


ISSN: 0973-7510
E-ISSN: 2581-690X
Diagnosis of Tuberculosis (TB) is a challenging problem with the currently available conventional methods such as microscopy for Acid Fast Bacilli (AFB) and culture techniques.The diagnosis of Extra Pulmonary tuberculosis (EPTB) is still more challenging due to the low yield of bacilli in the clinical specimens. Recently, a chip based Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) was introduced in India. This study was conducted for finding out the sensitivity and specificity of TrueNAT RT-PCR for the diagnosis of Pulmonary and EPTB at a Tertiary Care Hospital in Southern India. A total of 145 samples including both Pulmonary (80) and EPTB (65) were examined by Smear microscopy, culture on Lowenstein Jensen (LJ) medium and TruNat RT PCR. All the positive samples were confirmed by conventional PCR technique as well. Out of 80 Pulmonary samples such as sputum, bronchial wash and tracheal aspirate 41(51.25%) samples were positive in RT-PCR, 22 (27.5%) were positive in microscopy and 29 (36.25%) was positive for culture on LJ medium. Among the 65 EPTB samples such as pus, pleural fluid, Cerebro spinal fluid (CSF), ascitic fluid, Tissue, Peritoneal fluid, Pericardial fluid, Urine, synovial fluid, Fine needle aspiration cytology (FNAC) 38 (58.46%) were positive in RT-PCR, 08 (12.30%) were positive in microscopy and 31(47.69%) were positive for culture on Lowenstein Jensen (LJ) medium.The sensitivity and specificity of TrueNat RT-PCR for the diagnosis of Pulmonary tuberculosis (PTB) is 93.1% and 72.5 % and for EPTB is 96.77 % and 76.4 %, respectively. The newer diagnostic tool has a Turn Around Time (TAT) of less than 2 hours, can detect rifampicin resistance, longer shelf life, cost effective and can work from 2°C to 40°C. It is portable and comes with an inbuilt rechargeable battery which makes it a compatible equipment for any health care setup and out reach programs to detect and treat patients even in remote villages.
Extrapulmonary, Mycobacterium, Pulmonary, RT-PCR, TrueNat.
Tuberculosis is a serious infectious disease and a major public health problem worldwide, causing significant mortality and morbidity in developing countries like India. As per the global TB report 2017 the estimated incidence of TB in India is approximately 28,00, 000 accounting for about a quarter of the world’s TB cases1. Tuberculosis affects primarily the Lung (PTB)and also other parts of the body like Kidney, Urinary tract, joint, Pericardium, Peritoneum, Pleura, Lymph Node, Skin, Tissue, Central nervous system (CNS), Ovaries, Fallopian tubes etc can be involved (EPTB)2.
The chief difficulty with extrapulmonary specimens is the low yield of bacilli and are consequently associated with lower sensitivity in Microscopy and culture. Microscopy is positive in only 10% of EPTB cases whereas culture positivity ranges from 12 to 70% of cases3. The positivity rates of Ziehl-Neelsen smear, culture, and multiplex PCR were 30%, 26.3% and 91.3%, respectively, in confirmed tubercular lymphadenitis patients4 and its diagnosis remains a challenge since granulomatous lymphadenopathy has an extensive differential diagnosis. Several conditions, including sarcoidosis, fungal infections, and other inflammatory conditions, can present the same cytology and/or histopathology as tuberculous lymphadenopathy. A diagnosis of tuberculosis is then confirmed by the presence of AFB and/or isolation of MTB on culture. However, owing to the paucibacillary nature of the specimens, the sensitivity of AFB smear and culture are low; cultures grows mycobacteria in 39 to 80% of cases5.
The diagnosis of Mycobacterium tuberculosis infection is made by conventional methods like microscopy for acid fast bacilli staining and culture on LJ medium and it correlation with clinical presentation, Chest x ray (CXR )and ESR. Though, Acid Fast staining of the sputum smear is considered the gold standard, it has several limitations6. First, high number of bacteria much be present in the sputum to yield a positive report indicating a low sensitivity7; second, it cannot differentiate natural infection and BCG immune infections indicating a low specificity. It is also time consuming and requires technical expertise8.
Culture on LJ medium has a comparatively higher sensitivity and specificity than the smear microscopy. It can distinguish between dead and live bacilli and also helps in determining drug susceptibility. But it is time consuming and takes six to eight weeks. Non Tuberculous Mycobacterium can also grow in the culture medium, so this does not totally meet the clinical requirements9.
Quantiferon TB (TB Gold) though a rapid method is not reliable due to the high cost and its positivity for latent Tb. Molecular methods like conventional PCR and RT PCR has a higher sensitivity and specificity and is capable of detecting 1-100 fg of purified MTB DNA10. PCR as a diagnostic tool for tuberculosis has been studied extensively10-15. The overall reported sensitivity of PCR ranges from 58 to 100 percent. Sensitivity is higher for smear positive TB (95-100%) than smear negative TB (46-63%)12. Specificity of PCR has interlaboratory variations due to the choice of primers, different cross contamination rates and the type of procedure used. The limitations with PCR is the need of an comfortable infrastructure such as air conditioning, uninterrupted power supply, higher cost and the lower shelf life16.
The newer diagnostic tool for MTB introduced by Molbio diagnostics is a mini RT-PCR chip based instrument TrueNAT, has a higher sensitivity and specificity same like existing PCR methods and a lower kit cost and a better shelf life. It is users friendly, no need air conditioned rooms, works from 15°C to 45°C and power interruption is not a problem since it comes with inbuilt rechargeable battery operated system. It is compact and portable17. These make TrueNat an emerging tool in the diagnosis of Tuberculosis.
Study design and population
A prospective cross sectional study was conducted at a tertiary care hospital in southern India from April 2018-April 2019. Patients referred with symptoms suggestive of Pulmonary and Extra Pulmonary Tuberculosis were included in the study. The study was approved by the institutes ethical committee. A total of 80 samples were collected from patients with symptoms suggestive of PTB. Of the samples spot and early morning sputum was collected in 59 patients, 16 were bronchial wash specimen and 5 were tracheal aspirate. A total of 65 EPTB suspected samples like urine, pus, FNAC, pleural fluid, peritoneal fluid, ascitic fluid, Synovial fluid, tissue, pericardial fluid and CSF sent to the Central laboratory were also processed3. Consecutive whole early morning urine were collected in sterile container. It was centrifuged at 3000 rpm for 10 minutes. The sediment was used for microscopy, culture and RT PCR.
A total of 145 clinical samples from both Pulmonary and extra Pulmonary sites were examined by routine smear microscopy for AFB, culture and PCR. The data were compared with the clinical information
Acid fast staining
A direct smear was made from each sample and stained by Ziehl Neelsen staining (ZN) method. The suspect was considered as smear positive TB if atleast one of the two smears were positive by ZN method.
Culture and identification
For culture sputum samples were first decontaminated and concentrated by centri-fugation. 0. 25 ml of the sample is inoculated on to the slants of LJ medium in duplicates. The inoculated LJ medium slants were incubated at 37°C and examined for growth twice weekly for the first 2 weeks and once weekly thereafter up to 8 weeks before reporting as negative. Cultures were considered positive if at least one of the two slants showed growth and culture negative if both the slants showed no growth.
TrueNat RT PCR
PCR was performed using TrueNat chip based mini RT-PCR. The method mini PCR will done in three steps, first step sample preparation, second step DNA extraction and third is amplification. The Trueprep Auto is an electro-mechanical system pre-programmed to sequentially heat, mix and add reagents to the contents of the cartridge placed in the cartridge holder and has a 2-line LCD screen that displays the status. Specimen pre-treated with lysis reagent is added to the the sample chamber of the cartridge which is then placed in the cartridge holder of the device. Sample processing is initiated upon pressing the start button on the device, through an automatic pre-programmed process where in Nucleic Acids released by chemical and thermal lysis of cells bind to the proprietary matrix in the matrix chamber. In subsequent steps, the captured nucleic acids are washed with buffers to remove the PCR inhibitors and finally eluted from the matrix using the elution buffer. At the end the cartridge is automatically ejected and the elute, containing purified nucleic acids is then collected from the elute chamber for further analysis
(Fig. 1, 2).
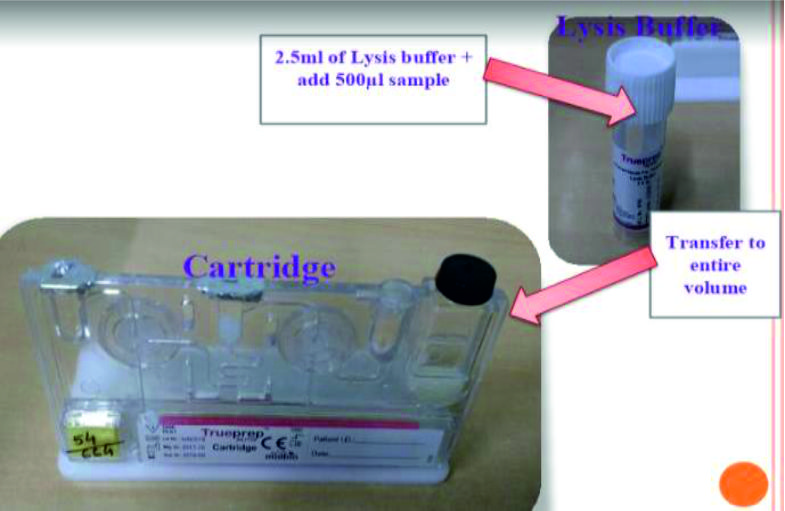 Fig. 1. DNA extraction process
Fig. 1. DNA extraction process Fig. 2. Loading of the chip with elute DNA
Fig. 2. Loading of the chip with elute DNAThe process involves amplifying a specific piece of DNA in a sample using an enzyme called DNA polymerase and periodic cycling of temperature, which anneal and split strands, respectively. With each round of annealing and splitting, the amount of nucleic acid doubles leading to an exponential amplification of the starting trace nucleic acid in a short amount of time. For instance, a typical PCR reaction that runs for thirty-five cycles, at 100% efficiency, will give you
2 35 = 34 billion copies The amplified DNA is then analyzed separately.
Two amplification curves will be obtained on the screen for each test run. Both the target and the internal positive control (IPC) curves will take a steep, exponential path when the fluorescence crosses the threshold value in case of positive samples. The cycle threshold (Ct) will depend on the number of bacterial genomes in the sample. The target curve will remain horizontal throughout the test duration and the IPC curve will take an exponential path in case of negative samples. In case the IPC curve remains horizontal in a negative sample, the test is considered as Invalid. At the end of the test procedure the screen will show DETECTED for Positive sample (Fig. 3) and NOT DETECTED for the negative samples (Fig. 4). The screen will also display Ct value for positive samples.
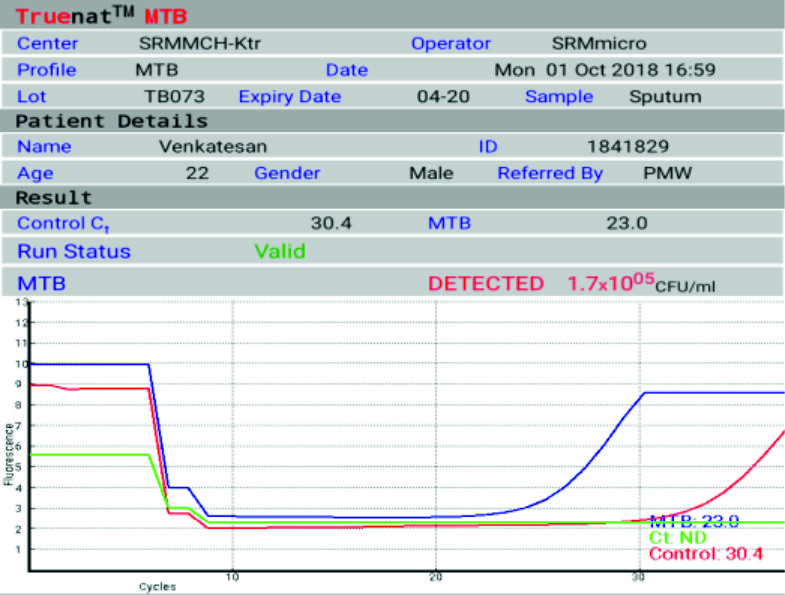
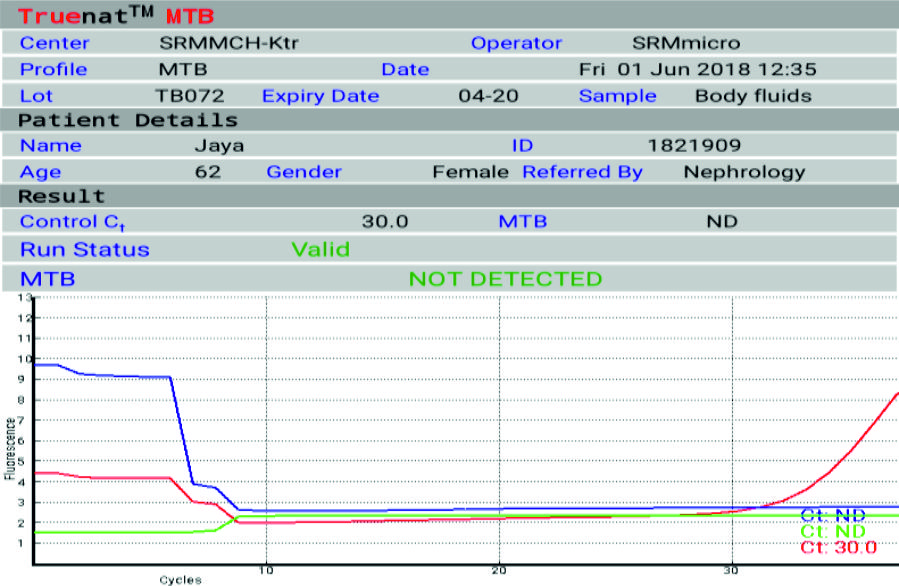 Fig. 3,4. Positive and negative RT PCR outcome
Fig. 3,4. Positive and negative RT PCR outcomeA total of 145 samples from both Pulmonary and extra Pulmonary TB were compared between smear microscopy, culture and RT PCR. Table 1 shows the distribution of various samples with RT PCR results.
Table 2 shows the results obtained from smear microscopy, culture and RT PCR. As evident from Table 2 it is clear that RT PCR has a higher positivity of 51.25% in Pulmonary and 58.46 % in the case of extra Pulmonary tuberculosis when compared to smear microscopy and culture.
Table (1):
Distribution of samples from pulmonary and extra Pulmonary tb and the RT PCR test outcome
Sample |
Total samples (N=145) |
RT PCR Positive |
|---|---|---|
Sputum |
59 |
32 |
Bronchial wash |
16 |
08 |
Tissue |
10 |
03 |
CSF |
12 |
07 |
Pleural fluid |
06 |
03 |
Urine |
14 |
11 |
FNAC |
04 |
02 |
Peritoneal fluid |
01 |
0 |
Synovial fluid |
03 |
02 |
Pericardial fluid |
01 |
0 |
Pus |
11 |
09 |
Ascitic fluid |
03 |
01 |
Tracheal aspirate |
05 |
01 |
Total |
145 |
79 |
Table (2):
Comparison of Microscopy, Culture and RT PCR for Pulmonary and extra Pulmonary samples
Sample |
Pulmonary Tb
(N=80) |
Extra Pulmonary Tb
(N=65) |
|---|---|---|
Microscopy |
22 ( 27.5%) |
08 (12.30%) |
Culture |
29 (36.25%) |
31 (47.69% ) |
RT –PCR |
41 (51.25% ) |
38 (58.46%) |
Considering culture as thr gold standard test the results of Truenat RT PCR was compared for both Pulmonary and extra Pulmonary tuberculosis. The sensitivity and specificity of RT PCR in Pulmonary tuberculosis is 93.1% and 72.5% respectively. SPSS software version 21 was used in making the statistical analysis. (X2 = 42.342) df=1 and p<0.01 showing significant association. TrueNat RT PCR in EPTB has a sensitivity and specificity of 96.77% and 76.4% respectively. (x2=29.7594) df=1, p<0.01 showing significant association. The comparison of RT PCR results with culture in PTB and EPTB is shown in Table 3 and 4.
Table (3):
Comparison of Culture and RT PCR results in Pulmonary Tuberculosis
Pulmonary Tb |
Culture Positive |
Culture Negative |
Total |
|---|---|---|---|
RT PCR Positive |
27 |
14 |
41 |
RT PCR Negative |
02 |
37 |
39 |
Total |
29 |
51 |
80 |
Out of the 80 RT PCR positive samples conventional PCR was negative in 2. Out of the 3 culture negative RT PCR positive samples all the three were positive by conventional PCR.
Table (4):
Comparison of Culture and RT PCR results in Extra Pulmonary Tuberculosis
Pulmonary Tb |
Culture Positive |
Culture Negative |
Total |
|---|---|---|---|
RT PCR Positive |
30 |
08 |
38 |
RT PCR Negative |
01 |
26 |
27 |
Total |
31 |
34 |
65 |
Early and accurate diagnosis of tuberculosis infection is important to prevent the emergence of resistance and to initiate treatment. Currently available conventional diagnostic methods includes smear microscopy for ZN staining and culture on LJ medium. Though smear microscopy is low cost and easy to perform it has poor sensitivity and distinct specificity.
Culture is the gold standard test with good sensitivity and specificity but takes 2-4 weeks and drug susceptibility testing even longer. The conventional methods lacks sensitivity and specificity in EPTB due to the low bacillary load and uneven distribution.
The exact diagnostic role of PCR assay for M. tuberculosis in high-prevalence areas for tuberculosis has to be assessed in appropriate control groups, particularly in the case of extrapulmonary tuberculosis. But PCR has several limitations like high cost, shorter shelf life, need for a sophisticated infrastructure and technical expertise. In contemporary practice, clinicians neither start nor stop treatment solely on PCR results. So there is need for a rapid test in the diagnosis of TB. Taking this into account, this study was conducted to evaluate the role of the multipurpose mini RT-PCR instrument in the diagnosis of Pulmonary and extrapulmonary tuberculosis. Another method currently used method is CB NAAT (Cartridge based nucleic acid amplification technique)though has a turn around time of <2 hours is very costly. True Nat PT PCR is cheaper, TAT of <1 hours, and less than 2 hours to detect Rifampicin resistance, better shelf life, compact, closed cartridge system so there is no false positive results from contaminating saprophytic Mycobacteria.
Among the 145 samples included in the study TrueNat RT PCR was positive in a total of 79 patients (54.48%) whereas microscopy and culture was positive in only 6.2% and 41.3% respectively. Among the pulmonary samples Sputum The low positive values in smear microscopy could be due to the paucibacillary nature of extra Pulmonary samples. This results obtained are in concordance with other studies18,19). The sensitivity and specificity for PTB and EPTB obtained in our study are in concordance with a study done by
Nikam et al.
We show here that mini RT-PCR would be particularly useful for the diagnosis of both Pulmonary and extrapulmonary tuberculosis in patients where the provisional diagnosis of tuberculosis is made on the basis of clinical presentation and conventional microbiological examination without evidence of AFB. Mini RT-PCR methodology was found to be highly suitable for processing fluid and tissue samples and completely compatible with AFB detection, culture, and conventional PCR. The strengths of this technology included (i) the ability to apply smear microscopy, culture, and conventional PCR tests on the same sample aliquot and (ii) its efficiency and robustness given the scanty amounts of tissue and the proteinaceous (coagulum-laden) nature of pleural fluid that were often obtained. The limitation with TrueNat MTB is that it cannot determine MDR-TB, which is of most significance in high burden countries like India.
Acknowledgements
None.
Conflict Of Interest
The authors declare that there is no conflict of interest.
Authors’ Contribution
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Funding
None.
Data Availability
All datasets generated or analyzed during this study are included in the manuscript.
Ethics Statement
The study was approved fro the institutes ethical committee (1144/IEC/2017).
- World Health Organization. Global tuberculosis control: surveillance, planning, financing. World Health Organization, Geneva, Switzerland. [Online. ] W. H. O. /CDS/TB/2002. 295. http://www. who. int/gtb/publications/globrep02/index. html
- Aggarwal A.N., D. Gupta and S.K. Jindal. Diagnosis of tubercular pleural effusion. Indian J. Chest Dis. Allied Sci. , 1999; 41: 89–100.
- Sharma K., Gupta N., Sharma A. et al. Multiplex polymerase chain reaction using insertion sequence 6110(IS6110) and mycobacterial protein fraction from BCG of Rm 0.64 in electrophoresis target genes for diagnosis of tuberculous lymphadenitis. Ind jrnl of Med Microbio. 2013;31:24-28.
- Appling D. and R.H. Miller. Mycobacterial cervical lymphadenopathy: 1981 update. Laryngoscope, 1981; 91: 1259–1266.
- Baek C.H. S.I. Kim Y.H. Ko and K.C. Chu. Polymerase chain reaction detection of Mycobacterium from FNA for diagnosis of cervical tuberculosis. Laryngoscope, 2000; 110: 30–34.
- F.A. Al-Zamel “Detection and diagnosis of Mycobacterium tuberculosis,” Expert Review of Anti-Infective Therapy, 2009; 7(9) pp. 1099–1108.
- P. Sule, R. Tilvawala, P. Behinaein, G.K. Walkup, and J.D. Cirillo “New directions using reporter enzyme fluorescence (REF) as a tuberculosis diagnostic platform,” Tuberculosis, 2016; 101(supplement.): pp. S78–S82.
- Y.J. Lee, S. Kim, Y. Kang et al., “Does polymerase chain reaction of tissue specimens aid in the diagnosis of tuberculosis?” Journal of Pathology and Translational Medicine, 2016; 50(6): pp. 451– 458.
- Soini H., Musser J.M. Molecular diagnosis of mycobacteria. Clin Chem., 2001; 47(5).
- Brisson-Noכl A., Gicquel B., Lecossier D. et al. Rapid diagnosis of tuberculosis by amplification of (mycobacterial DNA in clinical samples. Lancet, 1989; 13(4): 1069 –71.
- Claridge J.E., Shawar R., Shinnick T.M., Plikaytis B.B. Large (scale use of polymerase chain reaction in a routine 14. mycobacteriology laboratory. J. Clin. Microbiol., 1993; 31: 2049-56.
- Noordhoek G.T., Van Embden J.D., and Kolk A.H. Reliability (of nucleic acid amplification for detection of Mycobacterium tuberculosis: an international collaborative quality control study among 30 laboratories. 15. J. Clin Microbiol., 1996; 34: 2522-2525.
- Della-Latta P., and Whittier S. Comprehensive evaluation (of performance, laboratory application and clinical usefulness of two direct amplification technologies for 16. the detection of Mycobacterium tuberculosis complex. Am. J. Clin. Pathol., 1998; 110: 301-310. (
- Wang S.X., and Tay L. Evaluation of three nucleic acid (amplification methods for direct detection of Mycobacterium tuberculosis complex in respiratory 17. specimens. J. Clini. Microbiol., 1999; 37: 1932-34.
- Kambashi B., Mbulo G., McNerney R. et al. Utility of nucleic acid amplification techniques for the diagnosis of pulmonary tuberculosis in sub-saharan Africa. Int J. Tuberc 18. Lung Dis., 2001; 5: 364-369.
- MMWR Centers for Disease Control and Prevention. Update: nucleic acid amplification tests for tuberculosis. Morb. Mortal Wkly Rep., 2000; 49: 593–594.
- C. Nikam, M. Jagannath, M.M. Narayanan, et al., Rapid diagnosis of Mycobacterium tuberculosis with TrueNat MTB: a near-care approach, PLoS One, 2013; 8 (1): e51121.
- M.R. Purohit, T. Mustafa, H.G. Wiker, O. Morkve, L. Sviland. Immunohistochemical diagnosis of abdominal and lymph node tuberculosis by detecting Mycobacterium tuberculosis complex specific antigen MPT64. Diagn. Pathol., 2007;2:36
- M.R. Purohit, T. Mustafa, H.G. Wiker, L. Sviland. Rapid diagnosis of tuberculosis in aspirate, effusions, and cerebrospinal fluid by immuno-cytochemical detection of Mycobacterium tuberculosis complex specific antigen MPT64. Diagn. Cytopathol., 2012; 40(9): 782–91.
- Nikam C., Jagannath M., Narayanan M.M., Ramanabhiraman V., Kazi M., Shetty A., et al. Rapid Diagnosis of Mycobacterium tuberculosis with Truenat MTB: A Near-Care Approach. PLoS ONE, 2013; 8(1): e51121.
© The Author(s) 2019. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.