

The current global health emergency, COVID-19, is not the first time that coronaviruses have posed a threat to human world shrinking our numbers by thousands. Before this SARS-CoV in 2003 and MERS-CoV in 2013 have caused epidemics. Four months in existence, and it has already affected 1,995,983 people and taken over 131,037 lives worldwide, yet we do not have any specific treatment available with us and the management is purely empirical. Looking at the similarities between SARS-CoV and SARS-CoV-2 in origin, genomics, pathogenesis and epidemiology, we can bring the researches done for SARS-CoV in use which can be our guide in finding an effective management strategy against SARS-CoV-2. There are various researches and studies reporting the use and effect of various phytochemical compounds in SARS-CoV treatment. Already, the thought has been put into action and in-silico screening for various natural plant compounds have been done to find a potential candidate compound. One such example is of curcumin, a secondary metabolite of turmeric, which is found to be effective against COVID-19 protease by molecular docking analysis.
Coronavirus, SARS-CoV, Herbal medicine, Complementary medicine
Coronaviruses are well known pathogenic organisms of humans and animals which cause a broad spectrum of respiratory, gastrointestinal, neurological and systemic diseases1.
Deriving its name from the word ‘corona’2 meaning outer fringe(because of the presence of spiky outer enveloped protein coat), coronaviruses belong to the family Coronaviridae which are further subdivided into four genera namely, Alphacoronavirus, Betacoronavirus, Gammacoronavirus and Deltacoronavirus3.
Table (1):
Recognised strains of Coronavirus affecting humans.
Alphacorona virus |
HCoV- 229E |
HCoV-NL63 |
|
Betacorona virus |
HCoV-OC43 |
HCoV-HKU1 |
|
SARS-CoV |
|
MERS-CoV |
|
SARS-CoV-2 |
Evolution of Covid-19
The genera Alphacoronaviruses and Betacoronaviruses contain viruses infecting both humans and animals (Table 1)4,5 while the genus Gammacoronavirus and Deltacoronavirus contains viruses specifically infecting animals (Table 2)4; the first one being seen in whales and birds, and the latter ones are isolated from pigs and birds4.
Table (2):
Recognised strains of Coronavirus affecting animals.
Alphacorona virus |
Mi-BatCoV-HKU7 |
Mi-BatCoV-HKU8 |
|
Mi-BatCoV-1A |
|
Mi-BatCoV-1B |
|
Rh-BatCoV-HKU2 |
|
PEDV |
|
My-BatCoV-HKU6 |
|
Sc-BatCoV-512 |
|
Hi-BatCoV-HKU10 |
|
Ro-BatCov-HKU10 |
|
TGEV |
|
FIPV |
|
PRCV |
|
Betacorona virus |
|
β-CoV A |
RCoV Parker |
MHV |
|
RbCoV HKU14 |
|
Antelope CoV |
|
B CoV |
|
E CoV |
|
PHEV |
|
DcCoV-UAE-HKU23 |
|
β-CoV B |
SARSr-Rh batCoV-HKU3 |
SARSr-CiCoV |
|
β-CoV C |
Erinaceous CoV |
MERS-CoV |
|
Neo-CoV |
|
Ty-batCoV-HKU4 |
|
Pi-BatCoV-HKU5 |
|
KSA-Camel-363 |
|
β-CoV D |
Ro-Bat-CoV-HKU9 |
γ-CoV |
IBV-partridge |
TCoV |
|
IBV-peafowl |
|
BdCoV-HKU22 |
|
BWCoV-SW1 |
|
δ-CoV |
NHCoV HKU19 |
WiCoV HKU20 |
|
CmCoV HKU21 |
|
MunCoV HKU13 |
|
MRCoV HKU18 |
|
PorCoV HKU15 |
|
SpCoV HKU17 |
|
WECoV HKU16 |
|
ThCoV HKU12 |
|
BuCoV HKU11 |
Discovered in early 1930’s as a pathogen causing mild respiratory infection in domesticated chickens1 coronaviruses gained major attention in 2003 after the emergence of SARS(Severe Acute Respiratory Virus) which caused a major global epidemic wiping out thousands of global population.
Before 2003 epidemic was inked in the history of humankind, coronaviruses were known to cause mild respiratory infections. It was the first time, when coronaviruses were seen posing such a serious threat. This was a game-changing event which led to various researches. As reported, SARS was known to be caused by cross species transmission- from bats to humans.
Since then, coronaviruses are seemingly undergoing variety of mutations and leaping into humans causing infections, both mild and severe. After SARS, four more strains of coronaviruses have been recognised till now of which two strains namely, HCoV HKU-1 and NL63 are known to cause mild respiratory disease while two strains namely, MERS-CoV and SARS-CoV-2 have caused epidemics affecting human population in large numbers and severity1. All the seven strains of coronaviruses recognised in humans are known to jump to humans from animals crossing species barrier (Fig. 1). The progenitor viruses of the recognised strains are seen in different host animals. HCoV- NL63, HCoV-229E, MERS- CoV and SARS- CoV are considered to have their origin in bats while HCoV-HKU1 and HCoV-OC43 are most likely to be originated from rodents3,6,7. Domesticated animals may play important roles as intermediate hosts which enable transmission of these viruses from their natural hosts to humans. SARS-CoV finds its intermediate hosts in civets3,8,9, HCoV-229E in camelids while MERS-CoV most likely found its way to humans through dromedary camels3,10.
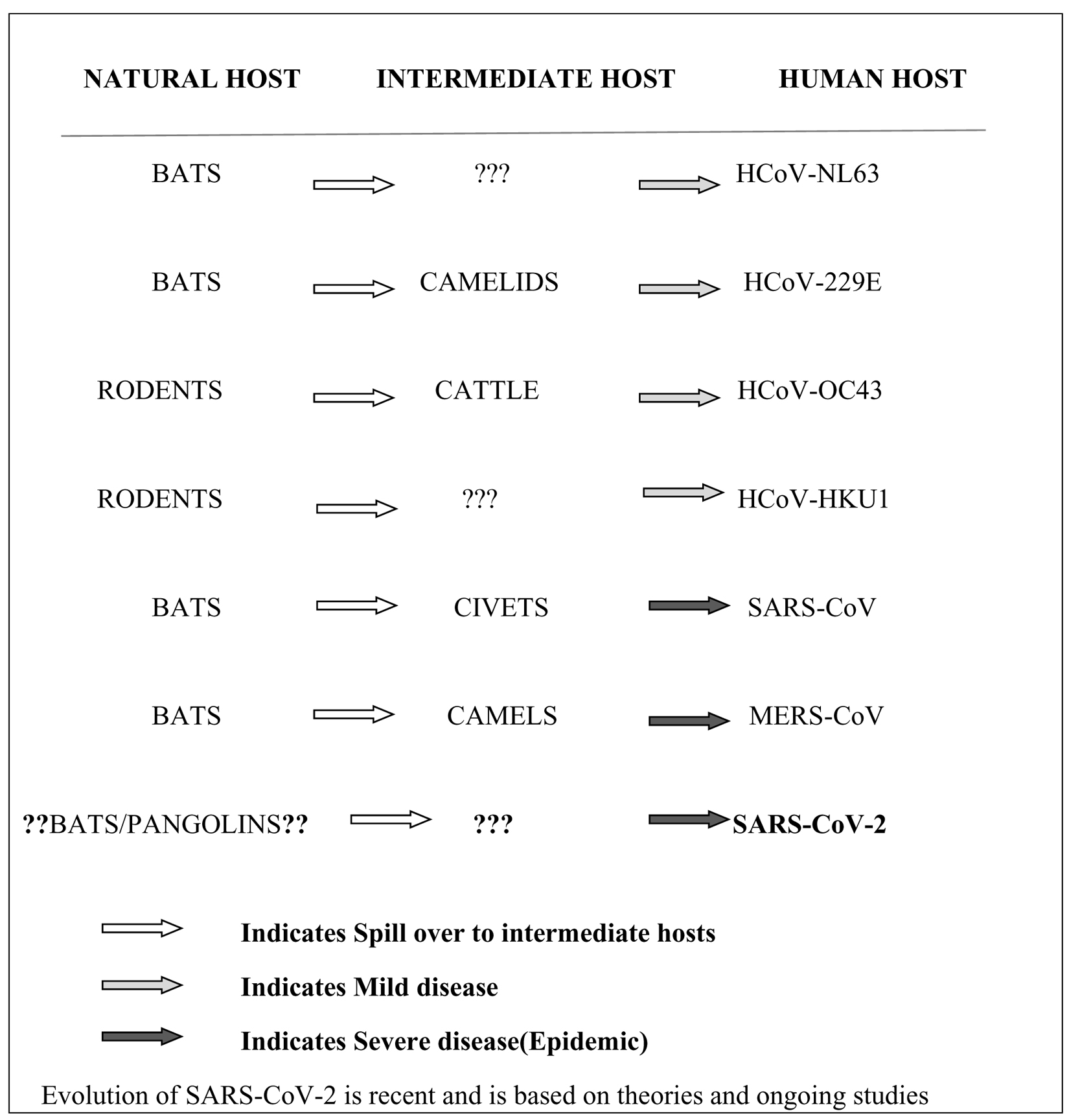
Fig. 1. Evolution of various strains of recognised human coronavirus from natural to human host
The latest recently recognised strain of all, SARS-CoV-2, was recognised in December 2019, in Wuhan city of China. Seeing its genomic similarity with SARS-CoV, it is thought to have paved its way to humans from animals through the live animal markets of China. The two probable theories of the origin of the virus gives bats11-13 or pangolins13, 4 as the natural host of the virus, bats being the most closest. The virus, likely, then mutated and evolved to spread most probably though an intermediate animal bridge to humans and now human to human transmission can be easily noted.
Being of the common origin as of SARS-CoV, it was hypothesized that the virulence of SARS-CoV-2 will also be affected by the increasing temperatures especially above 39°C (same as in case of SARS-CoV). According to the various studies conducted in this regard, the result remains inconclusive. According to a study conducted in China, COVID-19 mortality decreased with increase in ambient temperature (above 39°C) along with increased absolute humidity15. A study conducted by Wang et al.16 showed reduction in transmission of the disease while studies conducted by Ye Tao et al.17 and Zhu et al.18 showed ambient temperature had no effect on the transmission of SARS-CoV-2.
Complementary Medicine
Since the emergence of human race, plants have been the source of countless compounds having medicinal properties and lead to drug discovery. Since the ancient times, Indian Ayurveda, Traditional Chinese Medicine Literature, ancient Egyptian Ebers Papyrus all gives description of various plants and herbs having medicinal properties which are even today used all over the world for various health benefits. Different plant compounds act as immune boosters and can act as antibacterials, antivirals as well as antifungals. The coronaviruses encodes various proteins which enables its functioning. Many plants produce compounds interfere with these proteins and can become a target for drug development. Since the gene sequence of COVID-19 has very high similarities between the man proteins of COVID-19 and in SARS or MERS, thus previously reported anti-SARS or anti-MERS natural compounds may become a valuable guide to find the affective anti-COVID-19 herbal plants (Table 3).
Table (3):
Plant products effective against various strains of Human Coronavirus.
Virus |
Plant/Plant Product |
Mode of Action |
Reference |
|---|---|---|---|
SARS-CoV |
Phenolic plant compounds and Extract of roots of Isatis indigotica |
Inhibits SARS-3CLpro enzyme activity |
[28,29] |
Flavanoid Baicalin from Scutellaria baicalensis |
Inhibits Angiotensin Converting Enzyme |
[30,31,32] |
|
Water extract of Houttuynia cordata |
Inhibit the activity of viral SARS-3CLpro Block viral RNA-dependent RNA polymerase activity |
[32,33,34] |
|
Glycyrhizzin from the liquorice roots |
Affects various cellular signalling pathways |
[35,36,37] |
|
Mannose-specific plant lectins derived from Galanthus nivalis ,Hippeastrum hybrid and Allium porrum |
Inhibition of virus replication at an early stage by blocking S- receptor interaction |
[35, 38, 39] |
|
Reserpine derived from various species of Rauwolfia |
Inhibits replication of SARS-CoV |
[35, 40] |
|
Scutellarein and myricetin |
Inhibit nsP13 helicase by affecting the ATPase activity |
[32,41] |
|
Escin from horsechestnut |
[35, 42] |
||
Extracts of Rheum palmatum |
Inhibit SARS-3CLpro activity |
[32, 43] |
|
Flavonoids (herbacetin, pectolinarin, epigallocatechin gallate, rhoifolin,quercetin, and gallocatechin gallate) |
Inhibit SARS-3CLpro activity |
[32,44, 45, 46] |
|
Quercetin and TSL-1 from leaves of Toona sinensis Roem |
Inhibit the cellular entry of SARS-CoV |
[32, 47] |
|
Emodin derived from genus Rheum and Polygonum |
Inhibits interaction of SARS-CoV spike protein and ACE2 Blocks 3a ion channel inhibiting SARS-CoV triggered apoptosis |
[32, 48, 49] |
|
Tetra-O-galloyl-β-D-glucose from Galla chinensis |
Binds with surface spike protein thus interrupting with membrane fusion of SARS-CoV |
[32, 50] |
|
Luteolin from Veronicalina riifolia |
Binds with surface spike protein thus interrupting with membrane fusion of SARS-CoV |
[32, 50] |
|
Lycorine extracted from Lycoris radiate |
Unclear |
[51] |
|
Ginsenoside-Rb1 from Panax ginseng |
– |
[40] |
|
Biflavonoids(Amentoflavone, apigenin,quercetin,luteolin) from Torreya nucifera |
Inhibits SARS-CoV 3CL pro activity |
[52] |
|
Kaempferol derivatives |
Interfers with 3a ion channel of SARS CoV |
[32, 53] |
|
Dieckol from edible brown algae Ecklonia cava |
Inhibits SARS-CoV 3CLpro activity |
[54] |
|
MERS-CoV |
Herbacetin, quercetin, isobavaschalcone, 3-β-D glucoside and helichrysetin |
Inhibits cleavage activity of 3CLpro enzyme |
[32, 55] |
HCoV-229E |
Saikosaponins A,B2,C,D (from Bupleurum spp., Heteromorpha spp., Scrophularia scorodonia) |
Inhibits viral attachment and penetration at an early stage(saikosaponin B2) |
[29, 56] |
HCoV-OC43 |
Tetrandrine, fangchinolif ne, and cepharanthine |
Inhibit the expression of HCoV- OC43 spike and nucleocapsid protein. Immunomodulation |
[32,57, 58] |
Emodin derived from genus Rheum and Polygonum |
Blocks 3a ion channel inhibiting HCoV-OC43 triggered apoptosis |
[32,49, 49] |
There are more than a dozen of proteins which are encoded by coronavirus. Some of these proteins are essential to viral entry and replication. Papain-like protease (PLpro), 3C-like protease (3CLpro) and spike protein are the well studied proteins so far. All of these three proteins make attractive targets for drug development. Some of the herbal plants have been screened in silico by Narges & Neda 2020 to find the inhibitors for COVID-19 proteases, which could be an effective strategy for combating against this deadly virus. Due to the strong interaction of these natural compounds with enzymatically conserved regions and specific functionality, these compounds can be considered as effective antiviral drugs due to their natural origin and less likely to produce adverse effects if they enhance the interaction. Out of the eight tested secondary compounds curcumin was found to have strong interaction with protease of COVID- 1919. In another studies in silico screening with AI has been performed. It is a very fast method of screening reducing the cost of experiment as well as few human trials are required which leads to a fast development of drug20.
Until now, many existing allopathic drugs are also being tried continuously which may prevent worsening of the clinical condition of the patient and provide them early relief. Some of them being given to the patients include remdesivir, lopinavir, chloroquine or hydroxychloroquine and interferon beta-1a. Recently, convalescent plasma therapy is being tried21. But all these medicines have many potentially serious side effects thus limiting their use to critical patients only. Moreover, the efficacy of these medicines has not yet been proven and thus are restricted to compassionate use only22 (Table 4).
Table (4):
Commonly used Allopathic Medicines in COVID-19.
Drug |
Initial Use |
Mechanism of Action |
Side Effects |
References |
|---|---|---|---|---|
Remdesivir |
Ebola virus |
Inhibits viral RNA polymerase |
Kidney injury |
[21, 23,59] |
Lopinavir |
Anti HIV |
Acts against viral 3CL protease |
Gastrointestinal intolerance, Pancreatitis, cardiac conduction abnormalities, hepatotoxicity |
[21,23, 60] |
Chloroquine |
Antimalarial |
Decrease Lysosomal autophagy preventing entry of virus |
Abdominal cramps,anorexia, diarrhea,nausea, vomiting. Cardiovascular effects (QTc prolongation), hematologic effects (including hemolysis with G6PD deficiency), hypoglycemia, retinal toxicity, neuropsychiatric and central nervous system effects, idiosyncratic adverse drug reactions |
[21, 23, 61] |
Interferon beta-1a |
Treatment of Multiple Sclerosis |
Interfere with viral replication and up regulates CD73 in pulmonary endothelial cells |
injection site reactions, flu-like symptoms, headache, muscle aches, nausea, pain, fever, diarrhea, infections. |
[23, 62] |
Randomised Control Trials are continuously being done to see and prove the efficacy of these drugs and to find an appropriate effective treatment. One of the biggest international clinical trials is being conducted by WHO which has been given the name “Solidarity”. Seeing the urgency of the need of an effective treatment against the COVID-19, this trial is said to reduce the normal time taken by 80%. Four regimens are currently included namely, remdesivir, lopinavir with ritonavir, chloroquine or hydroxychloroquine and lopinavir with ritonavir with interferon beta-1a23.
Although same is the case with complementary medicine and their use is dependent upon their recorded effects in the treatment of SARS and MERS and upon the various small clinical trials and that their efficacy against COVID-19 is not yet proven, but the lack of potentially serious side effects gives us a possible and much needed window for their use in the treatment of COVID-19 not only in critical patients but also in patients with mild clinical disease. Although complementary medicine cannot replace modern medicine but can act as its supplementary. The integrated treatment can be clinically more effective and decrease the suffering of the patient in both time and severity. National Health Commission of the People’s Republic of China, on Feb 17, reported that 60,107 confirmed COVID-19 patients were successfully treated with integration of Western medicine and Traditional Chinese Medicine24,25. Also, traditional pool can be exploited as a prophylactic medicinal source against the disease especially in high risk population by boosting up immunity, blocking the infection, cutting off the inflammatory storm and promoting repair of the body24.
Although modern medicine came over traditional medicine in Darwinian process especially in developed countries, it is still being used widely by much of the population especially in developing countries. In fact, the trend is continuously growing towards the use of traditional medicine which is now no longer “the poor man’s alternative to conventional care”26. Although the ancient traditional medicine seriously lacks validation and standardization27, but the increasing tilt of the society towards the alternative medicine source due to widespread increasing rate of chronic diseases as well as lack of modern allopathic medicine in treating various infectious diseases due to antimicrobial resistance, has lead to various researches and studies which proves their efficacy and safety in various advanced clinical trials. Lately, when the world is under attack by COVID-19 and where modern medicine is incapable of saving us our heads turn towards the traditional medicinal source to be our shield. A lot of researches are being done to find the potential candidates from the conventional herbal pool which can prevent the spread and stop the effect of the virus.
In view of such newly emerging and re-emerging infectious diseases such as Ebola virus, Nipah virus, Zika virus, COVID-19, having potential to cause epidemics and thus seriously affect the human race not only in severity but also in numbers, traditional medicine can lend us a way out which, as quoted by WHO, is the care that is close to homes, generally available, accessible, affordable and sometimes the only care available to people at primary health care level26.
ACKNOWLEDGMENTS
Not applicable.
CONFLICT OF INTEREST
The authors declares that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
ETHICS STATEMENT
Not applicable.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript and/or the Supplementary Files.
- Peiris JSM. Coronaviruses. Viral Pathogens and Associated Diseases, 587-593.
- Sturman LS, Holmes KV. The molecular biology of coronaviruses. Advances in Virus Research. 1983;28:35–112.
- Cui J, Li F, Shi ZL. Origin and evolution of pathogenic Coronaviruses. Nat Rev Microbiol. 2019;17(3):181-192.
- Burrell CJ, Howard, CR, Murphy FA. Coronaviruses. Fenner and White’s Medical Virology (Fifth Edition) 2017; 437-446.
- Ko WC, Rolain JM, Lee NY, et al. Arguments in favour of remdesivir for treating SARS-CoV-2 infections. Int J Antimicrob Agents.2020; 105933.doi: 10.1016/j.ijantimicag.2020.105933
- Su S. et al. Epidemiology, genetic recombination and pathogenesis of coronaviruses. Trends Microbiol. 2016;24:490–502.
- Forni D, Cagliani R, Clerici M, Sironi M. Molecular evolution of human coronavirus genomes. Trends Microbiol. 2017; 25:35–48.
- Chinese SMEC. Molecular evolution of the SARS coronavirus during the course of the SARS epidemic in China. Science. 2004;303:1666–1669.
- Song HD, et al. Cross- host evolution of severe acute respiratory syndrome coronavirus in palm civet and human. Proc. Natl Acad. Sci. USA. 2005;102:2430–2435.
- Muller MA et al. MERS coronavirus neutralizing antibodies in camels, Eastern Africa, 1983–1997. Emerg. Infect. Dis. 2014;20:2093–2095.
- Wu F, Zhao S, Yu B et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579:265–269.https://doi.org/10.1038/s41586-020-2008-3
- Zhou P, Yang X, Wang X, et al.A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579:270–273.
- Andersen KG, Rambaut A, Lipkin WI, Holmes EC, Garry RF. The proximal origin of SARS-CoV-2. Nature Medicine. 2020;26:450–452.
- Zhang T, Wu Q, Zhang Z. Pangolin homology associated with 2019-nCoV. bioRxiv. 2020.https://doi.org/10.1101/2020.02.19.950253.
- Ma Y, Zhao Y, Liu J, et al. Effects of temperature variation and humidity on the death of COVID-19 in Wuhan, China. medRxiv. 2020. https://doi.org/10.1101/2020.03.15.20036426
- Wang J, Tang K, Feng K, Lv W. High temperature and high humidity reduce the transmission of COVID-19. arXiv. 2020. arXiv:2003.05003[q-bio.PE]
- Yao Y, Pan J, Liu Z,et al. No Association of COVID-19 transmission with temperature or UV radiation in Chinese cities. European Respiratory Journal. 2020. DOI: 10.1183/13993003.00517-2020.
- Xie J, Zhu Y. Association between ambient temperature and COVID-19 infection in 122 cities from China. The Science of the Total Environment. 2020;724:138201.
- Mohammadi N, Shaghaghi N. Inhibitory effect of eight Secondary Metabolites from conventional Medicinal Plants on COVID_19 Virus Protease by Molecular Docking Analysis. chemrvix, 2020. doi.org/10.26434/chemrxiv.11987475.v1.
- Zhang DH, Wub KL, Zhang X, Deng SQ, Peng B. In silico screening of Chinese herbal medicines with the potential to directly inhibit 2019 novel coronavirus. Journal of Integrative Medicine. 2020;18:152–158.
- Sanders JM, Monogue ML,Jodlowski TZ, Cutrell JB. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA. 2020. doi:10.1001/jama.2020.6019 .
- Holshue ML, DeBolt C, Lindquist S, et al. First Case of 2019 Novel Coronavirus in the United States. N Engl J Med. 2020;382:929-936.
- World Health Organisation. Solidarity clinical trial for COVID-19 teatments. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-clinical-trial-for-covid-19-treatments.
- Ren J-ling, Zhang A-Hua, Wang X-Jun. Traditional Chinese Medicine for COVID-19 Treatment. Pharmacological Research. 2020. https://doi.org/10.1016/j.phrs.2020.104743
- Publicity Department of the People’s Republic of China. Press conference of the joint prevention and control mechanism of state council on Feb 17, 2020. http://www.nhc.gov.cn/xcs/fkdt/202002/f12a62d10c2a48c6895cedf2faea6e1f.shtml
- World Health Organization. Address at the WHO Congress on Traditional Medicine by Dr. Margaret Chan Director- General of WHO, 2008. https://www.who.int/dg/speeches/2008/20081107/en/
- World Health Organisation. Traditional Medicine: Modern Approach for Affordable Global Health. World Health Organisation, Innovation on Intellectual Property, Innovation and Public Health. 2005.
- Lin CW, Tsai FJ, Tsai CH, et al. Anti‑SARS coronavirus 3C‑like protease effects of Isatis indigotica root and plant‑derived phenolic compounds. Antivir Res. 2005;68:36‑42.
- Lin LT, Hsu WC, Lin CC. Antiviral Natural Products and Herbal. J Tradit Complement Med. 2014;4(1):24–35.
- DengYF, Aluko RE, Jin Q, Zhang Y, Yuan LJ. Inhibitory activities of baicalin against renin and angiotensin-converting enzyme. Pharm Biol. 2012;50:401-406.
- Chen Z, Nakamura T.Statistical evidence for the usefulness of Chinese medicine in the treatment of SARS. Phytotherapy Research: PTR. 2004;18:592-594.
- Yang Y, Islam MS, Wang J, Li Y, Chen X. Traditional Chinese Medicine in the Treatment of Patients Infected with 2019-New Coronavirus (SARS-CoV-2): A Review and Perspective. Int J Biol Sci. 2020;16(10):1708-1717.
- Fung KP, Leung PC, Tsui KW, et al.Immunomodulatory activities of the herbal formula Kwan Du Bu Fei Dang in healthy subjects: a randomised, double-blind, placebo-controlled study. Hong Kong Med J. 2017;17(Suppl 2):41-43.
- Lau KM, Lee KM, Koon CM, et al.Immunomodulatory and anti-SARS activities of Houttuynia cordata. J Ethnopharmacol. 2008;118:79-85.
- Pyrc K, Berkhout B, Van der Hoek L. Antiviral Strategies Against Human Coronaviruses. Infectious Disorders – Drug Targets. 2007;7:59-66.
- Cinatl J, Morgenstern B, Bauer G, Chandra P, Rabenau H, Doerr HW. Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus. Lancet, 2003; 361(9374): 2045-2046.
- Chen F, Chan KH, Jiang Y, et al. In vitro susceptibility of 10 clinical isolates of SARS coronavirus to selected antiviral compounds. J.Clin. Virol. 2004;31:69-75.
- Balzarini J, Vijgen L, Keyaerts E, et al. Mannose specific plant lectins are potent inhibitors of coronavirus infection including the virus causing SARS. Abstracts of the 17th International Conference on Antiviral Research Tucson, USA. Antiviral Research. 2004;62(A76):no.122.
- Vijgen L, Keyaerts B, Damme EV, et al. Antiviral effect of plant compounds of the Alliaceae family against SARS coronavirus. Abstracts of the 17th International Conference on Antiviral Research Tucson, USA. Antiviral Res. 2004;62(A76): no 123.
- Wu CY, Jan JT, Ma SH, Ket al. Small molecules targeting severe acute respiratory syndrome human coronavirus. Proc. Natl. Acad. Sci. USA. 2004;101(27):10012-10017.
- Yu MS, Lee J, Lee JM, et al. Identification of myricetin and scutellarein as novel chemical inhibitors of the SARS coronavirus helicase, nsP13. Bioorg Med Chem Lett. 2012;22:4049-4054.
- Pyrc K, Bosch BJ, Berkhout B, et al. Inhibition of human coronavirus NL63 infection at early stages of the replication cycle. Antimicrob. Agents Chemother. 2006;50(6):2000-2008.
- Luo W, Su X, Gong S, et al. Anti-SARS coronavirus 3C-like protease effects of Rheum palmatum L. extracts. BioScience Trends. 2009;3(4):124-126.
- Gong SJ, Su XJ, Yu HP, et al.A study on anti-SARS-CoV 3CL protein of flavonoids from litchi chinensis sonn core. Chinese Pharmacological Bulletin. 2008;24:699-700.
- Nguyen TTH, Woo HJ, Kang HK, et al. Flavonoid-mediated inhibition of SARS coronavirus 3C-like protease expressed in Pichia pastoris. Biotechnol Lett. 2012;34:831-838.
- Jo S, Kim S, Shin DH, Kim MS.Inhibition of SARS-CoV 3CL protease by flavonoids. J Enzyme Inhib Med Chem. 2020;35:145-151.
- Chen CJ, Michaelis M, Hsu HK, et al. Toona sinensis Roem tender leaf extract inhibits SARS coronavirus replication. J Ethnopharmacol. 2008;120:108-111.
- Schwarz S, Wang K, Yu WJ, Sun B, Schwarz W. Emodin inhibits current through SARS-associated coronavirus 3a protein. Antiviral Res. 2011;90:64-69.
- Ho T, Wu S, Chen J, Li C, Hsiang C.Emodin blocks the SARS coronavirus spike protein and angiotensin-converting enzyme 2 interaction. Antiviral Res. 2007;74:92-101.
- Yi L, Li Z, Yuan K, Qu X, et al.Small molecules blocking the entry of severe acute respiratory syndrome coronavirus into host cells. J Virol. 2004;78:11334-11339.
- Li SY, Chen C, Zhang HQ, et al. Identification of natural compounds with antiviral activities against SARS-associated coronavirus. Antiviral Research. 2005;67:18–23.
- Ryu YB, Jeong HJ, Kim JH, Ket al. Biflavonoids from Torreya nucifera displaying SARS-CoV 3CL(pro) inhibition. Bioorg Med Chem. 2010;18(22):7940-7947.
- Schwarz S, Sauter D, Wang K, et al. Kaempferol Derivatives as Antiviral Drugs against the 3a Channel Protein of Coronavirus. Planta Medica. 2014;80:177-182.
- Park JY, Kim JH, Kwon JM, et al. Dieckol, a SARS-CoV 3CLproinhibitor, isolated from the edible brownalgae Ecklonia cava. Bioorganic and Medicinal Chemistry. 2013;21:3730-3737.
- Jo S, Kim H, Kim S, Shin DH, Kim MS.Characteristics of flavonoids as potent MERS-CoV 3C-like protease inhibitors. Chem Biol Drug Des. 2019;94(6):2023-2030.
- Cheng PW, Ng LT, Chiang LC, Lin CC. Antiviral effects of saikosaponins on human coronavirus 229E in vitro. Clin Exp Pharmacol Physiol. 2006;33:612‑616.
- Kim DE, Min JS, Jang MS, et al.Natural Bis-Benzylisoquinoline Alkaloids-Tetrandrine, Fangchinoline, and Cepharanthine, Inhibit Human Coronavirus OC43 Infection of MRC-5 Human Lung Cells. Biomolecules. 2019;9(11):pii: E696. doi: 10.3390/biom9110696.
- Zou HM, He TZ, Chen X.Tetrandrine inhibits differentiation of proinflammatory subsets of T helper cells but spares de novo differentiation of iTreg cells. Int Immunopharmacol. 2019;69:307-12.
- Grein J, Ohmagari N, Shin D, et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. The New England Journal of Medicine. 2020. DOI: 10.1056/NEJMoa2007016
- Baden LR, Rubin EJ. Covid-19 — The Search for Effective Therapy. N Engl J Med. 2020;382:1851-1852.
- Yang N, Shen H-M. Targeting the Endocytic Pathway and Autophagy Process as a Novel Therapeutic Strategy in COVID-19. International Journal of Biological Sciences. 2020;16(10):1724-1731. doi:10.7150/ijbs.45498.
- Sallard E, Lescure FX, Yazdanpanah Y, Mentre F, Smadja NP. Type 1 interferons as a potential treatment against COVID-19. Antiviral Res. 2020;178:104791. doi: 10.1016/j.antiviral.2020.104791.
© The Author(s) 2020. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.