


ISSN: 0973-7510
E-ISSN: 2581-690X
Stethoscopes are potential vector for health care associated infections worldwide. Ethyl alcohol (EA), isopropyl alcohol (IPA) and chlorhexidine (CH) are widely used for disinfecting stethoscope, however, comparative analysis of these disinfectants are scarce. Hence this paper aims to compare the reduction in bioburden with respect to stethoscope decontamination. A randomized, double-blind study was undertaken from various categories of health care workers (HCW) working in various departments. Each participant was asked to fill a questionnaire and diaphragms of their stethoscopes were imprinted on blood agar and sabourauds dextrose agar before and after disinfection with either 65%-EA, 70%-IPA or 1%-CH. The culture plates were incubated aerobically and the growth was further identified. 384 HCW participated in the study. 168 participants never cleaned their stethoscope, out of which 147 respondents (91.6%) comprised of students. EA (47%) and IPA (23%) were the two major types of alcohols used as disinfecting agents. 280 samples showed growth among which 51.8% were potent pathogens. Before disinfection, Staphylococcus aureus (27%) was the predominant pathogen, followed by Klebsiella (6.8%), Enterococcus and Candida respectively. Among the disinfectants used, maximum antimicrobial activity was exhibited by IPA (92.5%) compared to EA (82.5%) and CH (77.8%). Huge lacunae regarding knowledge, attitude and practice of stethoscope maintenance was found among student community. The microbial growth varies at various department. Disinfecting stethoscope with 70%-IPA for just 30 seconds is equally efficient compared to 1 minute and IPA was superior to EA and CH for decontaminating stethoscope. Stethoscopes are potential vector for health care associated infections worldwide. Ethyl alcohol (EA), isopropyl alcohol (IPA) and chlorhexidine (CH) are widely used for disinfecting stethoscope, however, comparative analysis of these disinfectants are scarce. Hence this paper aims to compare the reduction in bioburden with respect to stethoscope decontamination. A randomized, double-blind study was undertaken from various categories of health care workers (HCW) working in various departments. Each participant was asked to fill a questionnaire and diaphragms of their stethoscopes were imprinted on blood agar and sabourauds dextrose agar before and after disinfection with either 65%-EA, 70%-IPA or 1%-CH. The culture plates were incubated aerobically and the growth was further identified. 384 HCW participated in the study. 168 participants never cleaned their stethoscope, out of which 147 respondents (91.6%) comprised of students. EA (47%) and IPA (23%) were the two major types of alcohols used as disinfecting agents. 280 samples showed growth among which 51.8% were potent pathogens. Before disinfection, Staphylococcus aureus (27%) was the predominant pathogen, followed by Klebsiella (6.8%), Enterococcus and Candida respectively. Among the disinfectants used, maximum antimicrobial activity was exhibited by IPA (92.5%) compared to EA (82.5%) and CH (77.8%). Huge lacunae regarding knowledge, attitude and practice of stethoscope maintenance was found among student community. The microbial growth varies at various department. Disinfecting stethoscope with 70%-IPA for just 30 seconds is equally efficient compared to 1 minute and IPA was superior to EA and CH for decontaminating stethoscope.
Stethoscope, hospital acquired infection, disinfection, isopropyl alcohol, ethyl alcohol, chlorhexidine
Health care associated infections (HCAI) are frequent hindrance for the effective functioning of health care system globally. It is estimated that in developing countries, every 10 patients out of 100 will develop at least one HCAI and the number is reduced to 7 in developed countries1 thus demanding a need to address the increased burden of HCAI in developing countries. In India and other developing countries, 22.5 infections per 1000 Intensive Care Unit (ICU) days were noticed corresponding to prevalence rate of 14.7%2. HCAI contribute critically by increasing the resistance to antimicrobials and creating additional financial burden to the patients and the family3-5.
Hospital surfaces, contaminated hands of health care workers (HCW), contaminated instruments or medical devices like thermometers, stethoscopes, lab coats, tables and wristwatches are sources for transmitting nosocomial infections. Stethoscopes act as one of the prime contributors as it is most commonly used instruments in daily medical practices6-8. Stethoscopes harbour many pathogenic organisms like Methicillin Resistant Staphylococcus aureus (MRSA), Escherichia coli, Pseudomonas, Acinetobacter, Klebsiella, Proteus, Citrobacter and Candida along with commensals like Micrococcus, Gram positive bacilli and Coagulase negative Staphylococcus9-14. Despite of the known fact that stethoscopes are vectors in transmitting HCAI7,15-17, disinfection of the stethoscopes are seldom done15,18-21 enabling the spread of infections between patients and HCW. Nosocomial pathogens can survive on the contaminated instruments for months and can be reservoir for transmitting infections if disinfection is practised irregularly22.
Disinfection of stethoscopes can be carried out mainly using physical and chemical methods23. While the chemical methods use reagents like alcohols, chlorhexidine, gels and liquid formulations; physical method involves a novel process wherein ultraviolet C radiation from a light-emitting-diode is used 24. The physical method takes about five minutes for the disinfection process which is relatively longer as compared to chemical method25 and the development of this technique is in the pilot research stage. Among the chemical disinfectants, isopropyl alcohol (IPA) is the most commonly used reagent to disinfect stethoscope by health care professionals26,27. The optimum bactericidal concentration is 60 to 90% 28. However, at a concentration beyond 70%, the cell wall is sealed up preventing further entry of alcohol29. Hence 70% alcohol is recommended. When the stethoscopes were swabbed with 70% IPA for 1 minute and 30 seconds, the colony forming units (CFU) were reduced by 92-94%30-32 and 89-100%33-35 respectively. Ethyl alcohol (EA) was equally effective and cheap compared to 70% IPA for disinfecting stethoscopes30,36. 65% EA is as effective as 70% IPA for disinfecting when used for 1 minute29. Around 28% reduction in contamination rate and less than 10 CFU with 65% EA was noted for disinfection carried out once in a day and the rate was decreased by 3% when disinfected after every use 37. The microbial growth was inhibited by 85.2%33 to 92.8%30 with IPA compared to 92.5%30,33 with ethyl alcohol, however, statistically the efficacy of EA and IPA remained same. Further studies revealed that 1% chlorhexidine (CH) also significantly reduced the bioburden and was superior to 70% IPA in preventing recontamination of the stethoscopes, however, there was no significant difference in the efficacy of IPA and CH22,38. Though IPA is widely used, the duration recommended is still unclear and the studies comparing the antimicrobial activity of various disinfectants on decontamination of stethoscope are scanty.
Hence this paper aims to study the knowledge, attitude and practice of the HCW towards disinfecting stethoscopes and to estimate the bioburden on their stethoscopes. It aims to find effect of duration of application of 70% IPA on microbial growth. It also aims to compare the antimicrobial activity of 65% ethyl alcohol, 70% IPA and 1% CH in decontaminating the stethoscopes at hospital setting.
Study area and period
The study was conducted at the department of microbiology for a period of 4 months from May 2019 to August 2019 at tertiary care teaching hospital, Karwar after obtaining approval from institutional ethical committee. In this study, doctors, nurses and medical students were included and first year undergraduate medical students were excluded.
Sample size
The sample size (n) for the study is estimated using Cochran’s formula given by equation
n=(Z2 pq)/e2
Where,
Z = 1.96, assuming a normally distributed data at 5% level of significance.
p = 0.5, since the probability of efficacy of antimicrobial agents are unknown, it is safe to assume that there is a 50% chance to proceed with the study.
q = 1 – p = 0.5
e = 0.05, the margin of error desired for the study is 5%.
This results in a sample size of 384 which is used in the present study.
Sampling technique
A total of 384 samples were collected from HCW working at tertiary care teaching hospital, Karwar. A randomized, double-blind study was conducted on these participants after obtaining written informed consent. Randomization was done by picking up chits. Each participant had to pick up any one chit with a letter A, B1, B2 or C written on it. The colour, texture and size of all the chits were similar to maintain concealment of allocation of disinfectants. Among 128 samples to be treated with IPA, 64 samples were cleaned for 30 seconds30,32 and the other 64 samples were cleaned for 1 minute30,32 and Stethoscopes were subjected to disinfection28 as shown in Table 1. The participants and the surveyor were blind to the randomization.
Table (1):
Nomenclature of disinfectant used in the study and duration of application.
Sl. No. |
Nomenclature |
Disinfectant |
Duration of application |
Number of samples |
|---|---|---|---|---|
1 |
A |
65% Ethyl alcohol |
30 seconds 33,35 |
128 |
2 |
B1 |
70% Isopropyl alcohol |
30 seconds 30,32 |
64 |
3 |
B2 |
70% Isopropyl alcohol |
1 minute 39,40 |
64 |
4 |
C |
1% Chlorhexidine |
1 minute 22,35 |
128 |
Data collection
After obtaining informed consent, study questionnaire was administered to obtain information on stethoscope usage, handling, and maintenance. The questionnaire survey included questions regarding awareness of stethoscope disinfection, frequency of disinfection, type of disinfectant used and maintenance of stethoscope during and after duty hours. The samples were collected from all the participants by imprinting the diaphragms of their stethoscopes for 5 seconds with gentle pressure on blood agar and sabouraud dextrose agar (SDA) as this method is quick and most efficient30,33 . According to the chit picked, the stethoscopes were disinfected with their respective disinfectant and imprint from the diaphragm was again taken on blood agar and SDA. Blood agar were incubated aerobically at 37°C and the plates were examined for growth after 48 hours. The colony count was done before and after decontamination. SDA were incubated at room temperature for a week.
Identification of pathogens
The bacterial isolates were presumptively identified by noting their colony characteristics and Gram reaction. The confirmation of Gram negative bacteria were done by performing a series of biochemical tests like catalase, oxidase, indole production, citrate utilization, carbohydrate fermentation on triple sugar iron media and motility was checked by hanging drop preparation. Gram positive cocci were confirmed by catalase, modified oxidase and coagulase test results. As Gram positive rods are considered as skin contaminants with low pathogenic potential, no further tests were performed. Lawn culture of Staphylococcus aureus isolates were done on Mueller-Hinton agar and resistance to cefoxitin (30 μg) was used to detect MRSA by disk diffusion testing following CLSI guidelines 202041. The identification of fungus was done by noting colony morphology and Lactophenol Cotton Blue (LPCB) preparation.
Data analysis
Data were entered and analysed using Microsoft Excel spreadsheets. Since the data obtained was non-parametric, chi-squared (c2) distribution is applied and the appropriate tests are carried out to ascertain the existence of significant relationship among different factors42. A confidence level of 95% is selected and the hypothesis test results are declared significant if the probability (p-value) falls below 0.05. The critical values and p-value for a given degree of freedom in the c2 test is calculated using Microsoft Excel software. The statements of the different alternate hypotheses tested in the current study are as follows:
H1: There is a significant association between category of HCW and awareness regarding stethoscope disinfection
H2: There is a significant association between category of HCW and the type of disinfectant used for cleaning stethoscope
H3: There is a significant association between the type of reagent and the growth after disinfecting a stethoscope
H4: There is a significant association between duration of application of IPA and the growth after disinfecting a stethoscope
H5: There is a significant association between the microbial growth after disinfection and the workplace (department)
Survey data
A total of 384 samples were taken for the study and were equally divided among the three disinfecting reagents. The samples were taken from HCW including doctors, nurses and undergraduate students working in various departments like Orthopaedics, Obstetrics & Gynaecology (OBG), Medicine, Operation Theatre (OT), Paediatrics, Surgery and other departments (Casualty, Dermatology and ENT). The distribution of samples obtained for doctors, nurses and students are 97, 74 and 213 respectively. Fig. 1 shows the distribution of samples across different departments and health care workers. 168 participants (43.8 %) were unaware about maintenance recommended for disinfecting stethoscope. 147 participants (91.6%) comprising of students never cleaned their stethoscopes. 145 participants (65.3%) used alcohol as disinfecting agent and the other disinfecting agents used by HCW were soap water (10.4%), hypochlorite (10.4%) and others (14%). EA (47%) and IPA (23%) were the two major types of alcohols used as disinfecting agents.
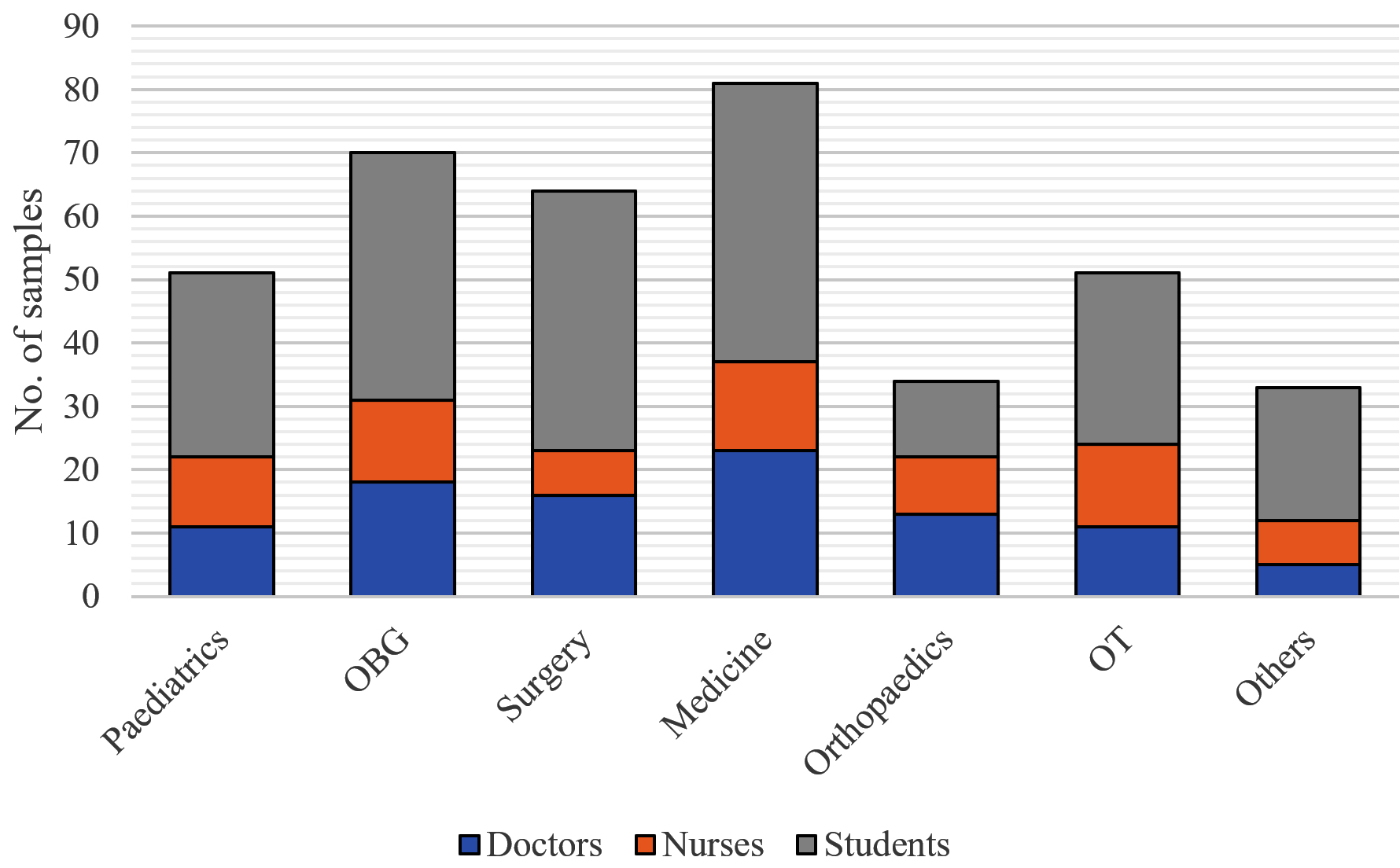
Fig. 1. Distribution of the samples among various departments and health care workers
Table (2):
Major data obtained from questionnaire survey.
| Particulars | Healthcare worker | |||||
|---|---|---|---|---|---|---|
| Doctors | Nurses | Students | Total | |||
| Awareness about stethoscope disinfection | Yes | 95 | 62 | 59 | 216 | |
| No | 2 | 12 | 154 | 168 | ||
| Total | 97 | 74 | 213 | 384 | ||
| Frequency of stethoscope cleaning | Every patient | 9 | 3 | 15 | 27 | |
| Few patients | 64 | 32 | 22 | 118 | ||
| End of duty | 15 | 24 | 16 | 55 | ||
| Never | 2 | 13 | 147 | 162 | ||
| Others | 7 | 2 | 13 | 22 | ||
| Total | 97 | 74 | 213 | 384 | ||
| Department | Paediatrics | 11 | 11 | 29 | 51 | |
| OBG | 18 | 13 | 39 | 70 | ||
| Surgery | 16 | 7 | 41 | 64 | ||
| Medicine | 23 | 14 | 44 | 81 | ||
| Orthopaedics | 13 | 9 | 12 | 34 | ||
| OT | 11 | 13 | 27 | 51 | ||
| Others | 5 | 7 | 21 | 33 | ||
| Total | 97 | 74 | 213 | 384 | ||
| Type of disinfectant used | Soap water | 0 | 14 | 9 | 23 | |
| Alcohol | Ethyl alcohol | 44 | 17 | 7 | 68 | |
| Isopropyl alcohol | 23 | 5 | 5 | 33 | ||
| Other alcohol | 8 | 15 | 21 | 44 | ||
| Total | 75 | 37 | 33 | 145 | ||
| chlorine | 16 | 5 | 2 | 23 | ||
| others | 5 | 9 | 17 | 31 | ||
| total | 96 | 65 | 61 | 222 | ||
Culture study
Out of 384 samples cultured, 280 samples (72.9%) showed growth before any reagent was applied. After disinfecting, 44 samples (11.4%) showed growth. The distribution of the organisms isolated from the samples before and after decontamination is shown in Fig. 2.
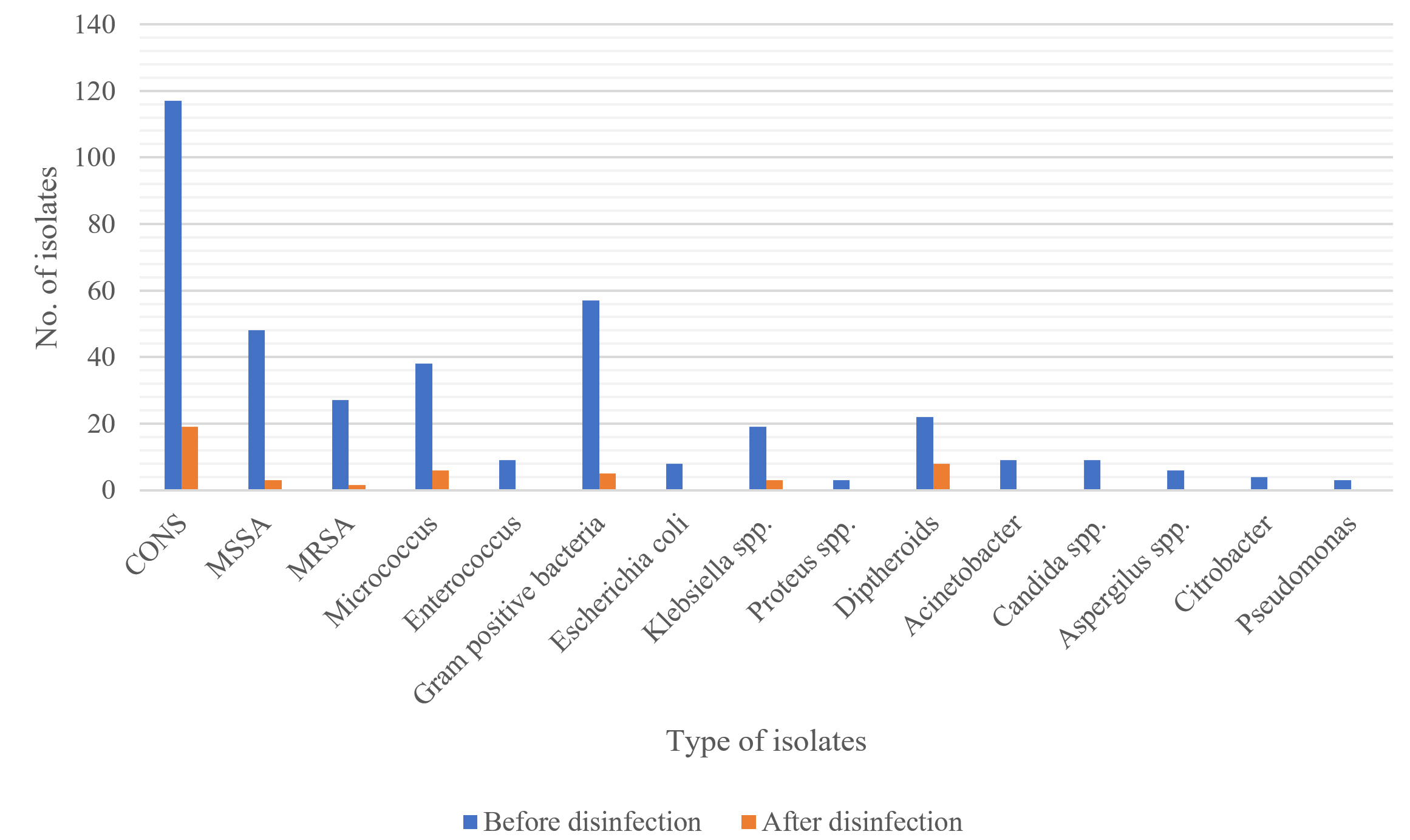
Fig. 2. Number of isolates obtained before and after disinfection
Out of 280 samples that showed growth, 145 samples (51.8%) were potent pathogens. Out of 145 pathogens isolated before disinfection, S. aureus (27%), Klebsiella (6.8%), Enterococcus (3.2%) and Candida (3.2%) contributed mainly for the bioburden which are well established cause of HCAI. Several studies reveal that S. aureus was the most common pathogen isolated from the stethoscope and the prevalence rate ranged from 12-55%10,33,37,40,43,44 followed followed by Klebsiella with prevalence range of 4.7 -20%10,43,45 which are well known cause of HCAI, posing potential risk in the health care settings proving that stethoscopes acts like a potential vector in transmitting HCAI.
Table (3):
Microbial growth (number of samples) after disinfection with the reagents.
| Disinfectant | After Disinfection | Total | |
|---|---|---|---|
| Stethoscopes not showing colonization | Stethoscopes showing colonization | ||
| 65% Ethyl Alcohol | 80 | 17 | 97 |
| 70% Isopropyl Alcohol | 86 | 7 | 93 |
| 1% Chlorhexidine | 70 | 20 | 90 |
| Total | 236 | 44 | 280 |
Among the 384 samples selected for the study, 280 samples had shown growth before disinfection. From Table 3, it can be clearly seen that among the disinfectants used, maximum antimicrobial activity was exhibited by IPA. 86 out of 93 samples (92.5%) were inhibited with IPA compared to 80 out of 97 samples (82.5%) with EA and 70 out of 90 samples (77.8%) with CH. IPA was applied for two different duration (time): (i) for 30 seconds and (ii) for 1 minute as described in Table 1. Table 2 tabulates the major data obtained from questionnaire survey. Among the 128 samples that was disinfected with IPA, 93 samples had shown growth. After applying IPA for 30 seconds, 45 out of 47 samples (95.7%) did not show colonization compared to 41 out of 46 samples (89.1%) for which IPA was applied for 1 minute. Table 4 shows the microbial growth after disinfection categorised against various departments/workplaces.
Table (4):
Microbial growth after disinfection in various departments.
| Department | After disinfection | Total | |
|---|---|---|---|
| No growth | Growth | ||
| Orthopaedics | 20 | 2 | 22 |
| Obstetrics and Gynaecology | 56 | 7 | 63 |
| Medicine | 56 | 7 | 63 |
| Operation Theatre | 23 | 1 | 24 |
| Paediatrics | 26 | 14 | 40 |
| Surgery | 37 | 9 | 46 |
| Others | 18 | 4 | 22 |
| Total | 236 | 44 | 280 |
The data obtained from the experimental results were mainly non-parametric and hence c2 tests of significance with 95% confidence level (a = 0.05) were carried out in this study to know if there were any associations between the varying factors like departments, type of HCW, growth after disinfection and type of reagents used. A significant association is confirmed if the probability falls below 0.05 (a = 5%).
KAP among different categories of HCW regarding stethoscope disinfection
The awareness regarding stethoscope maintenance was varying among the different HCW. 44% of the respondents were unaware of the maintenance and hence a c2 test was applied to know if there was any relationship between the awareness and the category of HCW. The test resulted in a p-value » 0, indicating a very highly significant association suggesting that the level of awareness about disinfection practice of stethoscopes were different among different categories of HCW. From the survey data, we can observe that students (40.1%) were least aware regarding maintenance compared to nurses (3.1%) and doctors (0.5%).
Another test of significance was applied to seek if any relationship exists between the category of HCW and the disinfecting agent they used. Similar to the previous test, the resulting p-value » 0 indicated that there was a very high association between the type of cleaning agent used and the category of HCW. Further from the survey data, we can observe that alcohol usage was maximum among doctors (34.2%) and least among students (15.7%). Soap and water usage was maximum among nurses (6.5%) and nil among doctors.
The results of the KAP study revealed that the awareness, knowledge and practice of stethoscope maintenance was not satisfactory among the students suggesting that there is a need to create awareness for the student community who are in the beginning stages of their medical practice, regarding the maintenance of the stethoscope and its role in transmitting HCAI.
Comparison of different reagents on the microbial growth after disinfection
A test of significance was carried out to see if there were any associations between the type of reagents and growth after disinfection. The contingency table for the same is shown in Table 3. A p-value of 0.02 suggested that there was a significant association between growths after disinfection with the type of reagent used. When tests of significance were made by coupling any two reagents, the following results were obtained:
- After disinfection, microbial growth had no association with EA and CH (p = 0.06) stating that there is no difference in antimicrobial activity using 65% EA or 1% CH in hospital environment with respect to stethoscope decontamination.
- After disinfection, microbial growth had a significant association with EA and IPA (p = 0.038). Hence, it can be statistically stated that the antimicrobial activity is different for EA and IPA. Further from the Table 3, we can observe that 70% IPA is superior to 65% EA.
- Similarly, significant association with CH and IPA (p = 0.005) was obtained suggesting the antimicrobial activity is different for CH and IPA. From Table 3, we can observe that 70% IPA is also superior to 1% CH.
Effect of duration of application of 70% IPA on the microbial growth
A c2 test of significance was carried out to know if there was any association between the duration of application of IPA with the growth after disinfection. A p-value of 0.23>>0.05 suggested that, there is no relationship between the microbial growth and the duration of application of IPA. In other words, the antimicrobial activity remains unaltered when IPA is applied either for 30 seconds or 1 minute.
Microbial growth after disinfection in different work places (departments)
A c2 test of significance was carried out to ascertain any associated relationship between growth and department in which the samples were obtained. A p-value of 0.009 suggested that there was a highly significant relationship between the microbial growth after disinfection and the departments statistically stating that the bioburden varies according to the departments. From Table 4, it can be noted that the highest growth was obtained in paediatrics department and the least from the operating rooms which is similar to the studies done by Worku, Derseh and Kumalo45. This may be due to either inadequate cleaning techniques followed in the paediatrics department or may be due to better maintenance followed in operating rooms with respect to decontamination of stethoscope. Another reason could be that, the microbes might have developed higher resistance to disinfecting agents in paediatrics department. However, further investigation on the departmental wise analyses lies out of the scope of this work which may be undertaken in future course.
A comparative study of three reagents namely, 65% ethyl alcohol, 70% isopropyl alcohol and 1% chlorhexidine was carried out to study their effectiveness on stethoscopes of health care workers. Stethoscope samples were obtained from various departments among doctors, nurses and students and questionnaires gathered data regarding the knowledge and practice. The bioburden was checked before and after disinfection. The major finding in this paper is that there is a huge lacuna in the knowledge and practice of stethoscope maintenance among the student community who are in their beginning stages of their medical practice. Hence this demands adequate awareness programmes to be imparted even in their curriculum regarding the role of stethoscope in HCAI and also its maintenance. It is also found that there is an association of microbial growth on various departments and paediatrics department shows highest growth. However, further studies to be carried out to ascertain chances in the growth pattern at various departments. 70% IPA has better antimicrobial activity compared to EA and CH with respect to stethoscope decontamination in hospital settings. Disinfecting stethoscope with 70% IPA for just 30 seconds is equally efficient in reducing the contamination rate compared to 1 minute, which will be a time saviour especially in the busy schedules. The antimicrobial susceptibility test was not performed and other than Staphylococcus aureus, other organisms were not identified to species level. The time since last usage of stethoscope, decontamination and data on adherence to hand hygiene and recontamination was not addressed demanding more studies addressing these issues.
ACKNOWLEDGMENTS
The authors would like to thank Indian Council of Medical Research (ICMR) for funding this project and Mr. Sooraj Mohan, Manipal Institute of Technology, Manipal who has provided assistance for the statistical techniques.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All listed author(s) have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
This project was supported by the Indian Council of Medical Research (ICMR) vide reference no. STS-2019-09116.
ETHICS STATEMENT
The study was approved by the ethical committee, Karwar Institute of Medical Sciences, Karwar, India.
AVAILABILITY OF DATA
The data will be made available on request.
- World Health Organization. Health care-associated infections FACT SHEET. https://www.who.int/gpsc/country_work/gpsc_ccisc_fact_sheet_en.pdf. Accessed March 17, 2020.
- Rosenthal VD, Maki DG, Salomao R, et al. Device-associated nosocomial infections in 55 intensive care units of 8 developing countries. Ann Intern Med. 2006;145(8):582-591.
Crossref - Kothari A, Sagar V, Ahluwalia V, Pillai BS, Madan M. Costs associated with hospital-acquired bacteraemia in an Indian hospital: a case-control study. J Hosp Infect. 2009;71(2):143-148.
Crossref - Stone PW. Economic burden of healthcare-associated infections: an American perspective. Expert Rev Pharmacoecon Outcomes Res. 2009;9(5):417-422.
Crossref - Narendranath V, Nandakumar BS, Sarala KS. Epidemiology of hospital-acquired infections in a tertiary care teaching hospital in India: a cross-sectional study of 79401 inpatients. Int J Community Med Public Heal. 2017;4(2):335.
Crossref - Kılıc I, Ozaslan M, Karagoz I, Zer Y, Savas E, Davutoglu V. The role of stethoscopes in the transmission of hospital infections. Afr J Biotechnol. 2011;10.
- Ghosh P, Chattopadhyay S, Gupta I, Pramanik S, Nandi P, Mitra GD. Unclean Stethoscope – A Tool For Hospital Acquired Infection. Int J Med Sci Clin Invent. 2016;3(9).
Crossref - Cohen HA, Amir J, Matalon A, Mayan R, Beni S, Barzilai A. Stethoscopes and otoscopes – a potential vector of infection? Fam Pract. 1997;14(6):446-449.
Crossref - Bukharie HA, Al-Zahrani H, Rubaish AM, Abdulmohsen MF. Bacterial contamination of stethoscopes. J Family Community Med. 2004;11(1):31-33.
- Shiferaw T, Beyene G, Kassa T, Sewunet T. Bacterial contamination, bacterial profile and antimicrobial susceptibility pattern of isolates from stethoscopes at Jimma University Specialized Hospital. Ann Clin Microbiol Antimicrob. 2013;12(1):39.
Crossref - Thapa S, Sapkota LB. Bacteriological assessment of stethoscopes used by healthcare workers in a tertiary care centre of Nepal. BMC Res Notes. 2017;10(1):353.
Crossref - Knecht VR, McGinniss JE, Shankar HM, et al. Molecular analysis of bacterial contamination on stethoscopes in an intensive care unit. Infect Control Hosp Epidemiol. 2019;40(2):171-177.
Crossref - Bansal A, Sarath RS, Bhan BD, Gupta K, Purwar S. To assess the stethoscope cleaning practices, microbial load and efficacy of cleaning stethoscopes with alcohol-based disinfectant in a tertiary care hospital. J Infect Prev. 2018;20(1):46-50.
Crossref - Bham G, Bhandari J, Neupane MR, Dawadi R, Pradhan P. Aerobic Bacteria in the Diaphragmatic Portion of Stethoscope of Medical Professionals of Tertiary Care Hospital. JNMA J Nepal Med Assoc. 2015;53(199):166-168.
Crossref - Vajravelu RK, Guerrero DM, Jury LA, Donskey CJ. Evaluation of Stethoscopes as Vectors of Clostridium difficile and Methicillin-Resistant Staphylococcus aureus. Infect Control Hosp Epidemiol. 2012;33(1):96-98.
Crossref - Gupta N, Gandham N, Misra R, Jadhav S, Ujgare M, Vyawahare C. The potential role of stethoscopes as a source of nosocomial infection. Med J Dr DY Patil Univ. 2014;7(2):156-159.
Crossref - Whittington AM, Whitlow G, Hewson D, Thomas C, Brett SJ. Bacterial contamination of stethoscopes on the intensive care unit. Anaesthesia. 2009;64(6):620-624.
Crossref - Holleck JL, Merchant N, Lin S, Gupta S. Can education influence stethoscope hygiene? Am J Infect Control. 2017;45(7):811-812.
- Jenkins IH, Monash B, Wu J, Amin A. The third hand: Low rates of stethoscope hygiene on general medical services. J Hosp Med. 2015;10(7):457-458.
Crossref - Sahiledengle B. Stethoscope disinfection is rarely done in Ethiopia: What are the associated factors? PLoS One. 2019;14(6):e0208365.
Crossref - Messina G, Spataro G, Rosadini D, et al. A novel approach to stethoscope hygiene: A coat-pocket innovation. Infect Dis Heal. 2018;23(4):211-216
Crossref - Alvarez JA, Ruiz SR, Mosqueda JL, et al. Decontamination of stethoscope membranes with chlorhexidine: Should it be recommended? Am J Infect Control. 2016;44(11):205-209.
Crossref - Napolitani M, Bezzini D, Moirano F, Bedogni C, Messina G. Methods of Disinfecting Stethoscopes: Systematic Review. Int J Environ Res Public Health. 2020;17(6):1856.
Crossref - Messina G, Fattorini M, Nante N, et al. Time Effectiveness of Ultraviolet C Light (UVC) Emitted by Light Emitting Diodes (LEDs) in Reducing Stethoscope Contamination. Int J Environ Res Public Health. 2016;13(10):940.
Crossref - Messina G, Rosadini D, Burgassi S, et al. Tanning the bugs – a pilot study of an innovative approach to stethoscope disinfection. J Hosp Infect. 2017;95(2):228-230.
Crossref - Billings A, Ambos S, Aying B, Rabenstein L, Cole J. Disinfecting Stethoscope Diaphragms Using an Alcohol-Based Handrub. Am J Infect Control. 2013;41(6):41.
Crossref - Cohen SR, McCormack DJ, Youkhana A, Wall R. Bacterial colonization of stethoscopes and the effect of cleaning. J Hosp Infect. 2003;55(3):236-237.
Crossref - Centers for Disease Control and Prevention. Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008.; 2019.
Crossref - Price PB. Ethyl Alcohol as A Germicide. Arch Surg. 1939;38(3):528-542.
Crossref - Lecat P, Cropp E, McCord G, Haller NA. Ethanol-based cleanser versus isopropyl alcohol to decontaminate stethoscopes. Am J Infect Control. 2009;37(3):241-243.
Crossref - Bernard L, Kereveur A, Durand D, et al. Bacterial Contamination of Hospital Physicians’ Stethoscopes. Infect Control Hosp Epidemiol. 1999;20(9):626-628.
Crossref - Boyce JM. Alcohols as Surface Disinfectants in Healthcare Settings. Infect Control Hosp Epidemiol. 2018;39(3):323-328.
Crossref - Raghubanshi BR, Sapkota S, Adhikari A, Dutta A, Bhattarai U, Bhandari R. Use of 90% ethanol to decontaminate stethoscopes in resource limited settings. Antimicrob Resist Infect Control. 2017;6(1):68.
Crossref - Jones JS, Hoerle D, Riekse R. Stethoscopes: A Potential Vector of Infection? Ann Emerg Med. 1995;26(3):296-299.
Crossref - Hibbard JS. Analyses comparing the antimicrobial activity and safety of current antiseptic agents: a review. J Infus Nurs. 2005;28(3):194-207.
doi:https://journals.lww.com/journalofinfusionnursing/Abstract/2005/05000/
Analyses_Comparing_the_Antimicrobial_Activity_and.8.aspx - Grandiere-Perez L, Bovet J, Beaudron A, et al. Efficacy of an ethanol-based hand sanitizer for disinfection of stethoscopes. J Hosp Infect. 2015;91(2):183-184.
Crossref - Parmar RC, Valvi CC, Sira P, Kamat JR. A prospective, randomised, double-blind study of comparative efficacy of immediate versus daily cleaning of stethoscope using 66% ethyl alcohol. Indian J Med Sci. 2004;58(10):423-430.
Crossref - Shukla B, Howell V, Griffiths A, et al. Superiority of chlorhexidine 2%/alcohol 70% wipes in decontaminating ultrasound equipment. Ultrasound. 2014;22(3):135-140.
Crossref - Fujita H, Hansen B, Hanel R. Bacterial contamination of stethoscope chest pieces and the effect of daily cleaning. J Vet Intern Med. 2013;27(2):354-358.
Crossref - Tonelotto B, Tortora JC, Tonelotto MDF. Profile bacteriological contamination of stethoscopes from intensivist physicians before and after decontamination with alcohol at 70%: 12AP4-3. Eur J Anaesthesiol. 2014;31.
Crossref - Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. 30th ed. Pennsylvania: Clinical and Laboratory Standards Institute; 2020.
- Montgomery DC. Design and Analysis of Experiments. John Wiley & Sons; 2008.
- Jeyakumari D, Nagajothi S, Kumar PR, Ilayaperumal G, Vigneshwaran S. Bacterial colonization of stethoscope used in the tertiary care teaching hospital: a potential source of nosocomial infection. Int J Res Med Sci. 2017;5(1):142-145.
Crossref - Grecia SC, Malanyaon O, Aguirre C. The effect of an educational intervention on the contamination rates of stethoscopes and on the knowledge, attitudes, and practices regarding the stethoscope use of healthcare providers in a tertiary care hospital. Philipp J Microbiol Infect Dis. 2008;37:20-33.
- Worku T, Derseh D, Kumalo A. Bacterial Profile and Antimicrobial Susceptibility Pattern of the Isolates from Stethoscope, Thermometer, and Inanimate Surfaces of Mizan-Tepi University Teaching Hospital, Southwest Ethiopia. Sanguinetti M, ed. Int J Microbiol. 2018:1-7.
Crossref
© The Author(s) 2020. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.