


ISSN: 0973-7510
E-ISSN: 2581-690X
Dermatophytosis is a superficial fungal infection involving the keratinized tissues. Limited dermatophytosis is usually treated with topical antifungals. Amorolfine and luliconazole are relatively newer and superior topical antifungals much in use in recent times. To study the therapeutic efficacy and safety of luliconazole 1% and amorolfine 0.25% cream in patients with tinea cruris. A single-center, randomized, double-blind, non-inferiority study comparing luliconazole and amorolfine was conducted on patients with localized tinea cruris. 81 patients completed the study, with 40 patients treated with luliconazole and 41 patients treated with amorolfine. Both groups of patients were followed up at the end of 2 weeks. No statistically significant difference was found between luliconazole and amorolfine regarding improvement in erythema, scaling, pruritus, and mycological cure. Both the medications were safe and well tolerated by the patients. The duration of the study was short, and there was no long-term follow-up. Amorolfine is not inferior to luliconazole in treating limited tinea cruris.
Tinea cruris, Topical Antifungal, Luliconazole, Amorolfine
Dermatophytosis (tinea) is an infection caused by dermatophytes which is a keratinophilic fungi. Infection involves the epidermis, particularly the stratum corneum and appendageal structures rich in keratin (hair and nail).1 Infection is seen mainly in tropical countries due to the warm and humid climate, overcrowded areas, and people with low socioeconomic status. Tinea cruris is the dermatophytic infection of the groin. Topical antifungal monotherapy is mainly indicated for limited dermatophytosis.2 Because of their great efficacy and minimal risk of adverse effects, topical antifungal medication is typically regarded as the first-line therapy for dermatophytosis. Luliconazole is an azole that inhibits the enzyme lanosterol 14-demethylase, preventing ergosterol synthesis.3 Amorolfine, a morpholine derivative, blocks delta 14 reductase and delta 7-8 isomerase, impeding ergosterol production in the fungal cell membrane.4 Luliconazole is in vogue for treating dermatophytosis, but use of amorolfine is relatively less. Though amorolfine has been used as a nail lacquer for onychomycosis since long, its cream form has come up recently, and there are limited studies proving its efficacy. We have undertaken this study to demonstrate that amorolfine is as efficacious as luliconazole in treating tinea cruris.
This study was a double-blinded, randomized, non-inferiority study to evaluate the efficacy and safety of luliconazole and amorolfine cream in treating tinea cruris. This study was conducted over 2 years.
All the patients above 18 years of age with tinea cruris affecting ≤3% of their body surface area (BSA) with positive potassium hydroxide (KOH) mount were included. Patients treated with topical or systemic antifungal or formulations containing topical steroids within the last 4 weeks, pregnant or lactating females, patients on any immunosuppressive drugs, coexisting onychomycosis, and patients with known chronic diseases (hypertension/Diabetes mellitus/Tuberculosis/Asthma) were excluded from the study.
With reference to the article by Khanna et al., the cure rate of luliconazole was 95%, and with reference to the study done by Zaug et al., the cure rate of amorolfine was 81.1%.5,6 Considering the effect size of 0.139 (difference of the response rate), alpha value of 0.05, power of 80%, and a clinically acceptable limit of 20%, the sample size was calculated to be 37 in each arm. Presuming a dropout rate or loss to follow-up of 10%, the sample size was inflated to be 41 in each arm (82 in both arms). The sample size was calculated by using the formula “N=2 × [{(Z1-α +Z1-β)/δ0]2 × p×(1-p)” for the noninferiority study, referring to the article by Zhong Baoliang.7
The patients who met all the inclusion criteria and did not meet any of the exclusion criteria were considered for participation in this study. Informed consent was signed by the subjects, stating that he/she understands the possible outcome of therapy and agrees to undergo it. The patients were randomised according to a random number generator and allocated to two interventional groups (Figure 1). The two medications were available in identical-sized and coloured unlabeled tubes and were dispensed by the co-investigator. Both the patient and the primary investigator were blinded. The medicines were supplied by INTAS® Pharmaceuticals bearing batch no. HP20050-Amorolfine and OA0065-Luliconazole (Figure 2).
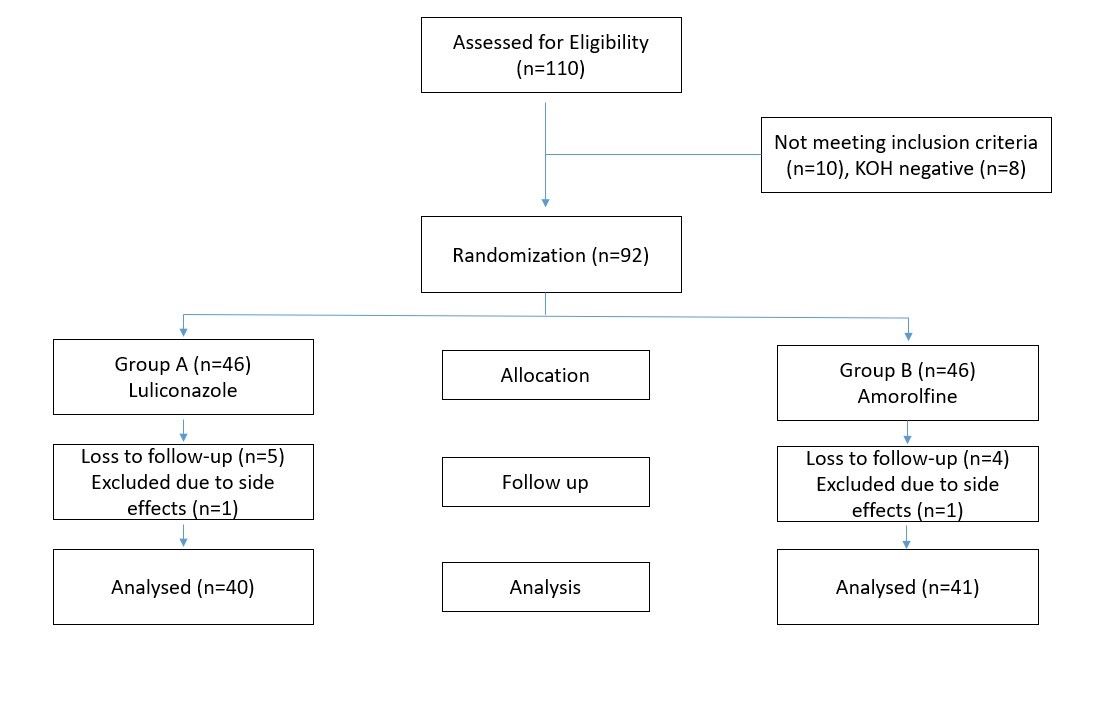
Figure 1. Participants flow diagram for analysis of the study

Figure 2. Same coloured and sized lamitubes containing two different molecules i.e luliconazole and amorolfine
One group was prescribed luliconazole 1% cream to apply once daily. The other group was given amorolfine 0.25% cream to apply once daily. The medications were applied as a thin layer of at least 2 FTU directly to the lesions and two centimetres beyond the lesions. All cases were given an antihistamine (levocetirizine 5 mg) once daily at bedtime as an anti-pruritic medication. Follow-up was done at the end of two weeks. Clinical parameters like BSA involvement, erythema, scaling, and pruritus were recorded at the baseline and follow-up using a grading system. The BSA was calculated using the number of palms involved (1 palm is equivalent to 1% BSA). The outcome was evaluated by comparing the improvement in the clinical parameters along with the mycological cure.
Erythema, scaling, and pruritus were graded as 0 – absent, 1 – mild, 2 – moderate, and 3 – severe. Scales covering less than one-third of the lesion were considered as mild scaling, up to two-thirds as moderate scaling, and more than two-thirds as severe grades. A total composite score was calculated at both visits by adding up the grades of erythema, scaling, and pruritus. KOH mount with microscopy was done at the beginning to confirm the diagnosis and after two weeks to look for a mycological cure. Fungal culture was done once during the first visit to confirm the diagnosis and identify the species. Antifungal drug sensitivity test could not be done because of lack of facility at the study site. Clinical photographs were obtained at baseline and at two weeks to look for improvement without revealing the patient’s identity. The patients were asked to report immediately if they developed any side effects like redness or burning sensation and were physically examined at the end of two weeks. To ensure compliance, the patients were asked to return the empty tubes at the end of treatment.
Ethical approval to conduct this study was taken from the institutional ethics committee. Trial registration was done under the Clinical Trials Registry India (CTRI).
Statistical analysis was performed using the software IBM SPSS version 25.0. All continuous or quantitative variables were assessed in mean ± SD. Categorical variables were expressed as frequency percentages. An independent sample t-test was used to find out the association of all quantitative variables between the two groups. Likewise, a chi-square test was used to find out the association of categorical variables with all groups of patients. A paired t-test was used to compare the effect of treatment at pre-and post-intervention. The p-value <0.05 was set for the statistical significance.
81 patients were analyzed in this study. The mean age was 38.50 ± 12.38 years in the luliconazole group and 40.93 ± 10.15 years in the amorolfine group. The demographic data of patients in both the luliconazole and amorolfine groups were comparable with each other. No statistically significant difference was found in the site involved or the duration of disease among the two groups at baseline (Table 1).
Table (1):
Comparison of Clinicodemographic profile of patients
| Luliconazole | Amorolfine | p-value | ||
|---|---|---|---|---|
| Age | 38.53 ± 12.37 | 40.93 ± 10.15 | 0.342 | |
| Gender | Male | 25 (62.5%) | 20 (48.8%) | 0.214 |
| Female | 15 (37.5%) | 21 (51.2%) | ||
| Education | Illiterate | 2 (5.0%) | 1 (2.4%) | 0.084 |
| 10th pass | 4 (10.0%) | 11 (26.8%) | ||
| 12th pass | 10 (25.0%) | 9 (22.0%) | ||
| Graduate | 12 (30.0%) | 16 (39.0%) | ||
| Postgraduate | 12 (30.0%) | 4 (9.8%) | ||
| Occupation | Employed | 20 (50.0%) | 14 (34.1%) | 0.478 |
| Self employed | 11 (27.5%) | 15 (36.6%) | ||
| Retired employees | 0 (0.0%) | 1 (2.4%) | ||
| Student | 4 (10.0%) | 3 (7.3%) | ||
| Housewife | 5 (12.5%) | 8 (19.5%) | ||
| Family members affected. | Yes | 23 (57.5%) | 18 (43.9%) | 0.221 |
| No | 17 (42.5%) | 23 (56.1%) | ||
| Urban/Rural | Rural | 13 (32.5%) | 12 (29.3%) | 0.753 |
| Urban | 27 (67.5%) | 29 (70.7%) | ||
| Sites affected.
|
Groin | 23 (57.5%) | 25 (61.0%) | 0.467 |
| Inner thigh | 10 (25.0%) | 6 (14.6%) | ||
| Perianal | 5 (12.5%) | 9 (22.0%) | ||
| Pubic | 2 (5.0%) | 1 (2.4%) | ||
| Duration (days) | 59.75 ± 44.06 | 45.61 ± 46.18 | 0.163 | |
The reduction in BSA involved and improvement of the clinical parameters (erythema, scaling, pruritus) was statistically highly significant post-treatment in both groups (p value <0.001) (Figures 3, 4, 5). On intergroup comparison, there was no significant statistical difference between the groups at baseline and follow-up. (Table 2). Though the reduction of pruritus was greater in the luliconazole group, the difference was statistically not significant.
Table (2):
Intergroup comparison of the body surface area (palm area) involved and the clinical parameters
Luliconazole |
Amorolfine |
p-value |
|
|---|---|---|---|
BSA (Baseline) |
2.04 ± 0.85 |
2.04 ± 0.69 |
0.996 |
BSA (Follow up) |
0.09 ± 0.24 |
0.19 ± 0.32 |
0.113 |
Erythema (Baseline) |
2.00 ± 0.68 |
2.20 ± 0.71 |
0.212 |
Erythema (Follow up) |
0.13 ± 0.33 |
0.27 ± 0.45 |
0.108 |
Scaling (Baseline) |
2.28 ± 0.45 |
2.39 ± 0.59 |
0.115 |
Scaling (Follow up) |
0.25 ± 0.44 |
0.37 ± 0.49 |
0.116 |
Pruritus (Baseline) |
2.10 ± 0.71 |
2.15 ± 0.69 |
0.767 |
Pruritus (Follow up) |
0.18 ± 0.38 |
0.37 ± 0.49 |
0.054 |
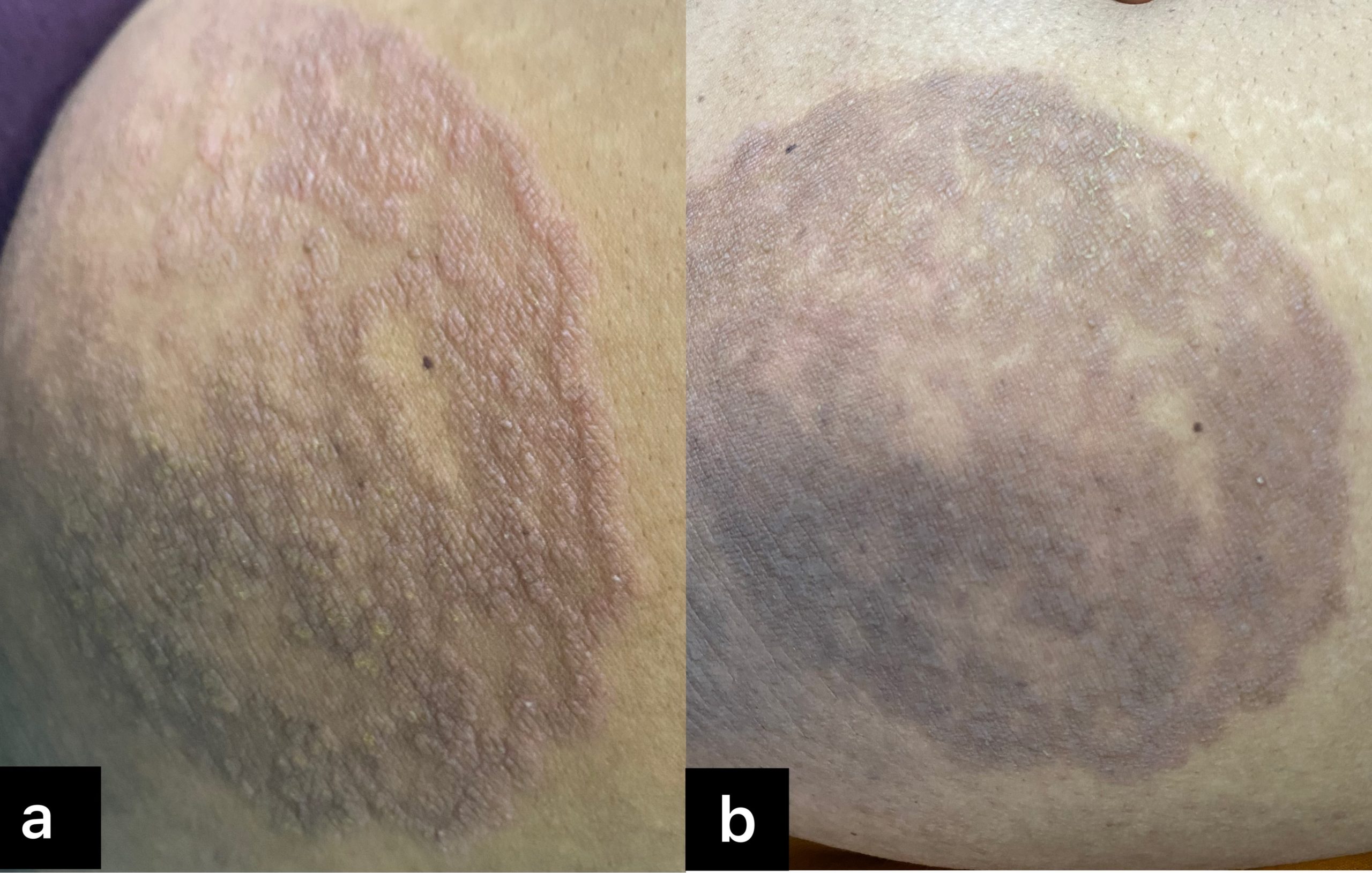
Figure 3. Improvement of the lesions with luliconazole cream
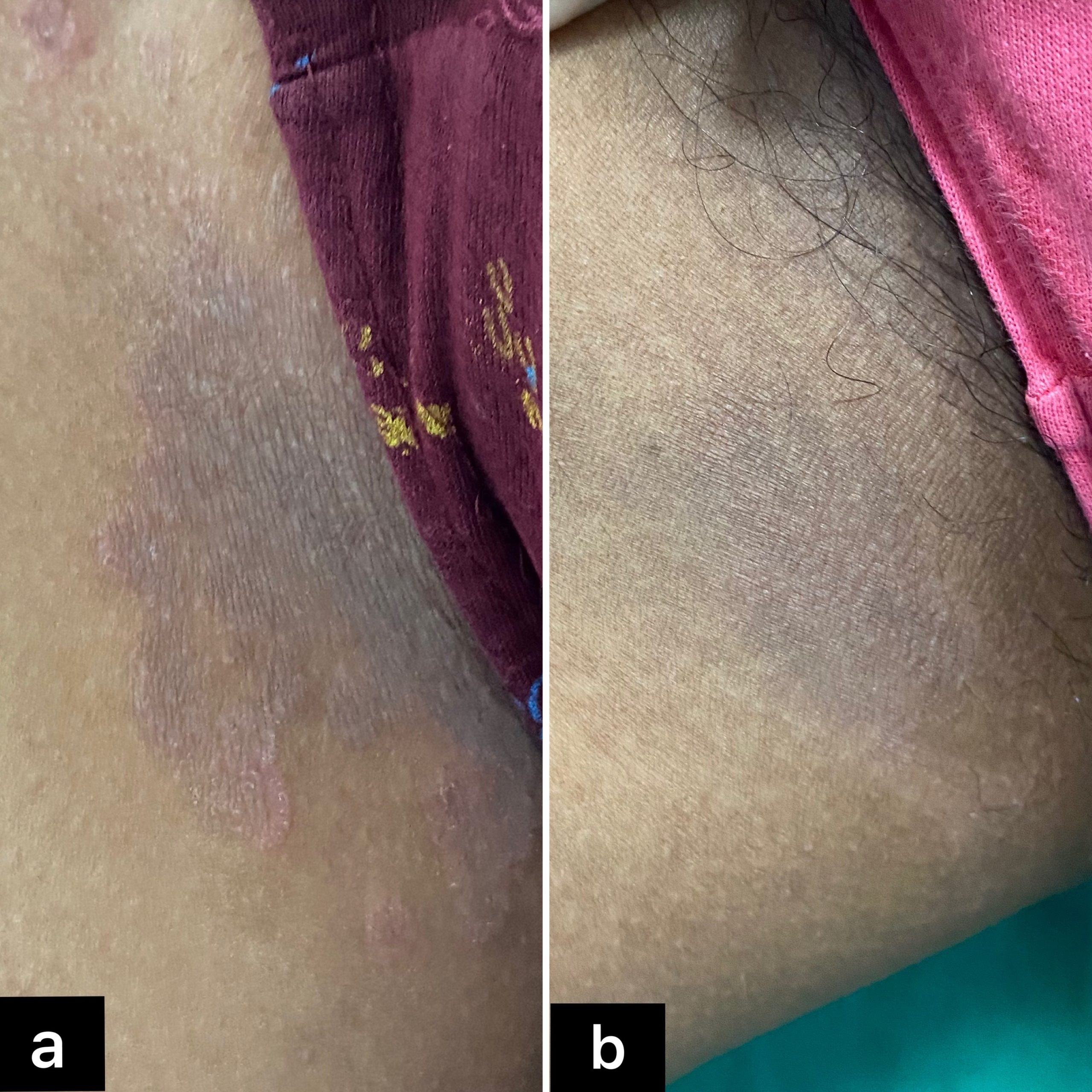
Figure 4. Improvement of the lesions with amorolfine cream
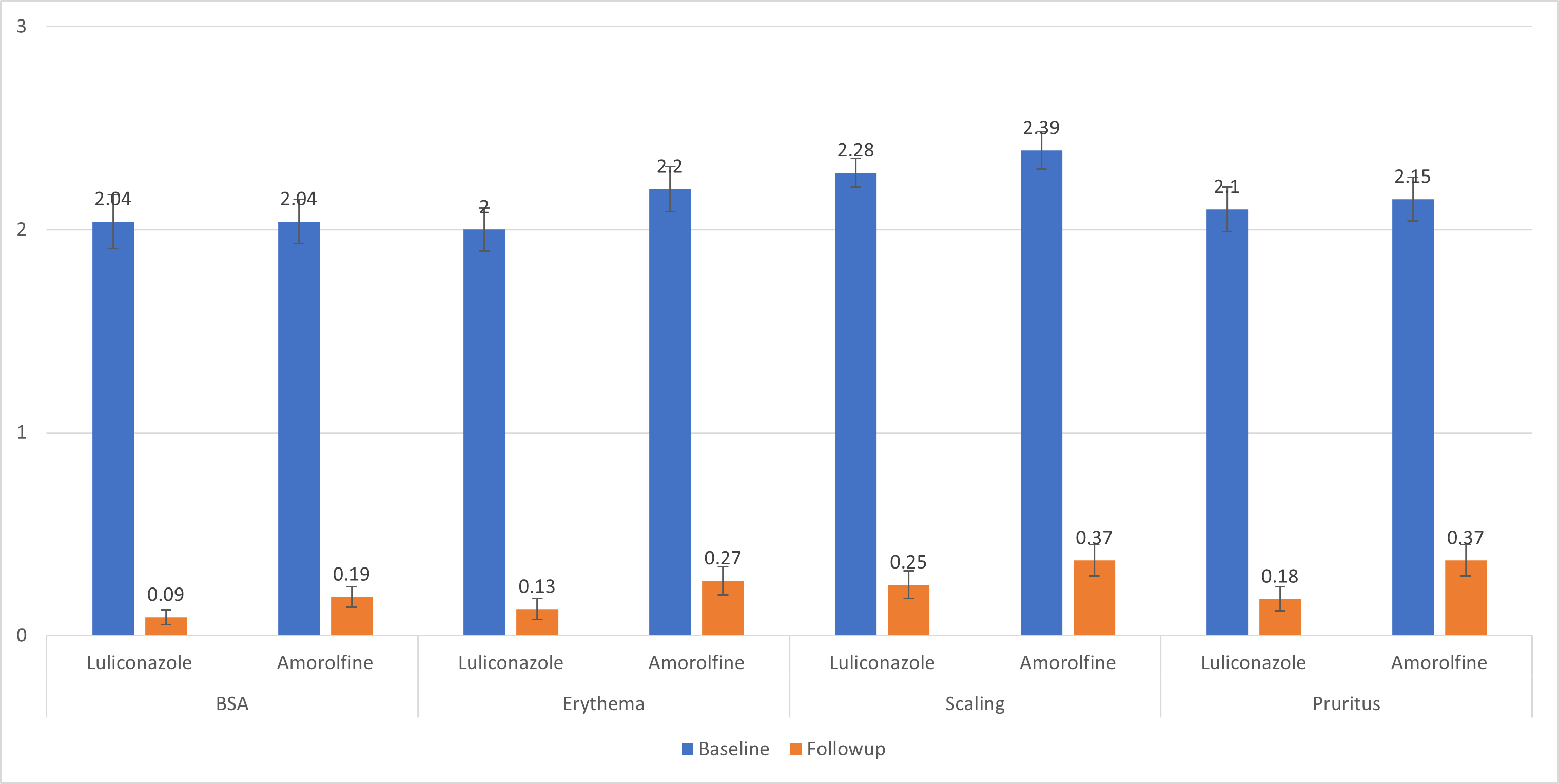
Figure 5. Intragroup comparison of various clinical parameters at baseline and follow up for both the groups
The total composite score was calculated at both visits by adding up the scores for erythema, scaling, and pruritus. We found a highly significant statistical difference (p value <0.001) in both groups after intervention. On intergroup comparison, there was no significant difference statistically between these two groups at baseline (p value 0.137). However, in follow-up, there was a significant difference between the two groups (p value 0.015), with luliconazole showing a better reduction of the score (Figure 6). The improvement in total composite score was 85.1% in the amorolfine group and 91.6% in the luliconazole group.
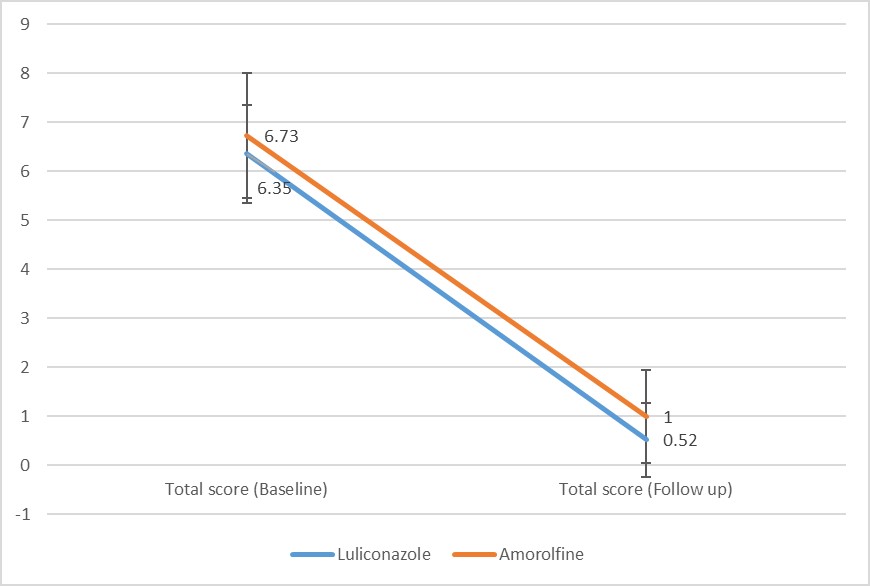
Figure 6. Inter group comparison of composite score at baseline and follow up
The change in KOH status was highly significant (p-value <0.001) in both groups after intervention. At follow-up, there was no significant difference between the two groups (p-value 0.615) (Table 3). 78% of the patients in the amorolfine group and 82.5% of the patients in the luliconazole group had a negative KOH at the end of two weeks.
Table (3):
Comparison of KOH status between the two groups
| KOH(Baseline) | KOH (Follow up) | p-value (intragroup) | ||
|---|---|---|---|---|
| Luliconazole | Positive | 40 (100.0%) | 7 (17.5%) | <0.001 |
| Negative | 0 (0.0%) | 33 (82.5%) | ||
| Amorolfine | Positive | 41 (100.0%) | 9 (22.0%) | <0.001 |
| Negative | 0 (0.0%) | 32 (78.0%) | ||
| p-value (intergroup) | *** | 0.615 | ||
In our study, we found 43.2% of patients showing culture positivity for Trichophyton mentagrophytes, 33.3% for Trichophyton rubrum, 9.8% for Microsporum canis, 4.9% of patients for Epidermophyton floccosum, 2.5% for Trichophyton tonsurans, and 7.4% of patients had no fungal growth (Figure 7).
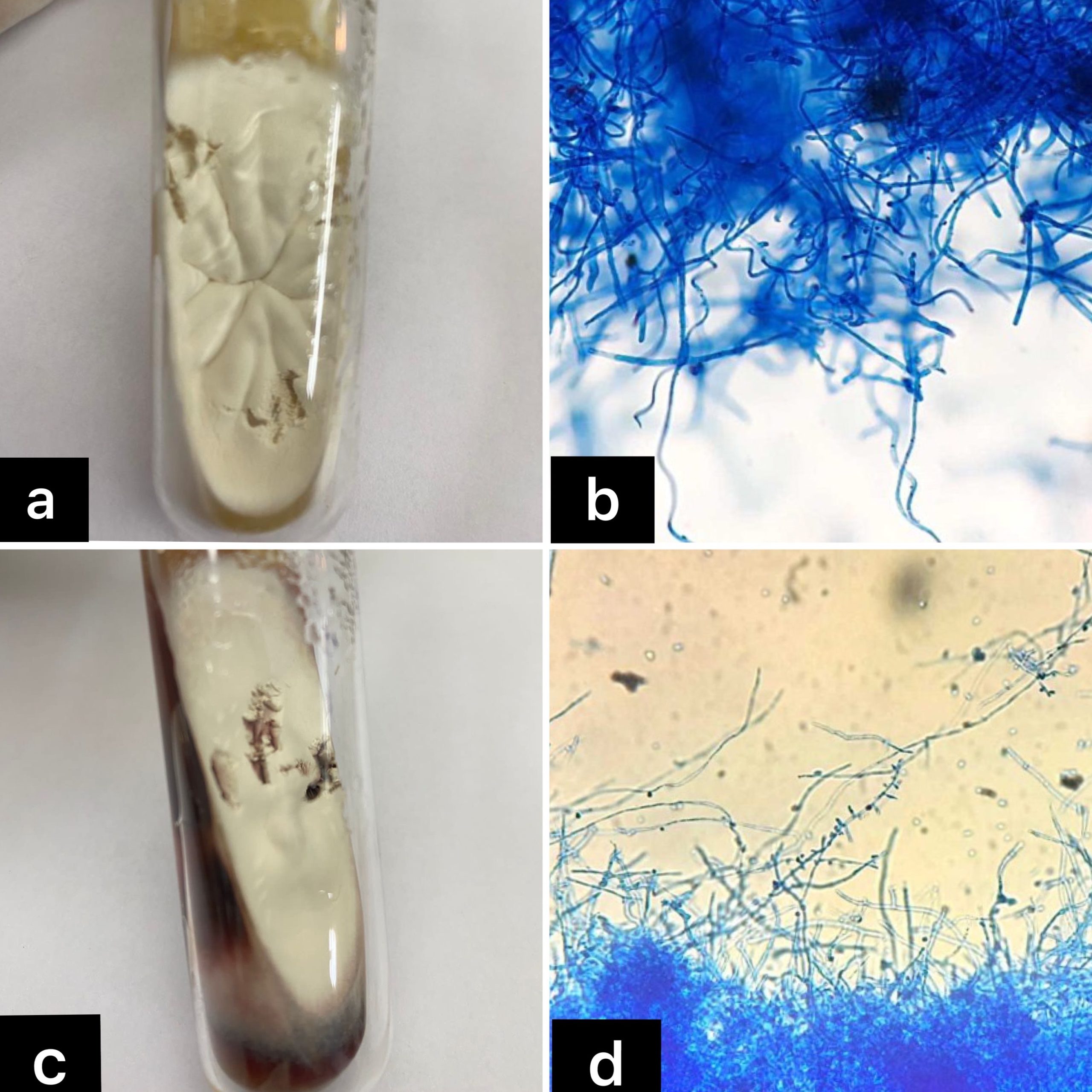
Figure 7. (a) Trichophyton mentagrophytes on Sabouraud’s Dextrose Agar (Obverse view). (b) Clustured spiral hyphae and microconidia of Trichophyton mentagrophytes (LPCB, 40x). (c) Trichophyton rubrum on Sabouraud’s Dextrose Agar (Obverse view). (d) Tear drop shaped microconidia attached to the hyphae of Trichophyton rubrum (LPCB, 40x)
The adverse effects were analysed. In both amorolfine and luliconazole group, one patient each dropped out of the study due to redness and burning sensation after two days of application and the development of erythematous scaly lesions on the site of application after seven days, respectively.
Superficial fungal infection is the commonest cause of infective dermatoses worldwide, affecting nearly 1/4th of the total world population during lifetime.8 Limited dermatophytosis is best treated by topical antifungals. It targets the site of infection and reduces the chances of systemic side effects.
81 participants were included in our study. Amongst them, 41 (50.60%) patients were allocated topical amorolfine and 40 (49.40%) patients were allocated topical luliconazole. The most common age group was 36-45 years (35.8%) and 26-35 years (25.9%), followed by patients in the age group 46-55 years (19.8%). The prevalence was lower among the age group of <25 years (8.6%), followed by >55 years (9.9%). In a study conducted by Balamuruganvelu et al., the maximum number of dermatophytic cases were in the age group of 21-40 years.9 It was less prevalent in the extremes of age, that is, below 10 and above 50 years. According to several authors, the increased prevalence could be in connection with outdoor manual work associated with excessive perspiration.
55.6% were males and 44.4% were females amongst our study participants, with the male-to-female ratio being 1.2:1. This was similar to results in some previous studies with a male to female ratio of less than 2.10 This might be due to more physical outdoor labour and increased exposure of males to the environmental conditions favourable for the growth of fungus.
45.6% of patients were found to be undergraduates, and 54.3% of patients were graduates and postgraduates. Kaur et al. stated that the frequency of infection was higher in the literate patients (64.6%) than the illiterate (35.3%).11 Literate people being more aware and desiring to seek medical care could be a possible explanation for the above finding.
Family history of the infection was found in 41 patients (50.6%), similar to a study conducted by Singh et al.10 Overcrowded homes, sharing of clothes among family members, and fomite transmission account for the higher frequency of infection in the family.
In our study, 69.1% were from an urban background, possibly because the study was conducted in an urban setting. Previous studies showed high prevalence in rural areas. In a study conducted by Edukondala et al., a greater number of patients with dermatophytosis hailed from rural backgrounds (59.7%).12 Recently, studies are showing an urban predominance, which may be due to increased awareness, literacy, and easy availability of mixed creams.
The majority of patients (55%) presented with <1 month duration in contrast to the study by Agarwal et al. and Kumar et al., in which the maximum number of patients presented after 3 months of disease.13,14 An increased awareness about the disease in the recent scenario might result in patients presenting early. The most common fungal species found in our study was Trichophyton mentagrophytes, known to cause more inflammatory reactions.
The change in BSA involvement, improvement in erythema, scaling, and pruritus was statistically significant in each group after intervention. But the same was not statistically significant when compared among the two groups. This result is similar to a study by Banerjee et al. in which the cure rate showed no significant difference among patients in the clotrimazole and amorolfine groups.15 However, the findings are in contrast to a study conducted by Agrawal et al., in which the patients treated with luliconazole showed a greater improvement in clinical parameters as compared to amorolfine, terbinafine, and sertaconazole, and the difference was statistically significant (p value <0.05).16
On comparing the total composite score between the two groups at follow-up, we found a significant difference, with luliconazole showing a better improvement. However, the total composite score used in the study is not a validated score. The change in the total composite score was 85.1% and 91.6% in the amorolfine and luliconazole groups, respectively. This is similar to the finding of the study conducted by Jerajani et al., in which the reduction in total composite score in the luliconazole group was 92.9%.3 In a study conducted by Watanabe et al., the improvement in skin lesions was 91.5% and 91.7% in luliconazole and bifonazole, respectively.17 According to a study conducted by Chandana et al., sertaconazole showed higher clinical efficacy with 93.3% cure rates, and the cure rates by luliconazole, amorolfine, terbinafine, and eberconazole were 86.6%, 83.3%, 80.0%, and 73.3%, respectively.18 Das et al. have reported sertaconazole cream to be more efficacious as compared to amorolfine cream in reducing the number of lesions at the end of 12 weeks.19
In our study, there was a high statistical significance with a p value <0.001 seen in the KOH evaluation when compared between the baseline and follow-up in each group. There was no significant difference in intergroup comparison at follow-up. 78% of the patients achieved mycological cure in the amorolfine group, and 82.5% achieved mycological cure in the luliconazole group. In a study conducted by Banerjee et al., the mycological cure obtained was 70.5% on the 14th day and 78.9% on the 28th day in the amorolfine group, and the cure rate obtained in the clotrimazole group was 68.9% on day 14, and it reached 76.2% on the 28th day.15 The difference was not statistically significant. In a study conducted by Watanabe et al., the cure had high negative rates of 76.1% in the luliconazole group at the end of two weeks and 75.9% in the bifonazole group at the end of four weeks in patients with tinea pedis.17
The most common fungal species detected in our study was Trichophyton mentagrophytes (44.4%). Trichophyton rubrum, Microsporum canis, Epidermophyton, and Trichophyton tonsurans were detected in 33.3%, 8.6%, 4.9%, and 2.4% of the patients, respectively. This is similar to the findings of a study conducted in Eastern India by Singh et al., in which he found Trichophyton mentagrophytes as the most common species causing dermatophytes. The species causing dermatophytosis vary from place to place.10 Janardhan et al. found Trichophyton rubrum as the predominant organism causing dermatophytosis in the southern part of India.20
In the amorolfine group, one patient developed burning and redness, and in the luliconazole group, one patient developed erythematous scaly lesions. The rest of the patients tolerated the medications well. According to Dakhale et al., none of the patients in the luliconazole group developed any side effects.21 In the study by Banerjee et al., all the patients in the amorolfine group tolerated the medication well.15 According to Nolting et al., the most common local adverse event with amorolfine was burning and increased erythema.22 Lakshmi et al. reported a mild application site reaction with luliconazole in their study.23 Hassanandani et al. and Tanaka et al. reported allergic contact dermatitis to luliconazole.24,25
Antifungal resistance in dermatophytes is a major concern nowadays. It may result due to modification in the target site, activation of signaling pathways to antifungal stress response, decreased drug uptake, and increased drug efflux.26 In a recently published multicentric study from India, Trichophyton mentagrophytes complexes were collected for a period of five years (2014-2018) and antifungal susceptibility testing of the isolates was done. Amorolfine, luliconazole, miconazole, itraconazole, and voriconazole had low MIC90 values of 0.06, 0.125, 0.25, 0.25, and 0.25 mg/L, respectively, amongst all the antifungals tested, thus focusing on the need to use these novel antifungals to combat the current scenario of rising dermatophytosis.27
Our study portrays that both luliconazole and amorolfine are equally efficacious in the treatment of tinea cruris. We hypothesize that the combination of topical amorolfine with systemic azoles will yield a better outcome and help overcome resistance among dermatophytes as it belongs to a different class of drug, though further trials are required to confirm it. There is certainly an urgent need for longer-term studies to assess relapse and studies focusing on antifungal drug sensitivity testing to determine more effective regimens.
Limitation
The duration of the study was short, and there was no long-term follow-up to assess relapse. Classically the treatment duration is two weeks. But according to the present scenario, treatment should be continued for a longer duration after clinical cure.
We conclude that both amorolfine and luliconazole provide relief in limited tinea cruris. Amorolfine is not inferior to luliconazole in terms of efficacy. Both the molecules are equally safe and are tolerated well by the patients. Clinical trials with longer follow-up are the need of the hour to consolidate the findings of our study.
ACKNOWLEDGMENTS
The authors are thankful to INTAS Pharmaceuticals for providing topical medications.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Institute of Medical Sciences and Sum Hospital with reference number DRI/IMS.SH/SOA/2021/107.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Begum J, Mir NA, Lingaraju MC, Buyamayum B, Dev K. Recent advances in the diagnosis of dermatophytosis. J Basic Microbiol. 2020;60(4):293-303.
Crossref - Sahoo AK, Mahajan R. Management of tinea corporis, tinea cruris, and tinea pedis: A comprehensive review. Indian Dermatol Online J. 2016;7(2):77-86.
Crossref - Jerajani HR, Janaki C, Kumar S, Phiske M. Comparative assessment of the efficacy and safety of sertaconazole (2%) cream versus terbinafine cream (1%) versus luliconazole (1%) cream in patients with dermatophytoses: a pilot study. Indian J Dermatol. 2013;58(1):34-38.
Crossref - Polak A. Preclinical data and mode of action of amorolfine. Dermatology. 1992;184(Suppl 1):3-7.
Crossref - Khanna D, Bharti S. Luliconazole for the treatment of fungal infections: an evidence-based review. Core Evid. 2014;9:113-124.
Crossref - Zaug M, Bergstraesser M. Amorolfine in the treatment of onychomycoses and dermatomycoses (an overview). Clin Exp Dermatol. 1992;17(Suppl 1):61-70.
Crossref - Zhong B. How to calculate sample size in randomized controlled trial?. J Thorac Dis. 2009;1(1):51-54.
- Havlickova B, Czaika VA, Friedrich M. Epidemiological trends in skin mycoses worldwide. Mycoses. 2008;51(Suppl 4):2-15.
Crossref - Balamuruganvelu S, Reddy SV, Babu G. Age and Genderwise Seasonal Distribution of Dermatophytosis in a Tertiary Care Hospital, Puducherry, India. J Clin Diagn Res. 2019;13(2):WC06-WC10.
Crossref - Singh BSTP, Tripathy T, Kar BR, Ray A. Clinicomycological Study of Dermatophytosis in a Tertiary Care Hospital in Eastern India: A Cross-sectional Study. Indian Dermatol Online J. 2019;11(1):46-50.
Crossref - Kaur M, Gupta A, Mahajan R, Gill M. Efficacy, Safety, and Cost Evaluation of the Topical Luliconazole Therapy versus Topical Clotrimazole Therapy in Patients with Localized Dermatophytosis in a Tertiary Care Hospital: An Observational Study. Int J Appl Basic Med Res. 2020;10(4):260-264.
Crossref - Rao DE, Reddy NS. Study of clinical profile and etiological fungal species in patients with dermatophytosis at a tertiary hospital. MedPulse International Journal of Medicine. 2021;18(3):72-75.
Crossref - Agarwal US, Saran J, Agarwal P. Clinico-mycological study of dermatophytes in a tertiary care center in Northwest India. Indian J Dermatol Venereol Leprol. 2014;80(2):194.
Crossref - Sumit Kumar, P Shrikara Mallya, Pallavi Kumari. Clinico-Mycological Study of Dermatophytosis in a Tertiary Care Hospital. International Journal of Scientifi c Study. 2014;1(6):27-32.
- Banerjee M, Ghosh AK, Basak S, Das KD, Gangopadhyay DN. Comparative evaluation of effectivity and safety of topical amorolfine and clotrimazole in the treatment of tinea corporis. Indian J Dermatol. 2011;56(6):657-662.
Crossref - Agrawal V, Shenoy MM, Pinto M, Asfiya MIA, Hegde S. Comparative study of efficacy of topical amorolfine, luliconazole, sertaconazole, and terbinafine in tinea corporis and tinea cruris. IP Indian Journal of Clinical and Experimental Dermatology. 2019;5(2):111-115.
Crossref - Watanabe S, Takahashi H, Nishikawa T, et al. A comparative clinical study between 2 weeks of luliconazole 1% cream treatment and 4 weeks of bifonazole 1% cream treatment for tinea pedis. Mycoses. 2006;49(3):236-241.
Crossref - Chandana T, Saritha Ch, Puligilla S. Comparison of safety and efficacy of laliconazole and other antifungal agents. International Journal of Pharma Sciences and Research. 2014;5:1-9.
- Das A, Sil A, Sarkar TK, et al. A randomized, double-blind trial of amorolfine 0.25% cream and sertaconazole 2% cream in limited dermatophytosis. Indian J Dermatol Venereol Leprol. 2019;85(3):276-281.
Crossref - Janardhan B, Vani G. Clinico mycological study of dermatophytosis. Int J Res Med Sci. 2017;5:31-9.
Crossref - Dakhale GN, Gupta AV, Mukhi JI, Kalikar MV. Comparison of efficacy, safety, and cost-effectiveness of sertaconazole and luliconazole cream in patients with dermatophytoses: A prospective, randomized, open-label study. Perspect Clin Res. 2021;12(4):223-228.
Crossref - Nolting S, Semig G, Friedrich HK, et al. Double-blind comparison of amorolfine and bifonazole in the treatment of dermatomycoses. Clin Exp Dermatol. 1992;17(Suppl 1):56-60.
Crossref - Prabha ML, Meenakshi B, Devi PN, Ramya JE, Balan CR. A randomized comparative study to assess the efficacy of topical luliconazole versus topical clotrimazole in tinea corporis and tinea cruris. Natl J Physiol, Pharm, Pharmacol. 2019;9:756-62.
Crossref - Hassanandani T, Panda A, Kar BR. Allergic contact dermatitis to luliconazole: An uncommon side effect of a commonly used drug. Indian J Drugs Dermatol. 2020;6:47-8
- Tanaka T, Satoh T, Yokozeki H. Allergic contact dermatitis from luliconazole: implication of the dithioacetal structure. Acta Derm Venereol. 2007;87(3):271-272.
Crossref - Martinez-Rossi NM, Bitencourt TA, Peres NTA, et al. Dermatophyte Resistance to Antifungal Drugs: Mechanisms and Prospectus. Front Microbiol. 2018;9:1108.
Crossref - Shaw D, Singh S, Dogra S, et al. MIC and upper limit of wild-type distribution for 13 antifungal agents against Trichophyton mentagrophytes-Trichophyton interdigitale complex of Indian origin. Antimicrob Agents Chemother. 2020;64(4):e01964-19.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.