


Bacterial biofilms, structured communities of microorganisms enmeshed in an extracellular matrix, have emerged as significant players in various pathological processes. Renal calculi, commonly known as kidney stones, pose a prevalent medical concern, and recent research has highlighted the potential influence of bacterial biofilms in their formation and persistence. This review explores the development of biofilms on the surface of urinary tract stones and how they create a favorable environment for the colonization of bacteria. This colonization, in turn, can lead to chronic infections, stone enlargement, and recurrent stone formation. This review offers a comprehensive exploration of the dynamic interplay between bacterial biofilms and renal calculi. It emphasizes the role of biofilm-related mechanisms in chronic infections, inflammation, and mineral deposition, underscoring the potential for innovative therapeutic strategies aimed at managing and preventing biofilm-associated renal calculi.
Renal Calculi, Biofilm, Biofilm-producing Bacteria, Nephrolithiasis
In recent years, the study of bacterial biofilms and their role in various medical conditions has garnered significant attention within the field of life sciences.1,2 Bacterial biofilms, complex and dynamic microbial communities enclosed within a self-produced extracellular matrix, are widespread in nature and frequently exert a pivotal role in various processes, including disease pathogenesis.1 These biofilms can form on a broad spectrum of surfaces, including medical devices, industrial equipment, natural environments, and even within the human body. This review will discuss the bacterial biofilms in the renal calculi.
Renal calculi, more commonly referred to as kidney stones, are solid masses composed of crystals that typically originate within the kidneys. These stones vary in size and composition and can cause significant discomfort and medical complications.3 Kidney stones represent a prevalent urological problem that can affect people of all ages, and their formation is influenced by various factors.4 The term renal calculus is described as a solid and pebble-like structure that forms in one or both sides of the kidneys. The chemical constituents concentrate to form crystals and this condition leads to the development of renal stones.5 This condition is also known as nephrolithiasis, urolithiasis, urinary calculi, or renal calculi and its prevalence rate is increasing.6 The worldwide incidence of kidney stones exhibits significant variations across different regions.7,8 It can affect individuals of all ages, genders, and racial backgrounds but this exhibits a greater occurrence in males, ranging from 10% to 20%, in contrast to females, whose prevalence ranges from 3% to 5%. Notably, prevalence rates vary across different regions. For instance, in Asia, reported rates are approximately 1% to 5%, while in Europe, they range from 5% to 9%, and in North America, the range is 7% to 15%. It is noteworthy that Saudi Arabia deviates from these patterns, displaying an exceptionally elevated prevalence, where nearly 20% of its population suffers from kidney stones. Conversely, China presents a considerably lower incidence of kidney stones, affecting only around 4% of its population.8,9 These disparities highlight the influence of geographical and possibly genetic factors on the kidney stones prevalence in distinct populations. The available global data indicate a notable rise in the prevalence of kidney stones among individuals of all genders during the final 25 years of the twentieth century.8,10,11 While the pathogenesis of renal calculi has traditionally been attributed to physicochemical processes, emerging research suggests that bacterial biofilms may exert a significant influence on stone formation and growth. A comprehensive investigation was carried out on a sample of 10,663 individuals to investigate the prevalence and risk factors linked to kidney stones. The results of this study uncovered several factors contributing to the formation of kidney stones, including middle age, male gender, overweight status, higher socioeconomic status, and other factors.8
The association between bacterial biofilms and renal calculi stems from their capacity to serve as niduses, providing a surface for crystal nucleation and subsequent growth. These biofilms can form on the surfaces of existing calculi or within the renal papillae, where they create a conducive environment for crystal adherence.12 The formation of a kidney stone is the result of the interaction between pathogens that cause infection and mineral components obtained from urine.13 The examination of kidney stones obtained from persons with infections at a microscopic level has provided insights into the characteristics of bacterial biofilms. The bacterial cells present both on the external and inside kidney stones have a distinct organization in the form of micro-colonies, which are enveloped by a matrix composed of crystalline substances, specifically struvite.5,14,15
Numerous bacterial species have been implicated in the development of biofilms that are linked to the production of renal calculi. One of the noteworthy organisms in this group is Proteus mirabilis, which stands out for its capacity to synthesize the urease enzyme. This enzyme facilitates ammonia and carbon dioxide by hydrolysis of urea, resulting in the creation of an alkaline environment that fosters the precipitation of crystals.12,16-18 Other bacteria frequently found in urinary tract infections, such as Escherichia coli.18 Understanding the mechanisms underlying the interplay between bacterial biofilms and renal calculi formation has important implications for clinical management.19
In total, the intricate relationship between bacterial biofilms and renal calculi highlights the importance of gaining a thorough comprehension of their role in stone formation and associated infections. Further research into the specific interactions, molecular mechanisms, and potential therapeutic interventions is essential for advancing our knowledge in this field. As our understanding deepens, new avenues for targeted treatments and preventive strategies may emerge, offering potential benefits for individuals at risk of renal calculi and related complications. This review aims to delve into the intricate relationship between bacterial biofilms and renal calculi, shedding light on the underlying mechanisms, contributing factors, and potential implications for clinical management.
Formation of Renal Calculi
The formation of renal calculi, or kidney stones, is a complex process influenced by various factors, including urine composition, genetics, lifestyle, and medical conditions.3 Kidney stones typically develop when certain substances in the urine crystallize and aggregate, forming solid masses within the kidneys.5 Kidney stone formation often begins with the supersaturation of urine. This takes place when the concentration of certain minerals or salts in the urine exceeds their solubility limit, leading to the precipitation of crystals.20 The most common minerals associated with the formation of kidney stones include calcium, oxalate, uric acid, and cystine, 9%, 10%, and 1% of stones.20-22 Supersaturated urine provides the ideal environment for crystals to form.23 Nucleation is the initial step where tiny crystals, called nuclei, start to form around small particles present in the urine. These particles can include proteins, cellular debris, or even existing crystals. Once nuclei are formed, they serve as sites for further crystal growth.15 The growing crystals aggregate and form larger structures. The specific type of crystal that forms depends on the composition of the supersaturated urine and other factors like pH and temperature. As crystals grow, they can become embedded within an organic matrix, which includes substances like proteins and glycoproteins. This matrix can help bind the crystals together and form a solid stone. The kidneys have mechanisms to regulate crystal formation. Certain substances, like citrate and magnesium, help prevent crystal aggregation by binding to crystals and preventing their growth. Factors that promote crystal formation, such as elevated levels of calcium or oxalate in the urine, can intensify the process.5,24 Urine pH plays a crucial role in kidney stone formation. Different types of stones tend to form under specific pH conditions. For instance, acidic urine encourages the formation of uric acid stones, while alkaline urine supports the development of calcium phosphate stones. Adequate urine flow helps flush out crystals and prevent their aggregation. Stagnation or reduced urine flow can allow crystals to accumulate and aggregate, increasing the risk of stone formation. Genetic predisposition can influence an individual’s susceptibility to kidney stones.25 Additionally, dietary choices,21 hydration status,26 and medical conditions like obesity, diabetes, and certain metabolic disorders27 can impact urine composition and elevate the risk of stone formation. Certain medical conditions, such as hyperparathyroidism (increased levels of parathyroid hormone), gout (elevated uric acid levels), and urinary tract infections, can alter urine composition and promote crystal formation.28,29 In summary, the formation of renal calculi involves a sequence of events starting with supersaturation of urine, nucleation of crystals, their growth and aggregation, matrix formation, and potential crystal inhibitors and promoters. Understanding these processes is essential for developing strategies to prevent and manage kidney stone formation, which can have significant implications for patients’ health and well-being (Figure 1).
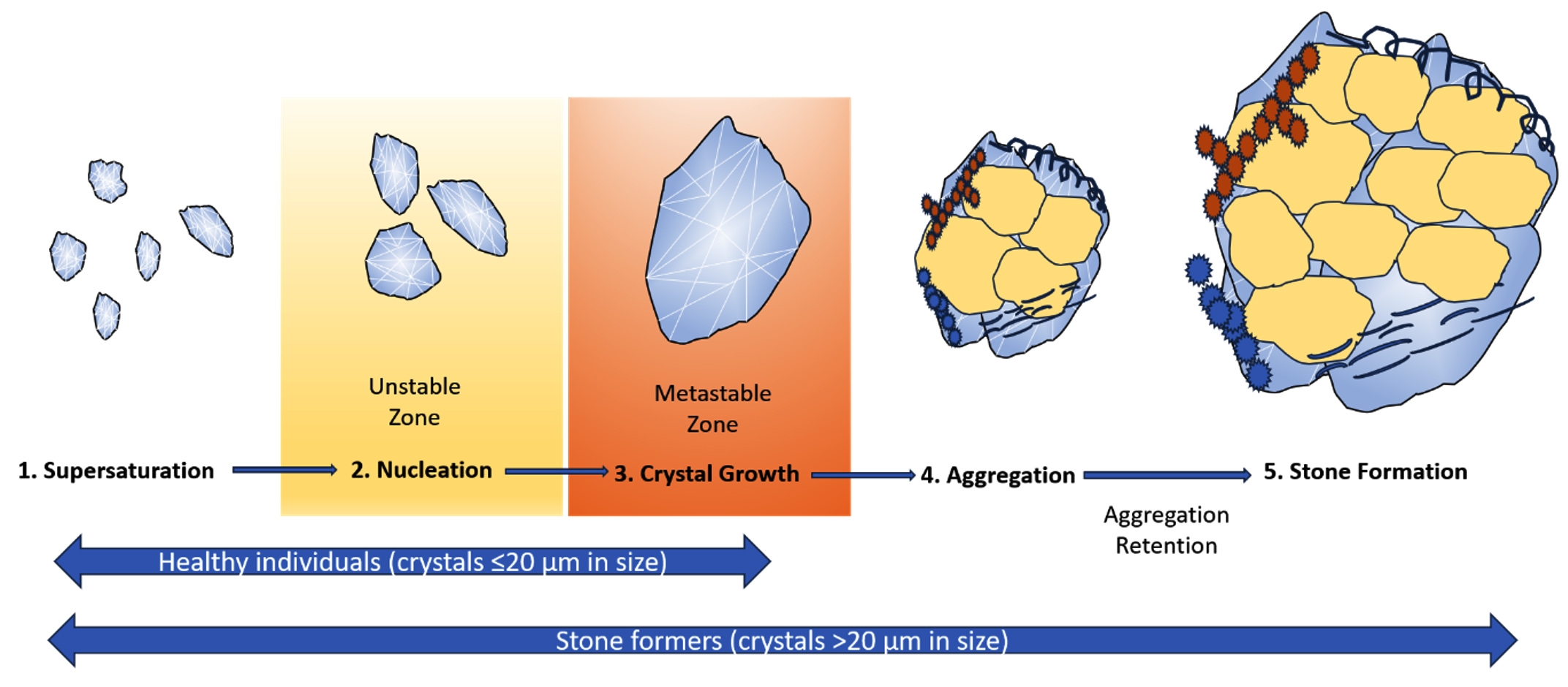
Figure 1. The formation of stones through crystalline growth in the physicochemical process. Supersaturation is when solutes exceed their solubility limit in a solution, a key factor for the formation of stone (Step 1). Nucleation, where solutes cluster into microscopic particles, happens either homogeneously (extremely high supersaturation, ‘unstable zone’) or heterogeneously (lower supersaturation, ‘metastable zone’ with a surface requirement) (Step 2). Crystal growth follows the formation of a critical nucleus when exposed to highly concentrated urine (in the ‘metastable zone’), permitting the migration of ions from the solution. (Step 3). Aggregation leads to larger particles embedded in organic macromolecules, forming the stone matrix (proteins, carbohydrates, glycosaminoglycans, lipids). Crystal growth also occurs in non-stone formers, with smaller crystals (≤20 µm) passing through the urinary tract. Particles >20 µm may cause obstruction, pain, or infections (step 4)
Association between bacterial biofilms of urinary tract and Renal Calculi
Bacterial biofilms within renal calculi have garnered significant attention due to their potential role in recurrent renal calculi infections. Bacterial biofilms can form within the core of renal calculi, which are solid mineral deposits that develop within the urinary tract of the kidney.17 The process begins with bacterial attachment to the stone surface, followed by the accumulation of bacterial cells. As these bacteria multiply and produce EPS, a protective matrix forms around them, giving rise to a mature biofilm structure within the stone’s interior.30 Renal calculi containing bacterial biofilms exhibit distinctive characteristics. The biofilm matrix is comprised of EPS, proteins, polysaccharides, and nucleic acids, which collectively contribute to the biofilm’s structural integrity. The matrix serves a dual purpose by not only providing protection for bacteria against host immune responses but also by impeding the efficacy of antibiotics through the establishment of a physical barrier.30 The compact structure of the biofilm confers increased resilience to antibacterial interventions. Bacterial biofilms within renal calculi are closely linked to recurrent renal calculi infections. A retrospective study on 1325 patients revealed that 28% of UTI-infected patients developed kidney stones.31 A comprehensive nationwide investigation conducted in Taiwan reported that among 1679 pediatric individuals newly diagnosed with urolithiasis, UTI emerged as the predominant correlated ailment, affecting 34.1% of the entire subject cohort.32A comprehensive investigation conducted in Pakistan revealed that out of 100 patients with UTI, 18.98% developed kidney stones.33 In 1679 patients more than 18 years old with kidney stones and UTI revealed that UTI is the most prevalent condition associated with kidney stones, occurring in 34.1% of cases.32 A study conducted on 599 patients with UTI revealed that stone size was identified as a risk factor for UTI in individuals with kidney stones.34,35 These UTI biofilms can serve as reservoirs for pathogenic bacteria, contributing to persistent infections and treatment resistance. A Retrospective study in Japan showed UTI infection is more likely to have kidney stones in 286 patients infected with UTI caused by S. aureus.36 In a recent systematic review comprising 17 papers, a robust connection between kidney stones and UTI was established, indicating that UTI and kidney stones often coexist.37 The presence of biofilms within calculi complicates treatment approaches, as the bacteria encased in the biofilm display reduced susceptibility to antibiotics and can readily evade the immune system’s defenses. Biofilm-associated infections in renal calculi are perpetuated by several mechanisms. The protective biofilm matrix shields bacteria from immune cells and antibiotics.38 Additionally, bacteria within biofilms can enter a dormant state, rendering them less susceptible to conventional treatments. These factors collectively contribute to the chronic nature of infections associated with biofilm-containing renal calculi.
Microorganisms in Renal Calculi
Certainly, examining the various microorganisms commonly found in renal stones and their roles in stone pathogenesis provides valuable insights into the complex interplay between microbial communities and kidney stone formation. UTI is the result of the bacterial ability to adhere and colonize the urethra, perineum, bladder, gut, renal pelvis, and renal interstitium (intertubular, extraglomerular, and extravascular space of kidney). Prospective research was conducted to analyze 100 patients who were hospitalized for the removal of kidney stones in Thailand. The investigation identified the presence of Klebsiella spp, E. coli, and P. mirabilis in the stones.39 In a study of renal calculi from the southern part of India, out of the 42 infected renal calculi, E. coli was isolated from 16 stones, Pseudomonas spp. from 14, Proteus spp. from 5, Klebsiella spp. from 4, Enterococci spp. from 2, and Coagulase-negative Staphylococcus from a single stone were detected to form biofilms and sensitive against most of the antibiotics.40 The conventional microbiological examination of kidney stones extracted from a sample of 200 patients revealed an infection in 51% (103) of the stones. The highest number of bacteria present were Proteus mirabilis and Escherichia coli. Staphylococcus haemolyticus, Pseudomonas aeruginosa, Klebsiella pneumoniae, Enterococcus faecalis, Staphylococcus aureus, and Acinetobacter baumannii. In which Staphylococcus aureus, Klebsiella pneumonia, Proteus mirabilis, Pseudomonas aeruginosa, and Acinetobacter baumannii exhibited urease activity. These might contribute to stone growth and retention.41 P. mirabilis exhibits the capacity to generate intracellular crystals within epithelial host cells, therefore evading the effects of antibiotics and immunological responses. This phenomenon contributes to the development of chronic and recurring infections, which may be identified by the utilization of an in vitro model.42 A Retrospective study in Japan showed UTI infection is more likely to cause kidney stones in 286 patients infected with S. aureus.36 Urease, an enzyme that hydrolyses urea into ammonia and carbon dioxide. This increased level of ammonia leads to an alkaline environment, promoting the development of struvite stones. Fungal species have also been detected in kidney stones. These include species like Candida and Aspergillus. Fungi might interact with bacteria and impact stone formation through various mechanisms, such as altering the urinary pH and promoting biofilm formation. Fungal involvement in renal calculi formation is an emerging area of research, shedding light on the complex interplay between microbial communities and stone development. Amplicon gene sequencing identified the presence of fungi in 11 out of 20 fragment groups of kidney stones from the patients. In which Aspergillus and Candida are preserved within CaOx, CaHPO4, and struvite stone.43 In a separate investigation on the filtration of urate and oxalate renal stones, the identification of micromycetes on the nutritional medium revealed a random distribution, resulting in a minimal quantity of fungal colonies.44,45 A study overlooked the kidney stone for the fungal presence by using Fourier transform infrared spectroscopy. A distinct investigation using 21 distinct samples of renal stones with varying compositions found a minimal presence of fungal colonies. The phosphate renal stones exhibited a significant expansion of fungal and bacterial colonies.44 In a study of urinary calculi complicated with UTI, detected 29.41% of fungus species out of 407 strains of microbial species. In which Candida glabrata, Candida tropicalis, Candida parapsilosis, Monilia albicans, and Meyerozyma guilliermondii were there.46
Roles of microorganisms in stone pathogenesis
Crystal nucleation and growth
Microorganisms can profoundly impact kidney stone development by participating in crystal nucleation and subsequent growth. The urinary tract environment, replete with ions and molecules conducive to mineral precipitation, provides a suitable setting for crystal formation. This interaction potentially leads to the accumulation of these ions in the proximity of bacterial cells, consequently expediting the crystallization process.47 Microorganisms, particularly those endowed with urease-producing capabilities, contribute significantly to this process. An artificial laboratory model was employed to investigate the growth within cells and the process of crystallization when exposed to bacterial strains such as P. mirabilis, Klebsiella pneumoniae, and Escherichia coli.42 Urease-positive bacteria will generate ammonium and raise the level of pH of the surrounding milieu. This alkaline environment promotes the formation of crystals, particularly struvite and carbonate apatite, which are frequently linked with infection-related stones. In patients with metabolic syndrome, urea excretion via urine is reduced. Therefore, in these patients, the alkalinity of urine will increase and they are highly susceptible to developing struvite stones.48 The mineral components of stones, such as calcium phosphate and calcium oxalate, can adsorb onto microbial surfaces. The microorganisms serve as nucleation sites for these crystals, aiding in their growth.
Biofilm formation
Urinary tract infection (UTI) arises from the remarkable bacterial capacity to adhere to and colonize various regions including the urethra, perineum, bladder, gut, renal pelvis, and the intricate renal interstitium, encompassing the intertubular, extraglomerular, and extravascular spaces within the kidney’s structure.49 Specifically, uropathogens affiliated with the Enterobacterales order exhibit electronegativity and possess a minute charge, enabling them to navigate the repulsion induced by epithelial cells owing to their negative charge.50 A significant facet in the development of infectious struvite stones involves the biofilm formation orchestrated by ureolytic bacteria within the urinary tract. Ureolytic organisms, which possess urease enzymes, break down urea to produce ammonium, leading to a rise in urine alkalinity and promoting the development of struvite stones. The process of biofilm formation and struvite biomineralization can be divided into several sequential stages which is illustrated in Figure 2.
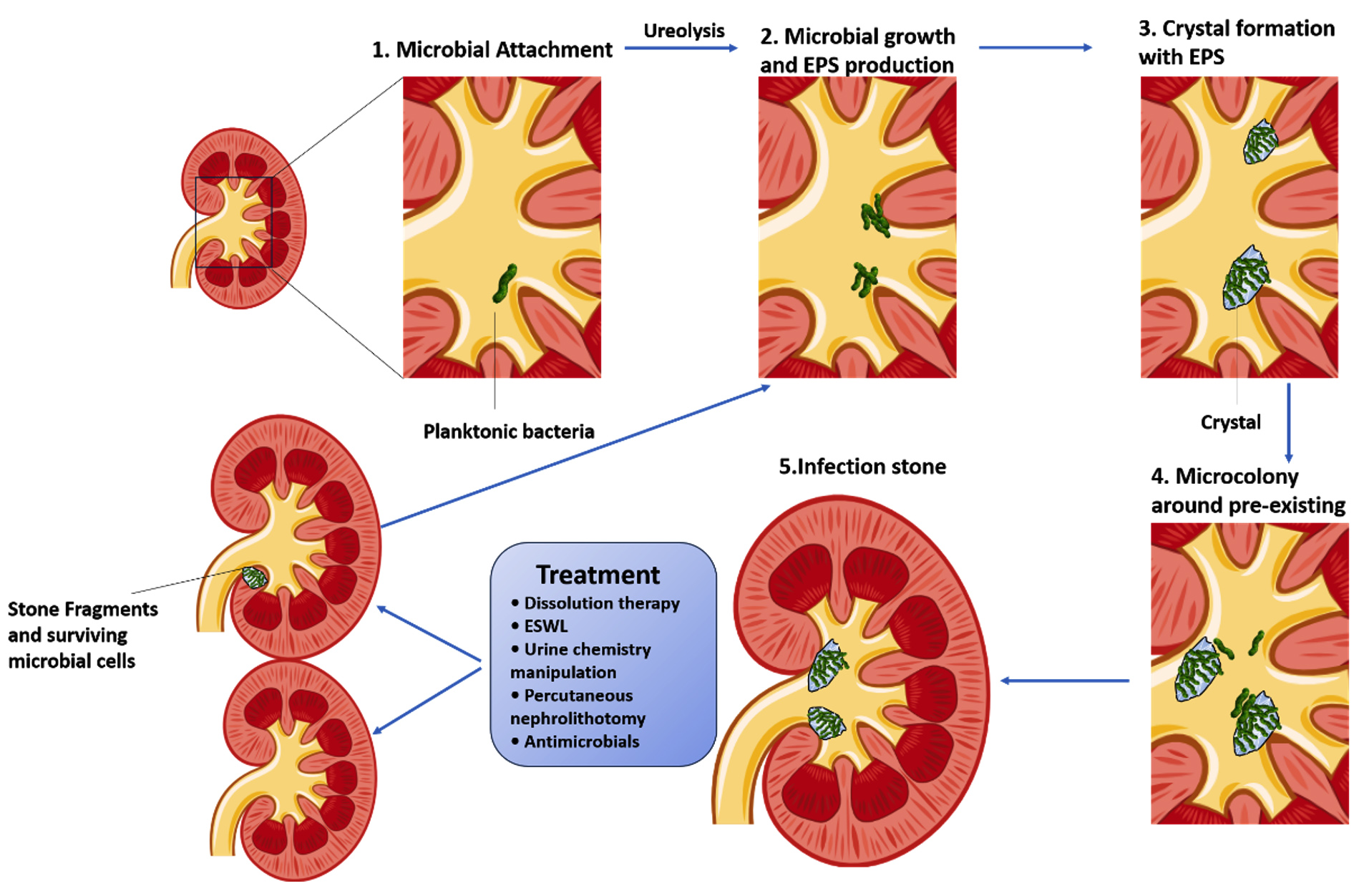
Figure 2. Microorganisms and biofilms association in the formation of renal calculi Initially, a thin layer of urinary constituents, such as ions, proteins, and polysaccharides, adheres to surfaces within the urinary tracts, creating a foundation for the planktonic microorganism’s attachment. This process involves ureolysis, which raises urine pH and generates ammonium ions (NH4+) in (step 1). Subsequently, microbial microcolonies emerge, and EPS is produced. (Step 2) involves an increased level of pH, NH4+ concentration, and carbonate ions (CO32-), which will lead to microcrystal formation. NH4+ reacts with Mg2+ and PO43- ions to form struvite, while CO32- combines with Ca2+ and PO43- ions to create carbapatite. In (step 3), crystals emerge within the EPS matrix and on the surface of the biofilm, potentially causing microbial detachment into the urinary tract. (Step 4) encompasses the growth of crystals and secondary nucleation occurring within the EPS matrix, with planktonic bacteria adhering to crystals and forming microcolonies within biofilm-driven crystal structures. These processes are repeated, resulting in the integration of crystals into the biofilm, and ultimately culminating in the development of infectious stones. After treatment, stone fragments or viable cells might endure in the urinary tract, possibly leading to recurring infections, continued biofilm growth, and additional biomineralization (step 5). One potential treatment option is extracorporeal shock wave lithotripsy (ESWL)
Inflammation and stone formation
Microbes, particularly those possessing urease-producing capabilities, can instigate inflammation within the urinary tract.51 The interaction between these crystals and the uroepithelium can initiate an immune response characterized by the inflammatory cytokines and chemokines release.52 The immune response triggered by microbial presence and crystal formation involves the recruitment of immune cells such as neutrophils and macrophages to the site of infection. These immune cells release various inflammatory mediators that contribute to tissue damage and inflammation. In particular, the discharge of reactive oxygen species (ROS) and pro-inflammatory cytokines can lead to oxidative stress and further tissue injury.52,53 Chronic inflammation in the urinary tract can have several consequences that promote kidney stone formation.37 Inflammation can disrupt the uroepithelial barrier, allowing crystals and bacteria to penetrate deeper into the tissues. Additionally, inflammation-induced tissue damage can lead to the release of cellular debris, which can act as nucleation sites for crystal formation. The persistent presence of microbes and crystals can perpetuate the inflammatory response, creating a vicious cycle that exacerbates tissue damage and stone formation.54
Recurrent infections
The presence of kidney stones and associated biofilms provides a protected environment where microbes can evade host immune defences and antimicrobial treatments. Biofilms, composed of bacterial cells embedded in an extracellular matrix, create a physical barrier that hinders the immune cells’ penetration and antibiotics. This protective environment enables the microbes to persist and potentially cause recurrent infections. Moreover, the chronic inflammation induced by microbial presence and stone formation can contribute to the cycle of recurrent infections. Inflammation disrupts the uroepithelial barrier and can lead to tissue damage, providing additional sites for microbial attachment and biofilm formation.55 The ongoing immune response, characterized by the release of inflammatory mediators, can create an environment conducive to microbial persistence. The presence of bacteria in a protected biofilm state makes them less susceptible to antibiotic treatments.26,53,37
Stone composition
Microbial biofilms, characterized by the presence of microorganisms enclosed within their self-generated extracellular matrix, have the potential to act as a focal point for the initiation and development of crystal formation. The biofilm matrix composition, in conjunction with the bacteria’s interactions with the urinary environment, can impact the crystalline formations that develop inside the biofilm. A hypothesis has been put forth suggesting that the bacterial polysaccharides found within the Proteus genus, which encompass macromolecules containing negatively charged residues, possess the capability to bind with Ca2+ and Mg2+ ions. This interaction potentially leads to the accumulation of these ions in the proximity of bacterial cells, consequently expediting the crystallization process.42,47 Struvite stones frequently exhibit an association with urinary tract infections and are frequently observed in persons who suffer from persistent infections. Likewise, the elevation in pH levels caused by the enzymatic action of microorganisms on urea might also facilitate the development of carbonate apatite stones.11 These stones are primarily made up of calcium phosphate and are frequently observed in the presence of urease-positive bacteria. In some cases, stones can be composed of a mixture of different minerals. For instance, infection-related stones may exhibit a combination of struvite, carbonate apatite, and other components.14 The biofilm’s matrix and the urinary environment contribute to the formation of these mixed stones. Table shows the type and stones and related microbial species infection.
Table:
Varieties of stones and infections attributed to associated microbial species
| Types of stones and infections caused by related microbial species. | Stone Type | Patients Number | Infected stones | Microbial Type | Ref. |
|---|---|---|---|---|---|
| Struvite; calcium oxalate; brushite | 86 | 76% | • (60%) monoculture • (40%) mixed culture • E.coli • Pseudomonas spp. • Proteus mirabilis • Klebsiella spp. • Pseudomonas spp. • Staphylococcus spp. • Yeast |
58 | |
| Calcium oxalate; struvite | 100 | 36 | • (33%) E. coli (33%) • (7%) P. mirabilis • (3.7%) Pseudomonas aeruginosa • (3.7) Citrobacter freundii • (11%) Klebsiella spp. • (3%) Klebsiella pneumoniae |
59 | |
| Calcium oxalate; struvite | 63 | 38% | • P. mirabilis (7% calcium oxalate; 86% struvite) • E.coli (53% calcium oxalate; 50% struvite) |
60 | |
| Non-struvite | 132 | 24 | • (31.3%) E. coli • (28.1%) P. aeruginosa • (9.4%) P. mirabilis • (9.4%) Klebsiella pneumoniae • (6.3%) Enterobacter spp. • (3.1%) Serratia marcescens • (3.1%) Staphylococcus cohnii • (3.1%) Candida albicans • (3.1%) Citrobacter spp. |
61 | |
| Calcium oxalate (mixed) | 5 | 5 | • (80%) Gardnerella spp. • (100%) Pseudomonas spp. • (80%) Enterobacteria |
62 | |
| Mixed stones | 25 | 25 | • E. coli • Shigella spp. • Klebsiella spp. • Enterococcaceae • Proteus Sphingomonas, |
63 | |
| Ca phosphate and struvite crystals | 177 | 175 | • E. coli • Klebsiella pneumoniae • Klebsiella oxytoca |
64 |
Diagnostic techniques for biofilms in Renal Calculi
Detecting biofilms in renal calculi is essential for understanding the microbial component of stone formation and developing effective treatment strategies. Despite extensive research spanning several decades, there is a significant knowledge gap about the underlying processes responsible for the development of infection stones. A comprehensive comprehension of the molecular processes involved in the genesis and progression of renal calculi, as well as the role of biofilms in the formation of stones and the subsequent medical ramifications of these findings, might prove to be of utmost importance in the advancement of enhanced therapeutic interventions. The use of tools and methodologies in diverse fields such as chemistry, engineering, mineralogy, and microbiology can be employed to enhance comprehension of the interactions between microorganisms that contribute to the development of biofilms. Here are some of the diagnostic methods commonly employed for renal calculi biofilms research and understanding:
Microscopy techniques
Scanning Electron Microscopy (SEM) provides high-resolution images of the surface of renal stones, allowing visualization of biofilm structures and microorganisms. It offers detailed morphological information and can identify the presence of biofilms on the stone’s surface. Confocal Laser Scanning Microscopy (CLSM): CLSM is employed to generate three-dimensional images of biofilm structures within stone samples. It employs fluorescent dyes to visualize biofilm components, such as microorganisms and extracellular matrix. SEM can help identify the precise composition of a stone by visualizing the crystal structures and patterns unique to each type.62 SEM and FIB/SEM (Focused Ion Beam/Scanning Electron Microscope) techniques have provided compelling evidence that the persistence of microorganisms within renal calculi over extended periods, will lead to biofilm formation. These biofilms consist of a mucoid matrix with diverse physiochemical microenvironments that foster cooperative bacterial communities, as highlighted in Didenko’s work in 2014.63 Bacterial cells under a thick layer of matrix, friable and dense perforated mucous formations were visualized on the surface of 9 out of 19 kidney stones by using a Quanta 200 3D microscope. Therefore, the electron microscopic examination of kidney stones demonstrated that microorganisms in patients with KSD are able to form biofilms.41 In a specific study conducted in Cairo, Egypt, a total of 54 kidney stones were carefully gathered from both male and female patients from various laboratories. Notably, these kidney stones were found to harbour Nano-bacterial infections, prompting a comprehensive SEM analysis. The SEM images revealed intriguing insights: after a 30-day incubation period, clusters of coccoid nanobes and individual coccal nano-bacteria were observed. Furthermore, transmission electron microscopy unveiled the distinctive characteristics of these nano-bacterial isolates, showcasing their spherical coccoid morphology and robust cell walls, which contributed to the formation of mineral structures, as elucidated by Nora et al.64 Moreover, these microscopic techniques were employed for qualitative assessments of biofilm production by the Nanobacterial isolates.
This holistic approach not only advances our understanding of the persistent presence of microorganisms within renal stones but also sheds light on the complex dynamics of biofilm development in this context, which could have implications for clinical interventions and treatment strategies. These high-resolution microscopic methods have the advantage of providing visual confirmation of biofilms’ presence and their structure. It allows for precise spatial information within the calculi. The limitation of these microscopic methods requires specialized equipment and expertise. Another constraint of their approach is that they focused solely on seeing the top of the biofilm, potentially overlooking the underlying layers. The practical use of very sensitive microscopic techniques in the clinical domain is currently limited, as these technologies are predominantly confined to research laboratories. The SEM and CLSM are typically associated with high costs, time-intensive procedures, and limited accessibility within conventional medical microbiology laboratories.
Molecular techniques
Detecting biofilms on kidney stones requires a multifaceted approach that combines molecular techniques with microscopy and other methods. These molecular techniques can help identify the specific microorganisms within biofilms and provide valuable insights into their composition and behaviour. The identification of specific bacteria within a diverse biofilm community can be accomplished by employing fluorescent in situ hybridization (FISH) probes. The utilization of peptide nucleic acid FISH with epifluorescence microscopy to identify certain bacteria is a molecularly specialized technique that has been implemented in a biofilm model.65 FISH involves using fluorescently labelled probes that target specific microbial DNA or RNA sequences within biofilms. This technique allows for the identification and quantification of microbial species. An advantage of employing probes combined with horseradish peroxidase is their capacity to prevent the destruction of microorganisms within a biofilm. The FISH method may be utilized to ascertain the growth rate of microorganisms inside a biofilm. This is because the ribosome quantity present in a microbe is directly correlated to its growth activity. The probe should be meticulously developed to specifically target and identify the preserved area of a solitary species.66,67 The limitation of FISH requires knowledge of target microbial sequences and might not provide information on biofilm structure and organization.68 Urea-splitting bacteria in individuals with infection stones may not always be reliably detected through traditional stone or urine culture methods. In such cases, the Polymerase Chain Reaction (PCR) emerges as a promising alternative. PCR techniques are employed for the purpose of identifying pathogens through the amplification of nucleic acid sequences that are specific to particular species. Additionally, these techniques are utilized for the detection of virulence factors by amplifying target genes associated with virulence, such as biofilm genes, using primers that are specific to these genes. Importantly, PCR techniques enable the detection of these genes even in cases where the pathogen is present in the sample but cannot be cultured. PCR is capable of identifying genetic components contained within calculi and holds significant potential as a valuable diagnostic tool for this purpose.69 PCR amplifies specific microbial DNA sequences, aiding in the identification of microorganisms present in the stone. PCR techniques, including conventional PCR, multiplex PCR, and qualitative real-time PCR (qPCR) are utilized for the detection of the biofilm-associated genes in microorganisms. The resulting PCR product is examined by visualization on an agarose gel containing DNA-intercalating dye like ethidium bromide when using conventional and multiplex PCR protocols for gene detection. This visualization step confirms the amplification and presence of the target gene. The qPCR can provide information about microbial load.41,70 Molecular approaches enable the detection of several components inside bacterial nucleic acids, including, DNA, proteins, surfactants, lipids, glycolipids, membrane vesicles, and ions such as calcium. The advantages of using these molecular techniques are high specificity for microbial identification and can be used on both surface and deeper layers of biofilms.71
Culturing techniques
Microbial culture is a crucial method in the examination of kidney stone samples. This process entails the cultivation and growth of microorganisms from the samples on selective media. Its primary objective is to identify viable microorganisms present within the kidney stones and assess their susceptibility to antibiotics. One of the primary purposes of microbial culture is to identify the types of microorganisms present within kidney stones. By isolating and growing these microorganisms on selective media, it becomes possible to determine the specific bacterial strains or fungi responsible for the infection or stone formation.72 Microbial culture allows for the quantification of microbial load within the kidney stone samples.73 Understanding the extent of infection and its potential impact on the patient’s health can make this information essential. Culturing microorganisms from kidney stones enables researchers and clinicians to assess their antibiotic susceptibility.74 This information is critical for selecting the most effective antibiotics for treatment and avoiding ineffective ones, thus improving patient outcomes. By knowing which microorganisms are causing the infection and their antibiotic susceptibility, healthcare providers can tailor antibiotic therapy to the specific pathogens present.73,74 This targeted approach can lead to more successful treatment and faster recovery. Microbial culture also contributes to scientific research and epidemiological studies related to kidney stone infections.57 It helps in understanding the prevalence of different microorganisms associated with stone formation, which can inform preventive measures.72 In laboratory settings, microbial culture is a quality control step to ensure that the results obtained from kidney stone samples are accurate and reliable. It helps validate the presence or absence of particular microorganisms or individuals with recurrent kidney stones or complicated infections, microbial culture results can guide long-term management strategies and help healthcare providers monitor the effectiveness of treatments over time.73,75 This information is essential for both patient care and scientific understanding of kidney stone-related infections. Bacterial cultivation may be performed directly from the stones. Between 1973 and the present, research in Asia and North America has shown that bacteria may be detected in approximately 15-70% of stones after clinical culture.57,72,76,56 The limitation of bacterial culture is that culture may not capture all microorganisms present in the calculi (non-culturable species), and also does not provide insight into the biofilm structure.
Metagenomics analysis
Identifying microbial species within a sample is accomplished by sequencing the 16S rRNA gene using the 16S rRNA Gene Sequencing technique. Metagenomics analysis provides a comprehensive view of microbial diversity and community composition. Traditional Microbiological methods typically involve the cultivation of individual microorganisms in a laboratory setting. Microbiologists isolate and grow specific bacteria or fungi on agar plates, making it possible to study them individually. Metagenomics, on the other hand, focuses on studying entire microbial communities in their natural habitats without the need for isolating and cultivating individual species. This approach allows researchers to investigate the collective genetic material of all microorganisms present, including bacteria, viruses, archaea, and fungi.
For instance, in one investigation, researchers employed 16S rRNA gene sequencing to identify and assess the diversity of eubacteria within metabolic stones containing calcium oxalate (CaOx).77 Using 16S rRNA sequencing, another study observed changes in the gut microbiota composition in individuals with kidney stones.78 Additionally, a separate study uncovered that the microbiome becomes encapsulated during in vivo CaOx stone formation and may play an active and/or passive role in influencing the biomineralization of kidney stones.43
In a study conducted by Yuan et al., the investigators examined the relationship between dietary patterns and gut microbial communities in individuals, both with and without kidney stones.79 They employed 16S rRNA sequencing as their research method. The findings revealed that individuals in the high-risk stone formation group exhibited a notable increase in the abundance of certain microorganisms, including Corynebacterium, Pseudomonas, Stenotrophomonas, Sphingomonas, Slackiain, Arcobacter, Hydrogenoanaerobacterium, and Faecalitalea. The regulation of gut microbial balance by dietary choices has the potential to prevent and treat calcium oxalate stones. In a recent investigation, a machine learning algorithm was developed with the objective of forecasting the probability of calcium oxalate kidney stone occurrence. This was achieved by integrating clinical data and gut microbiota characteristics. The study had 180 participants total, researchers heightened a total of 80 machine-learning methodologies by analyzing gut and clinical microbiome datasets obtained from 66 persons without stones and 54 individuals diagnosed with kidney stones. Through their analysis, the authors successfully identified three bacterial species (Flavobacterium, Rhodobacter, and Gordonia) that are associated with kidney stone formation.80
Hence, the findings from metagenomic analysis in renal stone biofilm research have implications for understanding the role of microbial communities in nephrolithiasis. Researchers can explore how specific microorganisms or genetic pathways may contribute to stone formation, biofilm development, or clinical outcomes.
Immunofluorescence techniques
Immunofluorescence methods provide high specificity and sensitivity for biofilm detection, allowing researchers to visualize the spatial distribution of specific biofilm components or antigens. Immunofluorescence Staining: This method uses antibodies labelled with fluorophores to target specific biofilm components, such as microorganisms or extracellular matrix proteins. It can provide information on biofilm composition and is useful for visualizing specific biofilm components. The utilization of immunofluorescence technology, which relies on the specificity of the antigen-antibody (Ag-Ab) interaction, has the capacity to meet the stringent specificity demands of clinical applications. Concurrently, the progressive advancements in fluorescence labelling and fluorescence detecting technology have consistently enhanced the heightened sensitivity to the technology of immunofluorescence. The conventional method of bacterial culture, utilized for the identification of bacterial species, is susceptible to delays in diagnosis and antibiotic treatment due to its time-consuming nature and limited sensitivity. In recent times, a plethora of novel detection techniques encompassing immunological and molecular biology approaches have been employed.81 An immunofluorescence biosensor was developed by employing an optical fiber probe. The device under consideration effectively used the advantageous properties of Ag-Ab specificity, fluorescence labeling, and the efficient propagation of fluorescence signals through an optical fiber. The surface of the probe was deliberately rendered immobile with the use of antibodies that selectively targeted E. coli. 82,83 Quantum dots (QDs) exhibit notable optical advantages that can enhance the intensity and precision of fluorescence signal detection. These advantages include high fluorescence emission, extended lifetimes with exceptional photostability, and substantial Stocks.84 Researchers have successfully constructed immunofluorescence-based biosensors utilizing quantum dots for S. aureus detection. These biosensors have the potential to be further enhanced for the detection of various species, hence enabling researchers to simultaneously detect several species. One potential drawback of Immunofluorescence approaches is the restricted specificity of the antibodies now available, which may result in incomplete capture of the full biofilm structure.
Each of these diagnostic techniques has its strengths and limitations, and a combination of methods is often used to gain a more comprehensive understanding of bacterial biofilms in renal stones. Integrating information from various techniques can provide valuable insights into biofilm presence, composition, structure, and spatial distribution, and contribute to a deeper understanding of microorganisms’ role in kidney stone pathogenesis.
Impact on Renal Calculi management and treatment
The presence of bacterial biofilms in renal calculi can significantly impact the management and treatment of stones, as well as the potential for recurrence. Gaining insight into the pivotal role of biofilms in stone formation and their resilience against conventional treatments is imperative for the development of enhanced strategies. Here’s an analysis of how biofilms influence treatment approaches and stone recurrence:
Impact on treatment strategies
Antibiotic resistance
Renal stone-associated infections are often chronic in nature. Bacteria residing within biofilms exhibit greater resistance to antibiotic agents when compared to their planktonic counterparts. This robust resistance in biofilms can be attributed to several key factors. First and foremost, the extracellular polymer matrix functions as a formidable physical barrier impeding the penetration of antibiotics. This structural shield reduces the antibiotic’s effectiveness in reaching concealed bacteria within the biofilm. 85-87 Furthermore, biofilm communities exhibit the secretion of enzymes dedicated to inactivating antibiotics. These enzymes are upregulated through QS mechanisms, further fortifying the biofilm’s resistance.88 Within the biofilm, phenotypic variations are also at play, fostering the emergence of persister cells. These cells, due to their suppressed metabolic activity, inherently resist antibiotics. Another crucial factor is the elevated expression of efflux pumps. Within bacterial cells, these membrane-bound transport proteins play a vital role in expelling various toxic molecules, including antimicrobial agents. This efflux mechanism significantly contributes to antibiotic resistance within biofilms. Additionally, antibiotic resistance genes of horizontal gene transfer (HGT) play a crucial role in the development of antimicrobial resistance in biofilms.89,90 Detailed accounts of specific HGT instances and their role in antimicrobial resistance within biofilms have been extensively documented and reviewed in prior research studies.85,89,91 The protective matrix of extracellular polymeric substances shields bacteria within the biofilm, preventing effective penetration of antibiotics. The presence of resistance might provide challenges in the management of UTIs that are linked to kidney stones. A new study has revealed that individuals both children and adults, who undergo treatment with certain oral antibiotics have a notably increased susceptibility to kidney stone formation, mostly attributed to the phenomenon of antibiotic resistance.92,93 Biofilms show an elevated resistance to antibiotic agents that is found to be 10-100 times higher compared to the planktonic cells.75,94 This is the inaugural instance in which these medications have been associated with this particular ailment. The greatest significant hazards were observed in individuals of younger age groups and among patients who had more recent exposure to antibiotics. The research team utilized electronic health records obtained from the United Kingdom, encompassing a population of 13 million individuals, including both adults and children who sought medical care from general practitioners under The Health Improvement Network. The data spanned a period from 1994 to 2015. The study involved the examination of antibiotic exposure history in a cohort of over 26,000 individuals diagnosed with kidney stones, in comparison to a control group including roughly 260,000 participants. The findings of the analysis revealed a notable correlation between the formation of kidney stones and the presence of antibiotic resistance that had accumulated over time.92
Incomplete stone removal
Biofilms can coat the surface of stones and be deeply embedded within their structure. During surgical procedures like lithotripsy or ureteroscopy, it can be challenging to completely remove the biofilm-associated layers, leading to recurrent infections and stone regrowth. If a portion of the kidney stone is left behind after treatment, it can continue to grow over time, leading to the recurrence of symptoms and the need for further intervention. Teichman demonstrated a renal failure related mortality rate was 2.9% more with incomplete stone clearance.95 Monitoring and follow-up may be necessary to address any residual stones. Incomplete stone removal can increase the risk of complications, such as UTIs or obstruction of the urinary tract.96 This increases the risk of UTIs and can lead to more severe complications, including pyelonephritis (kidney infection). Biofilm-coated stones can result in recurrent symptoms such as pain, fever, and urinary symptoms.96 These recurrent symptoms can be frustrating for patients and require further evaluation and treatment. Biofilms can make bacteria more antibiotic resistant and immune system responses. This can complicate the UTI treatment associated with residual stones, requiring the use of more potent or longer courses of antibiotics.52 The presence of biofilms can lead to chronic inflammation in the urinary tract, even in the absence of acute infections. This ongoing inflammation can contribute to discomfort and complications. Biofilms can act as a protective barrier around stone fragments, making it more challenging to fragment and remove those using procedures like lithotripsy or ureteroscopy.96,52 These complications may require prompt medical attention and treatment adjustments. The presence of residual stones may require a modification in the treatment approach. This could include using different techniques or procedures to target and remove the remaining stones effectively.
Limited effectiveness of antimicrobial agents
Biofilms can significantly decrease the effectiveness of antibiotics in treating kidney stones and associated UTIs. Conventional antimicrobial agents might not effectively target bacteria within biofilms. This ineffectiveness can result in persistent infections, as even successful eradication of planktonic bacteria (free-floating) might not eliminate the bacteria protected within biofilms. This lower metabolic rate can make bacteria less susceptible to antibiotics that rely on active cellular processes for their mechanisms of action. This resistance can be both intrinsic (related to biofilm structure and metabolic changes) and acquired (resulting from genetic mutations or horizontal gene transfer within the biofilm community). As a result, antibiotics that may be effective against planktonic bacteria can be less effective against biofilm-encased bacteria.97,98
Strategies for biofilm disruption
Biofilm development takes a significant role in the pathogenicity of bacteria and resistance to antibiotics, it is imperative to develop specific solutions to address this issue. Based on prior research findings, it has been observed that antibiotics are more efficacious in treating premature biofilms compared to mature biofilms.99 The selection of an appropriate antibiotic for the treatment of biofilms should be based on both sensitivity and the ability to effectively enter the biofilm matrix.100 Previous investigations have demonstrated that bacteria residing beneath biofilms have a higher level of antibiotic resistance compared to their planktonic components. Hence, the utilization of combinatorial treatment is considered more favourable compared to antibiotic monotherapy.101 In addition, it is important to provide antibiotics correctly in terms of dosage and duration during the therapy.102 Urease producing bacteria have been seen to generate crystalline biofilms. In addition, urease inhibitors have been employed to hinder the breakdown of urea, hence increasing the pH of P. mirabilis in vitro. This pH elevation serves to reduce the occurrence of encrustation.103 Bacterial organisms establish a close and symbiotic relationship with the crystal layer, therefore shielding it from the antibacterial properties shown by impregnated chemicals. Hence, it is crucial to prevent the reduction in urine pH and the consequent crystallization in order to effectively inhibit the growth of biofilm.104 A study demonstrated the inhibitory effects of furanones on the growth of S. epidermidis biofilm on urinary catheters in animal models.105 Additionally, the researchers found that azithromycin effectively reduced QS-dependent phenotypes in vitro. Recent research has discovered that several natural substances possess antibacterial activities by influencing the phenotypes of QS.104 The utilization of non-pathogenic bacteria, sometimes referred to as bacterial interference or antagonisms, has been shown to effectively inhibit the adherence and production of biofilms by pathogens on the surface of catheters.103 The nanostructured metal ions and their compounds possess notable antibacterial properties, making them potentially effective in addressing the issue of hazardous biofilms. These solutions have potential applications not only in the field of medicine but also in ecological and industrial contexts.106,107 In a recent study, it was shown that the use of chitosan, a well-known biopolymer known for its antibacterial characteristics, may have the potential to eradicate uropathogens and bacterial biofilms often associated with kidney stones. In the context of laboratory culture experiments, it was observed that a minimal concentration of chitosan at a mere 0.0001% (w/v) effectively impeded the growth of planktonic forms of the commonly occurring uropathogens found in individuals with a predisposition to kidney stone formation. These uropathogens include E. coli, Proteus mirabilis, Klebsiella pneumoniae, and Staphylococcus aureus.108
Impact on stone recurrence
Reservoir for infection
Biofilms have the potential to serve as reservoirs for bacterial strains that are capable of inducing recurrent urinary tract infections. Despite receiving treatment for the original infection, the presence of viable bacteria within biofilms might result in subsequent infections, hence contributing to the recurrence of stones. A retrospective analysis examined a cohort of 120 individuals with recurrent UTIs who had undergone surgical extraction of stone. Recurrent UTIs were operationally defined as the occurrence of three or more UTIs during a single calendar year, or the occurrence of two or more UTIs over the prior six-month period. A study found that Group 1 did not exhibit any indications of recurrent infection one year following the removal of the stone, while Group 2 experienced the development of recurrent infection.109 The production of bacterial biofilms is a significant virulence factor in uropathogens since it given a crucial role in the persistence and recurrence of infections.110 Infections that are linked to the presence of kidney stones have the potential to disseminate throughout the urinary tract, giving rise to various problems, including pyelonephritis (infection of the kidneys) and sepsis, both of which possess the capacity to pose a significant risk to an individual’s life.111 A systematic review incorporated a total of 17 publications, which collectively provided substantial evidence supporting a robust correlation between kidney stones and the recurrence of UTIs. The surgical extraction of kidney stones typically leads to the cure of UTIs, however, there are conflicting findings about the rates of recurrence following surgery. In certain instances, the presence of bacterial colonization on stones has been found to elevate the likelihood of severe sepsis.37 In essence, the presence of kidney stone biofilms might function as reservoirs for infection as a result of the capacity of bacteria to cling to and construct defensive biofilms on the uneven surface of kidney stones. A comprehensive comprehension of the significance of biofilms in infections connected to kidney stones is crucial in order to ensure accurate diagnosis and efficient treatment. Failure to effectively address these infections can result in the development of serious consequences.
Surgical complications
The existence of biofilms has the potential to give rise to difficulties during surgical procedures. There are three regularly employed surgical techniques for kidney stone treatment, which are selected based on factors such as size and complexity. These procedures include ureteroscopy with laser lithotripsy and/or basket retrieval (URS), external shock-wave lithotripsy (SWL), and percutaneous nephrolithotomy (PCNL). Infection is the prevailing consequence subsequent to PCNL, and research has demonstrated that the prevalence of systemic inflammatory response syndrome (SIRS) might reach up to 35% among individuals afflicted with intricate stones.112 Biofilm-associated stones might be harder to fragment and remove, leading to incomplete stone clearance and a higher risk of recurrence. Manipulating kidney stones during surgery can disrupt biofilms, releasing trapped microorganisms into the urinary tract, potentially causing systemic infection or spreading the infection to other parts of the urinary system.109 The presence of biofilms may require more time and care during surgery, as surgeons may need to meticulously remove biofilm-encrusted stones and associated debris, which can prolong the surgical procedure.112 Surgery on kidney stones with biofilms can trigger a more significant inflammatory response in the body due to the release of bacterial components or toxins from disrupted biofilms.113 In a prospective trial comprising 1666 instances of kidney stone removal, the occurrence of inflammatory sequelae was detected in 34.1% of cases. However, in the group undergoing PCNL, this prevalence was comparatively lower at 24.6%. The contact ureterolithotripsy group exhibited a complication incidence rate of 7.8%, whereas the ureterolithoextraction group had a lower rate of 2.5%.114 Surgical procedures may be less effective if the underlying infection is not adequately treated before or after surgery. Aggressive surgical techniques or instruments used to remove stones with biofilms may inadvertently damage renal tissue, increasing the risk of complications such as hemorrhage or impaired kidney function. In a meta-analysis comparing SWL and URS for kidney stones measuring 10 to 20 mm in size, URS yielded superior SFR and a reduced need for retreatment, all without a concomitant rise in the rate of complications.115 Despite surgical removal, the presence of biofilm remnants or released microorganisms can lead to postoperative infections, which may require prolonged antibiotic treatment and additional medical interventions.113-115 In light of these challenges, researchers and clinicians are exploring innovative approaches to address biofilm-associated kidney stones. Developing targeted therapies that can penetrate biofilms and disrupt their structure; Using advanced imaging techniques to identify biofilm-associated stones before treatment; Combining surgical interventions with antibiofilm agents to enhance stone clearance.
Therapeutic approaches and research directions
Developing novel therapies specifically targeting biofilms is a promising research direction. Enzymes, antimicrobial peptides, and nanoparticles are being investigated for their potential to disrupt biofilm matrices and increase the efficacy of antibiotic treatments.
Protease enzymes
Bacterial biofilms frequently adhere to surfaces, encompassing both living organisms and non-living structures. They are composed of a mixture of proteins, polysaccharides, and nucleic acids. Consequently, chemicals, such as protease enzymes can disrupt any of these components and have the ability to impede or disturb the EPS matrix, potentially leading to the disintegration of the biofilm. Protease enzymes like bromelain, actinidin, papain, serratiopeptidase, carboxypeptidase, proteinase K, a-amylase, and trypsin have been documented to exhibit inhibitory effects on dental biofilms, including both single and multi-species biofilms.116
Antimicrobial peptides
A study revealed that AMPs have strong bactericidal properties against Streptococcus pneumoniae and Clostridium difficile.117 Furthermore, it demonstrates activity against biofilms formed by MRSA and the formation of biofilms involving other bacterial species. The main focus of their action is on bacterial membranes, exhibiting a wide range of antibacterial properties, including a heightened susceptibility to metabolically inactive bacteria seen in biofilms.118 AMPs are frequently utilized in conjugation with antibiotics and other anti-agents for the purpose of combating biofilms. In addition to their function as a vital element of innate immunity, HDPs have the ability to specifically target planktonic cells. Furthermore, they exhibit both anti-biofilm properties and immunomodulatory effects that are directed towards the host. In their study, Cohen et al. successfully synthesized complexes of antimicrobial peptides with vancomycin by the use of coupling chemistry. The researchers also demonstrated the enhanced broad-spectrum antibacterial activity of these complexes, surpassing that of vancomycin alone, as shown in vitro. In a recent investigation, Garvicin KS was found as a broad-spectrum antimicrobial peptide (AMP) that is generated by Lactobacillus garvieae.119 The AMP demonstrated bactericidal efficacy against a total of 240 strains, encompassing 19 distinct species of gram positive bacteria. Nonetheless, its efficacy against gram-negative bacteria was reported to have some limitations, as documented by Ovchinnikov. Various synthetic AMPs, such as HB43, Bac8c, P18, WMR, Omiganan, Polyphemusin, and Ranalexin, have demonstrated efficacy in eradicating S. aureus biofilms within catheters.119
Nanoparticles
Nanoparticles with antibacterial qualities have the ability to effectively infiltrate biofilms and directly administer antimicrobial drugs to the targeted region. The field of nanotechnology exhibits the potential to augment the effectiveness of medical therapy and mitigating the issue of resistance to antibiotics. The use of antimicrobial nanoparticles as a potential alternative to antibiotics is presently a prominent area of interest within the field of medicine, displaying encouraging potential. The functional properties of nanomaterials are significantly influenced by their micro-diameter. Nevertheless, it is worth noting that a significant proportion of nanoparticles have a tendency to form aggregates when suspended in a solution. This propensity for aggregation has the potential to restrict their effectiveness in the context of photothermal treatment (PTT) and photodynamic therapy (PDT). One viable strategy for surmounting this obstacle involves employing polymers, such as PEG and BSA, for the purpose of both transporting the substances and facilitating the requisite surface functionalization to augment their dispersibility and biocompatibility.118 The efficacy of gallium (Ga)-based nanoparticles in the eradication of biofilms has been investigated in mice, with promising outcomes both in vivo and in vitro methods. The efficacy of combating resistant bacteria can be attributed to the Ga2L3 (bpy)2, and lipophilic Ga complex which exhibits both Ga-induced disruption of iron metabolism and ligand-induced generation of reactive oxygen species (ROS).120 A novel protective coating material utilizing a combination of graphene and hydrogels has been presented. This unique coating aims to serve as an effective anti-biofilm agent by preventing the attachment of microbiological organisms.121 Recent studies have identified GO films as potential biocompatible substrates for bacterial adhesion120,122
Quorum sensing inhibitors
The use of Quorum Sensing Inhibitors (QSIs) for renal calculi biofilms is a developing area of research with the capability to provide innovative solutions for the treatment of kidney stone-related biofilms. QSIs impede bacterial intercellular communication and the process of biofilm development. The objective of research in this field is to ascertain substances that possess the ability to impede the signalling processes responsible for facilitating the production of biofilms. The efficiency of QSIs in therapeutically relevant bacterial biofilms has been thoroughly assessed through the utilization of both in vitro models and in vivo models. In the model of mouse wound (Sham), the application of an RNAIII inhibiting peptide resulted in a decrease in MRSA biofilms. The investigation’s findings showed that methanol extracts obtained from burdock roots (BR) did not demonstrate bactericidal activity (p > 0.05) against the uropathogens. However, the same extracts did demonstrate a significant inhibitory effect on biofilms (p < 0.05) formed on polystyrene and surfaces of glass, with 100 µg/mL of biofilm inhibitory concentration. The extracts derived from BR were found to have inhibitory effects on cellular phenotypes regulated by QS, including the production of violacein and prodigiosin, swarming motility, and cell surface hydrophobicity (Rajshekharan). Over the past few years, there has been a growing fascination with the potential of various medicinal plants, such as Syzygium aromaticum, Mentha piperita, Jasminum sambac, Rosmarinus officinalis, Ocimum sanctum, Lilium brownii, and others, to exhibit anti-quorum sensing properties. Peptides containing tryptophan were shown to disrupt the Pseudomonas quorum sensing system, resulting in the inhibition of biofilm formation, virulence factor synthesis, and accumulation of EPS. Disrupting the signalling transductions among microorganisms. The use of strategies that disrupt signalling pathways connected with QS in order to inhibit the gene expression associated with the formation of biofilm, is regarded as a recommended method. Numerous prior investigations have shown the acknowledged association between the modulation of QS and the alteration of genetic variants and bacterial transcriptomes. Ascorbic acid is a further chemical that possesses the advantageous qualities of being harmless to people, cost-effective, and readily accessible, while also demonstrating the capability to interfere with the QS mechanism. The ability of ascorbic acid to control the generation of reactive oxygen species led to an additional decrease in QS after the effector molecules underwent alkaline hydrolysis. The individual identified as Shivaprasad. The category of anti-diabetic drugs known as gliptins was evaluated for their anti-QS properties. It is worth mentioning that sitagliptin has been demonstrated to effectively decrease the expression of autoinducer synthetase genes in S. aureus, Serratia marcescens, and P. aeruginosa. This, in turn, leads to the inhibition of QS receptors, resulting in reduced biofilm formation and diminished expression of virulence factors.
Combination therapies
Combining traditional antibiotics with biofilm-disrupting agents might enhance treatment outcomes. This approach could be particularly beneficial in cases where biofilms are present. Broad-spectrum antibiotics can be used in combination to target a wider range of bacteria within the biofilm. Antibiotics that penetrate the biofilm matrix effectively, such as tobramycin, may be used alongside standard antibiotics like amoxicillin or ciprofloxacin. Multiple studies advocate for the utilization of combination therapy as the preferred approach in managing infections linked with biofilms, wherein macrolides are frequently among the initial antibiotics selected. Macrolides, including clarithromycin, erythromycin, and azithromycin, have significant antibiofilm efficacy against biofilm-related illnesses caused by Gram-negative bacteria.
In conclusion, the study of bacterial biofilms in the context of renal calculi has illuminated a previously understudied aspect of stone formation and urinary tract health. Biofilms, complex communities of microorganisms encased within a protective matrix, have been identified in kidney stones and are suspected to play a crucial role in stone pathogenesis. Emerging evidence suggests that bacterial biofilms are frequently associated with renal calculi, contributing to their formation, growth, and recurrence. The interaction between biofilms and stone formation has important implications for patient management, treatment strategies, and stone recurrence. Biofilms can render stones more resistant to treatment and may contribute to chronic urinary tract infections, exacerbating kidney stone formation and patient discomfort. Detecting biofilm-associated infections in renal calculi presents diagnostic challenges; conventional methods, such as urine cultures, might not effectively identify the presence of biofilm-associated bacteria. Newer diagnostic techniques, including molecular assays and imaging modalities, are being explored to improve the accuracy of detection.
Addressing recurrent renal calculi infections associated with bacterial biofilms requires innovative therapeutic strategies. Approaches include the development of biofilm-disrupting agents, combination therapies targeting both the biofilm and the underlying stone, and interventions to modulate the host immune response. The use of protease enzymes, antimicrobial peptides, and nanoparticles shows promising results in disrupting biofilm matrices and enhancing treatment efficacy. Additionally, exploring the use of quorum sensing inhibitors and immunomodulatory agents may provide new avenues for disrupting biofilm formation and reducing the risk of recurrence. Personalized treatment plans that account for the biofilm’s unique characteristics and the patient’s medical history hold promise in improving treatment outcomes.
Additionally, developing effective preventive strategies is essential. Nutritional and lifestyle interventions can lower the risk of stone formation, while maintaining good urinary tract health may prevent biofilm development. Exploring the potential of immunomodulators and bacteriophages as therapies against biofilms associated with renal calculi could hold promise. Further research is required to understand their safety and efficacy. Enhanced imaging methods can assist in identifying and characterizing biofilms inside kidney stones, guiding treatment decisions and monitoring effectiveness.
Kidney stone disease often requires long-term management and monitoring to prevent recurrence. Raising awareness about kidney stone risk factors, early symptoms, and the importance of timely medical attention is crucial for reducing the burden of stone-related complications. Collaboration among urologists, nephrologists, microbiologists, and biofilm researchers is essential to advance our understanding of the interplay between biofilms and renal calculi and to develop effective treatment strategies.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
Not applicable.
- Vestby LK, Gronseth T, Simm R, Nesse LL. Bacterial Biofilm and Its Role in the Pathogenesis of Disease. Antibiotics. 2020;9(2):59.
Crossref - Hoiby N. A short history of microbial biofilms and biofilm infections. APMIS. 2017;125(4):272-275.
Crossref - Leslie SW, Sajjad H, Murphy PB. Renal Calculi, Nephrolithiasis. StarPearls. 2023. https://www.ncbi.nlm.nih.gov/books/NBK442014. Accessed October 30, 2023.
- Trinchieri A. Body fatness, diabetes, physical activity and risk of kidney stones: a systematic review and meta-analysis of cohort studies. Eur J Epidemiol. 2019;34(12):1175-1176.
Crossref - Ratkalkar VN, Kleinman JG. Mechanisms of Stone Formation. Clin Rev Bone Miner Metab. 2011;9(3-4):187-197.
Crossref - Alelign T, Petros B. Kidney stone disease: An update on current concepts. Adv Urol. 2018;2018(3068365):1-12.
Crossref - Scales CD, Smith AC, Hanley JM, Saigal CS. Prevalence of Kidney Stones in the United States. Eur Urol. 2012;62(1):160-165.
Crossref - Moftakhar L, Jafari F, Johari MG, Rezaeianzadeh R, Hosseini SV, Rezaianzadeh A. Prevalence and risk factors of kidney stone disease in population aged 40-70 years old in Kharameh cohort study: a cross-sectional population-based study in southern Iran. BMC Urol. 2022;22(1).
Crossref - Safdar OY, Alzahrani WA, Kurdi MA, et al. The prevalence of renal stones among local residents in Saudi Arabia. J Family Med Prim Care. 2021;10(2):974-977.
Crossref - Funari R, Shen AQ. Detection and Characterization of Bacterial Biofilms and Biofilm-Based Sensors. ACS Sensors. 2022;7(2):347-357.
Crossref - Romero V, Akpinar H, Assimos DG. Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Rev Urol. 2010;12(2-3):e86-96.
- Hobbs T, Schultz LN, Lauchnor EG, Gerlach R, Lange D. Evaluation of Biofilm Induced Urinary Infection Stone Formation in a Novel Laboratory Model System. J Urol. 2018;199(1):178-185.
Crossref - Halinski A, Bhatti KH, Boeri L, et al. Spectrum of Bacterial Pathogens from Urinary Infections Associated with Struvite and Metabolic Stones. Diagnostics. 2022;13(1):80.
Crossref - Khan SR, Pearle MS, Robertson WG, et al. Kidney stones. Nat Rev Dis Prim. 2016;2(1):1-23.
Crossref - Coe FL, Evan A, Worcester E. Kidney stone disease. J Clin Invest. 2005;115(10):2598-2608.
Crossref - Hola V, Peroutkova T, Ruzicka F. Virulence factors in in Proteus bacteria from biofilm communities of catheter-associated urinary tract infections. FEMS Immunol Med Microbiol. 2012;65(2):343-349.
Crossref - Marcus RJ, Post JC, Stoodley P, et al. Biofilms in nephrology. Expert Opin Biol Ther. 2008;8(8):1159-1166.
Crossref - Elhoshi M, El-Sherbiny E, Elsheredy A, Aboulela AG. A correlation study between virulence factors and multidrug resistance among clinical isolates of Proteus mirabilis. Braz J Microbiol. 2023;54(3):1387-1397.
Crossref - Vertes A, Hitchins V, Phillips KS. Analytical Challenges of Microbial Biofilms on Medical Devices. Anal Chem. 2012;84(9):3858-3866.
Crossref - Evan AP. Physiopathology and etiology of stone formation in the kidney and the urinary tract. Pediatr Nephrol. 2010;25(5):831-841.
Crossref - Robertson WG, Heyburn PJ, Peacock M, Hanes FA, Swaminathan R. The effect of high animal protein intake on the risk of calcium stone formation in the urinary tract. Clin Sci (Lond). 1979;57(3):285-288.
Crossref - Riddle HAL, Zhang S, Qian F, et al. Kidney Stone Formation in a Novel Murine Model of Polycystic Kidney Disease. Am J Physiol Renal Physiol. 2022;323(1):F59-F68.
Crossref - Trinchieri A. Urinary calculi and infection. Urologia. 2014;81(2):93-98.
Crossref - Miller AW, Penniston KL, Fitzpatrick K, Agudelo J, Tasian G, Lange D. Mechanisms of the intestinal and urinary microbiome in kidney stone disease. Nat Rev Urol. 2022;19(12):695-707.
Crossref - Howles SA, Thakker RV. Genetics of kidney stone disease. Nat Rev Urol. 2020;17(7):407-421.
Crossref - Wallace B, Chmiel JA, Al KF, et al. The Role of Urinary Modulators in the Development of Infectious Kidney Stones. J Endourol. 2023;37(3):358-366.
Crossref - Taylor EN, Stampfer MJ, Curhan GC. Obesity, Weight Gain, and the Risk of Kidney Stones. JAMA. 2005;293(4):455-462.
Crossref - KC M, Leslie SW. Uric acid nephrolithiasis. In: Taal MW, Chertow GM, Marsden PA, et al., editors. Brenner and Rector’s The Kidney. 11th ed. Elsevier; 2020: 1093-1101.
- Bagale G, Pradhan SR, Basnet A. Recurrent Nephrolithiasis Due to Parathyroid Adenoma. Cureus. 2021;13(10):e18468.
Crossref - Di Martino P. Extracellular polymeric substances, a key element in understanding biofilm phenotype. AIMS Microbiol. 2018;4(2):274-288.
Crossref - Holmgren K, Danielson BG, Fellstrom B, Ljunghall S, Niklasson F, Wikstrom B. The relation between urinary tract infections and stone composition in renal stone formers. Scand J Urol Nephrol. 1989;23(2):131-136.
Crossref - Huang WY, Chen YF, Chen SC, Lee YJ, Lan CF, Huang KH. Pediatric Urolithiasis in Taiwan: A Nationwide Study, 1997-2006. Urology. 2012;79(6):1355-1359.
Crossref - Jan H, Akbar I, Kamran H, Khan J. Frequency of renal stone disease in patients with urinary tract infection. J Ayub Med Coll Abbottabad. 2008;20(1):60-62
- Brain E, Geraghty RM, Cook P, Roderick P, Somani B. Risk of UTI in kidney stone formers: a matched-cohort study over a median follow-up of 19 years. World J Urol. 2021;39(8):3095-3101.
Crossref - Cetin N, Gencler A, Tufan AK. Risk factors for development of urinary tract infection in children with nephrolithiasis. J Paediatr Child Health. 2019;56(1):76-80.
Crossref - Kitano H, Shigemoto N, Koba Y, et al. Indwelling catheterization, renal stones, and hydronephrosis are risk factors for symptomatic Staphylococcus aureus-related urinary tract infection. World J Urol. 2020;39(2):511-516.
Crossref - Ripa F, Pietropaolo A, Montanari E, Hameed BMZ, Gauhar V, Somani BK. Association of Kidney Stones and Recurrent UTIs: the Chicken and Egg Situation. A Systematic Review of Literature. Curr Urol Rep. 2022;23(9):165-174.
Crossref - Hanstock S, Chew B, Lange D. The Role of the Gut Microbiome in Kidney Stone Disease. Urologic Clinics of North America. 2024;51(4):475-482.
Crossref - Crivelli JJ, Maalouf NM, Paiste HJ, et al. Disparities in Kidney Stone Disease: A Scoping Review. J Urol. 2021;206(3):517-525.
Crossref - Janakiram B, Sunitha T, Babu MG, Sekhar B, Bondili JS. Etiology of urolithiasis from South Indian population: Correlation of recurrence and antibiotic resistance to biofilm production capabilities of uropathogenic microbes. Int J Pharma Bio Sci. 2014.
- Romanova YM, Mulabaev NS, Tolordava ER, et al. Microbial Communities On Kidney Stones. Molecular Genetics, Microbiol Virol. 2015;33:20-25.
Crossref - Torzewska A, Budzynska A, Bialczak-Kokot M, Rozalski A. In vitro studies of epithelium-associated crystallization caused by uropathogens during urinary calculi development. Microb Pathog. 2014;71-72:25-31.
Crossref - Saw JJ, Sivaguru M, Wilson EM, et al. In Vivo Entombment of Bacteria and Fungi during Calcium Oxalate, Brushite, and Struvite Urolithiasis. Kidney360. 2020;2(2):298-311.
Crossref - Izatulina A, Zelenskaya M, Frank-Kamenetskaya O. Microbial Colonies in Renal Stones. Springer Proceedings in Earth and Environmental Sciences. 2019:415-418.
Crossref - Paul S, Singh V, Sankhwar S, Garg M. Renal aspergillosis secondary to renal intrumentation in immunocompetent patient. Case Reports. 2013;2013:bcr2013200306-bcr2013200306.
Crossref - Cui H. Distribution and drug resistance of pathogens causing urinary tract infection in patients with urinary calculi. Am J Transl Res. 2021;13(9):10554-10561.
- Cherng JH, Hsu YJ, Liu CC, et al. Activities of Ca2+ -related ion channels during the formation of kidney stones in an infection-induced urolithiasis rat model. Am J Physiol Renal Physiol. 2019;317(5):F1342-F1349.
Crossref - Devuyst O, Pirson Y. Genetics of hypercalciuric stone forming diseases. Kidney Int. 2007;72(9):1065-1072.
Crossref - Behzadi P, Garcia-Perdomo HA, Gomez AMA, Pinheiro M, Sarshar M. Editorial: Uropathogens, urinary tract infections, the host-pathogen interactions and treatment. Front Microbiol. 2023;14:1183236.
Crossref - Silago V, Moremi N, Mtebe M, et al. Multidrug-Resistant Uropathogens Causing Community-Acquired Urinary Tract Infections among Patients Attending Health Facilities in Mwanza and Dar es Salaam, Tanzania. Antibiotics. 2022;11(12):1718.
Crossref - Konieczna I, Zarnowiec P, Kwinkowski M, et al. Bacterial Urease and its Role in Long-Lasting Human Diseases. Curr Protein Pept Sci. 2012;13(8):789-806.
Crossref - Sabih A, Leslie SW. Complicated Urinary Tract Infections. StarPearls. 2023.
- Klein RD, Hultgren SJ. Urinary tract infections: microbial pathogenesis, host-pathogen interactions and new treatment strategies. Nat Rev Microbiol. 2020;18(4):211-226.
Crossref - Purves JT, Hughes FM. Inflammasomes in the urinary tract: a disease-based review. Am J Physiol Renal Physiol. 2016;311(4):F653-F662.
Crossref - Mirzaei R, Mohammadzadeh R, Alikhani MY, et al. The biofilm associated bacterial infections unrelated to indwelling devices. IUBMB Life. 2020;72(7):1271-1285.
Crossref - Thompson RB, Stamey TA. Bacteriology of infected stones. Urology. 1973;2(6):627-633.
Crossref - Tavichakorntrakool R, Prasongwattana V, Sungkeeree S, et al. Extensive characterizations of bacteria isolated from catheterized urine and stone matrices in patients with nephrolithiasis. Nephrol Dial Transplant. 2012;27(11):4125-4130.
Crossref - Lewi HJE, White A, Hutchinson AG, Scott R. The bacteriology of the urine and renal calculi. Urol Res. 1984;12(2):107-109.
Crossref - Maier A, Man A, Chibelean C, et al. Bacteriological evaluation of the non-struvite nephrolithiasis and its association with urinary tract infections. Rev Rom Med Lab. 2015;23(4):457-468.
Crossref - Barr-Beare E, Saxena V, Hilt EE, et al. The Interaction between Enterobacteriaceae and Calcium Oxalate Deposits. PLOS ONE. 2015;10(10):e0139575.
Crossref - Lemberger U, Pjevac P, Hausmann B, et al. The microbiome of kidney stones and urine of patients with nephrolithiasis. Urolithiasis. 2023;51(1):27.
Crossref - Anderson GG, Palermo JJ, Schilling JD, Roth R, Heuser J, Hultgren SJ. Intracellular Bacterial Biofilm-Like Pods in Urinary Tract Infections. Science. 2003;301(5629):105-107.
Crossref - Didenko LV, Tolordava ER, Perpanova TS, Shevlyagina NV. Electron microscopy investigation of urine stones suggests how to prevent post-operation septic complications in nephrolithiasis. J Appl Med Sci. 2014;3(4):19-34
- Hassan NF, Ibrahim MA, El-Tablawy SY, Farrag HAA. Characterization of Biofilm Producer Nanobacteria Isolated from Kidney Stones of Some Egyptian Patients. Pak J Biol Sci. 2021;24(9):953-970.
Crossref - Malic S, Hill KE, Hayes A, Percival SL, Thomas DW, Williams DW. Detection and identification of specific bacteria in wound biofilms using peptide nucleic acid fluorescent in situ hybridization (PNA FISH). Microbiology. 2009;155(8):2603-2611.
Crossref - Biofilm Eradication and Prevention: A Pharmaceutical Approach to Medical Device Infections | Wiley. Wiley.com. Accessed October 30, 2023.
- Stahl D. Development and application of nucleic acid probes. Semantic Scholar. Available at: https://www.semanticscholar.org/paper/Development-and-application-of-nucleic-acid-probes. Accessed May 20, 2023.
- Hall-Stoodley L, Hu FZ, Gieseke A, et al. Direct Detection of Bacterial Biofilms on the Middle-Ear Mucosa of Children With Chronic Otitis Media. JAMA. 2006;296(2):202.
Crossref - Takeuchi H, Yamamoto S, Terai A, et al. Detection of Proteus mirabilis urease gene in urinary calculi by polymerase chain reaction. Int J Urol. 1996;3(3):202-206.
Crossref - Huang HS, Chen J, Teng LJ, Lai MK. Use of polymerase chain reaction to detect Proteus mirabilis and Ureaplasma urealyticum in urinary calculi. J Formos Med Assoc. 1999;98(12):844-850.
- Soto SM. Importance of Biofilms in Urinary Tract Infections: New Therapeutic Approaches. Adv Biol. 2014;2014(1):543974.
Crossref - Price TK, Dune T, Hilt EE, et al. The Clinical Urine Culture: Enhanced Techniques Improve Detection of Clinically Relevant Microorganisms. J Clin Microbiol. 2016;54(5):1216-1222.
Crossref - Mufarrij PW, Lange JN, Assimos DG, Mirzazadeh M, Holmes RP. Multibacterial growth from a surgical renal stone culture: a case report and literature review. Rev Urol. 2012;14(3-4):108-114.
- Shah P, Baral R, Agrawal CS, Lamsal M, Baral D, Khanal B. Urinary Calculi: A Microbiological and Biochemical Analysis at a Tertiary Care Hospital in Eastern Nepal. Int J Microbiol. 2020;2020(1):8880403.
Crossref - Singh VK, Rai PK. Kidney stone analysis techniques and the role of major and trace elements on their pathogenesis: a review. Biophys Rev. 2014;6(3-4):291-310.
Crossref - Wang X, Krambeck AE, Williams JC, et al. Distinguishing Characteristics of Idiopathic Calcium Oxalate Kidney Stone Formers with Low Amounts of Randall’s Plaque. Clin J Am Soc Nephrol. 2014;9(10):1757-1763.
Crossref - Suryavanshi MV, Bhute SS, Kajale SC, Gune RP, Shouche YS. Molecular Imprints of Bacteria in Oxalate Containing Kidney Stone: A Preliminary Report. J Clin Diagon Res. 2018;12(3).
Crossref - Tang R, Jiang Y, Tan A, et al. 16S rRNA gene sequencing reveals altered composition of gut microbiota in individuals with kidney stones. Urolithiasis. 2018;46(6):503-514.
Crossref - Yuan C, Jin X, He Y, Liu Y, Xiang L, Wang K. Association of dietary patterns with gut microbiota in kidney stone and non-kidney stone individuals. Urolithiasis. 2022;50(4):389-399.
Crossref - Xiang L, Jin X, Liu Y, et al. Prediction of the occurrence of calcium oxalate kidney stones based on clinical and gut microbiota characteristics. World J Urol. 2022;40(1):221-227.
Crossref - Tenover FC, Tickler IA, Le VM, Dewell S, Mendes RE, Goering RV. Updating Molecular Diagnostics for Detecting Methicillin-Susceptible and Methicillin-Resistant Staphylococcus aureus Isolates in Blood Culture Bottles. J Clin Microbiol. 2019;57(11):e01195-19.
Crossref - Liu T, Zhao Y, Zhang Z, et al. A fiber optic biosensor for specific identification of dead Escherichia coli O157:H7. Sens Actuators B: Chem. 2014;196:161-167. Accessed 2014.
Crossref - Zhang Z, Hua F, Liu T, et al. A double-taper optical fiber-based radiation wave other than evanescent wave in all-fiber immunofluorescence biosensor for quantitative detection of Escherichia coli O157:H7. PloS One. 2014;9(5):e95429.
Crossref - Cui J, Zhou M, Li Y, et al. A new optical fiber probe-based quantum dots immunofluorescence biosensor in the detection of Staphylococcus aureus. Front Cell Infect Microbiol. 2021;11:665241.
Crossref - Balcazar JL, Subirats J, Borrego CM. The role of biofilms as environmental reservoirs of antibiotic resistance. Front Microbiol. 2015;6:1216.
Crossref - Uruen C, Chopo-Escuin G, Tommassen J, Mainar-Jaime RC, Arenas J. Biofilms as Promoters of Bacterial Antibiotic Resistance and Tolerance. Antibiotics. 2020;10(1):3.
Crossref - Hoiby N, Bjarnsholt T, Givskov M, Molin S, Ciofu O. Antibiotic resistance of bacterial biofilms. Int J Antimicrob Agents. 2010;35(4):322-332.
Crossref - Mah TFC, O’Toole GA. Mechanisms of biofilm resistance to antimicrobial agents. Trends Microbiol. 2001;9(1):34-39.
Crossref - Abe K, Nomura N, Suzuki S. Biofilms: hot spots of horizontal gene transfer (HGT) in aquatic environments, with a focus on a new HGT mechanism. FEMS Microbiol Ecol. 2020;96(5):fiaa031.
Crossref - Blesa A, Berenguer J. Contribution of vesicle-protected extracellular DNA to horizontal gene transfer in Thermus spp. Int Microbiol. 2015;18(3):177-187.
Crossref - Lila ASA, Rajab AAH, Abdallah MH, et al. Biofilm Lifestyle in Recurrent Urinary Tract Infections. Life. 2023;13(1):148.
Crossref - Scotland K, Lange D. The link between antibiotic exposure and kidney stone disease. Ann Transl Med. 2018;6(18):371-371.
Crossref - Tasian GE, Jemielita T, Goldfarb DS, et al. Oral Antibiotic Exposure and Kidney Stone Disease. J Am Soc Nephrol. 2018;29(6):1731-1740.
Crossref - Gilbert P, Maira-Litran T, McBain AJ, Rickard AH, Whyte FW. The physiology and collective recalcitrance of microbial biofilm communities. Adv Microb Physiol. 2002;46:202-256.
Crossref - Teichman JMH, Long RD, Hulbert JC. Long-term renal fate and prognosis after staghorn calculus management. J Urol. 1995;153(5):1403-1407.
Crossref - Aggarwal N, Leslie SW, Lotfollahzadeh S. Recurrent urinary tract infections. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan. Updated May 2, 2024.
- Roy R, Tiwari M, Donelli G, Tiwari V. Strategies for combating bacterial biofilms: A focus on anti-biofilm agents and their mechanisms of action. Virulence. 2017;9(1):522-554.
Crossref - Ma H, Bryers JD. Non-invasive determination of conjugative transfer of plasmids bearing antibiotic-resistance genes in biofilm-bound bacteria: effects of substrate loading and antibiotic selection. Appl Microbiol Biotechnol. 2012;97(1):317-328.
Crossref - Hengzhuang W, Wu H, Ciofu O, Song Z, Hoiby N. Pharmacokinetics/Pharmacodynamics of Colistin and Imipenem on Mucoid and Nonmucoid Pseudomonas aeruginosa Biofilms. Antimicrob Agents Chemother. 2011;55(9):4469-4474.
Crossref - Wu H, Moser C, Wang HZ, Hoiby N, Song ZJ. Strategies for combating bacterial biofilm infections. Int J Oral Sci. 2014;7(1):1-7.
Crossref - Herrmann G, Yang L, Wu H, et al. Colistin Tobramycin Combinations Are Superior to Monotherapy Concerning the Killing of Biofilm Pseudomonas aeruginosa. J Infect Dis. 2010;202(10):1585-1592.
Crossref - Antonelli M, De Pascale G, Ranieri VM, et al. Comparison of triple-lumen central venous catheters impregnated with silver nanoparticles (AgTive®) vs conventional catheters in intensive care unit patients. J Hosp Infect. 2012;82(2):101-107.
Crossref - Nelius T. Recent Advances in the Field of Urinary Tract Infections. IntechOpen. 2013.
Crossref - Tenke P, Kovacs B, Jackel M, Nagy E. The role of biofilm infection in urology. World J Urol. 2006;24(1):13-20.
Crossref - Luthje P, Hirschberg AL, Brauner A. Estrogenic action on innate defense mechanisms in the urinary tract. Maturitas. 2014;77(1):32-36.
Crossref - Al-Wrafy FA, Al-Gheethi AA, Ponnusamy SK, Noman EA, Fattah SA. Nanoparticles approach to eradicate bacterial biofilm-related infections: A critical review. Chemosphere. 2021;288(Pt 2):132603.
Crossref - Robino L, Scavone P. Nanotechnology in biofilm prevention. Future Microbiol. 2020;15(6):377-379.
Crossref - Saadat S. AUA 2023: Antimicrobial and Antibiofilm Properties of Chitosan: An Ex-Vivo Study on Kidney Stones. J Urol. 2023.
Crossref - Omar M, Abdulwahab-Ahmed A, Chaparala H, Monga M. Does Stone Removal Help Patients with Recurrent Urinary Tract Infections? J Urol. 2015;194(4):997-1001.
Crossref - Delcaru C, Alexandru I, Podgoreanu P, et al. Microbial Biofilms in Urinary Tract Infections and Prostatitis: Etiology, Pathogenicity, and Combating strategies. Pathogens. 2016;5(4):65.
Crossref - Ciccarese F, Brandi N, Corcioni B, Golfieri R, Gaudiano C. Complicated pyelonephritis associated with chronic renal stone disease. Radiol Med. 2020;126:505-516.
Crossref - Korets R, Graversen JA, Kates M, Mues AC, Gupta M. Post-Percutaneous Nephrolithotomy Systemic Inflammatory Response: A Prospective Analysis of Preoperative Urine, Renal Pelvic Urine and Stone Cultures. J Urol. 2011;186(5):1899-1903.
Crossref - Zhou G, Zhou Y, Chen R, et al. The influencing factors of infectious complications after percutaneous nephrolithotomy: a systematic review and meta-analysis. Urolithiasis. 2022;51(1):17.
Crossref - Streltsova OS, Vlasov VV, Grebenkin EV, et al. Controlled Fragmentation of Urinary Stones as a Method of Preventing Inflammatory Infections in the Treatment of Urolithiasis (Experience in Successful Clinical Use). Sovrem Tekhnologii Med. 2021;13(3):55-61.
Crossref - Zheng C, Yang H, Luo J, Xiong B, Wang H, Jiang Q. Extracorporeal shock wave lithotripsy versus retrograde intrarenal surgery for treatment for renal stones 1-2 cm: a meta-analysis. Urolithiasis. 2015;43(6):549-556.
Crossref - Mugita N, Nambu T, Takahashi K, Wang PL, Komasa Y. Proteases, actinidin, papain and trypsin reduce oral biofilm on the tongue in elderly subjects and in vitro. Arch Oral Biol. 2017;82:233-240.
Crossref - Shin JM, Gwak JW, Kamarajan P, Fenno JC, Rickard AH, Kapila YL. Biomedical applications of nisin. J Appl Microbiol. 2016;120(6):1449-1465.
Crossref - Jiang Y, Zheng W, Tran K, et al. Hydrophilic nanoparticles that kill bacteria while sparing mammalian cells reveal the antibiotic role of nanostructures. Nat Commun. 2022;13(1):197.
Crossref - Zapotoczna M, Forde E, Hogan S, et al. Eradication of Staphylococcus aureus Biofilm Infections Using Synthetic Antimicrobial Peptides. J Infect Dis. 2017;215(6):975-983.
Crossref - Wang Y, Li J, Li X, Shi J, Jiang Z, Zhang CY. Graphene-based nanomaterials for cancer therapy and anti-infections. Bioact Mater. 2022;14:335-349.
Crossref - Cacaci M, Martini C, Guarino C, Torelli R, Bugli F, Sanguinetti M. Graphene Oxide Coatings as Tools to Prevent Microbial Biofilm Formation on Medical Device. Adv Exp Med Biol. 2019;1282:21-35.
Crossref - Ming J, Sun D, Wei J, Chen X, Zheng N. Adhesion of Bacteria to a Graphene Oxide Film. ACS Appl Bio Mater. 2020;3(1):704-712.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.