


ISSN: 0973-7510
E-ISSN: 2581-690X
Currently, the sole global concern is recurring waves of the COVID-19 virus that began in 2020 and is ongoing. This study aimed to compare the trends of COVID-19 infections in Egypt during the different waves. We calculated the COVID-19 positivity rate between March 2020 and the fourth week of April 2021 among those tested at the Reference Laboratory of the Egyptian University Hospitals. We then compared our results with those obtained from the WHO and the Egyptian Ministry of Health and Population websites. A dramatic increase in the positivity rate was observed during May and June 2020 (26.35% and 33.11%, respectively). This was followed by an abrupt reduction in July (11.7%), and flattening until a second increase was noted during November (9.6%), which reached its peak during December (17.8%). However, after the figures declined during January 2021, they began to rise again in February 2021 and continued to increase until the end of April 2021, simulating the first wave data. The analysis of the COVID-19 growth rate from April 1st to the 25th, 2021 revealed a slight downward trend in new cases. Data from both the WHO and the Egyptian Ministry of Health and Population websites showed similar patterns to our results. The third wave of COVID-19 started in Egypt. Analyzing future data can aid in forecasting the COVID-19 epidemic and allow us to use foresight to enact effective measures and strategies to keep this virus under control.
COVID-19, Egypt, Third wave, Forecasting, Growth rate
Coronavirus disease 19 (COVID-19) is an extremely contagious and pathogenic viral infection induced by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which arose in Wuhan, China and spread worldwide1. The World Health Organization (WHO) proclaimed the disease a pandemic on the 11th of March 20202. By that time, there were more than 118,000 cases in 114 countries with 4,291 deaths. The pandemic is surging through the majority of countries globally, showing the strongest effects in the United States of America (USA), India, Brazil, and certain European countries such as Italy, Spain, France, Germany, and the United Kingdom (UK)3.
All of these countries have reported more cases and deaths than the country of origin (China) in relation to this virus. By November 2020, there were approximately 55 million asserted cases of COVID-19 worldwide, and more than 1,300,000 deaths, with a mortality rate of 2.43%4.
The spread also included Egypt, with a total number of confirmed cases by November 2020 of greater than 110,000 and approximately 7,000 deaths, with close to a 6% death rate5. From the middle of March to the first week of April 2020, the death rate ranged from 10% to 15%. The death rate declined to 1%–2% from the beginning of May until the middle of November 20206.
COVID-19 diagnosis is based on the clinical and epidemiological history of the patient, in addition to the findings of ancillary examinations, for example, a chest X-ray and chest tomography reveal the characteristic images of ground glass that are also visible in asymptomatic patients. However, the main method of COVID-19 diagnosis is the identification of SARS-CoV-2 RNA in respiratory samples by nucleic acid analysis7.
There is heightened anxiety over the re-emergence of COVID-19 cases among communities. The concern over a “second wave” of the pandemic is widespread. A double-peaked epidemic curve was reported in the “Spanish flu” pandemic, and in the current COVID-19 crisis, a recurring rise in the incidence rate has been noticed in many countries. In Japan, a crisp two-peak incidence curve was evident, and similar trends have been reported in other countries8.
The concept of epidemics normally possessing two peaks of novel cases over time is widely accepted, although epidemiologists have not characterized this pattern as an established model. Generally, the resumption of international travel or the lessening of community control measures is the reason for the reappearance of disease incidence8.
Considering the relatively high case fatality rate during the first peak of the COVID-19 pandemic, we focus on how to predict a new wave to enable our health system to prepare and increase community awareness. Therefore, we aimed to estimate the positivity rate of COVID-19 cases from March 1, 2020, to April 25, 2021, and to compare the results of COVID-19 infection in the Reference Laboratory of the Egyptian Universities’ Hospitals (RLEUH) with those from the WHO and the Egyptian Ministry of Health and Population (MOHP) websites. We also aimed to compare the trend of COVID-19 infections in Egypt during the different waves beginning with the era preceding the first wave, through the first and second waves to the start of the third wave to aid in the prediction of future outbreaks.
Population of study
This was a cross-sectional study. All individuals who attended the RLEUH for COVID-19 RT-qPCR testing were included in the study. Data regarding the number of COVID-19 positive cases in Egypt were collected from the WHO and Egyptian MOHP websites. The study was approved by the Ethics Committee of the Supreme Council of University Hospitals 2020.
Clinical specimens and RT-qPCR
Nasopharyngeal swab specimens were collected from all individuals over a period of 61 weeks from the beginning of March 2020 to the fourth week of April 2021. Diagnosis of COVID-19 was performed by RT-qPCR using the automated Abbott m2000 Real Time System. First, sample preparation was performed using the Abbott m Sample Preparation System DNA and Abbott m2000 sp instrument (Abbott, Germany) followed by amplification and detection of COVID-19 RNA using the Abbott RealTime SARS-CoV-2 Assay with the Abbott m2000rt analyzer (Abbott, Germany) by targeting the RNA-dependent RNA polymerase (RdRp) and N genes. The entire process was automated and performed according to the manufacturer’s instructions.
Data collection
Data regarding COVID-19 in Egypt were obtained from the WHO and Egyptian MOHP websites.
Statistical analysis
Data were analyzed using Microsoft Excel. Frequency (count) and relative frequency (percentage) were used as categorical data. Comparisons between categorical data were performed using the chi-square (X2) test. Statistical significance was set at P ≤ 0.05.
In the present study, a total of 198,493 nasopharyngeal swabs were obtained from attendees at RLEUH over a period of 14 months from the beginning of March 2020 until the fourth week of April 2021. The participants aged from 0 to 85 years.
The study showed that the number of participants increased from 850 in March 2020 to 20,424 in June 2020. However, it reduced to 9,011 in September, followed by a second increase to 10,588 in October, reaching its peak at 20,578 during December 2020. A third, higher peak was observed in March 2021. Despite the reduction in the number of attendees from July to September, the total number subjected to COVID-19 PCR examination increased throughout the years 2020 and 2021 (Fig. 1 and 2) (Table 1).
Table (1):
The COVID-19 PCR positivity rates from March 2020 to April 2021.
Months |
Number of Attendees |
Positive Cases |
Positivity rate |
|---|---|---|---|
March 2020 |
850 |
4 |
4.71% |
April 2020 |
1598 |
184 |
11.50% |
May 2020 |
8432 |
2222 |
26.35% |
June 2020 |
20424 |
6762 |
33.11% |
July 2020 |
12692 |
1485 |
11.70% |
August 2020 |
10491 |
511 |
4.87% |
September 2020 |
9011 |
432 |
4.80% |
October 2020 |
10588 |
603 |
5.70% |
November 2020 |
14719 |
1436 |
9.6% |
December 2020 |
20578 |
3667 |
17.8% |
January 2021 |
22633 |
2425 |
10.71% |
February 2021 |
18839 |
1456 |
7.72% |
March 2021 |
25821 |
2253 |
8.72% |
April |
21817 |
2370 |
10.86% |
Total |
198493 |
25810 |
13.00% |
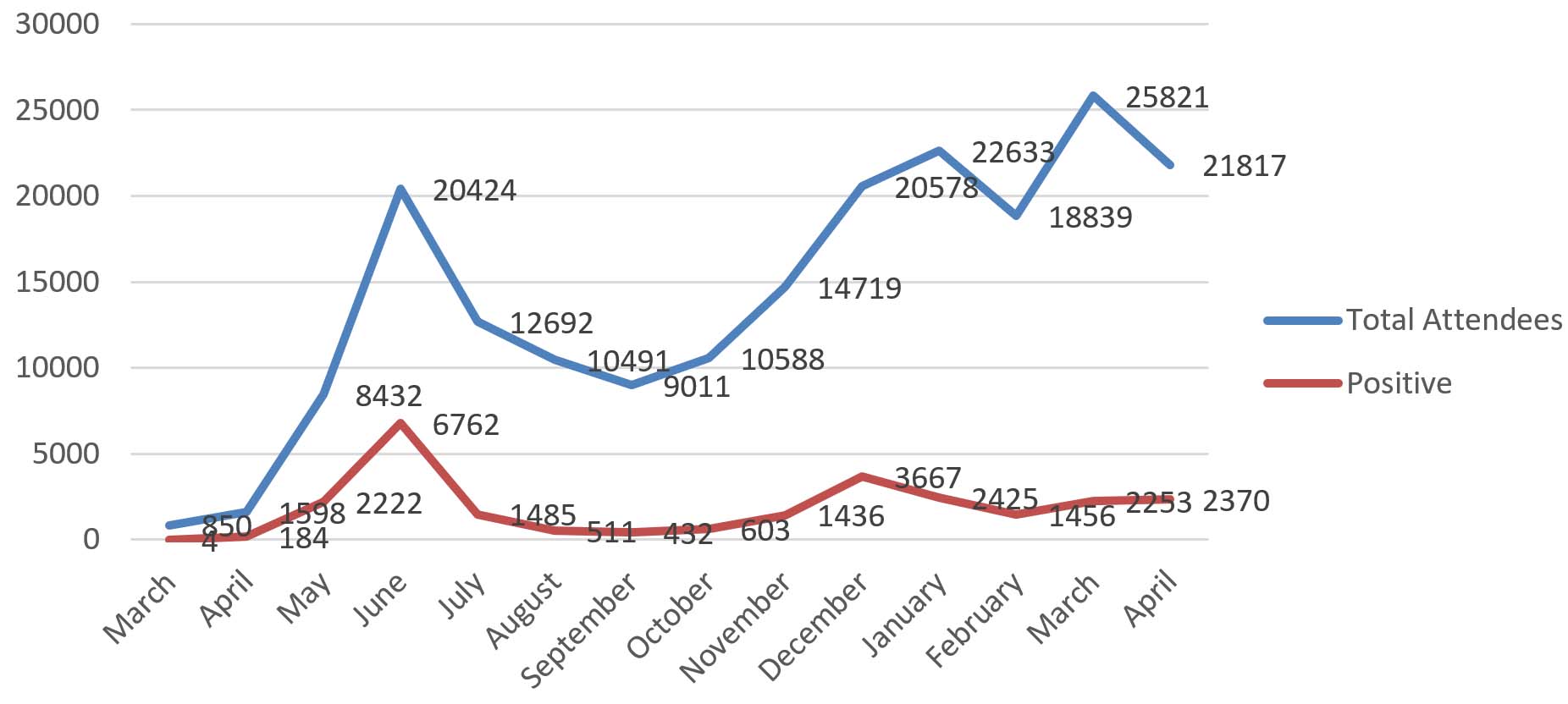
Fig. 1. The number of attendees and positive COVID-19 PCR cases in the Reference Laboratory of the Egyptian Universities’ Hospitals from March 2020 to April 2021
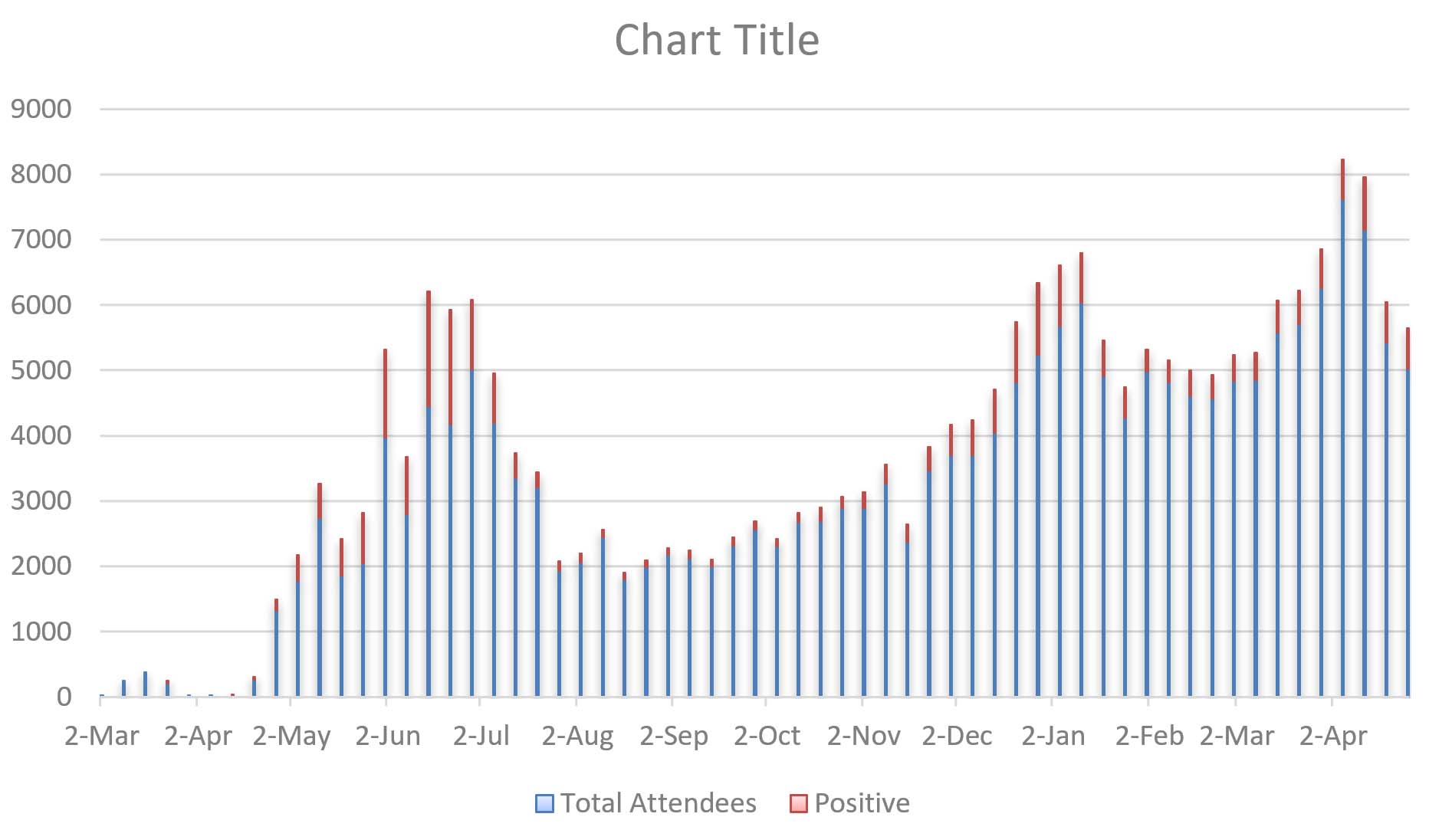
Fig. 2. The weekly changes in the number of attendees and the number of positive COVID-19 PCR cases in the Reference Laboratory of the Egyptian Universities’ Hospitals over a period of 61 weeks
The positivity rates of COVID-19 RNA throughout the study period are shown in Fig. 1. A dramatic increase in the positivity rate was observed during the months of May and June (26.35% and 33.11%, respectively). This was followed by an abrupt reduction in July (11.7%), and a leveling from August through October (ranging from 4% to 6%). A noticeable second increase occurred during November (9.6%), which continued into December 2020 (17.8%); however, the numbers decreased in January 2021 (10.71%) to reach a minimum in February 2021 (7.72%). Unfortunately, a third wave was observed during March and April 2021, which was still in play at the time of this study. The chi-square test of independence was performed to examine the relationship between sex and the risk of COVID-19 infection. We found a statistically higher positivity rate among women compared to men (14.5% [9,335/64,197] vs. 12.26% [16,475/134,296], p < 0.001), despite the higher number of men than women participating.
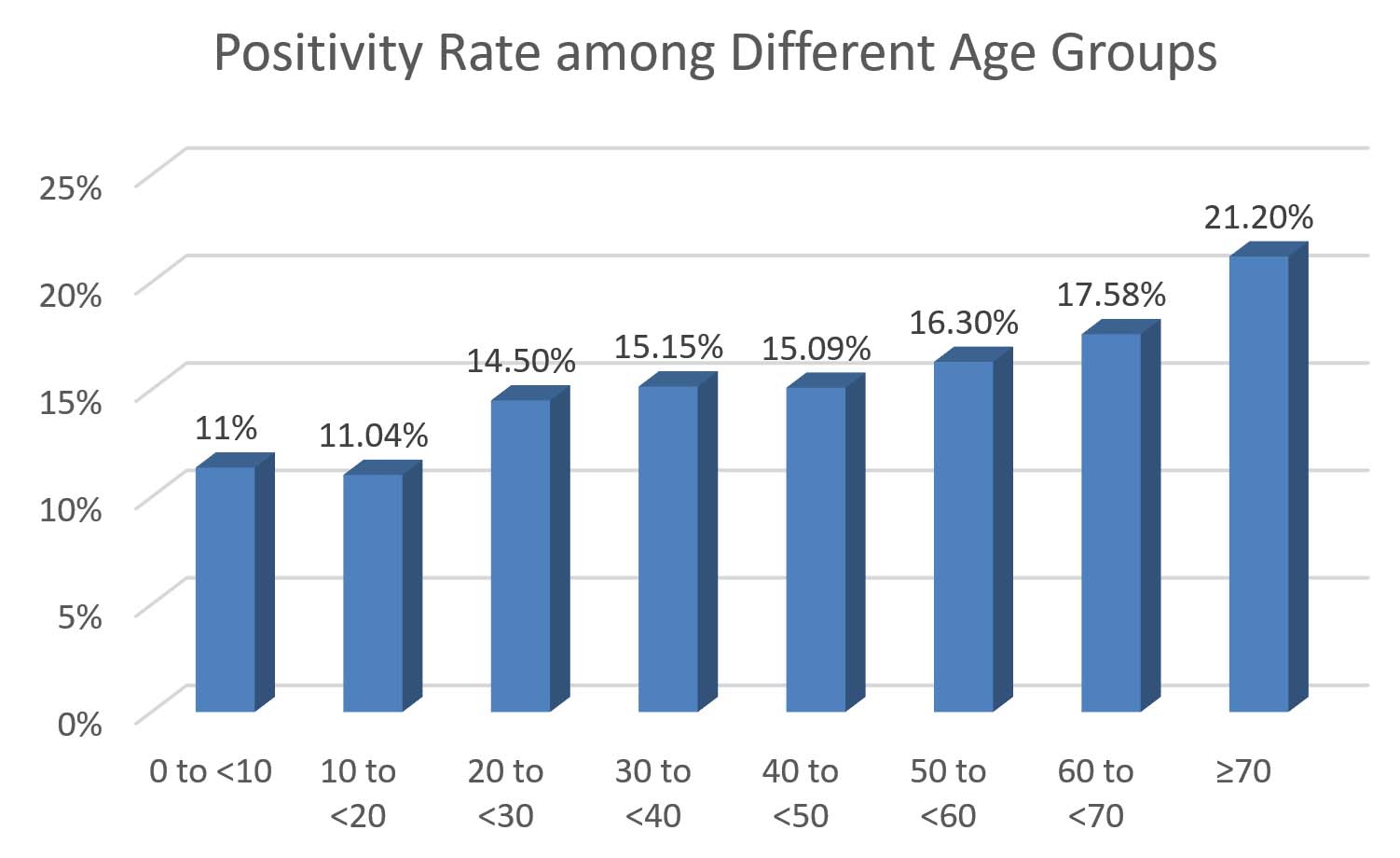
Fig. 3. COVID-19 PCR positivity rate among different age groups
The positivity rate of COVID-19 was higher among attendees above 70 years of age (21.2%), followed by those between 60 and 70 years (17.58%), while the lowest rate of positivity (11%) was found among those less than 20 years old. Fig. 3 shows that the risk of infection with COVID-19 increases with age. We divided the participants into three age groups: group 1, 0 to <20 years old; group 2, 20 to < 60 years; and group 3, 60+ years. We found that the risk of infection was significantly higher in group 3 (18.85%) than in group 2 (15.2%) and group 1 (11.15%), p < 0.001.
We studied the COVID-19 positivity rates among different nationalities. The highest rates were among people from Turkey (26%) and China (22.4%), followed by India (14.9%), and Thailand (12.9%). The lowest rates were among the Sudan (0.6%), the United Arab Emirates (0.9%), Jordan (1%), Nigeria (1.3%), and Kuwait (1.7%). The data are shown in Fig. 4.
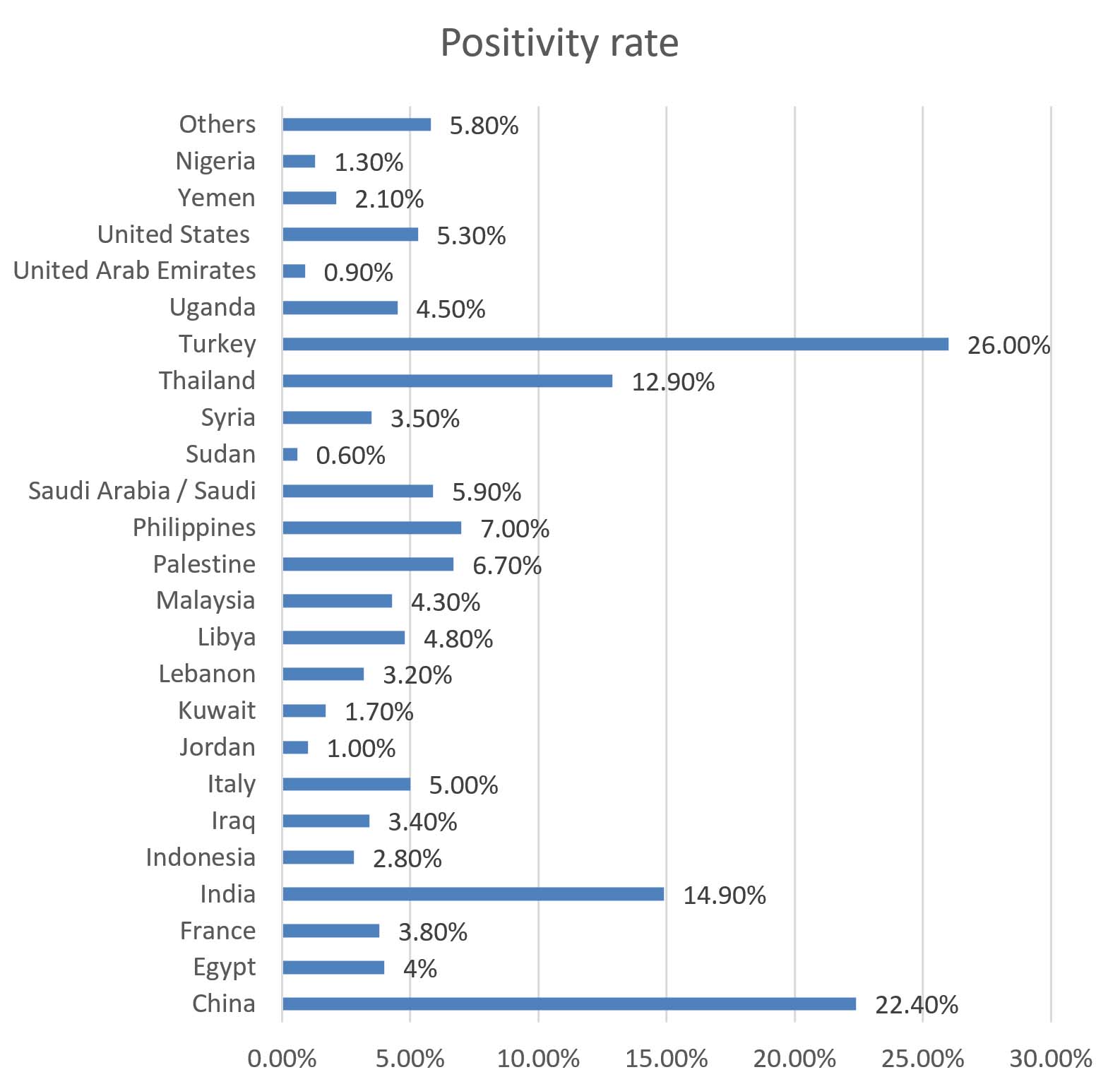
Fig. 4. COVID-19 PCR positivity rates among different nationalities
The COVID-19 PCR positivity rate was significantly lower among Egyptians (4%) than among non-Egyptians (21.6%) (p <0.001).
We calculated the growth rate of COVID-19 infections over a period of 18 days from April 1st to 25th, 2021 (Fig. 5). The lowest growth rate occurred on the 12th of April (-0.42), while the highest was on the 17th of April (0.43). We observed a slight downward trend in new COVID-19 cases during this period.
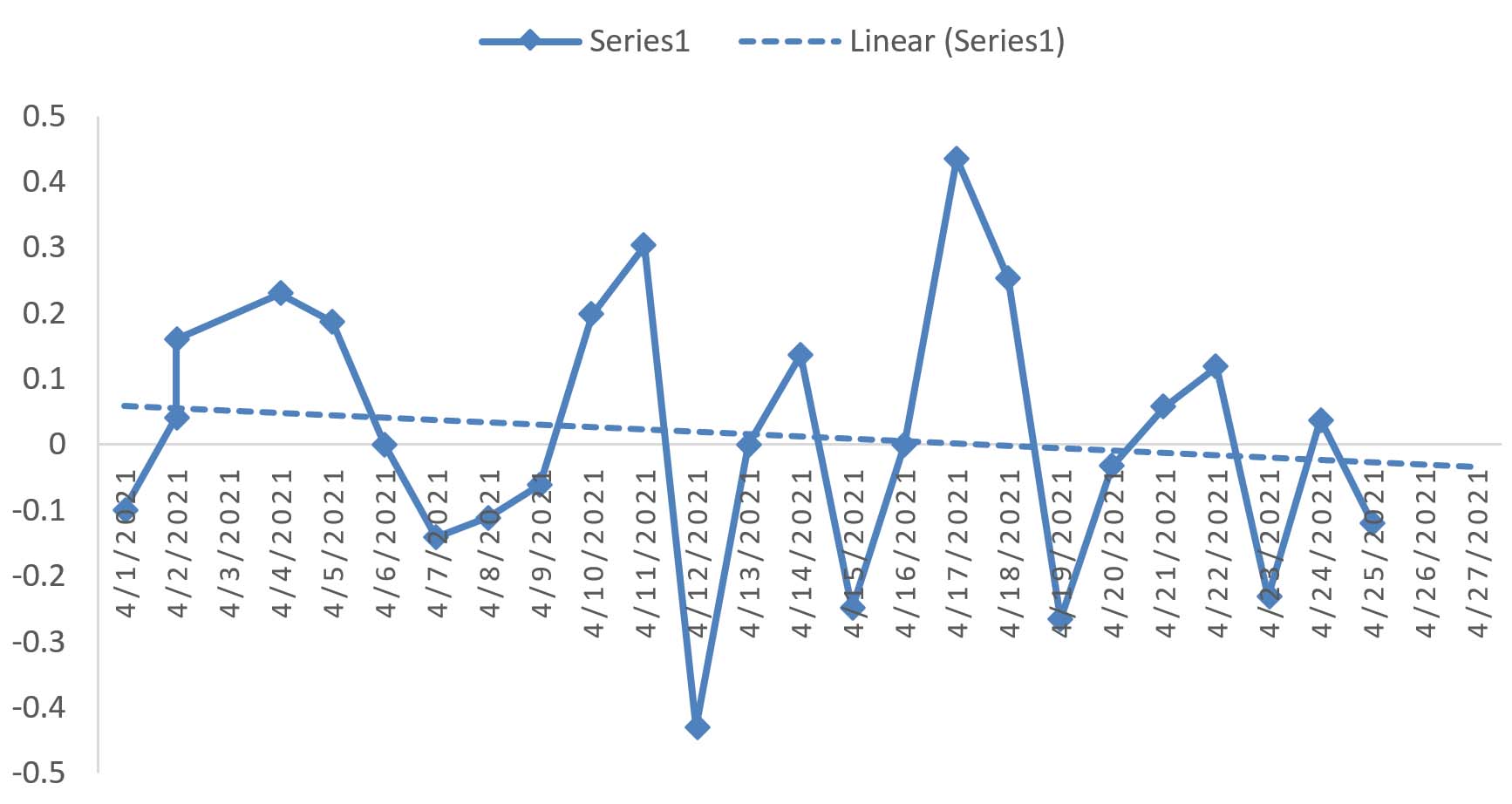
Fig. 5. The COVID-19 growth rate over a period of 25 days from the 1st to the 25th of April 2021
Data Collection from the WHO and the Egyptian MOHP
By searching the WHO and MOHP websites, we found that by May 1st, 2020, the total number of confirmed cases was 226,531, while the total number of deaths was 13,278. Data from both websites show that the highest infection rates of the first pandemic wave were detected during May and June, followed by a rapid reduction in July (Fig. 1). Despite the increase in the total number of confirmed cases from October 2020 to April 2021, the number of deaths did not increase to the same extent as that during the first wave. The peak of the second wave in Egypt was lower than that of the first wave for both the reported confirmed cases and the total deaths9. However, the peak in the number of deaths did not decrease in correlation with the number of positive cases in the third wave.
The present study showed that the number of positive cases among the attendees at RLEUH exhibited an increasing pattern, reaching its peak in June 2020, after which time the numbers declined to remain constant until the end of October 2020. The cases then surged to form a second peak in December 2020. Despite the positivity rate declining during January and February 2021, it began escalating by March 2021, signaling the beginning of the third wave. Although the rise and fall of both the total attendees and positive cases coincided, the peak of total participants was higher than that of the positive cases. This pattern can be attributed to the fact that travelers to other countries who undergo the COVID-19 PCR currently outnumber those with symptoms of the virus.
The transmission pattern of COVID-19 was classified as “clusters of cases.” Similar to our results with the RLEUH, data from both the WHO and MOHP websites indicate that the first wave exhibited the highest infection rates4.
The second increase occurring from November 2020 to January 2021 could be attributed to the start of the winter season in Egypt, as a significant negative correlation has been found between temperature and the incidence of COVID-1910. Another possible explanation could be the return of students after the reopening of schools and universities. The decline in the positive cases noticed during January coincided with the government’s decision to close schools and universities, cancel examinations, and shift to the online learning system, which assisted in minimizing the positivity rate11. Unfortunately, resumption of the second semester in Egyptian schools on March 13th correlated with a third increase in positive cases12. In our opinion, it is difficult to force children to adhere to the social distancing and mask-wearing policies; therefore, online learning appears to be an effective way to address this challenge, but we have no statistical evidence to support this.
According to the Egyptian MOHP, Egypt ranks 69th in the number of COVID-19 infections among 215 countries worldwide. It ranks 160th in terms of the total number of infections per 1 million citizens compared to the rest of the world. Egypt has a recovery rate of 75.0%, which is 188th, and a death rate of approximately 5.9%, ranked 8th globally9.
The start of the second wave in Egypt came later than in Europe, which could be related to the delayed start of the epidemic in Egypt than other countries13.
The second increase in the number of confirmed COVID-19 positive cases in October, November, and December 2020 was not accompanied by a rise in the number of deaths as was reported by the Africa Centres for Disease Control and Prevention (Africa CDC)14. The director of this organization and other researchers have proposed a number of reasons for this phenomenon: (1) the relatively young population in Egypt (over 60%) are below the age of 25 and are less likely to manifest symptoms of the virus, and (2) the use of infection control measures that prevent other ailments, such as secondary bacterial infections, cross-immunity from other coronaviruses, and lower rates of travel15-17. Another potential explanation is the free compulsory BCG vaccination instituted in Egypt against tuberculosis. Since it is efficient against similar viruses, it is postulated that the immune response boosting effect of this vaccine may also offer protection against SARS-CoV-2 infection. A study by Hussein et al. supports the fact that the BCG vaccination may have a protective role in avoiding severe/critical SARS-CoV-2 pneumonia and thereby decrease fatalities. Moreover, the partial lockdown imposed in Egypt may have aided in inducing an immune response among the population against COVID-19, decreasing the severity of the symptoms during the beginning of the second wave, before the appearance of new virus mutations and/or the waning of immunity18.
The peak in the number of deaths did not decrease in correspondence with the number of third-wave positive cases, which can be explained by the mutations found by multiple researchers. Zekri et al. studied the COVID-19 genomic sequence in Egyptian isolates, and similar to other countries worldwide, they detected 204 unique sequence variations19. Although the Egyptian Ministry of Health declared the absence of the double mutated strain originating in India20, future studies adopted by the WHO for tracking, detecting, and monitoring variants could reveal mutations incriminated in high mortality rates. Sallam et al. detected the D614G mutation of SARS-CoV-2 in countries of the Middle East and North Africa, including Egypt21. This mutation has proven its ability to increase both the infectivity and fatality rate, as revealed in previous studies22,23.
Egypt has started a program of mass population vaccination, which could play a pivotal role in decreasing the number of infected individuals or minimizing the severity of the virus20.
We found a statistically significant higher positivity rate of COVID-19 among women than men, which corroborates a study by Mostafa et al. in 2020 from Egypt24. This can be explained by the higher rate of exposure among men that could result in asymptomatic infections, accompanied by repeated exposure to low viral loads, providing men with more effective immunity than women.
When reviewing the data in terms of age the highest COVID-19 positivity rate was found in those over 70 years of age while those below 20 years exhibited the lowest positivity rate. These findings are consistent with those reported by Kalantari et al.25 Similarly, the WHO has published guidance on COVID-19 for the care of older people who are more susceptible to infection and the risk of becoming severely ill26. The low positivity rates of COVID-19 infection among younger people have been attributed to one or more childhood vaccinations, such as the BCG vaccine, as mentioned previously.
We studied the COVID-19 positivity rates among different nationalities, and found that the rate was significantly lower among Egyptians (4%) than non-Egyptians (21.6%). Egypt has different population demographics than other countries, particularly regarding life expectancy and population age, the latter being a known risk factor for symptomatic COVID-19 infections27.
After the confirmed diagnosis of the first case of COVID-19 in Egypt on February 14, 2020, that country declared the beginning of the COVID-19 epidemic in March 202028, and the Egyptian government did not underestimate the problem, taking certain restrictions as a part of early mitigation procedures to contain the situation, limit transmission, and increase recovery13. Schools and universities were closed on March 7 and mosques on March 2129. The Egyptian government has imposed different forms of lockdowns, enforced a night-time curfew, and banned all large community events and gatherings until further notice30. As the number of cases began to decrease, these facilities were allowed to operate at a limited capacity with mandatory mask-wearing, and fines were imposed on those who did not adhere to the rules31.
As a crucial part of the mitigation procedure and in accordance with the WHO guidelines, all Egyptian authorities began social awareness campaigns for citizens regarding COVID-19. The goal of these campaigns was to propagate the practices of personal hygiene among the public and urge them to stay home for safety reasons. The media also conducted awareness campaigns on preventative measures through informative messages to minimize the number of new cases30.
Our findings have confirmed that the efforts made by the government were successful in delaying and limiting the spread of COVID-19 in Egypt. This was demonstrated by the slow rise in positive cases, until May when there was a rapid increase coinciding with the loosening of lockdown measures during Ramadan. However, the abrupt decline in numbers might also be attributed to the increased compliance with physical distancing and other mitigation measures in place since March 202028.
Based on past experience, the Egyptian government successfully predicted the occurrence of the third wave during Ramadan 202132.
We calculated the growth rate of COVID-19 infections over the period from April 1st to the 25th, and noticed a slight downward trend in COVID-19 infections during this time. To successfully address this situation, it is crucial to continuously adhere to containment measures, including infection control, health education, and population awareness, and the health system and facilities must prepare for ongoing numbers of cases and deliver appropriate diagnostic, therapeutic, and preventive measures30.
This study summarizes the present situation of the COVID-19 epidemic in Egypt, allowing foresight for effective prevention and control measures to keep this epidemic under control, along with appropriate lockdown-exit strategies. Moreover, analyzing future data using statistical time series techniques can aid in the establishment of statistical models for forecasting the activity of the COVID-19 epidemic.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
ETHICS STATEMENT
The study was approved by the Ethics Committee at the Supreme Council of University Hospitals 2020.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript.
- Oliveira BA, Oliveira LA, Sabino EC, Okay TS. SARS-CoV-2 and the COVID-19 disease: a mini review on diagnostic methods. Rev Inst Med Trop Sao Paulo. 2020;62:e44.
Crossref - WHO Director-General’s opening remarks at the media briefing on COVID-19 – 11 March 2020. Accessed 5 January 2021. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020
- Coronavirus Worldwide Graphs. https://www.worldometers.info/coronavirus/worldwide-graphs/#countries-cases. Accessed 7 December 2020.
- WHO Coronavirus Disease (COVID-19) Dashboard. https://covid19.who.int/. Accessed 1 May 2021.
- WHO Coronavirus Disease (COVID-19) Dashboard, Egypt. https://covid19.who.int/region/emro/country/eg. Accessed 1 May 2021.
- Coronavirus Worldwide Graphs. https://www.worldometers.info/coronavirus/worldwide-graphs/#total-deaths. Accessed 1 May 2021.
- Naserghandi A, Allameh SF, Saffarpour R. All about COVID-19 in brief. New Microbe and New Infect. 2020;35:100678.
Crossref - Pedro SA, Ndjomatchoua FT, Jentsch P, Tchuenche JM, Anand M, Bauch CT. Conditions for a Second Wave of COVID-19 Due to Interactions Between Disease Dynamics and Social Processes. Front Phys. 2020;8:574514.
Crossref - Egyptian MOHP, Egyptian statistics. https://www.care.gov.eg/EgyptCare/Index.aspx. Accessed 28 January 2021
- Rosario DKA, Mutz YS, Bernardes PC, Conte-Junior CA. Relationship between COVID-19 and weather: Case study in a tropical country. Int J Hyg Environ Health. 2020;229:113587.
Crossref - Morsy A. Egypt cancels in-class education, postpones first-term exams amid coronavirus concerns 2020. http://english.ahram.org.eg/NewsContent/1/64/397893/Egypt/Politics-/UPDATED-Egypt-cancels-inclass-education,-postpones.aspx. Accessed 28 January 2021.
- https://www.egypttoday.com/Article/1/99778/Egypt-s-Health-Ministry-denies-Education-Ministry-s-appeal-to. Accessed 2 May 2021.
- Hasab AA, El-Ghitany EM, Ahmed NN. Situational Analysis and Epidemic Modeling of COVID-19 in Egypt. Journal of High Institute of Public Health. 2020;50(1):46-51.
Crossref - African CDC African Union and Africa CDC, 2020. Coronavirus Disease 2019 (COVID-19). Latest Updates on the COVID-19 Crisis from Africa CDC. https://africacdc.org/covid-19/. Accessed 6 January 2021.
- Njenga MK, Dawa J, Nanyingi M, et al. Why is There Low Morbidity and Mortality of COVID-19 in Africa? Am J Trop Med Hyg. 2020;103(2):564-569.
Crossref - Lone SA, Ahmad A. COVID-19 pandemic – an African perspective. Emerg Microbes Infect. 2020;9(1):1300-1308.
Crossref - Lawal Y. Africa’s low COVID-19 mortality rate: A paradox? Int J Infect Dis. 2021;102:118-122.
Crossref - Hussein AARM, Salem MR, Salman S, et al. Correlation between COVID-19 case fatality rate and percentage of BCG vaccination: is it true the vaccine is protective? Egypt J Bronchol. 2020;14(1):25.
Crossref - Zekri AN, Easa Amer K, Hafez MM, et al. Genomic characterization of SARS-CoV-2 in Egypt. J Adv Res. 2021;30:123-132.
Crossref - https://www.egypttoday.com/Article/1/100036/Health-Ministry-COVID%E2%80%99s-mutated-strain-not-in-Egypt-30K-vaccinated. Accessed 2 May 2021.
- Sallam M, Ababneh NA, Dababseh D, Bakri FG, Mahafzah A. Temporal increase in D614G mutation of SARS-CoV-2 in the Middle East and North Africa. Heliyon. 2021;7(1):e06035.
Crossref - Becerra-Flores M, Cardozo T. SARS-CoV-2 viral spike G614 mutation exhibits higher case fatality rate. Int J Clin Pract. 2020;74(8):e13525.
Crossref - Challen R, Brooks-Pollock E, Read JM, Dyson L, Tsaneva-Atanasova K, Danon L. Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: matched cohort study. BMJ. 2021;372:n579.
Crossref - Mostafa A, Kandil S, El-Sayed MH, et al. Universal COVID-19 screening of 4040 health care workers in a resource-limited setting: an Egyptian pilot model in a university with 12 public hospitals and medical centers. Int J Epidemiol. 2021;50(1):50-61.
Crossref - Kalantari H, Tabrizi AHH, Foroohi F. Determination of COVID-19 prevalence with regards to age range of patients referring to the hospitals located in western Tehran, Iran. Gene Rep. 2020;21:100910.
Crossref - World Health Organization. Regional Office for the Western Pacific. Guidance on COVID-19 for the care of older people and people living in long-term care facilities, other non-acute care facilities and home care. Manila: WHO Regional Office for the Western Pacific. 2020. https://apps.who.int/iris/handle/10665/331913. Accessed 5 January 2021.
- Negida A. Estimation of COVID-19 burden in Egypt. Lancet Infect Dis. 2020;20(8):894-895.
Crossref - Radwan GN. Epidemiology of SARS-CoV-2 in Egypt. East Mediterr Health J. 2020;26(7):768-773.
Crossref - Saba AI, Elsheikh AH. Forecasting the prevalence of COVID-19 outbreak in Egypt using nonlinear autoregressive artificial neural networks. Process Saf Environ Prot. 2020;141:1-8.
Crossref - Kasemy ZA, Bahbah WA, Zewain SK, et al. Knowledge, Attitude and Practice toward COVID-19 among Egyptians. J Epidemiol Glob Health. 2020;10(4):378-385.
Crossref - COVID-19 Information. https://eg.usembassy.gov/u-s-citizen-services/covid-19-information/. Accessed 6 January, 2021
- Egyptian officials: Third coronavirus wave will begin with Ramadan. “https://www.arabnews.com/node/1838026/middle-east. Accessed 3 May, 2021
© The Author(s) 2021. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.