


ISSN: 0973-7510
E-ISSN: 2581-690X
Pseudomonas aeruginosa poses a serious threat in healthcare settings. This bacterium can develop resistance to many antibiotics, rendering even last-resort treatments ineffective. Additionally, it forms protective biofilms that shield it from the immune system, making infection treatment challenging. This study investigated the susceptibility of five clinically isolated strains of the test bacteria to a combination of ciprofloxacin and cuminaldehyde. Cuminaldehyde (a natural phytochemical) and ciprofloxacin (an antibiotic) were separately found to show antimicrobial effect against test organism. However, the combination of selected compounds showed an additive effect in their microbial growth inhibitory activity. The mentioned compounds at their sub-MIC doses subjected to test whether they could show any extent of biofilm inhibition or disintegration property against the clinical strains of P. aeruginosa. The chosen concentrations of the compounds demonstrated significant antibiofilm activity against all the tested clinical strains. Additionally, it was observed that the compounds not only accumulated reactive oxygen species (ROS) but also enhanced the cell membrane permeability of the clinical strains. These findings suggest that the combination of ciprofloxacin and cuminaldehyde could explore new directions in fighting P. aeruginosa-linked infections.
Pseudomonas aeruginosa, Ciprofloxacin, Cuminaldehyde, Additive Interaction, Biofilm
P. aeruginosa, a major threat in clinical settings, is a Gram-negative opportunistic bacterium that could develop biofilms on various abiotic or biotic surfaces.1 These biofilms are slimy, multicellular communities that defend bacteria from the immune system.2 This promotes the rate of chronic infections, such as cystic fibrosis or those associated with implanted medical devices.3 The emergence of antibiotic-resistant biofilms of P. aeruginosa presents a noteworthy challenge in treating these chronic infections. Studies suggest a high prevalence of biofilm formation among P. aeruginosa isolates. One study reported 83.75% of clinical isolates displayed biofilm-forming ability.4 This ability to form biofilms, combined with growing resistance to antibiotics, makes P. aeruginosa a major contributor of prolonged untreated infections. Recent studies focus on exploring new treatment strategies to combat these resilient biofilms. One such approach is a combinatorial study investigating the effectiveness of combining natural compounds with antibiotics.5,6 In this regard, we had already used ciprofloxacin and cuminaldehyde against P. aeruginosa by considering the potential of ciprofloxacin against P. aeruginosa (MTCC 424), a non-pathogenic strain.7 Ciprofloxacin, a potent fluoroquinolone antibiotic has fairly good activity against the Gram-positive bacteria. However, its efficacy has proved to be more potent in Gram-negative bacteria when compared to other fluoroquinolones.8 The recent literature suggests that the clinically isolated strains of P. aeruginosa have been found to be more infectious and pathogenic than non-clinical strains.9 Clinical-pathogenic strains possess a range of virulence factors, such as toxins and enzymes that allow them to, less virulent strains invade and damage host tissues unlike the non-pathogenic. They also tend to be more adept at forming biofilms exhibiting different physiological patterns than the non-pathogenic strains.10 Although, the effectiveness of the compounds (cuminaldehyde and ciprofloxacin) has already been reported against the non-clinical strains of P. aeruginosa, the potential of the same has yet to be tested on the clinical strains of the same bacteria. Thus, in this study, we have combined ciprofloxacin and cuminaldehyde against the growth of the clinical strains of P. aeruginosa. The study revealed that ciprofloxacin and cuminaldehyde was highly effective and shows promise in inhibiting the microbial growth as well as managing biofilm threats of the clinical strains while applied in combination. Hence, this approach offers a possible solution to combat biofilm-mediated P. aeruginosa infections.
Microbial strains, chemicals and growth media
Five clinical strains of P. aeruginosa, obtained from Suraksha Diagnostic Centre, Kolkata, were considered as the organism of interest in the current study. The bacteria was cultivated at 37°C for 24 h in sterile Luria Bertani broth (LB; obtained from Sisco Research Laboratories). Cuminaldehyde, a natural compound (Sigma-Aldrich), and ciprofloxacin, an antibiotic (Sisco Research Laboratories), were selected as test compounds. Cuminaldehyde was dissolved in DMSO (Dimethyl Sulfoxide), while ciprofloxacin (10 mg/mL) was dissolved in MilliQ water and further diluted in LB as per the experimental requirement.
Estimating the minimum inhibitory concentration (MIC)
The minimum amount of any anti-microbials that prevents a microorganism to grow visibly is termed as the MIC value of that antimicrobial.11 Here, MIC of ciprofloxacin and cuminaldehyde was estimated against the clinical strains using a 2020 protocol of Chakraborty et al.12 In this regard, at first, equal numbers (106 CFU/mL) of the test organisms were cultured in autoclaved growth media (5 mL) in which various concentrations of the natural compound, cuminaldehyde (ranging from 0 µg/mL to 600 µg/mL) and ciprofloxacin (ranging from 0 µg/mL to 15 µg/mL) were added individually. After incubation at 37°C for a period of 24 h, the extent of microbial growth was determined at 600 nm using a colorimeter.
Determining Fractional-Inhibitory-Concentration Index (FICI)
The checker board assay was conducted to determine FICI to understand the possible interactions between cuminaldehyde and ciprofloxacin. For this experiment, an equal number (106 CFU/mL) of overnight inoculated cultures of all clinical isolates were further cultured into sterile growth media and subsequently treated with varying concentrations of cuminaldehyde (up to 600 µg/mL) and ciprofloxacin (up to 20 µg/mL), or left unexposed. After incubation at 37°C for a period of 24 h, microbial growth was assessed, and using the following formula the FICI was calculated:
FICI of cuminaldehyde against clinical strains = MIC (cuminaldehyde) while applied in combination / MIC (cuminaldehyde) while applied alone against clinical strains.
FICI of ciprofloxacin against clinical strains = MIC (ciprofloxacin) while applied in combination / MIC (ciprofloxacin) while applied alone against clinical strains
FICI = FIC (cuminaldehyde) + FIC (ciprofloxacin)
The interaction between the two selected compounds was calculated using the FIC index provided in established documents13:
When the value of FIC is ≤0.5, it is synergistic;
When the value of FIC is >0.5 and ≤1, it is additive;
When the value of FIC is >1 and ≤4, it is intermediate;
When the value of FIC is >4, it is antagonistic
Crystal-Violet (CV) assay
Assessment of bacterial biofilm using CV assay relies on the ability of the basic dye, CV, to bind to negatively charged cells and surface molecules of the extracellular polymeric substance.14 Thus, the CV staining assay is widely recognized as a conventional method for quantifying microbial biofilm formation on various surfaces.15 In this study, the degree of biofilm of both untreated and treated test organisms were analyzed using the CV assay, using the protocol adapted from Das et al.16 To proceed with the experiment,
106 CFU/mL of the test bacteria were inoculated into autoclaved growth media (5 mL) and subsequently treated with 50 µg/mL of cuminaldehyde (for all five selected isolates). Ciprofloxacin was either added along with cuminaldehyde (0.3 µg/mL for PSA1; 0.1 µg/mL for PSA2; 0.01 µg/mL for PSA3 and 1 µg/mL for PSA4, PSA5) or left unexposed. Following incubation, free-living planktonic cells were removed and the adhered biofilm on the test tubes was CV-stained and kept aside for half an hour. The non-adhered CV solution was discarded post incubation, and the tubes were washed with sterile double-distilled water. Thereafter, 33% acetic acid (glacial) solution (5 mL) was added to the respective tubes to dissolve the stain adhered with the biofilm cells. Finally, OD630 was recorded by measuring the intensity of the CV solution using a colorimeter.
Analysis of bacterial biofilm under light microscope
Microscopic images offer detailed visual presentation of biofilm formation of a microorganism under a given condition.17 Therefore, to analyze the biofilm profiles of test organisms in the absence or presence of selected doses (as mentioned previously) of test compounds, light microscopic image analysis was considered. To perform this analysis, clinical strains of P. aeruginosa (106 CFU/mL) were inoculated in LB media containing coverslips that supported the formation of biofilm clusters either in the absence or presence of the chosen concentrations of test compounds (ciprofloxacin and/or cuminaldehyde) under same experimental conditions. Following overnight incubation, coverslips from each experimental set were aseptically collected from each experimental set, gently washed with MilliQ water, subsequently stained CV (0.4%) in solution form for half an hour and observed under a light microscope (Olympus CX21i).
Assessment of total biofilm protein
As an indirect measure, quantifying total biofilm protein content offers a reliable method for the relative assessment of biofilm profile.18 To this end, the Bradford assay was conducted to analyze the total biofilm protein content of all clinically isolated P. aeruginosa strains, both in the absence and presence of test compounds, using the protocol outlined by Malik et al.7 For this assay, cells were either challenged with selected doses of cuminaldehyde and/or ciprofloxacin (as mentioned previously), or left untreated as a control set. After incubation at 37°C for a period of 24 h, biofilm cells adhered to the tube were considered. NaOH solution (5 mL, 0.3 M) was added in each tube and boiled for half an hour to extract the total protein of the biofilm present on the glass tube surface. Then the supernatant was collected by centrifuging the solution for 10 min at 8000 rpm. Bradford reagent was mixed with the supernatant in a 1:1 ratio and kept aside for 30 min at room temperature (RT). Finally, the OD at 595 nm was recorded to measure the intensity of the color developed by the biofilm protein.
Measurement of extracellular polysaccharides (EPS)
To measure the EPS of all clinical isolates, the phenol-sulfuric acid method, as outlined by Dubois et al.19 was followed. The EPS profile, consisting of primary and major constituents, reflects the degree of biofilm formation on the given surface. For this assay, 106 CFU/mL of test organism were cultivated to form biofilm on the glass surface in the presence or absence of the chosen concentrations of cuminaldehyde and/or ciprofloxacin (as mentioned previously). A control set was also prepared where 106 CFU/mL of test organism was left untreated. Post incubation, free-living planktonic cells were removed, and the attached biofilm cells on the glass tube were suspended in phosphate-buffered saline (PBS; pH 7.4). This prepared suspension was then subjected to centrifugation at a rate of 6000 rpm for around 10 min. The supernatant obtained from this step was the cell-free EPS and the pellet (re-suspended in 10 mM EDTA) obtained was re-centrifuged (10 min, 6000 rpm) to extract the cell-bound EPS matrix. Then, the supernatant obtained from each of the sets was dissolved in chilled ethanol (1:2.2 ratios) for an hour at 4°C. Then, this suspension was subjected to 6000 rpm centrifugation for 20 min. The pellet obtained from this step was termed as the total EPS content. To measure the degree of EPS extracted in both treated and untreated samples, the extracted pellets were re-suspended in 1 mL of PBS and mixed with phenol and concentrated sulfuric acid in a ratio of 2:1:5 (sample: phenol: sulfuric acid), respectively. The prepared mix solution was then boiled at 100°C for 10 min and cooled for 10 min at RT. Finally, the OD at 490 nm was recorded to measure the amount of EPS in each set.
Analysis of metabolic activity
The degree of metabolically active clinical isolates of the test bacteria was measured by employing FDA hydrolysis assay.20 In this regard, equal numbers of biofilm cells of the clinical strains of P. aeruginosa were either untreated or treated with the compounds and following incubation, the cells were collected by scrapping. The cells collected from the previous step were suspended in PBS (5 mL, pH 7.4). Subsequently, 500 µL (5 mg/mL) FDA in solution form was dispensed in each tube for an hour in darkness. All the prepared experimental sets were then subjected to 10,000 rpm centrifugation for a time span of 10 min. Then, fluorescein, collected from the obtained supernatant was recorded at 490 nm.
ROS accumulation estimation
Intracellular ROS accumulation was assessed for all the selected clinical isolates of P. aeruginosa. DCFDA method was employed for all the various sample conditions (treated and untreated) by following Das et al.21 To conduct this experiment, cells were either treated with 50 µg/mL of the natural test compound, cuminaldehyde and/or various concentrations of the antibiotic, ciprofloxacin (0.3 µg/mL for PSA1; 0.1 µg/mL for PSA2; 0.01 µg/mL for PSA3 and 1 µg/mL for PSA4 and PSA5). A separate untreated control set was prepared where only the clinical strains were grown over a similar incubation temperature for 6 h. Then, each set was supplemented with 0.5 µL of DCFDA to achieve a final ratio of 1:2000 (v/v), and incubation at 37°C for half an hour. Finally, the quantity of accumulated ROS produced under each condition was estimated at 488 nm (excitation), and at 535 nm (emission).
Estimation of cell membrane permeability by Ethidium Bromide (EtBr) influx assay
The cell membrane permeability of the clinical strains of the test bacteria was analyzed in response to the test compounds by following the EtBr influx assay.22 For this experiment, overnight-grown cells were centrifuged and the collected cell pellet (1 mL) was suspended in PBS (pH 7.4). The cell pellet was further treated with 50 µg/mL of cuminaldehyde and/or various concentrations of ciprofloxacin (0.3 µg/mL for PSA1; 0.1 µg/mL for PSA2; 0.01 µg/mL for PSA3 and 1 µg/mL for PSA4 and PSA5) at 37°C for 6 h. Following treatment, both the untreated and treated cell suspensions were supplemented with EtBr (0.5 µg/mL) and kept aside without exposure to light for 5 min. Finally, the fluorescence intensity was measured in a fluorometer (excitation at 520 nm, emission at 590 nm).
Analysis of biofilm disintegration
The disintegrating property of the clinically isolated strains of the test bacteria was assessed under the presence of the test compounds. Similar cells were permitted to develop biofilm for a period of 24 h, 37°C. Following incubation, overnight-grown biofilm was either treated with cuminaldehyde or ciprofloxacin or both at similar concentrations stated previously for a span of another 6 h. The degree of residual biofilm denoted the biofilm disintegration percent compared to the control set. Thus, this residual biofilm was subjected to various experiments (CV assay, total biofilm-protein estimation, EPS measurement and FDA assay) already discussed in previous sections.
Analysis of biofilm management on catheter tubes
To analyze the test compounds in managing microbial biofilm formation on catheter surfaces, two sets of experiments were conducted. In the first set, sterile catheter tubes measuring 1 cm in length and 0.3 cm in width were exposed to the clinical strains of the test bacteria under the presence of the selected concentrations of the natural compound, cuminaldehyde and/or the antibiotic, ciprofloxacin. In the second set, a control set was considered without any compound exposure. After similar conditions of incubation time and temperature, catheter tubes from the second set were treated with the chosen concentrations of ciprofloxacin and/or cuminaldehyde for another 6 h. Following treatment, catheter tubes from both sets were aseptically collected, and CV assay, protein estimation, and EPS measurement assay were conducted by following previously established protocol was carried out.
Statistical analysis
To statistically analyze the key observations, ANOVA, One-way analysis of variance was explored (ANOVA). The average recorded value of all the experiment(s) was estimated post a three times repetition. An error bar of each data set represents the standard deviation of each experiment in comparison to the control set. The p values less than 0.05 represented with (*), less than 0.01 represented with (**), and less than 0.001 represented with (***) in comparison to the control. Whereas, p values beyond 0.005 were denoted as N.S. (statistically no difference).
Antimicrobial activity of ciprofloxacin and cuminaldehyde against P. aeruginosa
The increasing challenge of treating infectious diseases caused by the opportunistic pathogen P. aeruginosa reinforces the scientific community relying on combinatorial therapies.23 In this context, in our previous study, cuminaldehyde combined with ciprofloxacin has already shown potential against laboratory strains of P. aeruginosa (MTCC 424).7 To ensure whether the findings are directly applicable to the challenges encountered in clinical practice,24,25 in present study, effort has been accumulated to investigate the applicability of cuminaldehyde along with ciprofloxacin against clinically isolated strains of P. aeruginosa. Literature showed that clinical strains of P. aeruginosa often exhibited increased virulence through structural, morphological and metabolic adaptation, which is critical for their survival and proliferation in human hosts.26 Moreover, clinical strains could show significant genetic diversity and frequent acquisition of mobile genetic elements, which confer diverse array of virulence factors and resistance to antibiotics commonly found in hospital environments.27 This genetic flexibility allows them to adapt rapidly to selective pressures, enhancing their survival and virulence.27 In contrast, laboratory strains often lack these adaptive mechanisms, making them less capable of interacting with and infecting human hosts. From a biological perspective, understanding host and pathogen interplay is essential for developing new therapeutic strategies.28 Studies on clinical isolates are likely to provide detailed insights into the drastically diverse forms of P. aeruginosa infections.29 Therefore, the present study focused on total five clinical isolates of P. aeruginosa (PA1 to PA5). At first, MIC of all the isolates was determined using a broth dilution assay. The observation revealed that the MIC of cuminaldehyde exhibited 600 µg/mL, and that of ciprofloxacin varied within 0.1-20 µg/mL across all the five isolates of test organism (Table). Furthermore, a checkerboard assay was conducted to understand the interaction between the two compounds. The result showed a reduction in effective concentrations of compounds when used together compared to individual application (Figure 1). Additionally, the FICI of >0.5 indicated a strong additive interaction between ciprofloxacin and cuminaldehyde against all clinical strains of P. aeruginosa (Table). Thus, the present study reports that the compounds either alone or in combination showed considerable antimicrobial activity. However, we reported that the compounds (ciprofloxacin and cuminaldehyde) in combination could show heightened antimicrobial potential against the clinical strains due to additive interactions.
Table:
According to the FIC index estimated from the checkerboard assay, cuminaldehyde and ciprofloxacin shows additive interaction against all clinical isolates P. aeruginosa. Sub-MIC doses of cuminaldehyde and ciprofloxacin suppressed biofilm development as well as efficiently disintegrated the pre-existing biofilm in all clinical isolate of P. aeruginosa
S. No. |
Organism name |
MIC of Cuminaldehyde (µg/mL) |
MIC of Ciprofloxacin (µg/mL) |
FICI (FIC index) |
Type of Interaction |
Amount of biofilm reduction (in comparison to the control group) |
Amount of residual biofilm (in comparison to the control group) |
|---|---|---|---|---|---|---|---|
01. |
PA1 |
600 |
3 |
0.5 |
Additive |
~ 45.23 |
~ 55.15 |
02. |
PA2 |
600 |
1 |
0.68 |
Additive |
~ 49.52 |
~ 58.90 |
03. |
PA3 |
600 |
0.1 |
0.58 |
Additive |
~ 39.18 |
~ 54.89 |
04 |
PA4 |
600 |
20 |
0.68 |
Additive |
~ 42.78 |
~ 52.70 |
05. |
PA5 |
600 |
10 |
0.88 |
Additive |
~ 45.60 |
~ 58.90 |
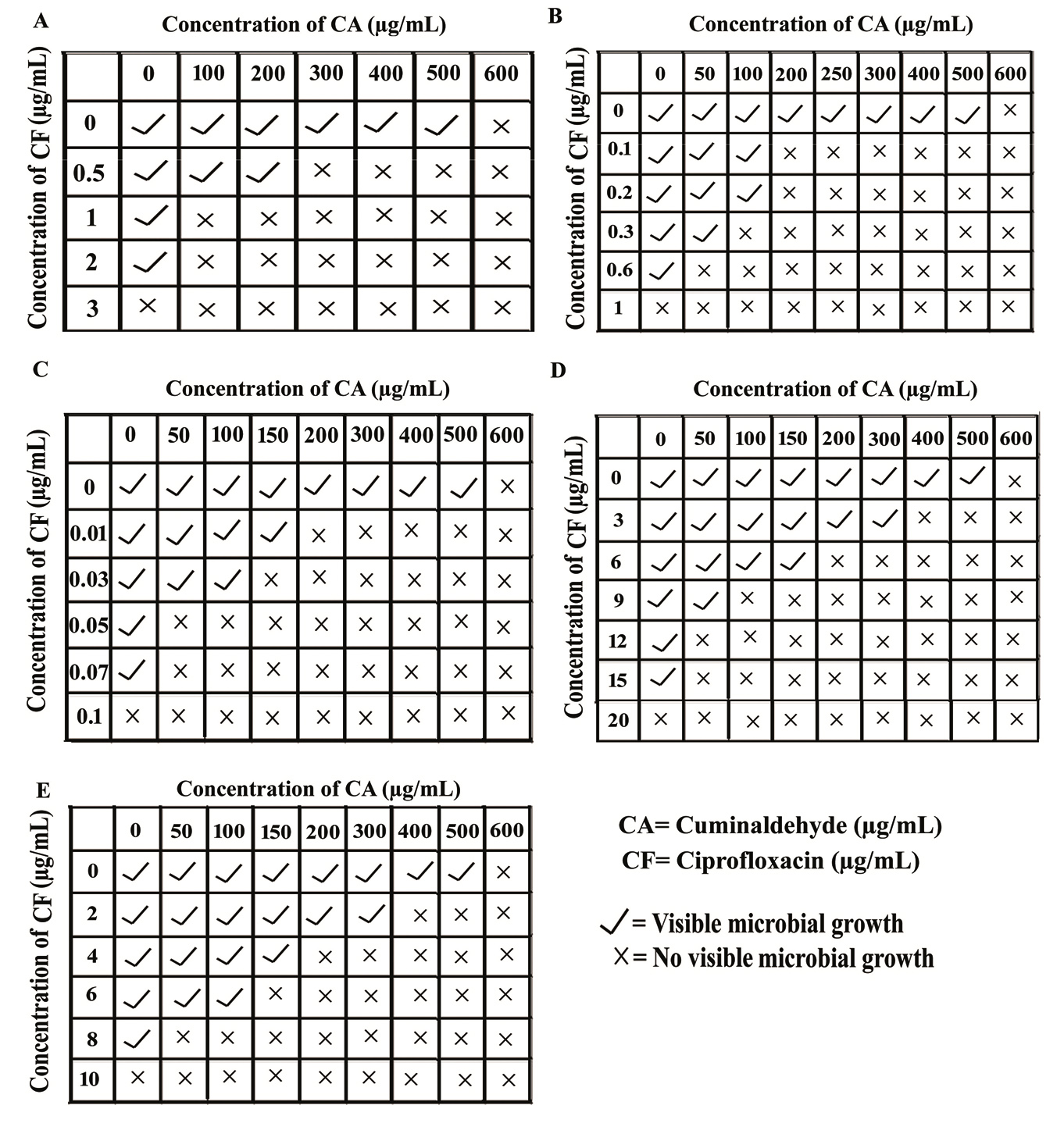
Figure 1. Antimicrobial activity of cuminaldehyde in combination with ciprofloxacin against the clinical strains of P. aeruginosa. A. Checkerboard assay of Isolate 1 (PA1). B. Checkerboard assay of Isolate 2 (PA2). C. Checkerboard assay of Isolate 3 (PA3). D. Checkerboard assay of Isolate 4 (PA4). E. Checkerboard assay of Isolate 5 (PA5)
Cuminaldehyde and ciprofloxacin showed promising effect in managing biofilm threat of the clinical isolates of P. aeruginosa
Combating biofilm-related infections has become a focal point in medical and scientific research, with a particular emphasis on developing new therapeutics targeting biofilm challenges associated with P. aeruginosa.30 Previous researches have demonstrated that sub-MIC doses of ciprofloxacin and cuminaldehyde in combination could inhibit microbial biofilm formation of the non-clinical strains of P. aeruginosa.7 Building upon this foundation, this research work focused in investigating whether the combined use of the selected compounds could inhibit biofilm formation across all the selected clinical strains of P. aeruginosa. Light microscopic image assessment, a method capable of visualizing bacterial biofilm morphology, revealed a noticeable reduction in biofilm formation under the combined application of the chosen concentrations of ciprofloxacin and cuminaldehyde in contrast to their individual treatments (Figure 2). To validate the microscopic observations, CV assay (evaluates the degree of biofilm formation on any surface), protein recovery assay (to quantify the protein content recovered from the biofilm adhered to the glass surface), EPS measurement assay (to assess the production of extracellular polysaccharides), and FDA-hydrolysis assay (to analyze the metabolically active biofilm cells adhering to the tube) were conducted. The results thus cooperatively demonstrated that the combination of the test compounds efficiently impeded microbial biofilm formation by approximately 50% across all five clinical isolates of P. aeruginosa (Figure 3A). Moreover, the selected sub-MIC concentrations of the compounds did not exhibit any inhibitory action on the microbial growth of the same microorganisms (Figure 3B). Treating pre-existing microbial biofilm is vital due to its role as a reservoir for persistent infections.31 Targeting and disrupting pre-existing biofilm enhance treatment efficacy and reducing recurrent infections.31 Therefore, understanding the ability of ciprofloxacin and cuminaldehyde to disintegrate existing biofilm suggest their potential as effective antibiofilm agents, capable of inhibiting as well as disintegrating the pre-existing biofilm, thereby addressing a critical aspect of combating biofilm-related infections.32 To investigate the disintegration property of cuminaldehyde and/or ciprofloxacin against the clinical isolates of test organism, CV-assay, protein recover assay, EPS-assay and FDA-assay were undertaken. The result revealed a significant reduction (approximately 45%) in pre-existing biofilm formation when treated in combination (Figure 3C). Hence, from all these observations, it was quite evident that the selected concentrations of ciprofloxacin and cuminaldehyde in combination could act as a potential antibiofilm agent for the clinical isolates of P. aeruginosa cells. The result also suggested that the combinations of the compounds at their sub-MIC doses could exhibit antibiofilm effect against the organisms without showing antimicrobial effect.
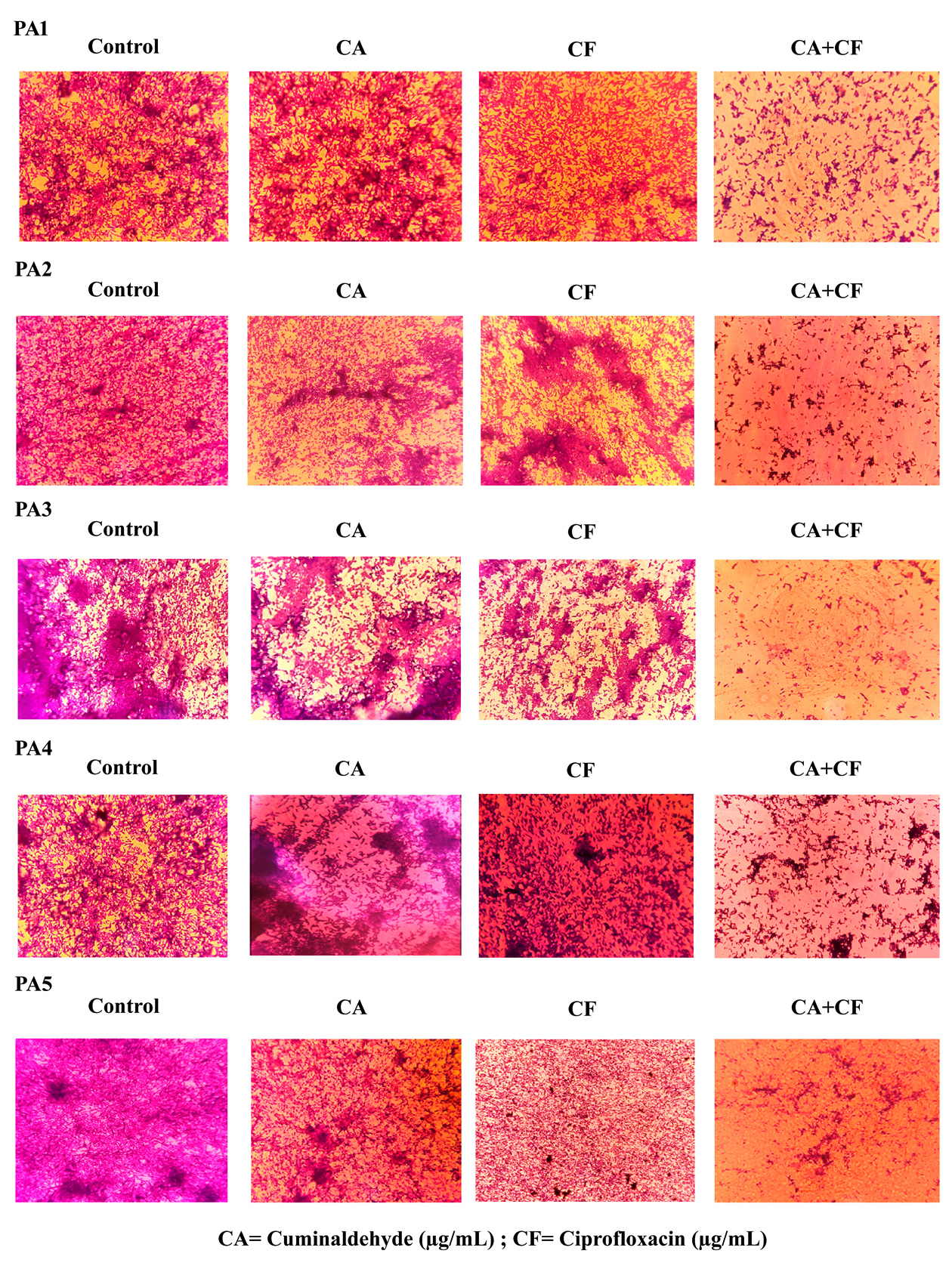
Figure 2. Microscopic image analysis of P. aeruginosa treated with cuminaldehyde in combination with ciprofloxacin. Sub-MIC doses of ciprofloxacin and/or cuminaldehyde were added in different tubes and incubated at 37°C for 24 h. Post incubation, coverslips were collected and stained with CV (0.4%) and observed under a light microscope. The figure is a representative image of 20 different spots of three independent experiments. A. Microscopic image of PA1. B. Microscopic image of PA2. C. Microscopic image of PA3. D. Microscopic image of PA4. E. Microscopic image of PA5
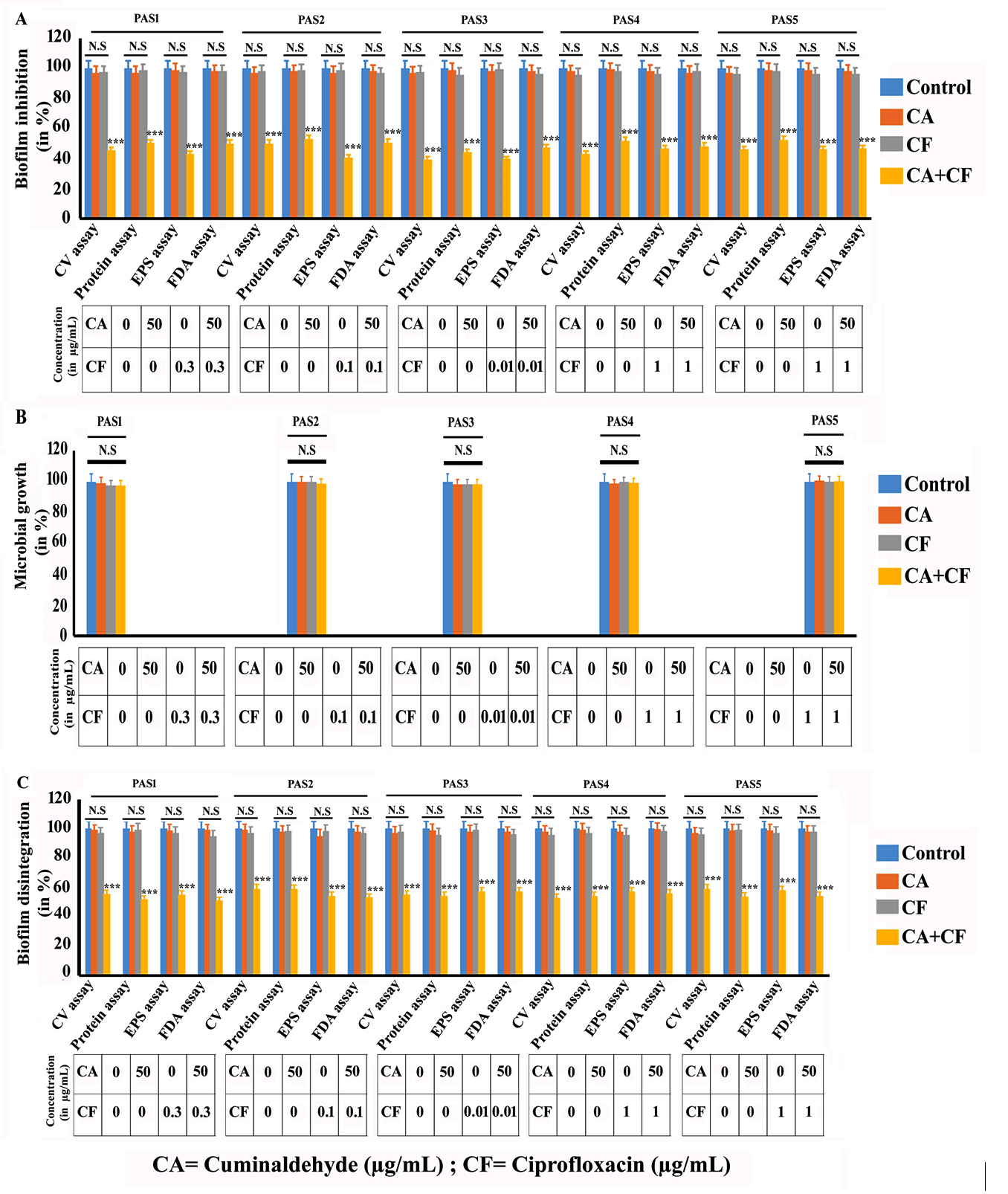
Figure 3. Cuminaldehyde in combination with ciprofloxacin exhibited considerable antibiofilm property against clinical strains of P. aeruginosa. A similar number of cells were cultured in sterile LB tube either in presence or in absence of sub-MIC doses of ciprofloxacin and/or cuminaldehyde for 24 h at 37°C. A. Biofilm profile. The extent of biofilm adhered on glass tube was measured by conducting CV assay, EPS measurement assay, total protein estimation assay and FDA assay. B. Antimicrobial profile. To understand the antimicrobial property of the selected sub-MIC doses of test compound upon the clinical strains, the OD of both treated and untreated sets of test samples were measured at 600 nm. C. Biofilm disintegration property. Overnight grown culture of P. aeruginosa was either treated with the selected sub-MIC doses of ciprofloxacin and/or cuminaldehyde or left untreated and further incubated for 6 h. Then, the degree of biofilm disintegration was estimated by performing CV assay, total EPS measurement assay, total protein estimation and FDA assay. Each experiment was carried out three times. The standard error of the mean was shown by the error bars. The p values were used to represent the statistical difference between the observations. The p values less than 0.05, 0.01, and 0.001 were marked by *, **, and ***, respectively
Exploration of underlying mechanism of the antibiofilm potential of the combination of ciprofloxacin and cuminaldehyde against clinical isolates of P. aeruginosa
To investigate the underlying mechanism behind antibiofilm potential of cuminaldehyde combined with ciprofloxacin, the ROS profile of five clinical isolates of P. aeruginosa using the DCFDA method was assessed. ROS is a well-documented microbial biofilm inhibitor.5 Elevated levels of ROS can trigger oxidative stress leading to damage of cellular components thereby inhibiting biofilm formation.33 Treatment with ciprofloxacin and cuminaldehyde together resulted in a significant increase in intracellular ROS accumulation compared to untreated cells (Figure 4A). The result also revealed that ROS profile increased by ~60% to ~80% across all the five selected clinical isolates. To confirm this finding, the experiment was repeated with ascorbic acid. Ascorbic acid acts as a ROS scavenger by donating electrons to neutralize ROS.7 The findings revealed a notable reduction in ROS levels when exposed to ascorbic acid alongside the test compounds (Data not shown). The finding suggested a marked decrease in biofilm activity correlating with increased ROS generation. Ascorbic acid treatment effectively mitigated ROS levels consequently restored the biofilm profile (Data not shown). These findings suggested that the antibiofilm properties of ciprofloxacin and cuminaldehyde could be attributed to the ROS accumulation. Additionally, cell membrane permeability was measured as it could play an important role in influencing microbial biofilm network. Cuminaldehyde has previously been shown to increase cell membrane permeability in P. aeruginosa.6 The result demonstrated a significant increase in membrane permeability when both cuminaldehyde and ciprofloxacin were applied together, with enhancements ranging from ~30% to ~70% across all the elected clinical isolates compared to controls (Figure 4B). This suggested that the combined action of these compounds could enhance intracellular ROS accumulation and increment of cell membrane permeability more effectively than their individual application. According to previous literature, reduced cell membrane permeability typically reinforces biofilm architecture whereas increased membrane permeability has a significantly diminished impact on biofilm structures.34 Taken together, it can be deduced that targeting cell membrane permeability can be an effective strategy for biofilm inhibition. The results demonstrated that a combined application of ciprofloxacin and cuminaldehyde can be considered as a potential cause of biofilm control of clinical strains of P. aeruginosa.
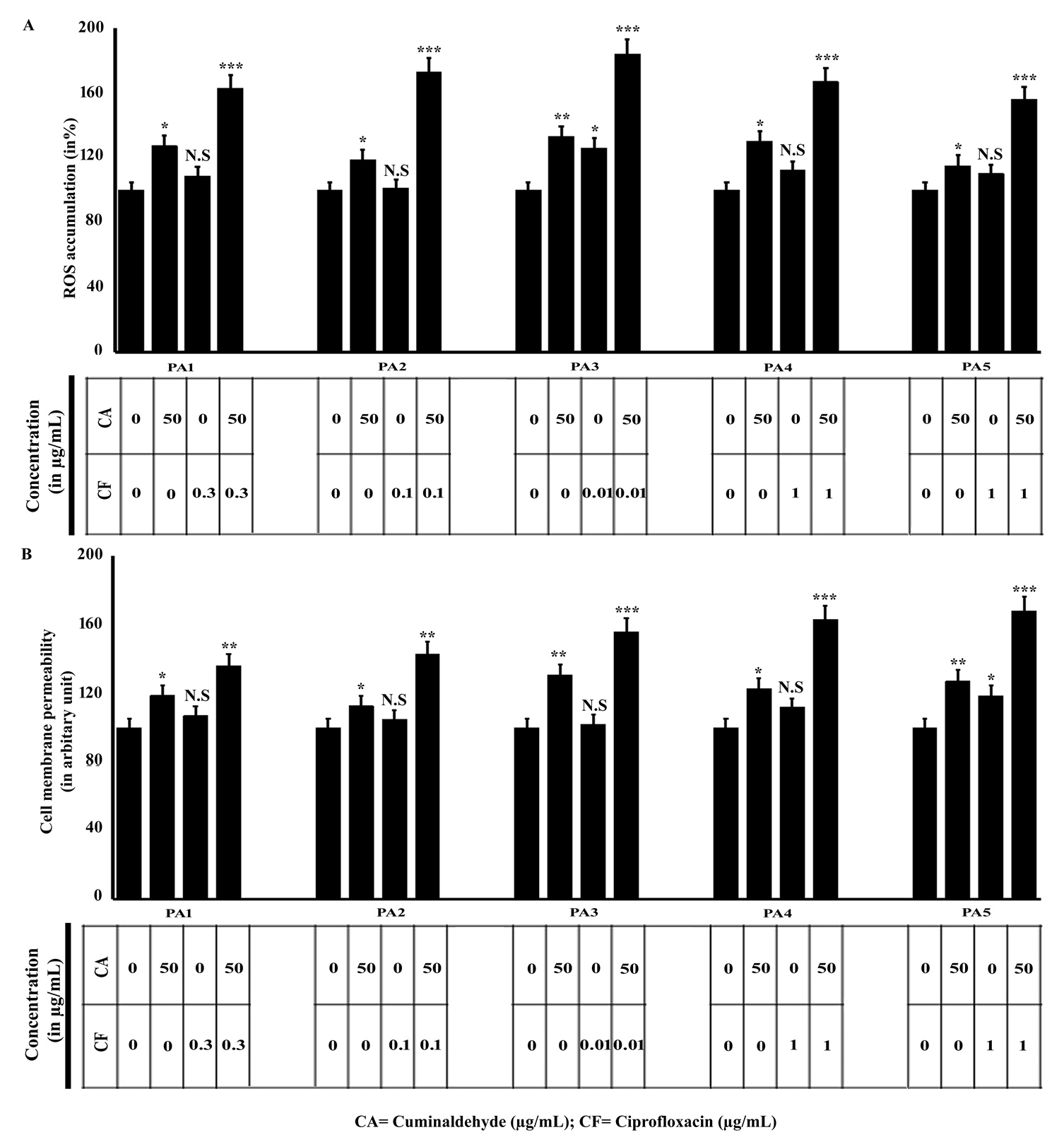
Figure 4. Investigating the mechanisms of cuminaldehyde combined with ciprofloxacin against the clinical strains of P. aeruginosa. A. Estimation of intracellular ROS accumulation. The intracellular ROS accumulation in clinical strains of P. aeruginosa from both compounds treated and untreated conditions were estimated by following the DCFDA assay. B. Estimation of cell membrane permeability. Accumulation of cell membrane permeability of P. aeruginosa cells from both treated and untreated conditions was estimated by EtBr influx assay as mentioned in the materials and method section. Each experiment was repeated three times. The standard error of the mean was shown by the error bars. The p values were used to represent the statistical difference between the observations. The p values less than 0.05, 0.01, and 0.001 were marked by *, **, and ***, respectively and p value greater than 0.05 signified Non-significant (NS)
Cuminaldehyde in combination with ciprofloxacin could curb biofilm linked threats of clinical isolates of P. aeruginosa from catheter model
Catheter-associated biofilm poses significant challenges in healthcare, leading to persistent and recurrent infections.5 Addressing these infections poses a major challenge for the healthcare system. Effort was accumulated to assess the effectiveness of our chosen compounds against in-vitro catheter-associated biofilm challenges from all five clinical isolates of the test bacteria under investigation. In this regard, various assays including CV-assay, protein recovery assay, and EPS-assay were conducted. The results indicated a substantial reduction in biofilm formation, ranging from 45% to 50%, when the biofilm of the test organism was developed on catheter surface, with or without cuminaldehyde and ciprofloxacin in combination (Figure 5A). Moreover, efficient disintegration of the pre-existing biofilm was assessed in the range from 40% to 45%, across all five selected clinical isolates (Figure 5B). Collectively, our data suggested that selected compounds effectively inhibits and disintegrates pre-existing biofilm on the catheter surface while applied in combination, offering a promising strategy for preventing and treating catheter-associated infections.
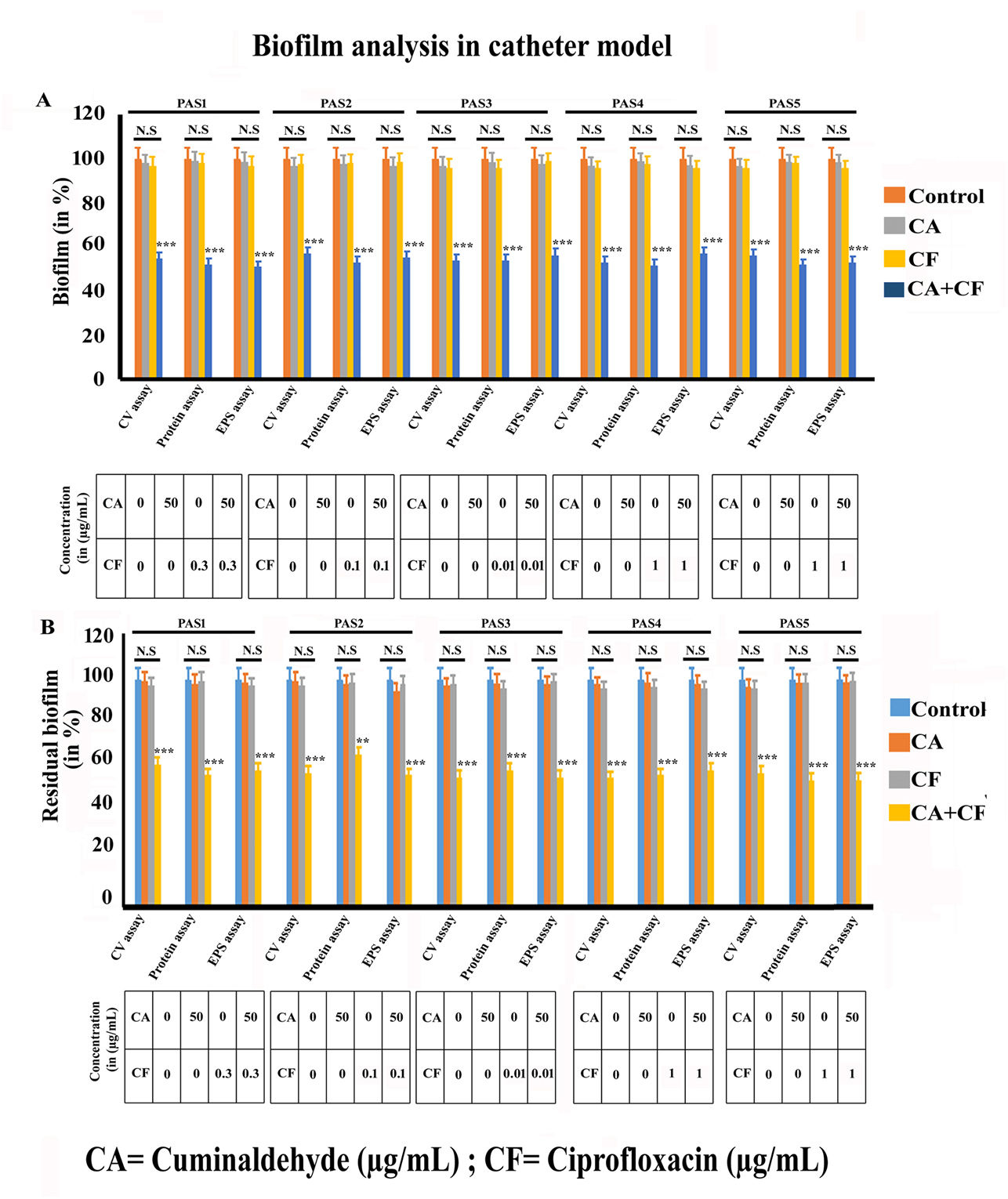
Figure 5. Ciprofloxacin and cuminaldehyde in combination exhibited considerable reduction in microbial biofilm formation of P. aeruginosa on catheter surfaces. A. Biofilm inhibition profile. Equal numbers of P. aeruginosa cells were grown on catheter tubes in LB medium for 24 h under various treatment conditions. After the incubation period, catheters were collected aseptically from all experimental sets. The biofilm inhibition profile was then assessed using several assays, including the CV assay, EPS estimation, and protein estimation. B. Biofilm disintegration profile. The extent of disintegration of the existing biofilm on the catheter surface was assessed under the treated and untreated conditions using the CV assay, EPS estimation, and protein estimation. Each experiment was carried out three times. The error bars represented the standard error of the mean. The p values were used to represent the statistical difference between the observations. The p values less than 0.05, 0.01, and 0.001 were marked by *, **, and ***, respectively
P. aeruginosa biofilm-related infections are becoming an alarming issue around the world, and as a result, controlling this threat is an enormous concern for the healthcare sectors. The findings of this study demonstrate that cuminaldehyde in combination with ciprofloxacin can inhibit the development and persistence of P. aeruginosa biofilms effectively, thereby offering a promising therapeutic strategy for combating against biofilm-associated infections.
ACKNOWLEDGMENTS
The authors’ would like to thank Suraksha Diagnostic Center, Kolkata, India, for providing some technical help in carrying out the research work.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
PT conceived the idea. MM, SD, PP, PC,AD,RR, PT and SS designed the experiments. MM, SD, PP, PC,AD,RR and SS performed the experiments. PT analyzed the data. MM, SD, PP, PC,AD,RR and SS wrote the manuscript. PT edited the manuscript. All authors read and approved the final manuscript for publication.
FUNDING
This study was funded by the Neotia University in the form of minor grant
(TNU/R&D/M/11).
DATA AVAILABILITY
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
ETHICS STATEMENT
Not applicable.
- Cepas V, Lopez Y, Munoz E, et al. Relationship between biofilm formation and antimicrobial resistance in gram-negative bacteria. Microb Drug Resist. 2019;25(1):72-79.
Crossref - Shree P, Singh CK, Sodhi KK, Surya JN, Singh DK. Biofilms: Understanding the structure and contribution towards bacterial resistance in antibiotics. Med. Microecol. 2023;16:100084.
Crossref - Mihai MM, Holban AM, Giurcaneanu C, et al. Microbial biofilms: Impact on the pathogenesis of periodontitis, cystic fibrosis, chronic wounds and medical device-related infections. Curr Top Med Chem. 2015;15(16):1552-1576.
Crossref - Kamali AM, Jafari N, Eftekhari K. Novel coronavirus in a 15-day-old neonate with clinical signs of sepsis, a case report. Infect Dis. 2020;52(6):427-429.
Crossref - Roy R, Paul P, Chakraborty P, et al. Cuminaldehyde and Tobramycin Forestall the Biofilm Threats of Staphylococcus aureus: A Combinatorial Strategy to Evade the Biofilm Challenges. Appl Biochem Biotechnol. 2024.
Crossref - Chatterjee S, Paul P, Chakraborty P, et al. Combinatorial application of cuminaldehyde and gentamicin shows enhanced antimicrobial and antibiofilm action on Pseudomonas aeruginosa. Folia Microbiol. 2024;69(4):823-834.
Crossref - Malik M, Das S, Chakraborty P, et al. Application of cuminaldehyde and ciprofloxacin for the effective control of biofilm assembly of Pseudomonas aeruginosa: A combinatorial study. Microb Pathog. 2024;190:106624.
Crossref - Ezelarab HAA, Abbas SH, Hassan HA, Abuo Rahma GEA. Recent updates of fluoroquinolones as antibacterial agents. Arch Pharm. 2018;351(9):1800141.
Crossref - Laborda P, Sanz-Garcia F, Hernando-Amado S, Martinez JL. Pseudomonas aeruginosa: an antibiotic resilient pathogen with environmental origin. Curr Opin Microbiol. 2021;64:125-132.
Crossref - Bjarnsholt T. The role of bacterial biofilms in chronic infections. Apmis. 2013;136:1-51.
Crossref - Kowalska-Krochmal B, Dudek-Wicher R. The minimum inhibitory concentration of antibiotics: Methods, interpretation, clinical relevance. Pathogens. 2021;10(2):165.
Crossref - Chakraborty P, Dastidar DG, Paul P, et al. Inhibition of biofilm formation of Pseudomonas aeruginosa by caffeine:a potential approach for sustainable management of biofilm. Arch Microbiol. 2020;202(3):623-35.
Crossref - Louie TJ, Miller MA, Mullane KM, et al. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med. 2011;364(5):422-431.
Crossref - Rollefson JB, Stephen CS, Tien M, Bond DR. Identification of an extracellular polysaccharide network essential for cytochrome anchoring and biofilm formation in Geobacter sulfurreducens. J Bacteriol. 2011;193(5):1023-1033.
Crossref - Skogman ME, Vuorela PM, Fallarero A. Combining biofilm matrix measurements with biomass and viability assays in susceptibility assessments of antimicrobials against Staphylococcus aureus biofilms. J Antibiot. 2012;65(9):453-459.
Crossref - Das S, Paul P, Chatterjee S, et al. Piperine exhibits promising antibiofilm activity against Staphylococcus aureus by accumulating reactive oxygen species (ROS). Arch Microbiol. 2022;204(1):59.
Crossref - Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506.
Crossref - Wilson SC, Trukhanova I, Dmitrieva L, et al. Assessment of impacts and potential mitigation for icebreaking vessels transiting pupping areas of an ice-breeding seal. Biol Conserv. 2017;214:213-222.
Crossref - DuBois M, Gilles KA, Hamilton JK, Rebers PA, Smith F. Colorimetric method for determination of sugars and related substances. Anal Chem. 1956;28(3):350-356.
Crossref - Dzionek A, Dzik J, Wojcieszynska D, Guzik U. Fluorescein diacetate hydrolysis using the whole biofilm as a sensitive tool to evaluate the physiological state of immobilized bacterial cells. Catalysts. 2018;8(10):434.
Crossref - Das S, Roy R, Paul P, et al. Piperine, a Plant Alkaloid, Exhibits Efficient Disintegration of the Pre-existing Biofilm of Staphylococcus aureus: a Step Towards Effective Management of Biofilm Threats. Appl Biochem Biotechnol. 2024;196(3):1272-1291.
Crossref - Orazi G, O’Toole GA. “It takes a village”: mechanisms underlying antimicrobial recalcitrance of polymicrobial biofilms. J Bacteriol. 2019;202(1):e00530-19.
Crossref - Pelegrin AC, Palmieri M, Mirande C, et al. Pseudomonas aeruginosa: a clinical and genomics update. FEMS Microbiol Rev. 2021;45(6):fuab026.
Crossref - Darch SE, McNally A, Harrison F, et al. Recombination is a key driver of genomic and phenotypic diversity in a Pseudomonas aeruginosa population during cystic fibrosis infection. Sci Rep. 2015;5(1):7649.
Crossref - Valcek A, Philippe C, Whiteway C, et al. Phenotypic characterization and heterogeneity among modern clinical isolates of Acinetobacter baumannii. Microbiol Spectr. 2023;11(1):e03061-22.
Crossref - Sutton JAF, Carnell OT, Lafage L, et al. Staphylococcus aureus cell wall structure and dynamics during host-pathogen interaction. PLoS Pathog. 2021;17(3):e1009468.
Crossref - Howden BP, Giulieri SG, Lung T WF, et al. Staphylococcus aureus host interactions and adaptation. Nat Rev Microbiol. 2023;21(6):380-395.
Crossref - Park JH, Shim D, Kim KES, Lee W, Shin SJ. Understanding metabolic regulation between host and pathogens: New opportunities for the development of improved therapeutic strategies against Mycobacterium tuberculosis infection. Front Cell Infect Microbiol. 2021;11:635335.
Crossref - Turner NA, Sharma-Kuinkel BK, Maskarinec SA, et al. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nat Rev Microbiol. 2019;(4):203-218.
Crossref - Del Pozo JL. Novel treatment dynamics for biofilm-related infections. Expert Rev Anti-infect Ther. 2021;19(11):1443-1456.
Crossref - Pandey N, Singh K, Ahmad F, Sharma R. Characterization of biofilm formation by Mycobacterium smegmatis during different environmental stress conditions: An in-vitro study. J Environ Biol. 2022;43(6):771-778.
Crossref - Jiang RD, Liu MQ, Chen Y, et al. Pathogenesis of SARS-CoV-2 in transgenic mice expressing human angiotensin-converting enzyme 2. Cell. 2020;182(1):50-58.
Crossref - Gambino M, Cappitelli F. Mini-review: Biofilm responses to oxidative stress. Biofouling. 2016;32(2):167-178.
Crossref - Derlon N, Peter-Varbanets M, Scheidegger A, Pronk W, Morgenroth E. Predation influences the structure of biofilm developed on ultrafiltration membranes. Water Res. 2012;46(10):3323-3333.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.