


ISSN: 0973-7510
E-ISSN: 2581-690X
Staphylococcus aureus (S. aureus) a noted versatile facultative commensal with pathogenic potential. This facultatively anaerobic cocci lives a commensal lifestyle in about a quarter of the world’s population awaiting a breach in the immune barrier to establish as a debilitating pathogen. This bacterium produces biofilms which acts as adhesive molecule enhancing the bacterial virulence and gives it an ability to withstand antibiotics, thereby causing tremendous burden on the healthcare community in terms of patient mortality and morbidity. This study assesses the biofilm producing ability among clinical isolates of staphylococci in comparison to colonizing staphylococci isolated from anterior nares of healthcare personnel. The present cross-sectional observational study was conducted in a tertiary care hospital in Mysore, India. In this study, 50 pathogenic isolates of S. aureus were assessed for phenotypic biofilm production. Additionally, 100 healthcare personnel were screened for nasal colonisation with S. aureus and the colonizing isolates were also screened for phenotypic biofilm formation. Phenotypic biofilm formation was evident among 22% of the pathogenic isolates. 23% of clinical S. aureus isolates demonstrated methicillin resistance (MRSA). There was no significant association of MRSA status with biofilm production (p > 0.05). Out of the 100 healthcare professionals screened for nasal carriage of S. aureus, 30% were colonized with S. aureus. Biofilm production among colonizing S. aureus isolates was found to be 26.6%. Methicillin resistance was a whopping 40% among the colonising strains. MRSA carriage was found to be highest among those healthcare personnel who had worked for an average of 20-30 years in the hospital environment. The Present study showed no significant association of biofilm production with the pathogenic potential of the S. aureus isolates (p > 0.05). Additionally, there was no significant association of methicillin resistance with the pathogenicity of the isolate. In conclusion, the interplay of virulence genes, biofilm forming ability, drug resistance of the isolate in coordination with the host immune status dictate the fate of the colonising as well as clinical isolates of S. aureus.
Biofilm, Methicillin Resistant Staphylococcus aureus (MRSA), Staphylococcus aureus, Immunocompromised, Health Care Personnel
Staphylococcus is a diverse genus of bacterium that encompasses both harmful pathogens and benign commensals. Among these, S. aureus stands out as a frequently encountered complex pathogen capable of causing severe morbidity in individuals with varying degrees of immune competence.1 S. aureus commonly inhabits the skin and nasal passages without causing harm. However, breaches in the skin barrier can lead to serious infections or even fatalities, highlighting the potential danger posed by this organism. As a pathogen, this bacterium is accountable for an assorted range of thousands to millions of invasive infections globally.2 S. aureus produces an array of virulence factors along with factors responsible for immune evasion3,4 resulting in acute, recurrent, chronic, or persistent infections.
The role of this bacteria as one of the foremost opportunistic pathogens can be attributed to its frequent human colonisation.5 Particularly concerning is the role of nasal conveyance of Staphylococcus among personnel working in healthcare setting, serving as a major source of infection and contributing to documented outbreaks worldwide. S. aureus colonisation in the anterior nares further increases the infection risk associated with this bacterium. Colonisation with S. aureus among Health Care Workers (HCWs) increases the chances of transmission and infection with antibiotic resistant hospital acquired S. aureus strains.6 MRSA was identified in the year 1961 from England. MRSA development involves horizontal transfer of staphylococcal cassette chromosome (SCC).7 Until the 1990s, MRSA was predominantly a hospital-associated pathogen. Healthcare workers act as reservoirs as well as victims of resistance cross-transmission given their workplace exposure.8 However, cases of community-acquired MRSA infections have emerged worldwide affecting individuals without any history of hospitalization.9 In the present day healthcare setting, community-acquired S. aureus infections resistant to methicillin present as moderately severe infections. Notably, healthy adults without predisposing conditions can also be infected. Today, both hospital-acquired and community-acquired MRSA have become a global concern.10
Notable among the virulence factors of S. aureus is the biofilm production, which enables host intracellular adhesion.11 Compared to their planktonic forms S. aureus cells encased by biofilms show higher rates of antibiotic resistance, and differences in phenotypic characteristics such as cell size, growth rate, gene expression and protein production.11 These biofilms facilitate chronic infections and bolster bacterial resistance against host defence mechanisms, posing significant challenges in treatment. The Present study discerns presence of biofilm forming capacity among clinical S. aureus isolates in comparison to colonising commensal S. aureus isolated among HCWs.
This Cross-sectional study was done in 1,800 bedded hospital. In the present study, 50 clinical S. aureus isolates were phenotypically characterised & studied for biofilm forming ability. Subsequently, 100 HCWs were screened for S. aureus colonisation in their anterior nares. The isolates thus obtained from HCW were phenotypically identified and studied for biofilm production.
Phenotypic identification of clinical S. aureus isolates
Patient samples like pus, exudate, urine, endotracheal secretions, and blood samples sent for culture and sensitivity were subjected to Gram staining and culture identification by VITEK-2 system and antibiotic susceptibility testing in accordance with the National Accreditation Board for Laboratories (NABL) standards. Demographical data & Clinical data was fetched through the Laboratory Information system.
Screening of HCW for nasal colonization of S. aureus
The HCWs were screened for S. aureus colonisation after obtaining a written informed consent. Demographic information, such as age, sex, designation, and number of years spent in hospital environment was documented.
Samples were obtained from both the anterior nares using sterile swabs. Labelled swabs were sent to the microbiology laboratory for bacteriological analysis. Swabs obtained were inoculated on sterile Blood Agar and incubated for 48 hours at 37°C.
Screening of S. aureus isolates for biofilm production & methicillin resistance
All S. aureus isolates included in the study were phenotypically screened for methicillin resistance and biofilm formation.
Methicillin resistance determination was performed by disc diffusion method using cefoxitin disc (30 µg). In brief, a lawn culture of the test organism was made on Mueller-Hinton agar (MHA) plate, inoculum was standardised to McFarland’s 0.5 standard, a cefoxitin disc (30 µg) was placed on the agar surface and lightly pressed. After incubation, for 24 hours at 37°C the zone of inhibition was documented. The quality controls were MSSA ATCC 25923 and MRSA ATCC 43300.
Interpretation
Isolates with inhibition zones of ≤21 mm in diameter were classified as MRSA, while those with zones diameter of ≥22 mm was classified as MSSA.12
Phenotypic method of Biofilm detection
The biofilm producing capacity of the isolates were screened by 3 methods: 1. Congo red agar (CRA) method, 2. Tube method (TM), 3. The gold standard-TCP method.13
CRA method
Sucrose supplemented Brain Heart Infusion (BHI) agar was prepared. Autoclaved Congo red dye was inoculated at a temperature of 55°C. Next, the test strains were inoculated onto this and incubated aerobically for 24 hours at 37°C.
Interpretation: Positive test
Development of black coloured colonies.
Negative test
Development of red coloured colonies.
Tube Method
1% glucose-supplemented Trypticase soy broth (TSB) was inoculated with the test organism. After 24 hour incubation at 37°C, the washed tubes were air-dried. Upon staining with Crystal violet (0.1%) tubes were dried in inverted position. Triplicate assay was performed and observed for biofilm formation.
Interpretation
Lining of the tube inner surface was considered as positive biofilm formation. Results were graded as strong (+++), moderate (++), weak/none (-) based on the intensity of the stain taken by the organisms in biofilm.
TCP Method
This is a micro-titre plate quantitative assay. The test organism from fresh culture was inoculated into 1% glucose-supplemented Trypticase Soy Broth (TSB) which after 24 hour incubation at 37°C was diluted hundred-fold (1:100) with fresh TSB. Next, 200 µl of this prepared specimen was inoculated into polystyrene, flat-bottom tissue culture wells. After incubation, at 37°C for 24 hours the contents of each well were gently removed by pipetting and slowly tapping the plates. The wells were washed at a pH of 7 and then air dried. Subsequently, using 2% sodium acetate and 1% crystal violet the wells were fixed & stained. Micro-ELISA auto reader was used to determine the optical density (OD) of stained adherent bacteria at 570 nm. Experiments for each isolate was performed in triplicate and biofilm production was detected & characterised based on OD reading
Biofilm production was categorised based on the optical density (OD) readings of adhering cells.13
Screening of Healthcare workers for nasal colonization of S. aureus
A total of 100 healthcare workers were screened during the study period. Swabs yielding white beta-haemolytic colonies on blood agar (Figure 1) were identified biochemically by catalase and coagulase test & further confirmed by Vitek 2 system as S. aureus isolates. Among the HCWs 97 were staff nurses and 3 were nursing interns. 85% of the HCWs were females and 15% were males. S. aureus colonisation was found in 30% of HCWs.
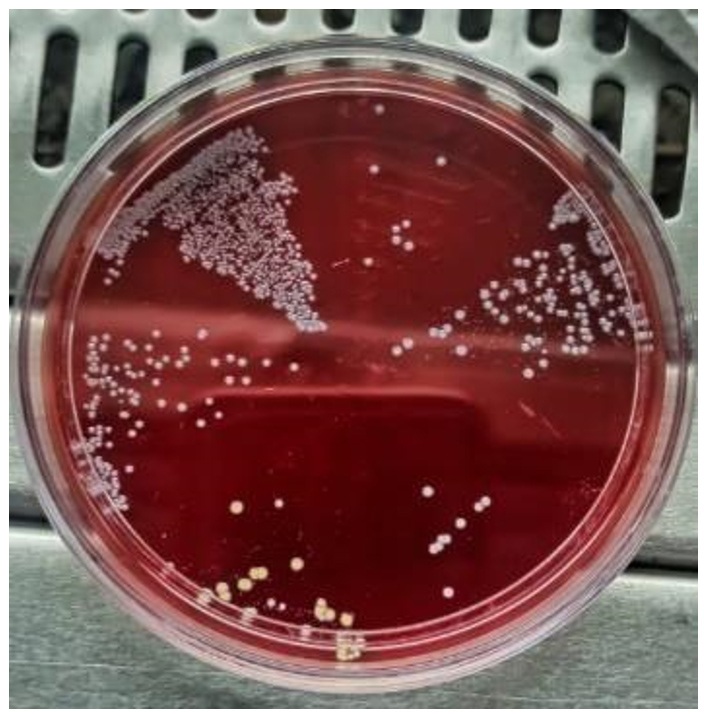
Figure 1. Swab inoculated on blood agar plates after incubation showing beta-lytic colonies
Methicillin resistance (Figure 2) was evident among 12 (40%) isolates. Maximum number of MRSA were isolated from HCWs with >20 years of exposure to the healthcare environment as depicted in Figure 3.
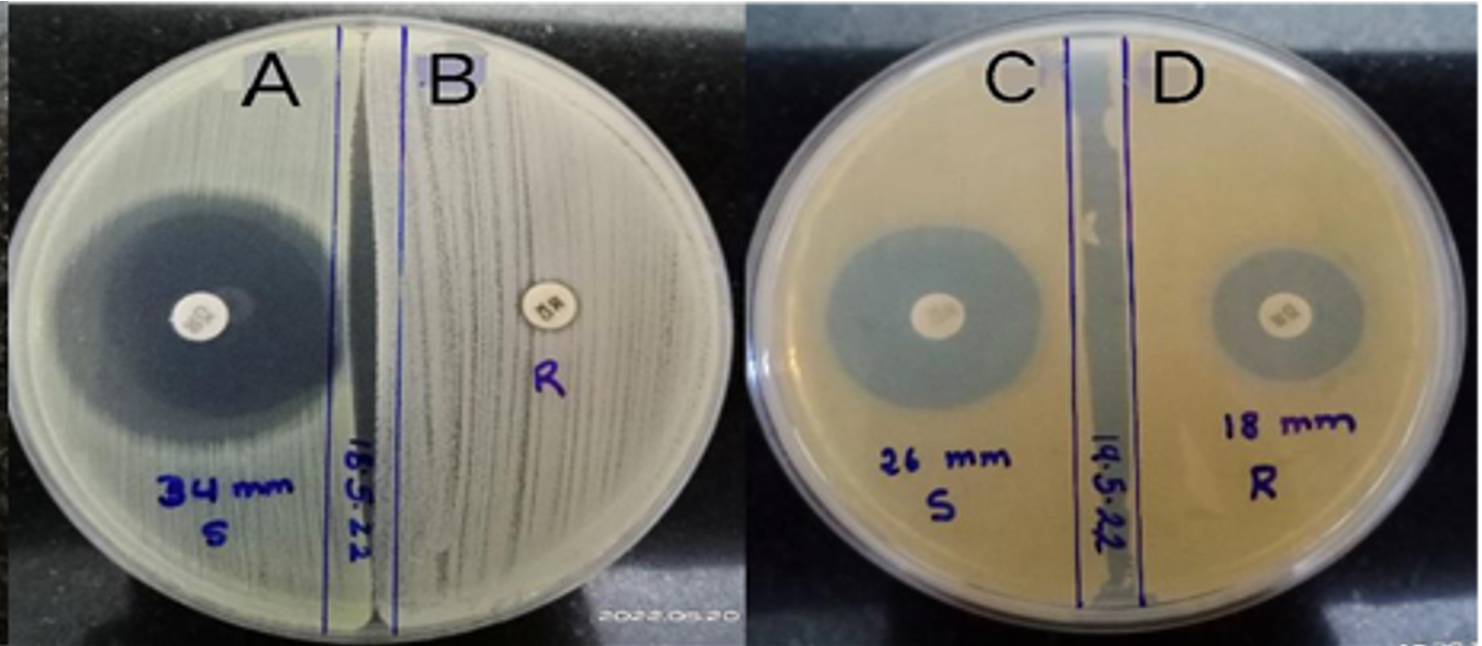
Figure 2. Methicillin resistance determination by disc diffusion
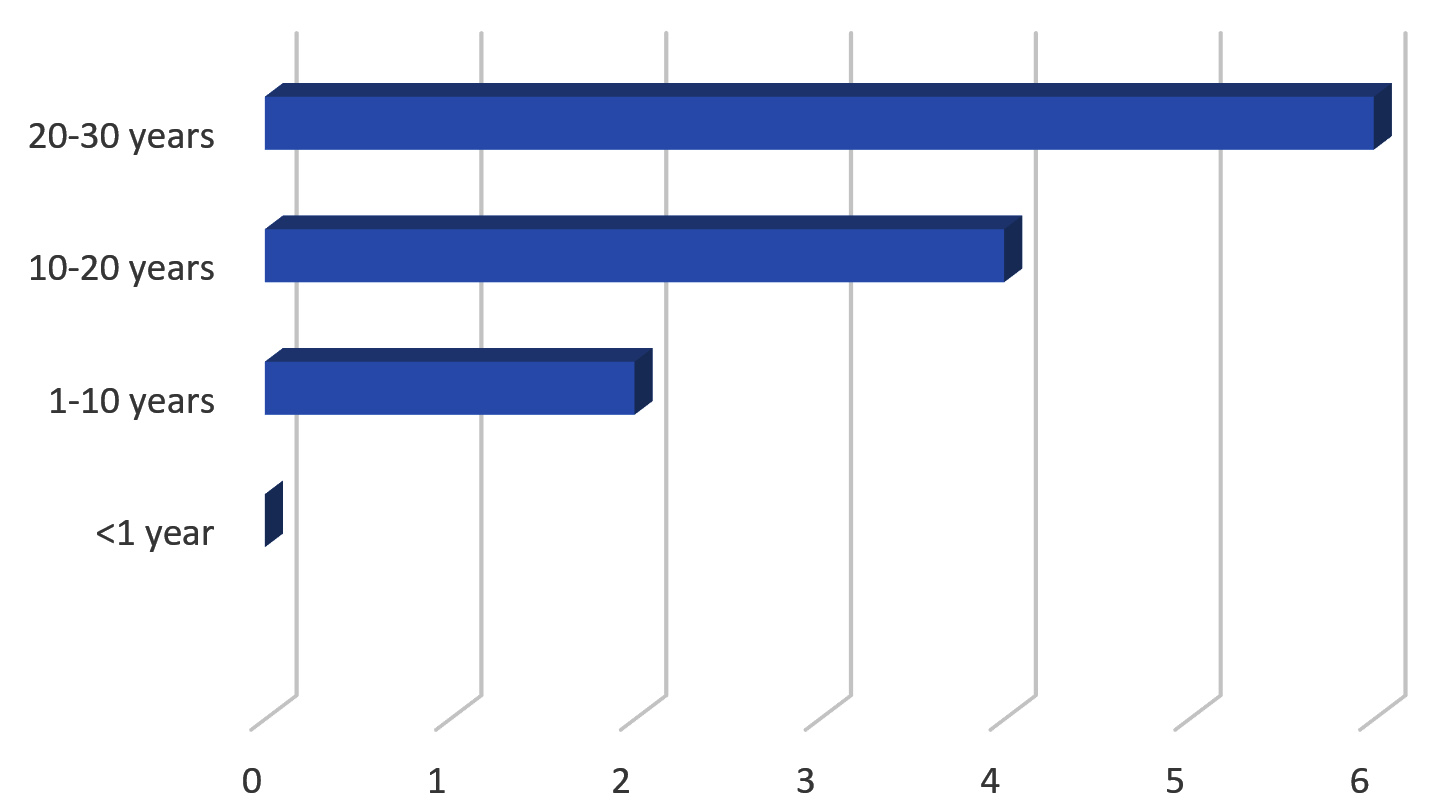
Figure 3. MRSA distribution in HCW with years of experience in health sector
Clinical Isolates
Among the 50 S. aureus isolates, 34 were obtained from pus, 11 from blood, and 5 from urine samples. Methicillin resistance was seen among 23 (46%) of the clinical isolates of S. aureus.
Biofilm production among clinical & colonizing S. aureus isolates by TCP method
Among the 50 clinical isolates of S. aureus, 11 (22%) isolates were biofilm producers of which 4 were strong & 7 were moderate biofilm producers.
Among the 30 colonizing S. aureus isolates, obtained from HCWs 8 (26.67%) were biofilm producers of which 3 were strong & 5 were moderate biofilm producers. Large proportion of biofilm producing S. aureus were isolated from HCWs with >20 years of exposure to the healthcare environment. Present study showed no significant association of biofilm production with the pathogenic potential of S. aureus (p > 0. 05).
Among the 80 S. aureus were isolated in the present study, 50 were clinical isolates and 30 were colonisers. Among the 50 clinical isolates of S. aureus, 23 (46%) were MRSA and 27 (54%) were MSSA. Among the 30 colonisers, 12 (40%) were MRSA and 18 (60%) were MSSA as depicted in Figure 4.
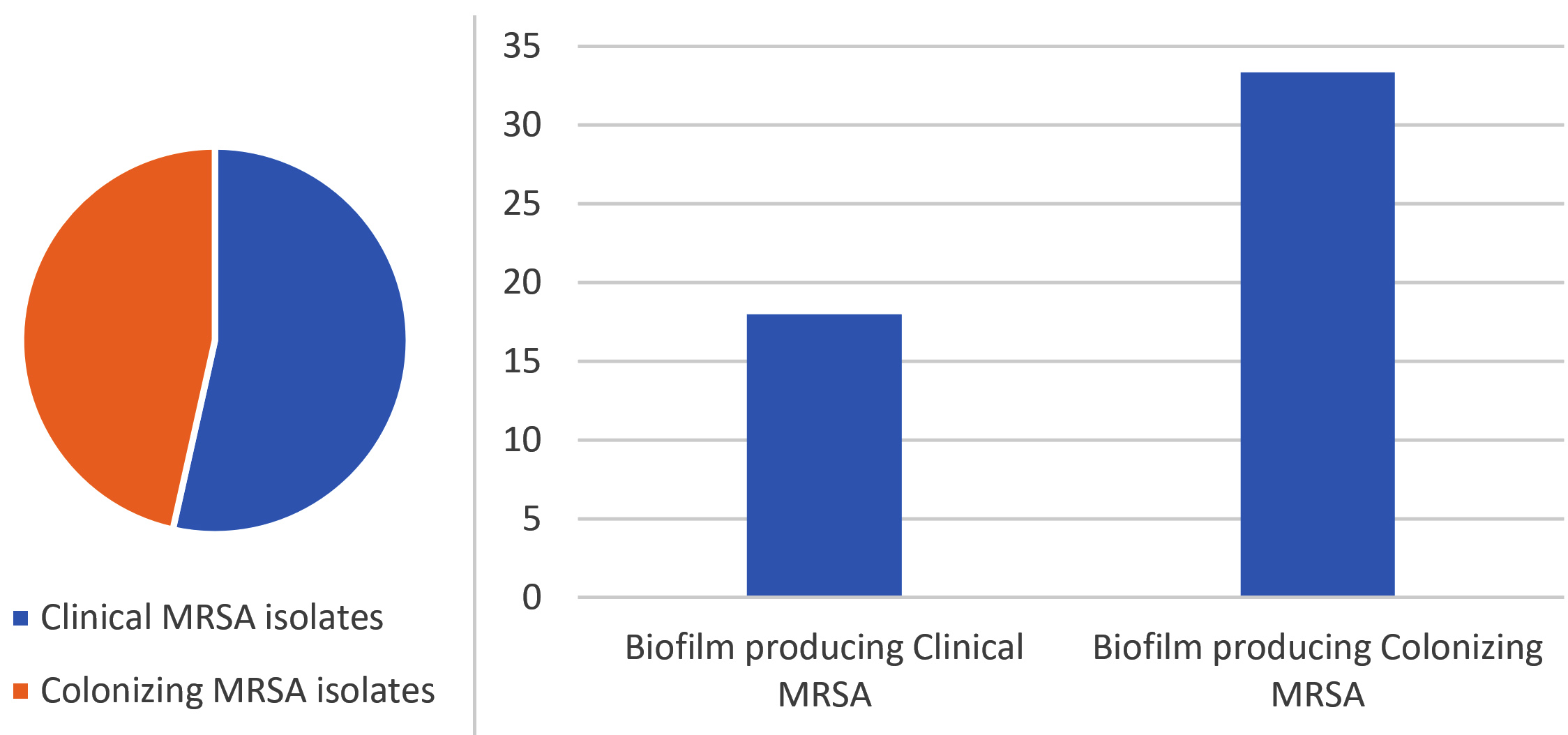
Figure 4. MRSA distribution and biofilm formation among MRSA isolates
Comparison of biofilm detection by different phenotypic methods
The 50 clinical isolates & 30 colonising S. aureus isolates were screened by 3 different phenotypic methods for biofilm which yielded the following results:
TCP method
19 (23.75%) isolates showed biofilm production (Figure 5). 7 isolates were strong and 12 were moderate biofilm producers as listed in Table 1.
Table (1):
Biofilm production using the TCP method
Samples |
Strong Biofilm |
Moderate Biofilm |
Weak/non biofilm producers |
|---|---|---|---|
Clinical isolates [50] |
3 |
8 |
39 |
Commensal isolates [30] |
4 |
4 |
22 |
Total and percentage (%) |
(7) 8.75% |
(12) 15% |
(61) 76.25% |

Figure 5. TCP method showing strong, moderate, weak/none biofilm
Tube method
Out of the 80 isolates which were screened for biofilm production by tube method, 17.5% showed biofilm formation (Figure 6) as depicted in Table 2.

Figure 6. Tube Method showing A: No-Biofilm; B: Moderate-Biofilm; C: Strong Biofilm
Table (2):
Biofilm production using the Tube method
Samples |
Strong Biofilm |
Moderate Biofilm |
Weak/non biofilm |
|---|---|---|---|
Clinical isolates [50] |
3 |
4 |
43 |
Commensal isolates [30] |
3 |
4 |
23 |
Total and percentage (%) |
(6) 7.5% |
(8) 10% |
(66) 82.5% |
Congo Red Agar method
The CRA method detected 16.25% of biofilm production (Figure 7) as depicted in Table 3.

Figure 7. CRA showing dry crystalline black biofilm producing colonies and red non biofilm producing colonies
Table (3):
Biofilm production using the Congo Red Agar method
Samples |
Positive |
Negative |
|---|---|---|
Clinical isolates [50] |
6 |
44 |
Commensal isolates [30] |
7 |
23 |
Total and percentage (%) |
(13) 16.25% |
(67) 83.75% |
Comparative analysis of Biofilm detection
Considering TCP as the gold standard detection method14 the statistical parameters were as follows: The Tube method showed a sensitivity of 79.17% with 100% specificity. The negative predictive value of the tube method was 92.42% with an accuracy of 94.12%. The CRA method showed a sensitivity of 76% and 100% specificity. The negative predictive value of CRA was found to be 91.04% with an accuracy of 93.02%. The ROC curve is depicted in Figure 8. Both the tests had an excellent positive predictive value of 100% in comparison to the gold standard test.
Figure 8. ROC analysis for phenotypic bio-film detection
In our study, the clinical S. aureus isolates were studied to assess their MRSA status & biofilm-forming ability. Synchronously, HCWs were screened for carriage of S. aureus in their anterior nares which were also looked for MRSA status & biofilm forming potential.
The clinical S. aureus isolates showed an MRSA rate of 46%. A study done in Nepal showed a similar 46% prevalence of MRSA rate from clinical isolates.15 Our study showed 30%
S. aureus carriage with 40% methicillin resistance among the colonising isolates. A study in Ethiopia by Mekuriya et al. showed 27.1% MRSA carriage among HCWs with S. aureus colonization.16 A study in Brazil showed 16.8% MRSA carriage among HCWs.17 A study in Nepal showed 35.3% methicillin resistance.18 All of the above studies saw the MRSA prevalence among different sectors of HCW including nurses, interns, doctors & other auxiliary hospital staff. In our study, the maximum enrolled HCWs were nurses working in close quarters for long hours in patient care which explains the higher rate of MRSA carriage encountered in this study.
Biofilm production rate was similar with no significant difference among clinical & colonising S. aureus isolates in this study. The study had 19 phenotypic biofilm forming S.aureus isolates among which 9 were MRSA (47.3%). A study in Hungary showed 39% MRSA isolates produced biofilms.19 Of the 3 methods used for phenotypic biofilm detection the yield of TCP method was the highest with 23.75% biofilm detection. A study by Knobloch et al.,20 have defied the use of CRA method for biofilm detection among S. aureus isolates. The present study also finds that CRA had only 76% sensitivity in comparison to the tube method which had a sensitivity of 79.17%. Under optimised conditions the TCP method yielded 23.75% biofilm formation with 57.89% being clinical isolates & 42.10% being commensal isolates therefore highlighting the biofilm-forming capacity of commensal isolates. Literature shows conflicting evidence in terms of the association of biofilm production with MRSA status. The Present study did not show any significant association with 52.7% of isolates being MSSA in agreement with results published by Arslan et al. & Senobar et al.19 This study shows an increasing rate of MRSA colonisation with the increase in the number of years of exposure to the health care environment among HCWs, therefore, highlighting the need for eradication of colonising S. aureus among HCWs in addition to timely monitoring of carrier status. This can reduce Healthcare associated S. aureus infections to a great extent while promising better health to our HCWs.
S. aureus is an exceptionally adaptable multifaceted pathogen capable of biofilm production and adaptable to both natural environment as well as clinical situations. The study deduces no concrete association of methicillin resistance with biofilm formation. Biofilm-formation among S. aureus isolates irrespective of methicillin resistance status is a cardinal step in the pathogenesis and establishment of chronicity. Comparative analysis of the three phenotypic methods used for biofilm detection showed higher detection rates by the gold standard TCP method. The tube method and CRA showed lower yield in comparison to the gold standard test.
Our study was a cross-sectional study hence it carried the limitation of selection bias and only phenotypic biofilm detection was done in the present study. However, the study provides insights regarding the methicillin susceptibility & biofilm-formation among commensal S.aureus with relevance to the clinical counterpart isolates. In conclusion, the interplay of virulence genes, biofilm forming ability, drug resistance of an isolate in coordination with immune footing of the host dictates the fate of the colonising or clinical S. aureus isolate.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, JSS Medical College, Karnataka, India, with reference number JSSMC/IEC/130924/49 NCT/2024-25.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Foster T. Staphylococcus. In: Baron S, editor. Medical Microbiology. 4th ed. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 12.
- Cheung GYC, Bae JS, Otto M. Pathogenicity and virulence of Staphylococcus aureus. Virulence. 2021;12(1):547-569.
Crossref - Spaan AN, van Strijp JAG, Torres VJ. Leukocidins: staphylococcal bi-component pore-forming toxins find their receptors. Nat Rev Microbiol. 2017;15(7):435-447.
Crossref - Thammavongsa V, Kim HK, Missiakas D, Schneewind O. Staphylococcal manipulation of host immune responses. Nat Rev Microbiol. 2015;13(9):529-543.
Crossref - Howden BP, Giulieri SG, Lung TWF, et al. Staphylococcus aureus host interactions and adaptation. Nat Rev Microbiol. 2023;21(6):380-395.
Crossref - McAdam PR, Templeton KE, Edwards GF, et al. Molecular tracing of the emergence, adaptation, and transmission of hospital-associated methicillin-resistant Staphylococcus aureus. Proc Natl Acad Sci U S A. 2012;109(23):9107-9112.
Crossref - Abusheraida NSA, AlBaker AAH, Aljabri ASA, et al. Rapid Visual Detection of Methicillin-Resistant Staphylococcus aureus in Human Clinical Samples via Closed LAMP Assay Targeting mecA and spa Genes. Microorganisms. 2024;12(1):157.
Crossref - Albrich WC, Harbarth S. Health-care workers: source, vector, or victim of MRSA. Lancet Infect Dis. 2008;8(5):289-301.
Crossref - Tenover FC, McDougal LK, Goering RV, et al. Characterization of a strain of community-associated methicillin-resistant Staphylococcus aureus widely disseminated in the United States. J Clin Microbiol. 2006;44(1):108-118.
Crossref - Junaidi NSSA, Shakrin NNSM, Desa MNM, Yunus WMZW. Dissemination Pattern of Hospital-Acquired Methicillin-Resistant Staphylococcus aureus and Community-Acquired MRSA Isolates from Malaysian Hospitals: A Review from a Molecular Perspective. Malays J Med Sci. 2023;30(2):26-41.
Crossref - Nguyen HTT, Nguyen TH, Otto M. The staphylococcal exopolysaccharide PIA-Biosynthesis and role in biofilm formation, colonisation, and infection. Comput Struct Biotechnol J. 2020;18:3324-3334.
Crossref - Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; 26 ed.CLSI supplement M100S. Clinical and Laboratory Standards Institute, Wayne, PA. 2016.
- Idrees M, Sawant S, Karodia N, Rahman A. Staphylococcus aureus Biofilm: Morphology, Genetics, Pathogenesis and Treatment Strategies. Int J Environ Res Public Health. 2021;18(14):7602.
Crossref - Panda PS, Chaudhary U, Dube SK. Comparison of four different methods for detection of biofilm formation by uropathogens. Indian J Pathol Microbiol. 2016;59(2):177-179.
- Kandel SN, Adhikari N, Dhungel B, et al. Characteristics of Staphylococcus aureus Isolated From Clinical Specimens in a Tertiary Care Hospital, Kathmandu, Nepal. Microbiol Insights. 2020;13:1178636120972695.
Crossref - Mekuriya E, Manilal A, Aklilu A, Woldemariam M, Hailu T, Wasihun B. Methicillin-resistant Staphylococcus aureus colonization among medicine and health science students, Arba Minch University, Ethiopia. Sci Rep. 2022;12(1):10161.
Crossref - da Silva LSC, Andrade YMFS, Oliveira AC, et al. Prevalence of methicillin-resistant Staphylococcus aureus colonization among healthcare workers at a tertiary care hospital in northeastern Brazil. Infect Prev Pract. 2020;2(4):100084.
Crossref - Giri N, Maharjan S, Thapa TB, et al. Nasal Carriage of Methicillin Resistant Staphylococcus aureus among Healthcare Workers in a Tertiary Care Hospital, Kathmandu, Nepal. Int J Microbiol. 2021;2021(1):8825746.
Crossref - Tahaei SAS, Stajer A, Barrak I, Ostorhazi E, Szabo D, Gajdacs M. Correlation between biofilm-formation and the antibiotic-resistant phenotype in Staphylococcus aureus isolates a laboratory-based study in Hungary and a review of the literature. Infect Drug Resist. 2021;14:1155-1168.
Crossref - Knobloch JKM, Horstkotte MA, Rohde H, Mack D. Evaluation of different detection methods of biofilm formation in Staphylococcus aureus. Med Microbiol Immunol. 2002;191(2):101-6.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.