride hexahydrate (FeCl3.6H20) and 83.3 ml of concentrated hydrochloric acid (HCl) in 10 ml of double distilled water. Solution-III: Mix 72.9mg of hexadecyl trimethyl ammonium bromide (HDTMA) powder in 40 ml of double distilled water. Gently mix all the three solutions to make a 100 ml dark blue colored CAS indicator solution. Add 23 ml of CAS indicator solution to 100 ml Luria Bertani agar medium and mix thoroughly. Pour about 20 ml of medium to each Petri plate and allow to solidify. Inoculate the test organism and incubate overnight at 37°C. Positive siderophore production indicated the formation of orange-colored halos around the colonies.10,11
Presence of capsule
All isolated uropathogens were subjected to capsule staining following standard procedures and the smears were examined under 100X oil emersion objective to observe the clear zones surrounding the bacterial cells.
Biofilm formation
Trypticase soy broth (TSB) tubes containing 1% glucose + 2% sucrose was inoculated with loopful of each test organism. About 200 µl of each inoculum were transferred to microtitre plate and incubated overnight at 37°C. Microtitre plates were decanted off and the plate wells washed in phosphate buffer saline having pH 7.3, air dried and then stained with 0.1% crystal violet. Deionized water was used to remove the excess stain. The adherence of bacteria was recorded by measuring the optical density (OD) at a wavelength of 590 nm using microplate reader. Trypticase soy broth (TSB) tubes containing 1% glucose + 2% sucrose without bacterial cells was used as negative control and the OD value of negative control was subtracted while recording the results. Biofilm producing ability of each test organism was evaluated using three-grade scale, i.e. OD<0.120 = no or weak biofilm producer; 0.120<OD<0.240 = moderate biofilm producer; OD>0.240 = strong biofilm producer.12
Confirmation of Isolates
Of the 350 clinical samples, Escherichia coli, Staphylococcus aureus, Klebsiella pneumonia and Bacillus spp. were identified based on microscopic, cultural and biochemical characterization. Among urine culture isolates, the majority (88.33%) were gram-negative rods, 9.1% and 2.5% were gram-positive cocci and gram-positive bacilli, respectively. However, only gram-negative rods were found in blood, sputum, swabs and other types of clinical samples. K. pneumoniae (51.42%) and E. coli (44.57%) were recovered from all the sample sources while S. aureus (3.15%) and Bacillus spp. (0.86%) were isolated from urine samples only. The details of microorganisms identified and their distribution among different sources are presented in Figure 1. Colony characteristics of different isolates on general purpose and selective media used in this study are given in Figure 2.
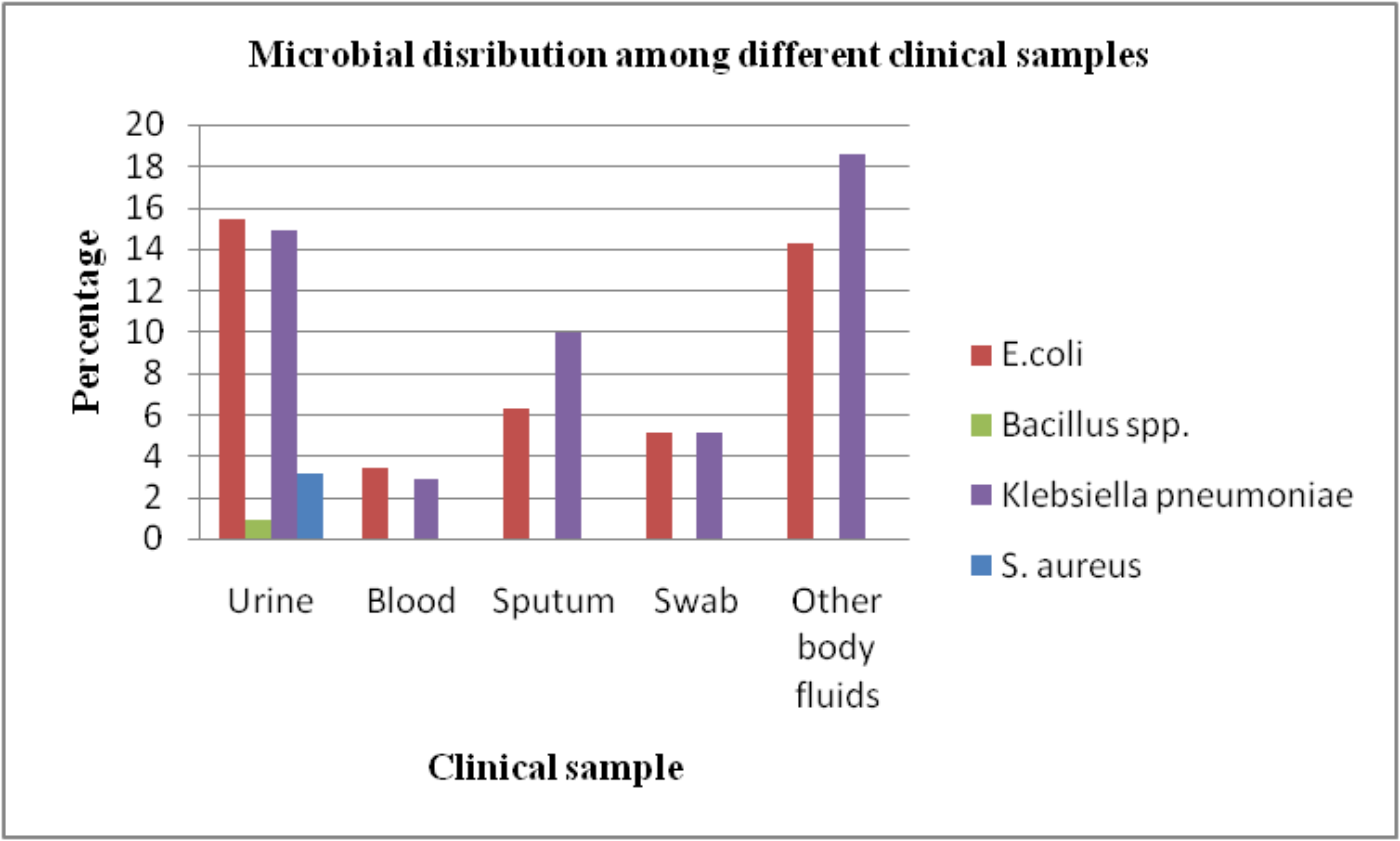
Figure 1. Proportion distribution of bacteria (E. coli, Bacillus spp., K. pneumonia and S. aureus) among various clinical samples
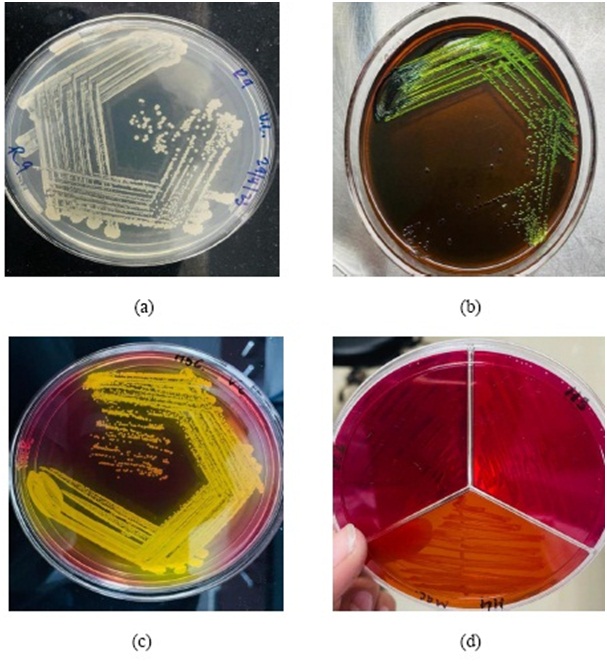
Figure 2. Colony morphology: (a) isolate no. R9 on nutrient agar medium; (b) isolate no. H2 on Eosin-Methylene Blue Agar; (c) isolate no. H5 on Mannitol salt Agar; (d) isolate no. H3 and H4 on MacConkey Agar
Antimicrobial profiling
Kirby-Bauer disc diffusion method was followed to perform antibiotic susceptibility testing for all bacterial isolates. Different antibiotics from diverse antibiotic classes were selected and used to perform in vitro culture sensitivity assay. All K. pneumoniae isolates (100%) were found resistant to ampicillin followed by ceftriaxone, cefepime and ciprofloxacin (97.7% each) and amoxicillin+clavulanic acid (97.22%). Majority (96.15%) of E. coli isolates were resistant to ampicillin followed by amoxicillin+clavulanic acid (91.02%), cefoxitin (85.25%) and cefepime (84.61%). Out of 11 S. aureus isolates, 72.72% were resistant to nitrofurantoin, nalidixic acid (54.54%) and cefixime (45.45%). On the other hand, isolates of Bacillus spp. were found susceptible to all the antibiotics tested except nitrofurantoin and nalidixic acid. Overall maximum resistance was observed against ampicillin (94.28%), amoxicillin+clavulanic acid (90.5%), cefepime (88%) and ceftriaxone (80.18%) while it was minimum for cefoperazone (0.85%), kanamycin (1.14%), lomefloxacin & norfloxacin (1.42% each) and cefixime (1.71%). Among different drug classes where at least 3 antibiotics were included in each class, highest resistance pattern was observed against penicillins (83.14%) followed by cephalosporins (49.61%), aminoglycosides (48.57%) and fluoroquinolones (17.02%). In contrast, resistance was least observed for macrolides class (4%) although only one antibiotic was tested in this group (Table 1).
Table (1):
Antibiogram showing the resistance pattern of the bacterial isolates to different antibiotic classes
| Bacteria (number) | Antibiotic classesa | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AMG | CEP | FQ | PEN | MAC | SLF | AMC | CRB | |||||||||||||||||
| AK (%) | K (%) | GEN (%) | CN (%) | CTR (%) | CFM (%) | CPZ (%) | CFR (%) | CFO (%) | CFZ (%) | CFP (%) | CFX (%) | NA (%) | LOM (%) | OF (%) | NX (%) | CPR (%) | AMP (%) | A/CL (%) | P/TZ (%) | NIT (%) | TRM/SUL (%) | CHL (%) | MRP (%) | |
| K. pneumoniae (180) | 115 (63.8) | NT* | 144 (80) | NT* | 176 (97.77) | NT* | NT* | 115 (63.88) | 144 (80) | 144 (80) | 176 (97.77) | 142 (78.88) | NT* | NT* | NT* | NT* | 176 (97.77) | 180 (100) | 175 (97.22) | 144 (80) | NT* | 144 (80) | 146 (81.11) | 130 (72.22) |
| E. coli (156) | 112 (71.79) | 3 (1.92) | 133 (85.25) | 6 (3.84) | 101 (64.74) | 1 (0.64) | 1 (0.64) | 112 (71.79) | 84 (53.84) | 84 (53.84) | 132 (84.61) | 133 (85.25) | 3 (1.92) | 2 (1.28) | 1 (0.64) | 1 (0.64) | 100 (64.10) | 150 (96.15) | 142 (91.02) | 82 (52.56) | 5 (3.20) | 105 (67.30) | 126 (80.76) | 114 (73.07) |
| S. aureus (11) | 0 | 1 (9.09) | 2 (18.18) | 1 (9.09) | 4 (36.36) | 5 (45.45) | 2 (18.18) | NT* | NT* | NT* | NT* | NT* | 6 (54.54) | 3 (27.27) | 1 (9.09) | 4 (36.36) | NT* | NT* | NT* | NT* | 8 (72.72) | NT* | NT* | NT* |
| Bacillus spp. (3) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | NT* | NT* | NT* | NT* | NT* | 1 (33.33) | 0 | 0 | 0 | NT* | NT* | NT* | NT* | 1 (33.33) | NT* | NT* | NT* |
| Total (350) | 227 (64.85) | 4 (1.14) | 279 (79.71) | 7 (2) | 281 (80.28) | 6 (1.71) | 3 (0.85) | 227 (64.85) | 228 (65.14) | 228 (65.14) | 308 (88) | 275 (78.57) | 10 (2.85) | 5 (1.42) | 2 (0.57) | 5 (1.42) | 276 (78.85) | 330 (94.28) | 317 (90.57) | 226 (64.57) | 14 (4) | 249 (71.14) | 272 (77.71) | 244 (69.71) |
aAbbreviations used:
For Antibiotic classes: AMG= aminoglycosides, CEP= cephalosporins, FQ= fluoroquinolones, PEN= penicillins, MAC= macrolides, SLF= sulfonamides, AMC= amphenicols, CRB= carbapenems. For Antibiotics: AK= Amikacin, CN= Cefalexin, CTR= Ceftriaxone, CFM= Cefixime, CPZ= Cefoperazone, NA= Nalidixic acid, K= Kanamycin, NIT= Nitrofurantoin, LOM= Lomefloxacin, OF= Ofloxacin, NOR= Norfloxacin, GEN= Gentamicin, AMP= Ampicillin, A/CL= Amoxicillin/clavulanate, CFR= Cefuroxime, CFO= Cefotaxime, CFZ= Ceftazidime, MRP= Meropenem, TRM/SUL= Trimethoprim/sulfamethoxazole, CHL= Chloramphenicol, CPR= Ciprofloxacin, CFP= Cefepime, P/TZ= Piperacillin/tazobactam, CFX= Cefoxitin. *NT= Not Tested
Among urine culture isolates, majority were found resistant to cefepime (91%), amoxicillin+clavulanic acid & gentamicin (90% each), ampicillin (83%) and cefoxitin (82%) while 1.6%, 2.5% and 3.33% resistance was observed for ofloxacin, cefoperazone and kanamycin respectively. 100% resistance was observed against ampicillin among all clinical samples except urine. Antibiogram showing resistance pattern among different clinical samples is presented in Figure 3. Overall, 52.28% of isolates were multidrug resistant (MDR) followed by multidrug sensitive (MDS) (34.28%) & extensive drug resistant (XDR) (13.42%). MDR & XDR were more prominent in isolates recovered from other body fluid samples which include tracheal fluids and cerebrospinal fluids (CSF). Overall allocation of MDS, MDR & XDR among different sample types is presented in Figure 4. Highest MDR percentage was recorded from E. coli (10.8%) and K. pneumoniae (10.2%) isolates recovered from other body fluids. Majority of the isolates with XDR phenotype were K. pneumoniae (3.42%) and E. coli (2%) and it was recorded least among S. aureus (0.85%). The percentage distribution of MDR & XDR among bacterial isolates recovered from different clinical sources is presented in Figure 5.
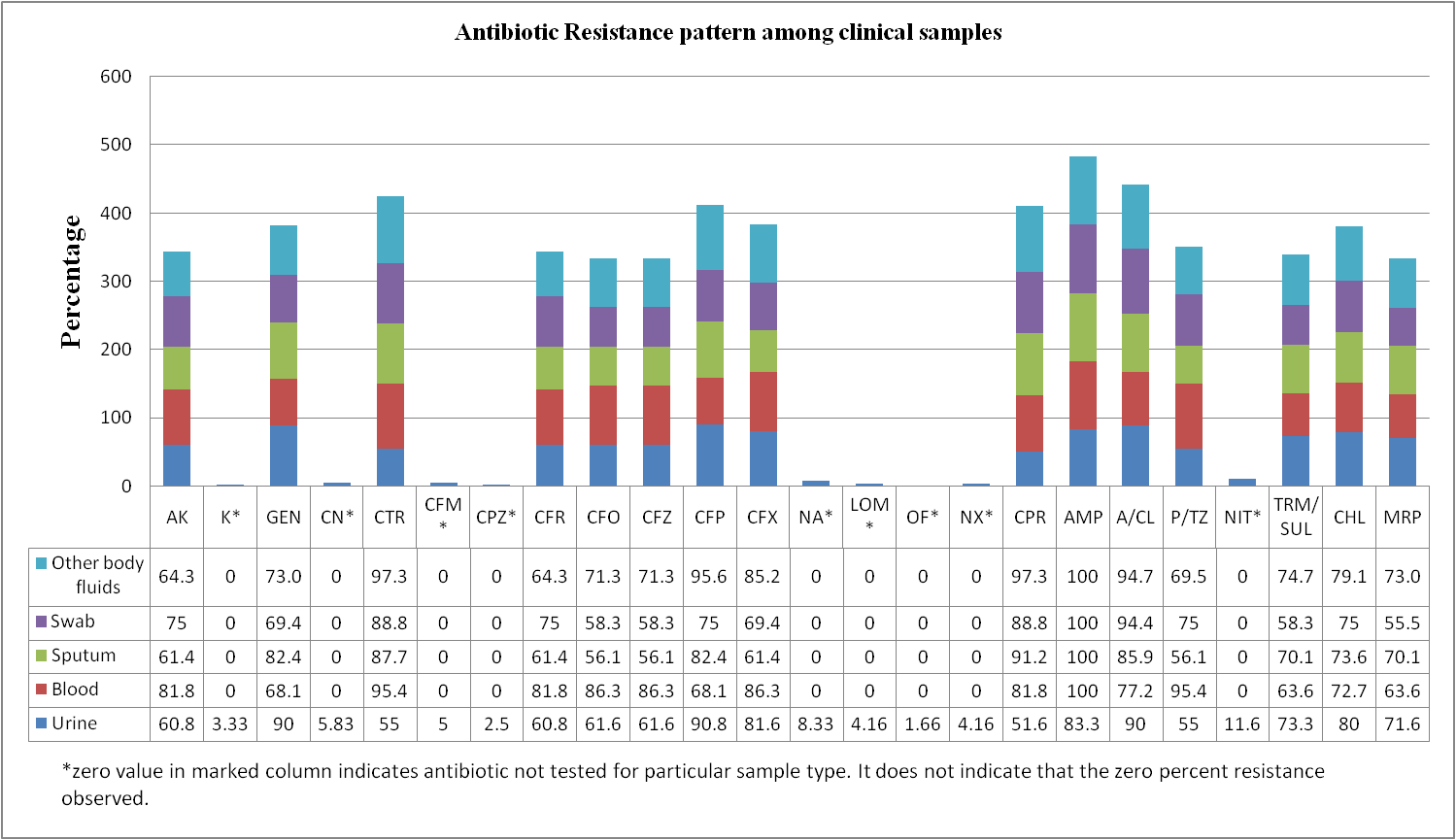
Figure 3. Antibiotic resistance pattern among various human clinical samples for antibiotics with different concentrations tested
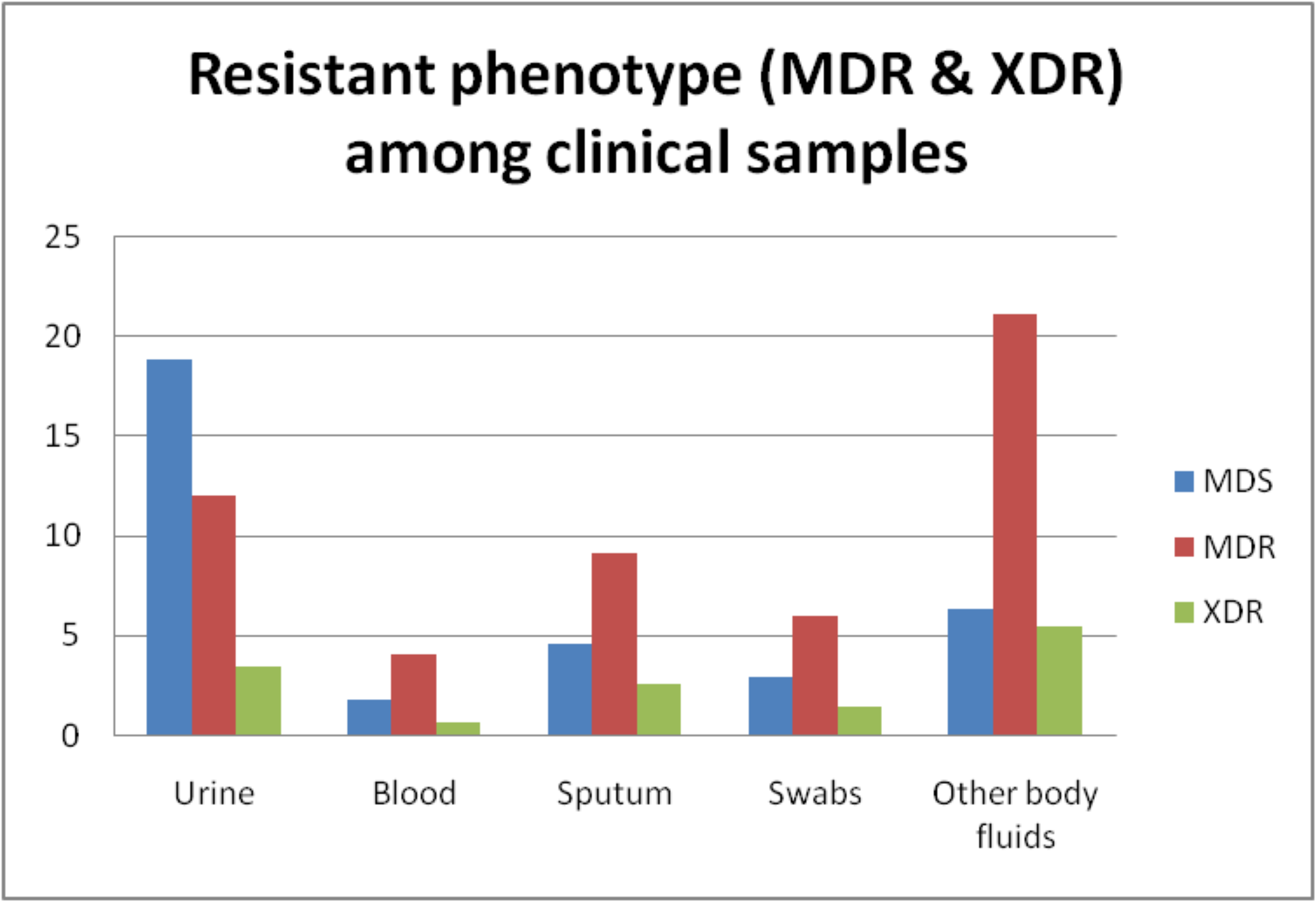
Figure 4. Percentage distribution of multidrug-resistant (MDR), multidrug-sensitive (MDS) and extensive drug resistant (XDR) among clinical samples
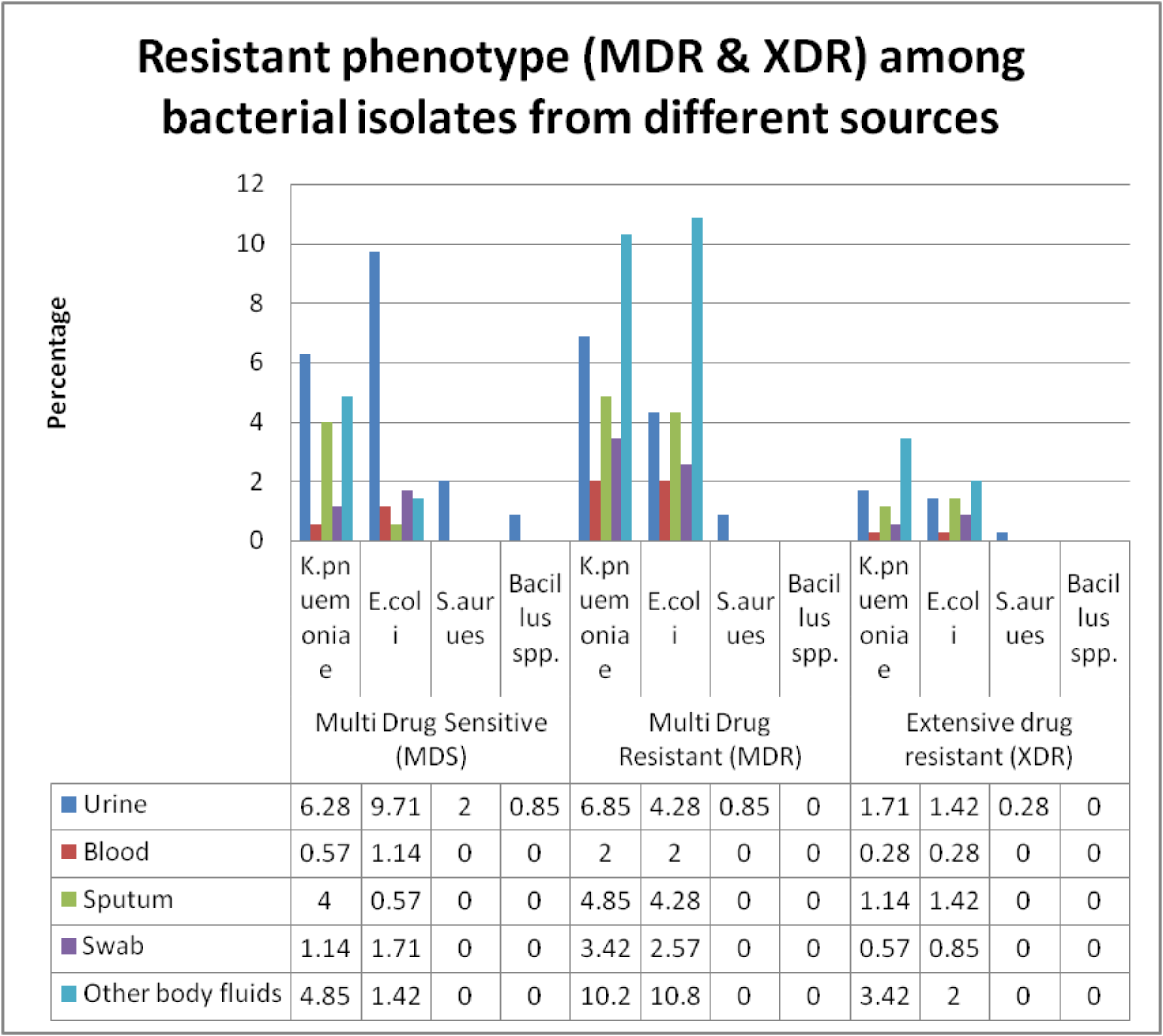
Figure 5. Frequency distribution of multidrug-resistant (MDR), multidrug-sensitive (MDS) and extensive drug resistant (XDR) among bacterial isolates from various clinical sources
Determination of virulence factors
Of 350 bacterial isolates, virulence factors were studied among uropathogens only. Out of 120 urine culture isolates, capsule production was observed in all the isolates, protease production (94.16%), lipase (90%), motility (47.5%), siderophore and biofilm production (45% each). Virulence factors like motility, lipase, protease and capsule production were expressed by both drug resistant as well as drug sensitive bacterial isolates. However, siderophore and biofilm production was seen among isolates with resistant phenotype only (Table 2). The probability value (p-value) corresponds to a c2 of 43.28 with 10 degrees of freedom is less than 0.05. Therefore, there was a statistically significant relation between drug resistant phenotype and expression of siderophore and biofilm as virulence factors, as p<0.05 for calculated c2 of 43.28. On the other hand, there was no significant relation between drug resistant characteristic and production of other virulence traits (lipase, protease, capsule and motility) as the p-value corresponds to more than 0.05 for calculated chi-square values (Table 3).
Table (2):
The number of bacterial isolates expressing different virulence factors and their distribution among MDR, MDS and XDR phenotype
| Virulence trait | Multi Drug Sensitive (MDS) | Multi Drug Resistant (MDR) | Extensive drug resistant (XDR) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| K. pnuemoniae | E. coli | S. aureus | Bacillus spp. | K. pnuemoniae | E. coli | S. aureus | Bacillus spp. | K. pnuemoniae | E. coli | S. aureus | Bacillus spp. | Total | |
| Motility | 0 | 34 | 0 | 3 | 0 | 15 | 0 | 0 | 0 | 5 | 0 | 0 | 57 |
| Lipase | 20 | 29 | 7 | 3 | 24 | 10 | 3 | 0 | 6 | 5 | 1 | 0 | 108 |
| Protease | 19 | 34 | 7 | 3 | 24 | 11 | 3 | 0 | 6 | 5 | 1 | 0 | 113 |
| Siderophore | 0 | 0 | 0 | 0 | 24 | 15 | 3 | 0 | 6 | 5 | 1 | 0 | 54 |
| Capsule | 22 | 34 | 7 | 3 | 24 | 15 | 3 | 0 | 6 | 5 | 1 | 0 | 120 |
| Biofilm | 0 | 0 | 0 | 0 | 24 | 15 | 3 | 0 | 6 | 5 | 1 | 0 | 54 |
Table (3):
Correlation between expression of virulence factors and drug resistant phenotype
| Variable 1 | Variable 2 | χ2 (calculated) | Significance level for calculated χ2 | Significant relation between both the variables |
|---|---|---|---|---|
| Drug Resistant phenotype | Siderophore production | 43.28 | p < 0.05 | Yes |
| Biofilm production | 43.28 | p < 0.05 | Yes | |
| Capsule production | 5.41 | p > 0.05 | No | |
| Lipase production | 4.55 | p > 0.05 | No | |
| Protease production | 5.84 | p > 0.05 | No | |
| Motility | 9.67 | p > 0.05 | No |
χ2 (tabular) = 18.307 (significance level 0.05 with degree of freedom 10)
Bacterial identification in fundamental clinical samples is necessary to study disease etiology and their associated markers like antimicrobial susceptibility pattern, resistance mechanisms, and other factors responsible for disease severity. The emergence of more virulent drug resistant strains also increases the cost of treatment and makes it difficult in terms of affordability and economic stability. This study intended to determine the antimicrobial susceptibility pattern of bacterial isolates from different clinical cases and their classification as MDR and XDR. The correlation between drug resistant phenotype and the expression of selective virulence traits was also determined statistically. In our study, gram-negative rods represented most of the clinical isolates and K. pneumoniae (51.42%) were most common followed by E. coli (44.57%). Similar findings were reported from Saudi Arabia (71.9%),13 Lebanon (81%),14 and China (81.6%).15 Gram-negative bacteria are significantly associated with various clinical conditions due to their distinctive structure, inherent properties to become resistant to antibiotics and the ability to pass along the resistant trait through horizontal gene transfer among bacterial species.
Broad spectrum antibiotics such as cephalosporins, fluoroquinolones, aminoglycosides and carbapenems are commonly prescribed for treating Klebsiella infections. In this study, the majority of K. pneumoniae isolates were resistant to ampicillin (100%), amoxyclav (97.22%) and even third and fourth generation cephalosporins (ceftriaxone & cefepime) which is comparable with other studies.16-18 A significantly decreasing trend in susceptibility to 1st, 2nd and 3rd generation cephalosporins has also been reported against K. pneumoniae isolates from Taiwan.19 E. coli isolates were found to be resistant to ampicillin (96.15%) & amoxyclav (91.02%), followed by cefoxitin (85.25%) and cefepime (84.61%) in our study. Similarly, lower susceptibility rates for ampicillin (39.1%) and amoxicillin-clavulanic acid (64.9%) were reported from Tunisia.20 Another study also reported the highest rate of E. coli resistance for amoxicillin (85%), followed by cefuroxime (65%) and ceftriaxone (60%).21 In this study, S. aureus and Bacillus spp. were found in urine samples only and majority of both the bacterial isolates were resistant to nitrofurantoin and nalidixic acid. Several studies reported lower susceptibility to nitrofurantoin and nalidixic acid among uropathogenic S. aureus strains.22,23 However, S. aureus is a relatively uncommon cause of urinary tract infections and accounts for only 0.5-6% cases worldwide and usually occur in patients with urinary tract catheterization.24 Catheterization associated with UTI signifies the restricted use of urinary instrumentation in essential and emergency cases only and removal of the device as soon as clinically indicated.25,26
In our study, resistance seems to be higher for cefepime (4th generation cepahalosporin) among uropathogens as compared to isolates recovered from other sources; this may be due to difference in sample sizes. However, developing resistance to an antibiotic with a wide spectrum of activity shows the indiscriminate use of a potent drug and production of extended spectrum beta lactamases (ESBLs). Further molecular characterization of the isolates may help in understanding the resistance mechanism, transmission dynamics and genotypes prevalent in this region of the country. Increased cefepime resistance in S. enteritidis due to blaCTX-M-55 gene harboring plasmids and their transmission among bacterial species has also been reported from Shanghai, China.27 While 52.28% of total isolates were MDR, followed by extensive drug resistant bacteria with a percentage of 13.42% which was more compared to the data reported by Basak et al.28 The discordance in reporting of MDR and XDR between both the studies could be the difference in sample sizes and indiscriminate use of antibiotics by the study population. MDR & XDR were more prominent in isolates from tracheal fluids and cerebrospinal fluids (CSF) in our study and that might be due to systemic spread of infection and prolonged use of antibiotics in due course. Our study reported higher frequency of extensive drug resistant K. pneumoniae which is comparable with one study from Middle East reported the expression of various b-lactamase and integron genes.29 MDR and XDR isolates from our study can be further characterized genotypically for extended spectrum beta-lactamases (ESBLs), metallo beta-lactamases (MBLs) and other possible drug resistance mechanisms.
The expression of siderophores and biofilm as virulence factor among drug-resistant phenotype and their correlation was found statistically significant in the present study. Biofilm producing bacterial strains are prominently associated with chronic infections, contribute to disease pathogenesis and disease severity.30 One study reported a positive association between hemolytic activity, biofilm formation and higher levels of antimicrobial resistance among uropathogenic E. coli strains.31 In contrast, our previous studies reported the expression of some virulence factors between MDR and MDS isolates is equally likely.9,32 Our study has certain limitations which includes the isolates could have been identified based on molecular methods but has not been attempted due to budgetary constraints to avail commercially available services. However, the molecular identification of the isolates will be done in the near future to confirm the bacterial species. The presence of virulence genes and their expression among drug resistant and drug susceptible bacterial strains will also be confirmed among the studied isolates.
Bacterial isolates recovered from various human clinical cases were identified and characterized as multidrug resistant (MDR) and extensive drug resistant (XDR) based on their antimicrobial resistance pattern. Among virulence traits studied for uropathogens, biofilm formation and siderophore production are significantly associated with drug resistant phenotype conferring increased pathogenicity and posing a great challenge to the treating clinicians. This study reported high resistance rates of K. pneumoniae amongst commonly prescribed antibiotics like ampicillin, amoxyclav and even third generation cephalosporins like ceftriaxone & cefepime. The percentage of MDR and XDR isolates were more noticeable in isolates from tracheal fluids and cerebrospinal fluids. Antimicrobial resistance (AMR) has become a major challenge to global health due to the lack of new antibiotics in the development pipeline and infections caused by MDR pathogens becoming untreatable. The awareness campaigns to combat AMR like antimicrobial stewardship programs offer an integrated approach to promoting and monitoring the judicious use of antimicrobials; prevent transmission of drug-resistant organisms, and improve environmental decontamination. Altogether “One Health” approach assemble various sectors at different levels to work together for the humanity as a whole and foster well-being of humans, animals and our ecosystem.
ACKNOWLEDGMENTS
The authors are thankful to the Vice Chancellor, Himachal Pradesh University (HPU) and the Chairman, Department of Microbiology, HPU Shimla, for providing infrastructural support to carry out this research work. Authors also acknowledges the support of private diagnostic centre for providing clinical samples.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
BM and NM conceptualized the study. VC, SA and VT applied methodology. VC, SA, AS and VT investigated the study. AS, BM and NM performed data curation. NM and BM performed formal analysis. BM and VC wrote original draft. NM wrote, reviewed and edited the manuscript. BM and NM performed supervision. All authors read and approved the final manuscript for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
Not applicable.
- Fluit AC, Visser MR, Schmitz FJ. Molecular Detection of Antimicrobial Resistance. Clin Microbiol Rev. 2001;14(4):836-871.
Crossref - Acar J. Broad- and narrow-spectrum antibiotics: an unhelpful categorization. Clin Microbiol Infect. 1997;3(4):395-396.
Crossref - Murray, Christopher J L, Ikuta, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;339(10325):629-655.
Crossref - Krishna AR, Aparna AR. Screening and Isolation of Antibiotic producing Microorganisms from Soil. Int J Sci Res Biol Sci. 2019;6(1):46-49.
Crossref - Varghese N, Joy PP. Microbiology Laboratory Manual. 1st ed. Aromatic and Medicinal Plants Research Station, Odakkali, Asamannoor P.O., Ernakulam District, Kerala, India; 2014. https://www.researchgate.net/publication/306018042_Microbiology_Laboratory_Manual.
- John G Holt. Bergey’s Manual of Determinative Bacteriology. 9th ed. Lippincott Williams & Wilkins. 1994.
- Bauer AW, Kirby WMM, Sherris JC, Turck M. Antibiotic susceptibility testing by a standardized single disk method. Tech Bull Regist Med Technol. 1966;45(4):493-496.
Crossref - Himedia Laboratories. Technical Data. Published online January 2011. https://www.himedialabs.com/media/TD/DE011.pdf
- Minhas N, Sharma PC. Studies on Multiple Drug Resistance (MDR) among Pseudomonas aeruginosa Isolates and their Virulence Factors. J Pure Appl Microbiol. 2015;9(2):1447-1456.
- Himpsl SD, Mobley HLT. Siderophore Detection Using Chrome Azurol S and Cross-Feeding Assays. Methods Mol Biol. 2019;2021:97-108.
Crossref - Schwyn B, Neilands JB. Universal chemical assay for the detection and determination of siderophores. Anal Biochem. 1987;160(1):47-56.
Crossref - Christensen GD, Simpson WA, Younger JJ, et al. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: a quantitative model for the adherence of staphylococci to medical devices. J Clin Microbiol. 1985;22(6):996-1006.
Crossref - Alhumaid S, Al Mutair A, Al Alawi Z, et al. Antimicrobial susceptibility of gram-positive and gram-negative bacteria: a 5-year retrospective analysis at a multi-hospital healthcare system in Saudi Arabia. Ann Clin Microbiol Antimicrob. 2021;20(1):43.
Crossref - Moghnieh RA, Abdallah DI, Fawaz IA, et al. Prescription Patterns for Tigecycline in Severely Ill Patients for Non-FDA Approved Indications in a Developing Country: A Compromised Outcome. Front Microbiol. 2017;8:497.
Crossref - Xu L, Zeng Z, Ding Y, Song M, Yang K, Liu J. Distribution and Antimicrobial Susceptibility of Gram-Positive and Gram-Negative Pathogens Isolated from Patients Hospitalized in a Tertiary Teaching Hospital in Southwestern China. Jundishapur J Microbiol. 2021;13(12): 111682.
Crossref - Aktas E, Yigit N, Yazgi H, Ayyildiz A. Detection of Antimicrobial Resistance and Extended-Spectrum a-Lactamase Production in Klebsiella Pneumoniae Strains from Infected Neonates. J Int Med Res. 2002;30(4):445-448.
Crossref - Manjula NG, Math GC, Nagshetty K, Patil SA, Gaddad SM, Shivannavar CT. Antibiotic Susceptibility Pattern of ESגL Producing Klebsiella pneumoniae Isolated from Urine Samples of Pregnant Women in Karnataka. J Clin Diagn Res. 2014;8(10):DC08-11.
Crossref - Jett BD, Ritchie DJ, Reichley R, Bailey TC, Sahm DF. In vitro activities of various beta-lactam antimicrobial agents against clinical isolates of Escherichia coli and Klebsiella spp. resistant to oxyimino cephalosporins. Antimicrob Agents Chemother. 1995;39(5):1187-1190.
Crossref - Lin WP, Wang JT, Chang SC, et al. The Antimicrobial Susceptibility of Klebsiella pneumoniae from Community Settings in Taiwan, a Trend Analysis. Sci Rep. 2016;6(1):36280.
Crossref - Daoud N, Hamdoun M, Hannachi H, Gharsallah C, Mallekh W, Bahri O. Antimicrobial Susceptibility Patterns of Escherichia coli among Tunisian Outpatients with Community-Acquired Urinary Tract Infection (2012-2018). Curr Urol. 2020;14(4):200-205.
Crossref - Wu D, Ding Y, Yao K, Gao W, Wang Y. Antimicrobial Resistance Analysis of Clinical Escherichia coli Isolates in Neonatal Ward. Front Pediatr. 2021;9:670470.
Crossref - Alshomrani MK, Alharbi AA, Alshehri AA, Arshad M, Dolgum S. Isolation of Staphylococcus aureus Urinary Tract Infections at a Community-Based Healthcare Center in Riyadh. Cureus. 2023;15(2):e35140.
Crossref - Yousefi M, Pourmand MR, Fallah F, Hashemi A, Mashhadi R, Nazari-Alam A. Characterization of Staphylococcus aureus Biofilm Formation in Urinary Tract Infection. Iran J Public Health. 2016;45(4):485-493.
- Akorthal EE, Ibadin OK. Incidence and antibiotic susceptibility pattern of Staphylococcus aureus amongst patients with urinary tract infection (UTI) in UBTH Benin City, Nigeria. Afr J Biotechnol. 2008;7(11):1637-1640.
Crossref - Mason CY, Sobti A, Goodman AL. Staphylococcus aureus bacteriuria: implications and management. JAC Antimicrob Resist. 2023;5(1):dlac123.
Crossref - Muder RR, Brennen C, Rihs JD, et al. Isolation of Staphylococcus aureus from the Urinary Tract: Association of Isolation with Symptomatic Urinary Tract Infection and Subsequent Staphylococcal Bacteremia. Clin Infect Dis. 2006;42(1):46-50.
Crossref - Fu Y, Xu X, Zhang L, et al. Fourth Generation Cephalosporin Resistance Among Salmonella enterica Serovar Enteritidis Isolates in Shanghai, China Conferred by blaCTX-M-55 Harboring Plasmids. Front Microbiol. 2020;11:910.
Crossref - Basak S, Singh P, Rajurkar M. Multidrug Resistant and Extensively Drug Resistant Bacteria: A Study. J Pathog. 2016;2016:1-5.
Crossref - Farhadi M, Ahanjan M, Goli HR, Haghshenas MR, Gholami M. High frequency of multidrug-resistant (MDR) Klebsiella pneumoniae harboring several a-lactamase and integron genes collected from several hospitals in the north of Iran. Ann Clin Microbiol Antimicrob. 2021;20(1):70.
Crossref - Vestby LK, Gronseth T, Simm R, Nesse LL. Bacterial Biofilm and its Role in the Pathogenesis of Disease. Antibiotics. 2020;9(2):59.
Crossref - Baldiris-Avila R, Montes-Robledo A, Buelvas-Montes Y. Phylogenetic Classification, Biofilm-Forming Capacity, Virulence Factors, and Antimicrobial Resistance in Uropathogenic Escherichia coli (UPEC). Curr Microbiol. 2020;77(11):3361-3370.
Crossref - Minhas B, Bali P, Minhas N. Isolation And Characterization Of Multi-Drug Resistant (Mdr) And Extensively Drug Resistant (Xdr) Bacteria From Diverse Environmental Niches. IJPSR. 2023;15(2):398-408.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.