

The current pandemic of COVID-19 has caused havoc all over world since its emergence and rapid spread. Within three months the virus SARS-CoV-2 which was isolated from pneumonia cases in Wuhan City, Hubei Province, China in late December 2019, has affected almost all countries. India reported its first case of COVID-19 from state of Kerala on January 30, 2020, a student returned from city of Wuhan. Till date in India the disease had affected 12759 patients with 420 deaths. With every passing day the mysterious virus is been uncovered with its unique characteristics enabling the researcher to unfold the various methods including hand washing and social distancing to curtail the pandemic. Measures like 21 days lockdown to certain extent are effective but considering asymptomatic spreaders, extended measured lockdowns will be useful in the long term war against COVID-19. Till the vaccine and therapeutic solutions are derived, answer to pandemic and SARS-CoV-2 lies in lockdown, social distancing, contact tracing and containment.
Pandemic, COVID-19, SARS-CoV-2, Lockdown, PPE
The current pandemic of COVID-19 has caused havoc all over world since its emergence and rapid spread. On 9th January 2020, the World Health Organization announced a novel coronavirus, which was identified by Chinese researchers.1 The virus was associated with pneumonia outbreak which was traced to Huanan seafood market in Wuhan City, Hubei Province, China.2 International Committee of Taxonomy of Virus has named the novel virus as “SARS-CoV-2” and the disease it causes as “Corona Virus Disease 2019” (abbreviated “COVID-19”).3 On 30th January 2020, the WHO- International Health Regulations Emergency Committee declared the outbreak a “public health emergency of international concern external icon”. On 11th March, WHO announced COVID-19 as a pandemic.4 For pandemic COVID-19 WHO has published four scenarios/ stages as in Table 1 during its spread in a community.3
Table (1):
Stage of COCID-19 Transmission.
Stage No. |
Scenario/Stage in Transmission of COVID-19 in a Country |
|---|---|
1 |
No cases. |
2 |
With 1 or more sporadic cases, which may be imported or locally detected |
3 |
Clusters of cases in time, geographic location, or common exposure in the community |
4 |
Larger outbreaks of community or local transmission. |
WHO has advised measures like emergency response mechanism, education on risk communication and public engagement to help detect early COVID-19 cases. It also had advised for early case detection and management, respiratory disease surveillance, and public health management like hand hygiene, respiratory etiquettes and social distancing. Because of limited or no drug treatment available it advocates that best cure for COVID-19 is by preventing its rapid spread.3 With worlds second most population country, India is at high risk of the disease burden having social, economic and health impact in terms of morbidity and mortality. But with its aggressive implementation of WHO recommendations and innovative approach like public curfew, 21 days lockdown, Indian Government and health authorities have at least time being have halted the transmission scenario compared to few of the developed countries. We review the latest updates of COVID-19 and preventive measures and other probable factors which may be responsible for slow spread of SARS-CoV-2 in India.
Virus Family
Corona viruses group belongs to the family Coronaviridae, subfamily Orthocoronavirinae, and order Nidovirales.5 Of all the corona viruses identified so far, seven are found to be associated with human diseases including the emerging corona virus nominated as SARS-CoV-2.6 The corona viruses are classified into four different types which consists of alpha, beta, gamma and delta corona viruses. Two of the seven corona viruses affecting humans belong to alpha viruses which are 229E and NL63. The remaining five are beta corona viruses which include HKU 1, MERS-CoV which causes Middle East Respiratory Syndrome (MERS), SARS-CoV which causes Severe Acute Respiratory Syndrome (SARS) and the most recent one SARS-CoV-2 which is responsible for deadly disease COVID-19.3,5,7 The virus was first isolated from pneumonia outbreak in Wuhan City of Hubei Province in China and has spread globally in no time.8
COVID-19 Pandemic
As of now across all continents it had affected most countries, with 1,991,562 confirmed cases and 130,885 deaths.4 The pandemic has affected India with first case detected on 30th January 2020 , a student from state of Kerala who had returned from Wuhan, China. Numbers of cases raised to 3 by 3rd February with two more students returning from China were positive. The number did not raised significantly till March 4 when 22 new cases were positive including 14 Italian members of a tourist group. Escalation of disease occurred during March with numbers of sporadic cases reported across the country with history of travel to affected countries.
India reported its first death from COVID-19 positive case, a 76 year old who had returned from Saudi Arabia on March 12. Within two and half months the number of infected patients has gone up to 12759 with 1514 cured cases and total 420 deaths and one migrating to other country as per data on 16 the April 2020.9 The global death toll is rising at a rapid pace continuously and the disease is causing social, economic impact all over world including India causing life to a standstill.
Morphology of SARS CoV-2
The CoV-2 virus is enveloped, round single stranded RNA virus and it measures 60-140 nm in size. (Fig. 1) The envelop is having spikes of glycoproteins which gives it as appearance of crown on basis of which it is named as Corona.10
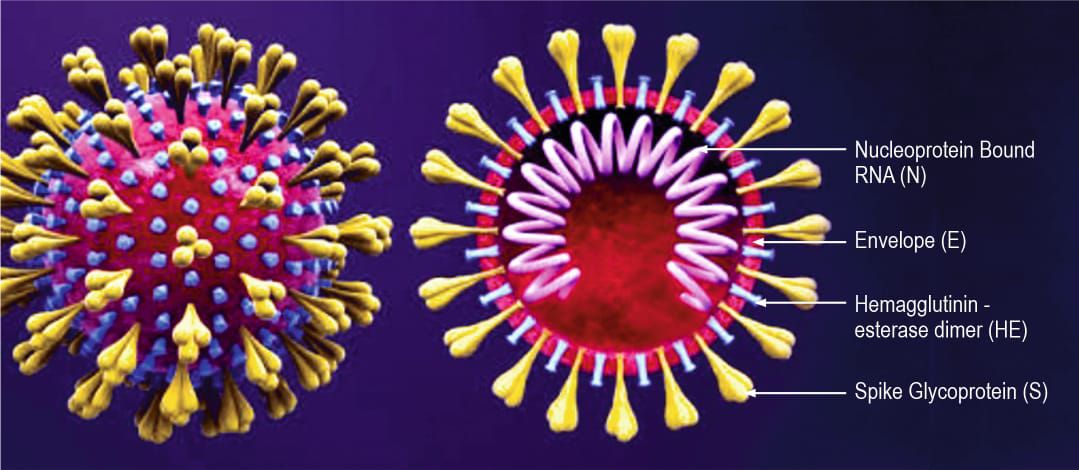
Fig. 1. SARS-CoV-2 Morphology
Genomic Structure
The RNA of the virus consists of 29891 nucleotides which encode total of 9860 amino acids. The nucleotide identity of SARS-CoV-2 matches with 89 % of bat SARS – like-CoV while 82 % of the nucleotides are having similarity with that of SARS-CoV 2002.11 The phylogenetic tree of various structure of the SARS-CoV-2 like orf1 a/b (Open Reading Frame), Spike (S), Envelope (E), Membrane (M) and Nucleoprotein (N) suggests that it is closely related with bat and human SARS-CoV. The major difference though in the SARS-CoV-2 and other SARS viruses lies in the external subdomain of spike’s receptor binding domain which has only 40 % identity. Also it has a novel protein encoded on the orf3b.11
Resistance
The virus is easily destroyed in heat and ultraviolet rays. The lipid solvents like ethanol, 75 % ether, hypochlorite, chloroforms and peroxy acetic acids effectively inactivates the virus.10
Surface stability
Recent study by Van Doremalen et al. had found the SARS-CoV-2 virus is viable in aerosols for three hours. 12 The virus remains alive for three days on stainless steel and plastic. The viability was 4 and 24 hours on copper and cardboard respectively. The study confirms the role of aerosol and fomite transmission as virus has remained viable in hours in aerosol and in days on surfaces.12
Transmission
Incubation period for the COVID-19 is 3 to 7 days but can get extended up to 12 days.13 Each COVID-19 patient transmits the infection to another 2.2 individual which is slightly less compared to SARS-CoV-2002 virus.14 Though the initial transmission was supposed to be from animals to human as per the reports from Huanan Sea Food Market, Wuhan, China further spread of the disease from epidemic to pandemic is human to human by respiratory droplets.10 The respiratory droplets or aerosols leave the patients mouth or nose during coughing or breathing out. The healthy individual gets infected by inhaling or contact from contaminated surface to his eyes, nose or mouth by hand. 3,10
Pathogenesis
The information gathered from COVID -19 patients so far suggests of increased immune response after entry of virus in host. Both nonstructural proteins (nsp) and structural proteins plays important role in patho-physiology and virulence. The virus envelope and spike proteins are important in virus entry, multiplication, assembly formation and release from host tissue which is respiratory cells in case of SARS-CoV-2 infection.15, 16 The spike proteins subunits S1 and S2 link the virus to host cell receptor. The virus multiplication provacates immune reaction in the patient releasing large amount of cytokines and chemokines. These includes IL 1, 7, 8, 9, 10, GCSF, GMCSF, IFNg, IP10, TNFα.17 This results in a reaction described as Cytokine Storm. As a result extensive tissue damage occurs. This has been confirmed on the basis of raised cytokine and chemokine specifically proinflammatory chemokines blood levels in patients with COVID-19.17 Study conducted by Pan et al. described four stages of pneumonia caused by COVID-19 on CT scan.18 In stage 1 that is in first 4 days ground glass opacity in the lower lobe with subpleural distribution in lower lobe is seen. In the second stage the ground glass opacity extends to bilateral multiple lobes with crazy paving pattern and consolidation which is seen in day 5 to 8. In the next four days, the stage 3 occurs in which dense consolidation goes to peak level in affected lung areas along with appearance of ground glass opacity, crazy paving pattern, after 14th day of appearance of symptoms gradual decrease in consolidation, crazy paving pattern occurs although ground glass is persistent for few more days.18
Clinical Features
Patients with COVID-19 manifests with pneumonia symptoms. Dry cough and fever not responding to antipyretics are characteristic features. After initial 8 to 10 days patients have shortness of breath indicating progression of the disease into acute respiratory distress syndrome.3,10 This complication usually is seen in older age group patients and patients with underlying predisposing conditions like diabetes mellitus and chronic heart disease. Other symptoms include severe body ache and diarrhea in few cases. Patients may suddenly develop hypoxia, tachypnoea and cyanosis in case of pediatric patients with oxygen saturation falling less than 90 %. Further sepsis may develop in with multi-organ failure specifically with renal involvement. Patient may present with altered sensorium, hypotension and sudden collapse.10,19 80 % of the patient recovers with mild disease while remaining patients may develop with moderate to severe stage of the COVID-19. So for mortality is seen in 2 to 6% of the patients in over all infected patients but if old age group is considered the mortality rate goes up to 8 to 10%.20
Laboratory diagnosis
Indication for COVID-19 Testing
Currently in India all international travelers are home quarantined. Symptomatic travelers with fever cough and breathlessness are hospitalized and tested immediately for COVID-19. Asymptomatic travelers are home quarantined for 14 days and tested only in case of symptoms. All members in the family of confirmed cases are home quarantined. Testing is indicated in all symptomatic contacts of laboratory confirmed cases, symptomatic health care workers, all admitted patients with ARDS. Health care workers who have used inadequate PPE as per WHO guidelines while examining a confirmed COVID 19 and family members residing with confirmed case are considered as high risk and direct contact group and must be tested on day 5 and 14 after coming in contact of a confirmed patient. 21,22
Specimen collection
Nasopharyngeal and oropharyngeal swabs are preferred specimens which have to be transported in viral transport medium (VTM) at 2 to 8 o C. Alternatively nasopharyngeal wash, endotracheal aspirate, or brancho- alveolar lavage can also be collected in VTM. The virus is also present in specimens like sputum, serum, blood, urine and stool. If there is likely delay in transport or testing of specimen for more than 5 days, it should be kept at – 70 oC. 23
RT PCR
Real time reverse transcriptase polymerase chain reaction (rRT PCR) is the test used for confirmation of diagnosis of SARS-CoV-2 infection. The S, E and N gene sequences of the virus are used for amplification which are spike, nucleocapsid and envelop antigen respectively. For RNA extraction BSL-2 is followed with PPE precautions. Any test kit with amplification of minimum two target sites or one target with genome sequencing confirms the disease condition in an area of otherwise COVID-19 free. In case of circulating COVID-19 in a area, single specific target amplification of COVID-19 is sufficient for diagnosis.23
Serology
Antibody detection rapid kits are available for testing on serum, plasma or blood specimens. Test is useful for detection of virus specific antibody only after 7 to 8 days of infection and gives results within 30 minutes. Serology tests are not recommended for the diagnosis of COVID-19.23
Managements
There are no specific antiviral drugs available for complete cure of the disease. Symptomatic management is the essential step to prevent complications in patient of COVID-19 .This includes nasal oxygen therapy, intubation in case of respiratory failure with ventilator support, ionotropic support in case of hypotension.10 The management has to be given by health care professional or worker with use of PPE which includes eye wear/goggles, N-95 mask , disposable theatre cap or face shield in case of intubating person, long sleeve gown or surgical gown, double gloves which may include a longer glove if required.10,24 Prophylactic antibiotics especially antimalarials chloroquine and hydroxychloroquine have been advocated in health care workers to prevent development of respiratory complications in many countries including India. 10,25 Combination use of lopinavir / ritonavir therapy on selected patients is been allowed in India considering its usefulness in SARS 2002 and MERS.26 Gordan et al. had found remdesivir a RNA polymerase inhibitor will be beneficial in patients suffering with COVID-19. 27 Early studies by Shen C. et al have found that convalescent plasma therapy containing neutralizing antibody have drastically improved the condition in critically ill patients of ARDS and COVID.28 Very recent study by Caly et al had encouraging findings for the antiparasitic drug ivermectin which had shown considerable antiviral activity against CoV-2 in their in vitro experiments.29 Ivermectin may be the wonder drug for the current pandemic once the clinical trials are completed.
Contact precautions and social distancing
Since there is no therapeutic solution for the virus till date, breaking chain of events in virus transmission is important to prevent infection from SARS-CoV-2. Regular hand washing with soap, water or sanitizer is advocated. Avoiding touching face is important to prevent virus entry via nose, mouth or eyes. Face has to be covered with hands, closed elbows or tissue paper during sneezing or coughing.3,10 Social distancing, avoiding unnecessary travels or keeping a safe distance of 1 meter from other person in a community, avoiding handshakes and hugs are important protocols. Wearing masks for a community person or PPE for health care worker while in contact with a confirmed COVID-19 person is key for halting transmission. Mask protocols like- changing, in case of wet mask or every six hourly, not touching outside of mask has to be followed.3, 10

Fig. 2. Number of COVID-19 cases in 21 Days Lockdown period in India
21 day lockdown
In one of the unprecedented move Prime Minister and Government of India announced a 21 day complete lockdown of the country starting from 24th of March 2020 to curb spread of COVID-19. Considering the spread rate of SARS-CoV-2 of 2.2 the epidemic could be delayed by 3 to 4 day by symptomatic testing and quarantine of international travelers as per initial strategy.30 But once these cases were responsible for local transmission, it is very important to test and isolate the contacts irrespective of symptom present or absent. Considering the testing load and limited testing and healthcare facility, it is very important to hold the community spread of the disease. The 21 day lockdown from 24th March 2020 with restriction on all people’s movement except the emergency services have to some extent broke the chain of transmission of the virus considering the 14 days of symptomatic phase of the disease. This is evident from Figure 2. The Centre for Disease Dynamics and Policy (CDDEP) has projected approximately 10 lakh COVID-19 cases by mid of April in India.31 The Government of India had claimed the projected number as 8.2 lakhs of cases without lockdown which ends on 14th April 2020.9 (Fig. 2) Tally of cases reached 1,251 with 35 deaths on March 31, at the end of first week of lockdown. By the end of second week of the lockdown on April 7, number of confirmed cases had raised to 4,778 with 124 deaths. By the last day of the 21- day lockdown, the death toll due COVID-19 stood at 339 with the number of cases escalating to 10,453 which was way below the projected number of cases. 9 This is attributed to effect of lockdown and other preventive measures. Though the number of new cases per day increased, the daily growth rate of confirmed new COVID-19 cases was on lower side.9 (Fig. 3) The linear trendline of growth rate showed declining trend across the period of 21 day lockdown as shown in Fig. 3. The lockdown also helped the health officials to establish better network of testing COVID-19 cases and creation of specialized isolation centers and testing centers for effective management including ventilator support in ARDS patients. The stay at home and work from home policy have further aided in restricting the disease in a particular area or local region preventing the mass or community spread on a large scale. What we feel is, considering the transmission of virus in asymptomatic phase in first few days of the COVID-19 confirmed cases 32 and late upsurge of COVID-19 cases in India especially in late part of third week of lockdown, it should be further extended in the country to prevent escalation of condition.
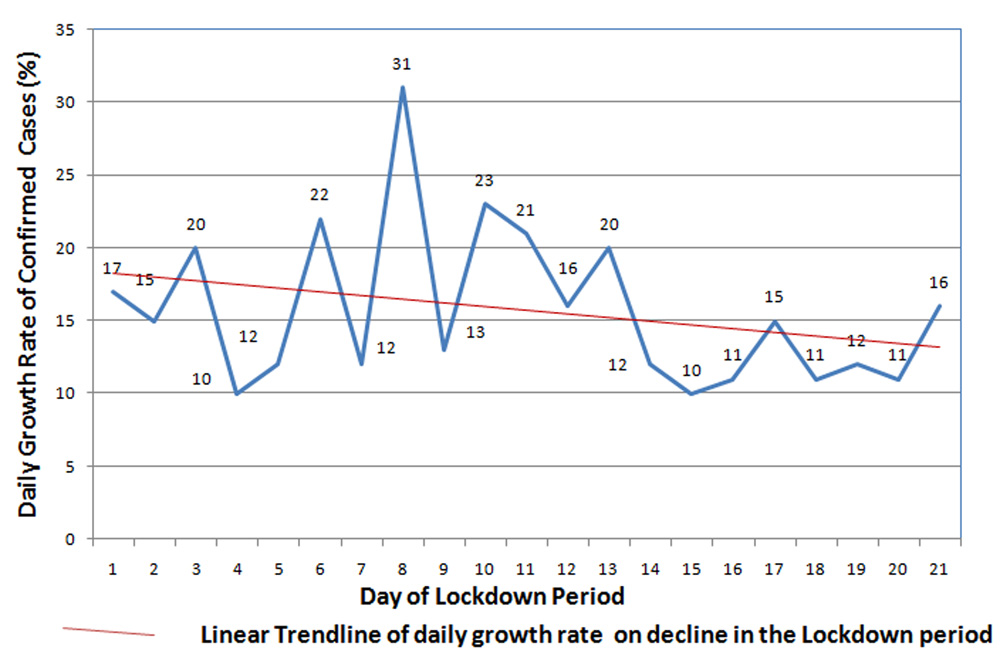
Fig. 3. Daily growth rate of COVID-19 confirmed cases (%) in 21 days lockdown period in India
Low transmission of COVID-19 in India
In India, rate of viral transmission is somewhat low considering the number cases in the period compared to few developed countries like USA, Italy, United Kingdom, Spain, and other European countries. The mortality rate is 4 to 10 % globally though it is comparatively less in India (2.75%). 33, 34 In old age group (age > 60 years) the mortality rate is up to 14 % above 80 years in Italy compared to 10 % in Wuhan.33 The lower rate in India might be related to less number of testing, but other factors like age distribution have played significant role. Only 6.4 % of Indian population is above 65 % compared to 22 % in Italy.34 The agent SARS-CoV-2 is having two types the S type which is original and L type which is aggressive mutant though type which is circulating predominantly in India is not known.35
Many studies have proved presence of better innate defense mechanism in Indian population. This is based on existence of higher killer cell immunoglobulin receptor gene, the hypothesis based on natural selection theory.36 More number of natural killer cells are present in Indian population which are prime in immunity against new type of viruses.37 Geographical location and data so far collected has shown that COVID-19 is so far having less mortality in malaria endemic countries including India. Role of BCG vaccination in COVID-19 protection has become a research question considering the stimulation of IL-1 which plays important role in viral immunity with studies pointing to reduced mortality in BCG vaccinated population.38
Environmental condition like temperature is one of the key factor in transmission of the virus though a lot of work has to be done to come to a conclusion. A study in china has found that optimum temperature is 8.72 °C for virus spread and number of cases was inversely proportional to every one degree rise in temperature. 39 Global Virus network has concluded that virus is more prevalent in countries between 30-50” N latitude countries with temperature between 5 to 11 °C and humidity between 47 % to 79 %.40 Naturally these parameter and 21 day lockdown is helping India to prevent escalation of COVID 19 spread. First few day of lockdown in India has seen number cases increasing but rate of increase in cases is steady or on decline.
COVID-19 Discharge policy
Patient of COVID-19 is discharged only after two respiratory specimens collected 24 hours apart, are virus free or negative by rRT PCR. If the patient is symptom free within seven days second specimen is collected seven days apart. Even after discharge patient is home quarantined for 14 days to prevent spread of infection. 41
Vaccine update
Vaccine trials have already started across globe with most focusing on spike protein. It will be year or so to complete the clinical trials and to assess the results of vaccine.42
With the rapid rate of its spread the COVID-19 pandemic has already made a catastrophic mark in this century. Till the researcher find a complete therapeutic solution or vaccine for the disease, social distancing, contact precautions and tracing, lockdowns, containment are the best remedy. In case of presence of clusters of COVID-19 patients, even after end of complete lockdown we suggest implementation of measured lockdowns in selected area of the country to curtail the pandemic. Perhaps answer to spread of pandemic COVID-19 was given century back by Sir William Osler in his quote “Soap, water and commonsense are the best disinfectants!”
ACKNOWLEDGMENTS
Authors are thankful to Mr. Dhananjay Kulkarni artist, for his creative work from home in preparing the SARS- CoV-2 image in this lockdown period.
CONFLICT OF INTEREST
The authors declare no conflict of interest, including competing or financial.
AUTHORS’ CONTRIBUTION
Both authors have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
ETHICS STATEMENT
This article does not contain any studies with human participants or animals performed by any of the authors.
AVAILABILITY OF DATA
Not applicable.
- WHO. https://www.who.int/health-topics/coronavirus/who-recommendations-to-reduce-risk-of-transmission-of-emerging-pathogens-from-animals-to-humans-in-live-animal-markets. Accessed 31 March, 2020.
- Wang W, Tang J, Wei F. Updated understanding of the outbreak of 2019 novel corona virus (2019-nCoV) in Wuhan, China. J Med Virol. 2020;92(4):441-7.
Crossref - WHO.https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/. Accessed 31 March, 2020.
- WHO. Coronavirus disease (COVID-19) outbreak situation. https :// www. who.int/ emergencies/ diseases/novel-coronavirus-2019.Accessed 16 april, 2020.
- Groot RJD, Baker SC, Baric R, et al. Virus taxonomy:classification and nomenclature of viruses. Ninth Rep Int. Comm. Taxon. Viruses. 2011;806-28.
- Lau SK, Lee P, Tsang AK, et al. Molecular epidemiology of human coronavirus OC43 reveals evolution of different genotypes over time and recent emergence of a novel genotype due to natural recombination. J Virology. 2011;85(21):11325-37.
Crossref - Vassilara F, Spyridaki A, Pothitos G, Deliveliotou A, Papadopoulos A. A rare case of human coronavirus 229E associated with acute respiratory distress syndrome in a healthy adult. Case reports in infectious diseases. 2018.
Crossref - Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;24:727-33. https://doi.org/10.1056/NEJMoa2001017
- GOI. https://www.mygov.in/covid-19/. Accessed 16 April, 2020.
Crossref - Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. Features, Evaluation and Treatment Coronavirus (COVID-19). InStatPearls [Internet] 2020 Mar 8. StatPearls Publishing.
- Chan JF, Kok KH, Zhu Z, et al. Genomic characterization of the 2019 novel human-pathogenic corona virus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerging Microbes & Infections. 2020;9(1):221-3.
Crossref - van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. New England J Med. 2020.
Crossref - Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382:1199-207.
Crossref - Bauch CT, Lloyd-Smith JO, Coffee MP, Galvani AP. Dynamically modeling SARS and other newly emerging respiratory illnesses: past, present, and future. Epidemiol. 2005:791-801.
Crossref - Lei J, Kusov Y, Hilgenfeld R. Nsp3 of coronaviruses: Structures and functions of a large multi-domain protein. Antiviral Res. 2018;149:58-74.
Crossref - Song W, Gui M, Wang X, Xiang Y. Cryo-EM structure of the SARS coronavirus spike glycoprotein in complex with its host cell receptor ACE2. PLoS pathogens. 2018;14(8):e1007236.
Crossref - Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;26:102433.
Crossref - Pan F, Ye T, Sun P, et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology. 2020:200370.
Crossref - Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506.
Crossref - WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report
- WHO. Coronavirus disease (COVID-19) technical guidance: Early investigations protocols. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/early-investigations
- ICMR. Revised Strategy of COVID19 testing in India https://www.icmr.gov.in/ [ Accessed 02 April, 2020]
- WHO Coronavirus disease (COVID-19) technical guidance: COVID-19 Critical Items. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/covid-19-critical-items. Accessed 02 April, 2020.
- Bedford J, Enria D, Giesecke J, et al. COVID-19: towards controlling of a pandemic. The Lancet. 2020;395:1015-18.
Crossref - WHO. Clinical management of severe acute respiratory infection (SARI) when COVID 19 disease is suspected. https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected
[ Accessed 02 April, 2020] - Bhatnagar T, Murhekar MV, Soneja M, et al. Lopinavir/ritonavir combination therapy amongst symptomatic coronavirus disease 2019 patients in India: Protocol for restricted public health emergency use. Indian J Med Res. 2020 Mar 11.
Crossref - Gordon CJ, Tchesnokov EP, Feng JY, Porter DP, Gotte M. The antiviral compound remdesivir potently inhibits RNA-dependent RNA polymerase from Middle East respiratory syndrome coronavirus. J Biologl Chem. 2020:jbc-AC120.
Crossref - Shen C, Wang Z, Zhao F, Yang Y, Li J, Yuan J. Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma. JAMA. 2020.
Crossref - Caly L, Druce JD , Catton MG, Jans DA, Wagstaff KM. The FDA approved. Drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antiviral Research.
Crossref - Mandal S, Bhatnagar T, Arinaminpathy N, et al Prudent public health intervention strategies to control the coronavirus disease 2019 transmission in India: A mathematical model-based approach. Indian J Med Res. 2020;151.
Crossref - Centre for Disease Dynamics and Policy (CDDEP). COVID-19 for India Updates https://cddep.org/wp-content/uploads/2020/03/covid19.indiasim.March23-2-eK.pdf
- Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y. Early transmission dynamics in Wuhan, China,of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382:1199-1207.
Crossref - The Centre for Evidence-Based Medicine. Global Covid-19 Case Fatality Rates. https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates/. Accessed 06 april, 2020.
- Indexmundi . Population Peramid.
[ Accessed 31 March, 2020] - Tang X, Wu C, Li X, et al. On the origin and continuing evolution of SARS-CoV-2. National Science Review. https: //academic.oup.com /nsr/ advance-article-abstract /doi /10.1093/ nsr /nwaa036/5775463Accessed 31 March, 2020.
Crossref - Du Z, Sharma SK, Spellman S, Reed EF, Rajalingam R. KIR2DL5 alleles mark certain combination of activating KIR genes. Genes & Immunity. 2008;9(5):470-80. https://doi.org/10.1038/gene.2008.39
- Nature India. More immunity genes in Indians.
Crossref - Miller A, Reandelar MJ, Fasciglione K, Roumenova V, Li Y, Otazu GH. Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study. medRxiv. 2020.
- Wang J, Tang K, Feng K, Lv W. High Temperature and High Humidity Reduce the Transmission of COVID-19. https://papers.ssrn.com /sol3/papers.cfm?abstract_id= 3551767. Accessed 31 March, 2020.
Crossref - Global Virus Network. Enhanced Model For Monitoring Zones Of Increased Risk Of COVID-19 Spread. https://gvn.org/enhanced-model-for-monitoring-zones-of-increased-risk-of-covid-19-spread/ Accessed 31 March, 2020.
- WHO : https://www.who.int/publications-details/global surveillance-for-human-infection-with-novel-coronavirus-(2019-ncov) [ Accessed 31 March, 2020]
- Bilal M, Nazir MS, Parra-Saldivar R, Iqbal HM.2019-nCoV/COVID-19 – Approaches to Viral Vaccine Development and Preventive Measures. J Pure App Microbiol. 2020;14(1):25-29.
Crossref
© The Author(s) 2020. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.