

ISSN: 0973-7510
E-ISSN: 2581-690X
This study was taken up to determine the prevalence of potential pathogens in most touched fomites in Neonatal Intensive Care Units (NICUs) and to determine their antibiogram. Fifty swabs each were collected from fomites from In-born (for babies born in our center) and out-born (for babies born elsewhere, brought to our center) NICUs, before and after cleaning. Samples were processed using standard Microbiological techniques. Antibiogram was determined by Kirby-Bauer disc diffusion method. From In-born NICU, before cleaning, 42 (84%) samples yielded growth with 48 bacterial isolates of which 31 (64.6%) were pathogens and after cleaning, 40 (80%) samples yielded growth with 41 bacterial isolates, of which 30 (73.1%) were pathogens. Most frequent isolates were non-fermenting gram-negative bacilli (NFGNB) and Klebsiella pneumoniae before and after cleaning, respectively. Prevalence of bacteria from In-born NICU before and after the cleaning was statistically significant (p = 0.025). From Out-born NICU, before cleaning, 42 (84%) samples yielded growth with 45 bacterial isolates, of which 25 (55.55%) were pathogens. Samples collected after cleaning; 42 (84%) samples yielded growth with 43 bacterial isolates of which 19 (44.18%) were pathogens. Most frequent isolates were NFGNB and Klebsiella pneumoniae from In-born NICU and K. pneumoniae and Escherichia coli from Out-born NICU before and after cleaning, respectively. Overall prevalence of pathogens was significant (p = 0.007). Staphylococcal isolates were resistant to Methicillin. NFGNB exhibited highest resistance (55.9%) towards Gentamicin. Significant decrease in the frequency of pathogens after cleaning indicates stringent practice of sterilization protocol would be essential in hospital environment.
NICU, Fomites, Prevalence, Nosocomial Pathogens, Gram-negative Bacteria, Sterilization
Fomites are inanimate objects capable of absorbing, harboring, and transmitting infectious microorganisms.1-4 The presence of potential pathogens on fomites in hospital environments like stethoscopes, suction equipment, the nozzle of the antiseptic dispenser, bed rails, bed linens, door handles, lavatory seats, work desks, mobile phones, etc., has been extensively reported.3,5,6 Transmission of the pathogens to the patient may occur through direct contact of the patient with the contaminated object, or via the hands or gloves of a clinician or any health care personnel.5,7,8 Microorganisms can survive for a long period on fomites in the hospital environment. Therefore, these fomites act as reservoirs or sources of a variety of nosocomial pathogens such as methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin-resistant Enterococci (VRE), Candida species, members of Enterobacteriaceae, etc. Hospital-acquired infections continue to be a serious and universal complication of hospitalization. The neonatal intensive care units (NICUs) are no exception to this. The inmates of NICUs are immunocompromised in one or the other way and also several risk factors are associated with infections in NICUs.2,6,9-11
Our Centre, being a tertiary health care center, caters to the health needs of neighboring districts also. We have two NICUs in our center. The “In born” NICU is for neonates born at our center and the “out born” NICU is for neonates born elsewhere and brought to our center for further care.
We strongly felt that baseline data needs to be created about the prevalence of microorganisms on fomites from our NICUs. It is even more essential to know the frequency of the presence of potential pathogens on these fomites from NICUs as these organisms can cause serious healthcare-associated infections. We also planned to study the Antibiogram of these probable pathogens. Thus, the study was taken up to know the frequency of potential pathogens in the fomites of NICUs and to assess the antibiogram of these organisms. Knowledge about the prevalence and the antibiogram will benefit us in improvising infection control practices and empirical therapy to a great extent.
This study was conducted in the Department of Microbiology of a tertiary healthcare teaching hospital. The study was conducted with the approval of the Institutional Ethics Committee. All culture media and antibiotic disks used in this study were procured from Hi Media Pvt. Ltd, Mumbai, India.
Samples were collected from two NICUs of our hospital before and after the routine cleaning process every Monday for 5 weeks. At the end of the study, a total of 50 swabs each were collected from fomites from Inborn and Out born NICUs before and after cleaning. Fomites that frequently come in contact with either the health care personnel or the patient were selected for this study (Table 1).
Table (1):
List of fomites used for sampling
No. |
Name of Fomite |
1 |
Cradle/bed railings |
2 |
Bed linen |
3 |
Medicine Trolley |
4 |
Telephones |
5 |
Wash basin |
6 |
Water taps |
7 |
Nurses’ station |
8 |
Main door handles |
9 |
Sterile towels |
10 |
Nozzles of antiseptic dispensers |
Sterile cotton swab pre-moistened with thioglycolate (TG) broth was rubbed over each fomite covering a 10 × 10 cm area for regular-shaped fomites and irregularly shaped fomites, the sample from different angles, and crevices were collected. After collection, these swabs were immediately transported to the laboratory in TG broth and incubated overnight at 37°C.12 Totally 50 samples each were collected from fomites from Inborn and Outborn NICUs before and after cleaning.
The TG broths showing turbidity were further subcultured on blood agar (BA) and Mac Conkey’s agar (MA) for isolation of bacteria and incubated at 37°C/ 24 hours. Sabouraud’s dextrose agar (SDA) was also inoculated for fungal isolation and was incubated at 37°C for 24 to 48 hours. The TG tubes without any turbidity at 24 hours were further incubated and read after 48 hours of incubation and considered sterile or no growth if turbidity was not present. Identification of organisms was done using standard microbiological methods.
Colony morphology on BA, MA was studied and Gram staining was done from each type of colony to determine Gram-positive, Gram-negative nature and also typical arrangement of bacteria that help in the identification of our isolates. A panel of biochemical tests such as sugar fermentation, citrate utilization, urease production, indole detection, methyl red reaction, Voges-Proskauer test, production of H2S, oxidase test, catalase test, coagulase test, hanging drop test, etc. were performed accordingly for the identification of isolates.13 Fungi were not recovered from our samples.
The bacterial isolates that can produce disease were considered potential pathogens and isolates without such ability were considered non-pathogens. All the potentially pathogenic bacterial isolates were tested for their antibiotic susceptibility against a panel of antibiotics according to Clinical and Laboratory Standards Institute (CLSI) guidelines using the Kirby-Bauer disc diffusion method.
Sterile and dry Muller Hinton (MH) agar plates were used for the disc diffusion method. The plates were inoculated with 6 hour-broth culture (0.5 McFarland Standard, 1.5 × 108 CFU/ml) using a sterile cotton swab to get a lawn culture. Antibiotic disks were placed on the MH plates using sterile forceps. The plates were incubated at 37°C overnight. The zone of inhibition of growth was measured in millimeters and compared with the standard Kirby-Bauer chart and results were recorded accordingly. The Cefoxitin disc (30 mcg/ disc) screening method was used to determine methicillin resistance. If the diameter of the zone of inhibition was ≤21 mm and ≤24 mm, then the isolates of S. aureus and CoNS were considered as MRSA and MRCoNS respectively.14,15
Statistical analysis of the data was done using Statistical Package for the Social Sciences (SPSS) version 20. The Chi-square test was applied to determine the significance of the difference observed in this study. Results were interpreted as significant if the p-value was <0.05. The frequency of isolation of organisms was expressed in percentage.
Samples were collected from the specified fomites as described earlier. A total of 177 bacterial isolates were observed in this study. Out of these 105 (59.32%) isolates were potential pathogens and the remaining 72 (40.67%) isolates were non-pathogens such as aerobic spore bearers and micrococci, which were not further processed in this study (Figure). Based on the earlier reports any bacterial isolate with the ability to produce disease was considered as a potential pathogen. We observed that the overall frequency of isolation of gram-negative bacilli was more (84.8 %, 89/105) than gram-positive cocci (15.2 %, 16/105). This difference could be due the better survival strategies of gram-negative bacilli as against gram-positive cocci at that point of time of this study. In the present study, we have not determined any association between the clinical isolates from neonates and isolates from fomites.
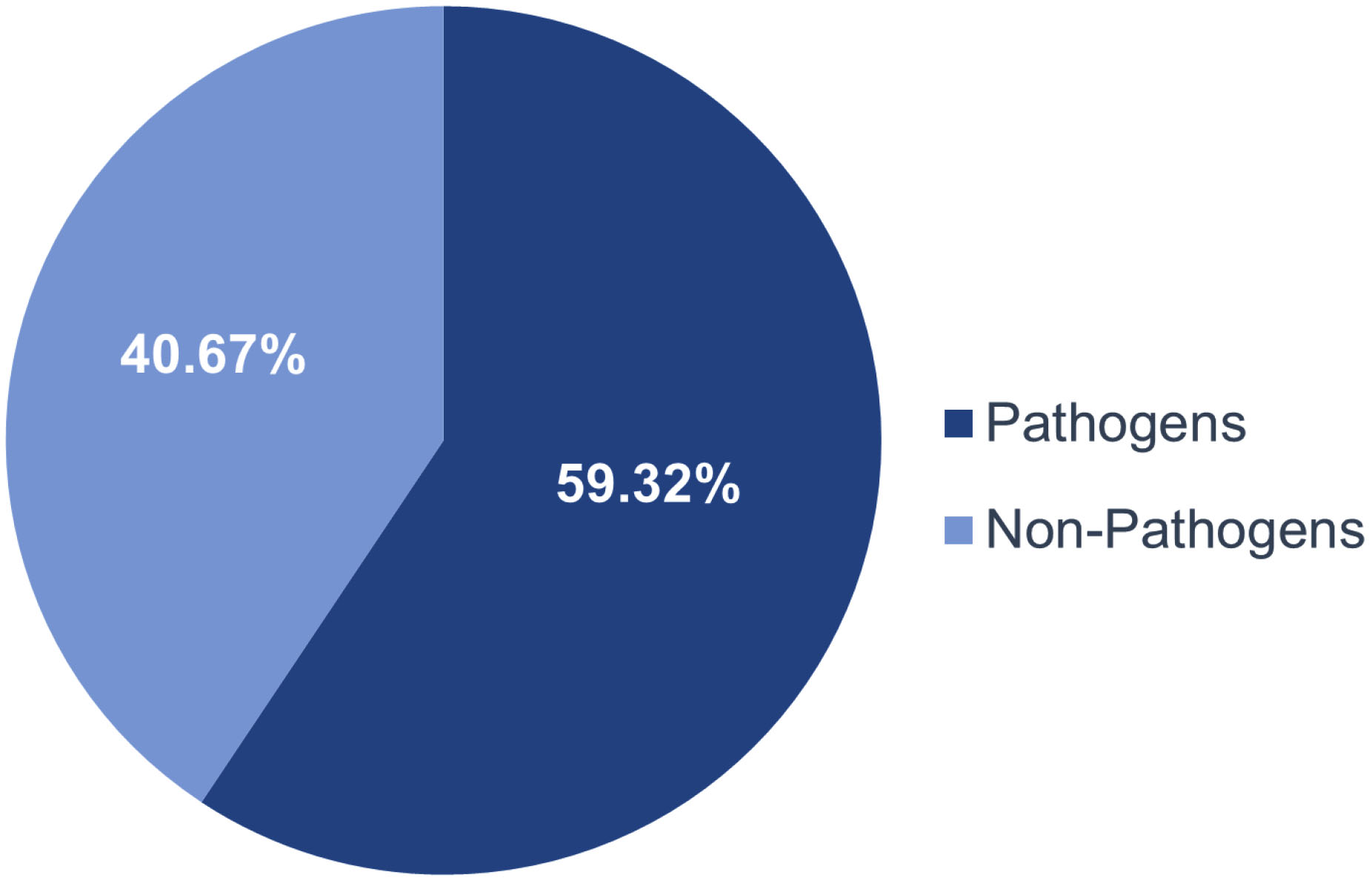
Figure. Prevalence of bacteria in both NICUs before and after cleaning
Prevalence of microorganisms in In-born and Out-born NICU before and after the routine cleaning procedure
The overall frequency of isolation of microorganisms from the In-born NICU before and after the cleaning procedure was 84% and 80% respectively. However, this variation was not statistically significant (p= 0.603). In the case of Out-born NICU, the overall prevalence of microorganisms remained unchanged before and after cleaning with an 84% rate of isolation.
In-born NICU before cleaning
Of 50 samples collected 42 samples (84%) yielded growth resulting in 48 bacterial isolates. 8 (16%) samples yielded no growth. Out of 48 isolates, 31 (64.6%) were potential pathogens and 17 (35.4%) were non-pathogens.
In-born NICU after cleaning
We observed that of 50 samples collected 40 (80%) samples yielded growth and the remaining 10 (20%) yielded no growth. 41 bacterial isolates were grown out of which 30 (73.1%) were potential pathogens and 11 (26.8%) were non-pathogens.
The most frequent isolates were non-fermenting gram-negative bacilli (NFGNB) before cleaning which was replaced by K. pneumoniae after cleaning. MRSA, E. faecalis, P. aeruginosa, C. diversus were not isolated from In-born NICU after cleaning (Table 2).
Table (2):
Prevalence of pathogenic bacteria in Inborn NICU before and after cleaning
Potential Pathogens |
Before cleaning n (%) |
After cleaning n (%) |
|---|---|---|
NFGNB |
7 (22.6) |
5 (16.6) |
E. faecalis |
6 (19.4) |
NI* |
E. coli |
5 (16.1) |
6 (20) |
E. aerogenes |
3 (9.7) |
7 (23.3) |
K. pneumoniae |
3 (9.7) |
8 (26.6) |
Acinetobacter spp. |
2 (6.5) |
2 (6.6) |
P. aeruginosa |
2 (6.5) |
NI* |
MRSA |
1 (3.2) |
NI* |
MRCoNS |
1 (3.2) |
2 (6.6) |
C. diversus |
1 (3.2) |
NI* |
Total (n) |
31 |
30 |
NI*: Not Isolated
The number of microorganisms isolated from In-born NICU before and after the cleaning was found to be 48 and 41, respectively. This observation was found to be statistically significant with p-value of 0.025 (Table 3). However, there was no significant difference in the isolation rate of pathogens from this NICU before and after cleaning (p = 0.385).
Table (3):
Number of bacteria isolated from Inborn NICU before and after cleaning
Number of Isolates |
Number of Pathogens |
|
|---|---|---|
Before Cleaning |
48 |
31 |
After Cleaning |
41* |
30† |
*Significant (p<0.05), †– Not Significant. Number of isolates before and after cleaning was compared.
Out-born NICU before cleaning
Of 50 samples collected from out-born NICU, 42 (84%) samples yielded growth and 8 (16%) samples did not yield any growth. 45 bacterial isolates were grown of which 25 (55.55%) were potential pathogens and 20 (44.44%) were non-pathogens.
Out-born NICU after cleaning
Of 50 samples collected from out-born NICU after routine cleaning, 42 (84%) samples yielded growth and 8 (16%) samples did not yield any growth. 43 bacterial isolates were grown of which 19 (44.18%) were potential pathogens and 24 (55.8%) were non-pathogens.
E. coli was the most prevalent isolate after cleaning, as against K. pneumoniae which was the most prevalent isolate from this unit before cleaning. A significant difference was not observed in the prevalence of potential pathogens before and after cleaning in the out-born NICU. Though there was no difference observed in the overall prevalence (84%) of microorganisms before and after cleaning in the Out-born NICU, K. pneumoniae was replaced by E. coli as the predominant organism after cleaning (Table 4).
Table (4):
Prevalence of pathogenic bacteria in Outborn NICU before and after cleaning
Potential Pathogens |
Before cleaning n (%) |
After cleaning n (%) |
|---|---|---|
NFGNB |
5 (20) |
3 (15.8) |
E. faecalis |
1 (4) |
3 (15.8) |
E. coli |
4 (16) |
5 (26.3) |
E. aerogenes |
NI* |
2 (10.5) |
K. pneumoniae |
8 (32) |
3 (15.8) |
Acinetobacter spp. |
2 (8) |
2 (10.5) |
P. aeruginosa |
3 (12) |
NI* |
MRSA |
NI* |
1 (5.3) |
MRCoNS |
1 (4) |
NI* |
C. diversus |
1 (4) |
NI* |
P. stutzeri |
NI* |
NI* |
Total (n) |
25 |
19 |
NI*: Not Isolated
When the overall frequency of isolation of potential pathogens in this study was considered, we observed that most frequent was K. pneumoniae closely followed by E. coli and NFGNB as compared to Staphylococci (Table 5).
Table (5):
Overall Frequency of isolation of pathogenic bacteria in this study (n= 105)
Pathogen |
Frequency of isolation n (%) |
|---|---|
NFGNB |
20 (19.4) |
E faecalis |
10 (9.52) |
E. coli |
20 (19.4) |
K. pneumoniae |
22 (20.95) |
E. aerogenes |
12 (11.43) |
Acinetobacter species |
8 (7.61) |
P. aeruginosa |
5 (4.76) |
MRSA |
2 (1.90) |
MRCoNS |
4 (3.80) |
C. diversus |
1 (0.95) |
P. stutzeri |
1 (0.95) |
The overall isolation rate of pathogens from both the NICUs considered together before and after cleaning was 60.21% (56 of 93) and 58.33% (49 of 84), respectively. This difference was statistically significant with a p-value of 0.007 (Table 6).
Table (6):
Overall Frequency of isolation of Pathogens from both the NICUs before and after cleaning
Number of Isolates |
Number of Pathogens n (%) |
|
|---|---|---|
Before Cleaning |
93 |
56 (60.21) |
After Cleaning |
84 |
49 (58.33)* |
* Significant (p < 0.05), number of pathogenic isolates before and after cleaning was compared
Antibiotic susceptibility testing
All the potentially pathogenic bacterial isolates were tested for their antibiotic susceptibility against a panel of antibiotics according to CLSI guidelines by the Kirby-Bauer disc diffusion method. Since the number of each potential pathogen was small, for interpretation and discussion of antibiogram, the probable pathogenic isolates were grouped into three broad groups (Table 7).
Table (7):
Grouping of pathogens isolated in this study
Group |
Isolates |
|---|---|
GNB |
E. coli, K. pneumoniae, E. aerogenes, C. diversus |
NFGNB |
NFGNB, Acinetobacter species, Pseudomonas species |
GPC |
MRSA, MRCoNS, E. faecalis |
Antibiotic resistance pattern of pathogens isolated in this study
All GNB isolates (100%) showed resistance to Ampicillin. The least resistance was shown towards Cefepime, Ceftazidime, Piperacillin/Tazobactam (1.8%). E. coli and K. pneumoniae isolates exhibited more resistance to antibiotics than the isolates of E. aerogenes. None of these was Extended Spectrum b-lactamase (ESBL producer) (Table 8).
Table (8):
Antibiotic resistance pattern of all Gram negative bacilli from fomites in both the NICUs
| Isolates (n) | Antibiotic Resistance Pattern n (%) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AMP | AT | AK | C | CTR | CTX | CPM | CAZ | CAC | CXM | PIT | IPM | GEN | CIP | COT | |
| E. coli (20) | 20 (100) | 8 (40) | 8 (40) | 10 (50) | 4 (20) | 2 (10) | 0 (0) | 5 (25) | 0 (0) | 1 (5) | 0 (0) | 0 (0) | 4 (20) | 0 (0) | 6 (30) |
| K. pneumoniae (22) | 22 (100) | 3 (13.6 | 1 (4.5) | 6 (27.2) | 6 (27.2) | 20 (90.9) | 0 (0) | 20 (90.9) | 0 (0) | 10 (45.4) | 0 (0) | 2 (9.1) | 7 (31.8) | 8 (36.36) | 6 (27.2) |
| E. aerogenes (12) | 12 (100) | 3 (25) | 2 (16.6) | 4 (33.3) | 2 (16.6) | 2 (16.6 | 0 (0) | 1 (8.3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 6 (50) | 6 (50) | 0 (0) |
| C. diversus (1) | 1 (100) | 1 (100) | 0 (0) | 0 (0) | 1 (100) | 1 (100) | 1 (100 | 1 (100) | 0 (0) | 1 (100) | 0 (0) | 0 (0) | 1 (100) | 0 (0) | 1 (100) |
AMP – Ampicillin, AT- Aztreonam, AK- Amikacin, C- Chloramphenicol, CTR- Ceftriaxone, CTX- Cefotaxime, CPM- Cefepime, CAZ- Ceftazidime, CAC- Ceftazidime/Clavulanic acid, CXM- Cefuroxime, PIT- Piperacillin/Tazobactum, IPM- Imipenem, GEN-Gentamycin, CIP- Ciprofloxacin, COT- Co-Trimoxazole (Trimethoprim/Suphamethoxazole)
We observed that all the isolates of S. aureus and CoNS were MRSA and MRCoNS. Overall highest resistance (83%) was shown against Amikacin (Table 9).
Table (9):
Antibiotic resistance pattern of all Gram Positive Cocci from fomites in both the NICUs
| Isolates (n) | Antibiotic Resistance Pattern n (%) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AK | E | P | CS | CIP | CX | NT | CD | LZ | TE | VA | LE | GEN | RIF | NIT | |
| MRSA (2) | 2 (100) | 1 (50) | 2 (100) | 2 (100) | 2 (100) | 2 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | NT | NT | 0 (0) | NT |
| MRCoNS (4) | 3 (75) | 2 (50) | 4 (100) | 2 (100) | 1 (25) | 4 (100) | 0 (0) | 0 (0) | 0 (0) | 2 (50) | 0 (0) | NT | NT | 0 (0) | NT |
| E. faecalis (10) | NT | 3 (30) | 2 (20) | NT | 4 (40) | NT | NT | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (10) | 0 (0) | NT | 1 (10) |
NT- Not tested, AK- Amikacin, E- Erythromycin, P- Penicillin, CS- Cefoperazone, CIP- Ciprofloxacin, CX- Cefoxitin, NT- Netillin, CD- Clindamycin, LZ- Linezolid, TE- Tetracycline, VA- Vancomycin, LE- Levofloxacin, GEN- Gentamycin, RIF- Rifampicin, NIT- Nitrofurantoin
In the case of NFGNB isolated in this study, the highest resistance (55.9%) was shown towards Gentamicin. None of the isolates showed resistance to Colistin (Table 10).
Table (10):
Antibiotic resistance pattern of Pseudomonas spp., Acinetobacter spp. and NFGNB Isolated from fomites in both the NICUs
| Isolates (n) | Antibiotic Resistance pattern n (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AT | AK | CL | LE | CPM | CAZ | CAC | PIT | IPM | GEN | CIP | COT | |
| Acinetobacter spp (8) | 1 (12.5) | 2 (25) | 0 (0) | 3 (37.5) | 4 (50) | 7 (87.5) | 0 (0) | 2 (25) | 0 (0) | 4 (50) | 3 (37.5) | 1 (12.5) |
| NFGNB (20) | 5 (25) | 6 (30) | 1 (5) | 6 (30) | 3 (15) | 5 (25) | 4 (20) | 3 (15) | 9 (40) | 11 (55) | 9 (45) | 12 (60) |
| P. aeruginosa (5) | 2 (40) | 4 (80) | 0 (0) | 2 (40) | 4 (80) | 3 (60) | 2 (40) | 2 (40) | 1 (20) | 3 (60) | 2 (40) | 2 (40) |
| P. stutzeri (1) | 1 (100) | 1 (100) | 0 (100) | 1(100) | 0 (0) | 1 (100) | 0 (0) | 0 (0) | 0 (0) | 1 (100) | 1 (100) | 1 (100) |
AT- Aztreonam, AK- Amikacin, CL- Colistin, LE- levofloxacin, CPM- Cefepime, CAZ- Ceftazidime, CAC- Ceftazidime/Clavulanic acid, PIT- Piperacillin/Tazobactum, IPM- Imipenem, GEN-Gentamycin, CIP- Ciprofloxacin, COT- Co-Trimoxazole(Trimethoprim/Suphamethoxazole)
The present study showed that the fomites sampled in our NICUs were harboring both potentially pathogenic and non-pathogenic microorganisms. These fomites are most frequently touched by healthcare personnel and also a few fomites such as bed linen frequently come in contact with neonates. However, determining the evidence of the role of these fomites in the transmission of the pathogens to neonates thereby causing infection was beyond the scope of this study. The incidence of potential pathogens like K. pneumoniae, E. coli, E. aerogenes, P. aeruginosa, P. stutzeri, C. diversus, NFGNB, Acinetobacter and gram-positive cocci such as MRSA, MRCoNS and E. faecalis was reported in our study. These contaminated fomites may act as sources of infection and thereby a cause for concern. Molds or Candida species were not isolated from any fomite in our study. Contamination of fomites with pathogenic microorganisms is a universal problem. Kiros et al. in an extensive review noted that the overall prevalence of bacterial contamination of fomites was found to be 70%. They also observed that the degree of contamination and the frequency of isolation of pathogenic microorganisms were governed by various factors.11
The frequency of overall isolation of bacteria (both pathogenic and non-pathogenic) from in-born NICU before and after the cleaning was significant (p= 0.025). Importantly, there was a significant decrease in the overall prevalence of pathogens after cleaning when both the NICUs were considered together (p= 0.007). This observation indicates that practicing proper infection control protocol would bring down the prevalence of pathogens in the critical hospital environment. Hewitt et al. utilized molecular methods to determine the diverse bacterial presence in a variety of fomites from two NICUs and reported the presence of potential pathogens like Acinetobacter, Pseudomonas species, a few members of family Enterobacteriaceae and also MRSA, MRCoNS along with other skin colonizers.16 However, Dramowski et al. noted the high prevalence of isolation of potential pathogens like S. aureus (9%), K. pneumoniae (9%), Serratia marcescens (12.8%) and Acinetobacter species (7.7%) from fomites such as sinks, humidifiers and suction pumps.9 In accordance with this, in our study also K. pneumoniae (20.95%) was the most prevalent organism, closely followed by NFGNB and E. coli (19%) in contrast, the present study showed a low frequency of isolation of MRSA (1.9%) and MRCoNS (3.8%).
Kanamori et al. in their review reported that contaminated fomites such as humidifiers, rectal thermometers, breastfeeding pumps, oxygen saturation probes, hand soap/sanitizer dispensers, stethoscopes, etc. were responsible for hospital-acquired infections (HAIs) in neonates. They reported that pathogens such as K. pneumoniae, E. aerogenes, P. aeruginosa, NFGNB, MRSA, MRCoNS, E. faecalis were the most frequent isolates from HAIs of neonates. They also noted that inappropriate disinfection practices led to HAIs.4
Shi et al. noted the presence of clinical isolates of ESBL producing K. pneumoniae from neonates in contrast to environmental isolates that did not carry genes for antibiotic resistance and other virulence factors. However, they opined that the environmental prevalence of K. pneumoniae should be considered seriously assuming its pathogenicity in humans.10
Osman et al. in their extensive review observed that Staphylococcus was the most frequent isolate. They also noted the high prevalence of E. coli, K. pneumoniae, A. baumannii, Enterococcus species, Enterobacter species, Candida species and multi-drug-resistant pathogens such as MRSA, VRE, ESBL producers. Of all the fomites tested, sphygmomanometer showed a 100% detection rate of nosocomial pathogens. They noted that NICUs had the highest rate of contaminated fomites as compared to other areas of the hospitals. NICU isolates included Enterobacter aerogenes, CoNS, S. aureus, E. coli and K. pneumoniae.6
We observed that all GNB isolates were resistant to Ampicillin. Resistance to Cefotaxime was exhibited by 45.5% of isolates. Though the isolates of E. coli and K. pneumoniae exhibited more resistance to antibiotics than the isolates of E. aerogenes, none of the GNB isolates was an ESBL producer. In the case of S. aureus and CoNS, all the isolates were found to be MRSA and MRCoNS. Two (40%) of the isolates of P. aeruginosa were ESBL producers. Acinetobacter and other NFGNB including Pseudomonas species are known to survive in the adverse hospital environment. Our study revealed a low frequency of isolation of Acinetobacter spp., and Pseudomonas spp. These isolates were highly resistant to Amikacin, Ceftazidime, Cefepime, and Gentamycin. The high degree of resistance, exhibited by nosocomial pathogens, enables them to sustain adverse hospital environment and aid in causing healthcare-associated infections.
The limitation of this study was that, we did not correlate the isolates from our study with the clinical isolates from neonates during the study period.
The overall isolation rate of microorganisms in the present study was significant. A noteworthy observation was that a significant decrease in the frequency of isolation of potential pathogens was seen after cleaning in both the NICUs when considered together. This baseline data would help us to further strengthen the stringent measures of surface cleaning, hand hygiene, and education of health care personnel.
ACKNOWLEDGMENTS
The authors would like to acknowledge ICMR-STS team as this research paper is based on ICMR-STS project work. Authors also acknowledge the support of NICU staff, faculty and technical staff of the Department of Microbiology for their support.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved the final version for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Shri Dharmasthala Manjunateshwara College of Medical Sciences and Hospital, Karnataka, India, with reference No. 03172015.
- Stephens B, Azimi P, Thoemmes MS, Heidarinejad M, Allen JG, Gilbert JA. Microbial Exchange via Fomites and Implications for Human Health. Curr Pollut Rep. 2019;5(4):198-213.
Crossref - Bhatta DR, Subramanya SH, Hamal D, et al. Bacterial contamination of neonatal intensive care units: How safe are the neonates? Antimicrob Resist Infect Control. 2021;10(1):26.
Crossref - Kamgaing EK, Ndong JC, Rerambiah LK, Siawaya JFT. Profiles of microorganisms isolated from neonates’ blood cultures, incubators, cradles, ventilators, washbasins, and health-workers of Libreville University Hospital Neonatal Service: focus on infection prevention and control measures. J Public Health Afr. 2021;12(1):1075.
Crossref - Kanamori H, Rutala WA, Weber DJ. The Role of Patient Care Items as a Fomite in Healthcare-Associated Outbreaks and Infection Prevention. Clin Infect Dis. 2017;65(8):1412-1419.
Crossref - Olsen M, Nassar R, Senok A, et al. Mobile phones are hazardous microbial platforms warranting robust public health and biosecurity protocols. Sci Rep. 2022;12(1):10009.
Crossref - Osman AH, Darkwah S, Kotey FCN, et al. Reservoirs of Nosocomial Pathogens in Intensive Care Units: A Systematic Review. Environ Health Insights. 2024;18:11786302241243239.
Crossref - Kovacs D, Silago V, Msanga DR, et al. The hospital environment versus carriage: transmission pathways for third-generation cephalosporin-resistant bacteria in blood in neonates in a low-resource country healthcare setting. Sci Rep. 2022;12(1):8347.
Crossref - Shimoda T, Okubo T, Enoeda Y, et al. Effect of thermal control of dry fomites on regulating the survival of human pathogenic bacteria responsible for nosocomial infections. PLoS One. 2019;14(12):e0226952.
Crossref - Dramowski A, Aucamp M, Bekker A, et al. NeoCLEAN: a multimodal strategy to enhance environmental cleaning in a resource-limited neonatal unit. Antimicrob Resist Infect Control. 2021;10(1):35.
Crossref - Shi Q, Zhao J, Wei Le, et al. Transmission of ST45 and ST2407 extended-spectrum b-lactamase-producing Klebsiella pneumoniae in neonatal intensive care units, associated with contaminated environments. J Glob Antimicrob Resist. 2022;31:309-315.
Crossref - Kiros T, Damtie S, Eyayu T, Tiruneh T, Hailemichael W, Workineh L. Bacterial Pathogens and Their Antimicrobial Resistance Patterns of Inanimate Surfaces and Equipment in Ethiopia: A Systematic Review and Meta-analysis. Biomed Res Int. 2021;2021:5519847.
Crossref - Detection and enumeration of bacteria in swabs and other environmental samples. National Infection Service Food Water and Environmental Microbiology Standard Method Document. Number FNES4 Version number 4. 2017. Public Health England 133-155. http://www.hpa.org.uk/ProductsServices/Microbiolo gyPathology/SpecialistMicrobiologyServices/FoodWa terEnvironmentalMicrobiologyServices/NationalRefe renceLaboratoryForFoodMicrobiology Accessed 20 May 2023.
- Tille PM, Bailey and Scott’s Diagnostic Microbiology, 13th Ed:193-231; Elsevier Inc;2013.
- CLSI. Performance standards for antimicrobial susceptibility testing. Twentieth Information Supplement 201;30(1):M100-S20. Wayne, PA: Clinical and Laboratory Standards Institute. Accessed 5 January 2023.
- CLSI. Performance standards for antimicrobial susceptibility testing. Seventeenth Information Supplement M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute, 2007. Accessed 30 December 2022.
- Hewit KM, Mannino FL, Gonzalez A, et al. Bacterial diversity in two Neonatal Intensive Care Units (NICUs). PLoS One. 2013;8(1):e54703.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.