

ISSN: 0973-7510
E-ISSN: 2581-690X
Group B Streptococcus (GBS) is an opportunistic harmless bacterium which the leading cause of neonatal infections. Our purpose was to determine capsular genotypes distribution and antibiotic resistance pattern of GBS isolated from clinical samples. Two hundred and twenty two GBS strains isolated from clinical samples from different hospitals in Tehran, Iran. After identification by specific cultures and biochemical tests, broth microdilution method was used to determine the minimal inhibitory concentration (MIC) of antibiotics based on standard protocol. The erythromycin-clindamycin double-disk test was used to determine the inducible resistance phenotypes. Capsular genotypes were identified by PCR method. The high rates of antibiotic resistance in GBS were related to gentamycin 89.18%, tetracycline 87.38%, kanamycin 62.16%, clindamycin (67.1%), erythromycin 57.2%, and chloramphenicol 32.8%. All strains were sensitive to vancomycin, penicillin, and ampicillin. Between eleven capsular antigens, serotypes such as III (50.9%), V (27.47%), Ib (17.76%), Ia (15.54%), Ic (5.85%) were the highest. The genotypes distribution and the patterns of resistance phenotypes of GBS may vary in different areas. Thus, it is required to be considered in each region to work out strategies for prevention. The PCR method is recommended as a rapid and reliable technique for identification and molecular epidemiology study of GBS.
Group B Streptococcus (GBS), Genotypic characterization, Antibiotic Resistance.
GBS is one of the primary agents of invasive infections such as sepsis and meningitis in neonatal from birth to 4 weeks of age. Also, GBS is a significant pathogen in geriatrics and those with underlying medical disorders1
Ten to 30% of pregnant women are colonized asymptomatically by GBS in their vagina and rectum. If newborns are exposed to GBS during delivery, close to 50.0% will be colonized and invasive infection will almost increase 2.0%. Routine screening for maternal colonization by GBS is useful for prevention of neonatal infections2-4
Drugs of choice for treatment of b-hemolytic streptococcal infections are penicillin and ampicillin. Non susceptible b-hemolytic Streptococcus isolates (i.e., penicillin MICs > 0.12 and ampicillin MICs > 0.25 µg/mL) are extremely rare .So, based on FDA reports (the US Food and Drug Administration), susceptibility testing for treatment of ²-hemolytic streptococcal infections need not to be performed routinely. If antibiotic susceptibility testing is done and each ²-hemolytic streptococcal strain detected to be non susceptible should be retested, and reported to an emergency for public health.
Penicillin or ampicillin is recommended for intrapartum prophylaxis against GBS. For at low risk, cefazolin is recommended for anaphylaxis. In case of patients at high risk clindamycin is consumed for anaphylaxis. GBS usually are not resistant to cefazolin, penicillin, and ampicillin, but may be resistant to clindamycin and erythromycin. When a GBS is detected in a pregnant penicillin-allergic woman, inducible clindamycin resistance should be tested by erythromycin and clindamycin, and only clindamycin should be reported. (5) Unfortunately, multi-drug resistant GBS is increasing and there is a little information on the antibiotic resistance patterns against β-lactams, aminoglycosides, and macrolides.
An important target for vaccine strategies against GBS is capsular polysaccharide. Having different chemical and antigenic characters, GBS capsular polysaccharides have been subdivided into eleven serotypes such as Ia, Ib, Ic, II-IX serotypes6 Vaccines against infections due to GBS must include the main serotypes associated with disease in different communities7 Study of the epidemiological distribution of GBS serotypes may be different based on several aspects, containing studied population, the geographical region, and source of bacterial isolate8
GBS can be subdivided into types Ia, Ib, Ic, II, and III. Almost, 99% of GBS strains can be belonged to one of these five antigen types9 In the United States and in some European countries, Ia, II, III and V are generally the most frequently isolates, and VI to IX serotypes are seldom detected6,8,10-12 In Brazil, the emerging of Ia, Ib, II, III, IV and V serotypes has been identified in a few studies in South and the Southeast area13-18
So, in this epidemiological study, we examined capsular genotypes of GBS by PCR regarding to antibiotic resistant pattern in clinical isolates by means of disk diffusion and broth dilution.
GBS detection
In this descriptive study, a total of 222 GBS isolated from clinical samples such as urine, skin and soft tissue, bone, joint, blood, CSF, pleural fluid. Clinical samples were gathered during two years (between June 2013 and May 2015) from Mofid Children hospital, Loghman Hakim hospital and Milad Hospital, Tehran, Iran. Appearance of GBS colonies on blood agar plates were gray-white and tiny colonies with a b-hemolysis halo. Primary identification was hemolytic, gram-positive cocci with catalase-negative reaction. GBS distinction from other streptococci was based on biochemical reactions including resistance to bacitracin and trimethoprim-sulfamethoxazole (SXT), sodium hippurate hydrolysis, and positive CAMP test2,4,9,19-22
Antimicrobial susceptibility testing Methods
All isolates were tested for ampicillin (10µg), cefotaxime, ceftriaxone (30µg), clindamycin (2µg), chloramphenicol(30µg), erythromycin(15µg), levofloxacin (5µg), penicillin (10 unit), vancomycin (30µg), kanamycin (30 µg), streptomycin (10 µg), gentamycin (30µ) and tetracycline (30µg). We used Mueller-Hinton agar (MHA) supplemented by 5% sheep blood for disk diffusion method. For broth dilution method we prepared cation-adjusted Mueller-Hinton broth (CAMHB) supplemented by 2.5% to 5% v/v lysed horse blood (LHB). For McFarland concentration preparation was done. All media were incubated in 35±2°C.Five percent of CO2 during 20 to 24 hours incubation was prepared for disk diffusion method; and for dilution methods was in ambient air condition during 20 to 24 hours incubation time.
Zone of inhibition (mm) was measured and reported as susceptible, intermediate or resistant by according to the CLSI guidelines. By following the guidelines recommended by the CLSI, screening test for detection of inducible clindamycin resistance in GBS was determined using a broth microdilution method. One µg/mL erythromycin and 0.5 µg/mL clindamycin in same well was used and minimal inhibitory concentration (MICs) was reported. Any growth was reported as inducible clindamycin resistance and no growth was reported as no inducible clindamycin resistance5
Additionally, to ensure the reproducibility of the MICs for each strain, determinations were repeated three times. Streptococcus pneumoniae ATCC 49619 was used as quality control strain. For β-lactamase activity detection, a nitrocefin-based disc procedure (BD Diagnostics) was used. To detection of the inducible resistance phenotypes, erythromycin-clindamycin double-disk test was used23
Capsular genotypes detection
By AccuPrep Genomic DNA extraction kit (cat.no.k-3032 lot no.1008J, BIONEER) DNA was extracted from all GBS isolates. PCR amplification profile comprised a 300nM concentration of each oligonucleotide primer (Eurofins MWG Operon); 200mM (each) deoxynucleoside triphosphates dCTP, dGTP, dATP, and dUTP; 0.125 U of Taq DNA polymerase; and 5.5mM MgCl2 (from GENET BIO, prime Taq TM DNA polymerase, URL: www.genetbio.com)
The PCR products were analyzed by gel electrophoresis on 1.5% BIONEER agarose gels in 1X TBE buffer (890mM of boric acid, 890mM Tris, 40ml of 0.5 M EDTA, pH 8.0) at 100 V for 60 min. Green loading buffer with DNA stain (Jena Bioscience, Lot:111.034) was used during loading the samples and ladder. The sizes of the PCR products were determined by comparison with the molecular size standard (50bp-1Kb linear scale; low range DNA ladder or 100bp-3Kb linear scale and mid-range DNA ladder, Jena Bioscience(. Primer sequences, PCR conditions ,and electrophoresis for Ia, Ib, Ic, II- IX6,13,22, S. agalactiea 16srRNA24, as described previously.
Statistics
As the study is a descriptive, there is no need to state about statistical methods and software.
A total of 222 GBS isolates collected from clinical samples (skin and soft tissue 18 (8.1%), bone10 (4.5%), join 13 (5.8%), CSF 16 (7.2%), pleural fluid 29 (13.06%), urine 16 (7.2%), and vagina107(48.19%)] were investigated for antibiotic susceptibility test. Capsular genotyping and resistance-related genes distribution of GBS were considered by PCR method.
The percentages of resistance to gentamycin (89.18%), tetracycline (87.38%), clindamycin (67.1%), kanamycin (62.16%), erythromycin (57.2%), and chloramphenicol (32.8%) were the highest. All of strains were sensitive to vancomycin, penicillin, and ampicillin. (Fig. 1)
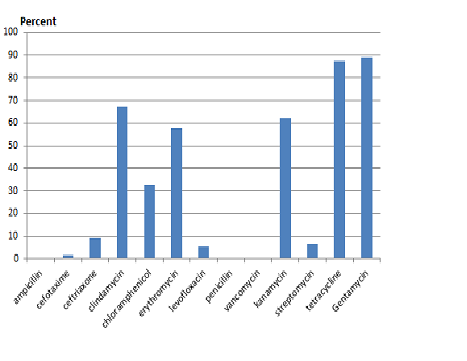 Fig. 1: Distribution of antibiotic resistant among S. agalactiae isolated from clinical samples
Fig. 1: Distribution of antibiotic resistant among S. agalactiae isolated from clinical samplesMICs of erythromycin and clindamycin were determined by for all isolates resistant or intermediate to erythromycin. The MICs of erythromycin and clindamycin 23.7% of these isolates were greater than 256 µg/ml.
Between eleven capsular antigens, serotype III (50.9%), V (27.47%), Ib (17.76%), Ia (15.54%), Ic (5.85%) were the highest. Four and ninth percent were nontypable. (Figure 2)
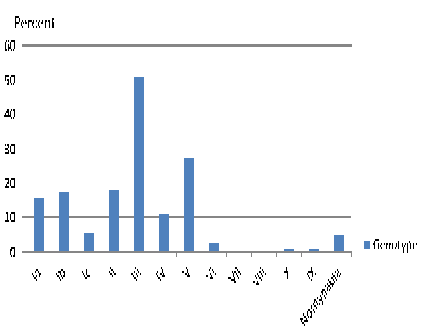 Fig. 2: Distribution of capsular genotyping among S. agalactiae isolated from clinical samples
Fig. 2: Distribution of capsular genotyping among S. agalactiae isolated from clinical samplesBased on our finding, being more than 67.1% of isolates resistant to clindamycin and almost 57.2% resistant to erythromycin, emphasis to do antimicrobial susceptibility testing for GBS strains isolated from clinical specimens. Penicillin and ampicillin were recommended by CLSI 2015 as first-line agents for intrapartum antibiotic prophylaxis. Vancomycin is drug of choices in cases for only women at high risk because of occurring anaphylaxis shock due to penicillin5
We detected 87.38% tetracycline-resistance rate among S. agalactiae isolates which was lower than other studies from Kuwait (89.5%), Iran (96%), Tunisia (97.3%) and Turkey (100%), and was more than tetracycline-resistance rate in Italy (68.1%) and Japan (46.5%). (25-30) In the current study, resistance to chloramphenicol was (32.8%), which was similar to the other study in Iran (45%), Turkey (44.2%) and Kuwait (30%). (25, 26, 28) The prevalence of drug resistance pattern in GBS can vary among ethnic groups, geographical locations, and the laboratory procedures carried out on the samples.
These data accompany with the other results are useful to define the importance of emergence and transmission of antibiotic resistance genes in GBS for supporting the decision of rational and economical program on specific antibiotics usage to treat GBS infections.
The multiplex PCR assay described in this work provides a simple tool for GBS capsular genotyping. We identified five common capsular antigens such as III (50.9%), V (27.47%), Ib (17.76%), Ia (15.54%), Ic (5.85%) were the highest, a hypothesis consistent with findings by a variety of groups6,8,11,13,20-22 The majority of isolates belonged to capsular antigens III, which is mostly involved in neonatal infections in human. The present findings, capsular antigens III is reported to be the most common GBS serotype around the world31-34 Also, we observed the capsular antigens of GBS at Ardabil, Tabriz, Kerman was different from capsular antigens of GBS reported from central Iran31, 36-39
This difference in distribution could be attributed to vary in materials and methods of research, geographical region, profile of the population being studied, and source of the bacterial isolates .Even subtle regional differences in demographic data gathering can affect GBS serodistribution within the same country.
The second capsular antigens which we identified with high level in GBS isolates was capsular antigens V. This serotype able to cause invasive infections in neonates and adolescents may be considered an emerging public health concern8,25,40,41
Other treatments for penicillin-allergic patients are clindamycin and erythromycin. Sad to say, erythromycin and clindamycin resistance have been enhanced in some countries.
All of differences related to the prevalence of genes related to antibiotic resistance may be explained by the different policies in the use of antimicrobials in different regions. The recognition of resistant strains in this study advance a proposal that these agents should be apply with precaution in the prophylaxis or remedy of GBS infection and that intermittent supervision is, therefore, needed to consider a proper therapeutic option in patients with allergy to β-lactam agents, necessary.
We conclude that GBS isolates represent various capsular antigens and resistant patterns relate to the origin of the sample, the studied population characteristics, different pattern of antibiotic consumption, and the geographical location. Dissemination and emergence of antibiotic-resistant GBS against erythromycin, tetracycline, and aminoglycoside are warning. Doing epidemiological studies and screening method for detection of MDR-GBS and appropriate drug prescriptions is recommended annually. PCR method particularly well adapted for GBS capsular antigens typing and detection of genes associated to resistance in large-scale epidemiological studies.
ACKNOWLEDGMENTS
This research has been supported by research center laboratory in school of allied medical sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran. A special thanks to Dr. Mir Davoud Omrani for all his assistance.
- Kimura, K., Nagano, N., Nagano, Y., Suzuki S.High frequency of fluoroquinolone- and macrolide-resistant streptococci among clinically isolated group B streptococci with reduced penicillin susceptibility. J. Antimicrob. Chemother., 2012; doi:10.1093/jac/dks423.
- Lu, B., Li, D., Cui, Y., Sui, W., Huang, L., Lu, X. Epidemiology of Group B streptococcus isolated from pregnant women in Beijing, China. Clin. Microbiol. Infect. 2014; 20: 370–3.
- Verani, J.R., McGee, L., Schrag, S.J. Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC). Prevention of perinatal group B streptococcal disease revised guidelines from CDC. MMWR. Recomm. Rep., 2010; 59: 1–36.
- Rodriguez-Granger, J., Alvargonzalez, J.C., Berardi, A., Berner, R., Kunze, M., Hufnagel, M., Melin, P., et al. Prevention of group B streptococcal neonatal disease revisited. Eur. J. Clin. Microbiol. Infect.Dis., 2012; 31: 2097–2104.
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty fifth Informational Supplement M100-S25. CLSI, Wayne, PA, USA, 2015.
- Slotved, H.C., Kong, F., Lambertsen, L., Sauer, S., Gilbert GL: Serotype IX, a proposed new Streptococcus agalactiae serotype. J. Clin. Microbiol., 2007; 9: 2929-36.
- Baker, C.J., Edwards, M.S. Group B streptococcal conjugate vaccines. Arch. Dis. Child., 2003; 88: 375-8.
- Dogan, B., Schukken, Y.H., Santisteban, C., Boor, K.J. Distribution of serotypes and antimicrobial resistance genes among Streptococcus agalactiae isolates from bovine and human hosts. J. Clin .Microbiol., 2005, 43: 5899-5906.
- Eschenbach, D.A .Specific Bacterial Infections: Group B Streptococcus.GLOWM 2016
- Luan, S.L., Granlund, M., Sellin, M., Lagergard, T., Spratt, B.G., Norgren, M. Multilocus sequence typing of Swedish invasive group B Streptococcus isolates indicates a neonatally associated genetic lineage and capsule switching. J. Clin. Microbiol., 2005; 43: 3727-33.
- Gherardi, G., Imperi, M., Baldassarri, L., Pataracchia, M., Alfarone, G., Recchia, S., Orefici, G., Dicuonzo, G., Creti, R. Molecular epidemiology and distribuition of serotypes, surface proteins, and antibiotic resistance among Group B streptococci in Italy. J. Clin. Microbiol., 2007; 9: 2909-16.
- Kim, E., Hans, C.S., Hans, V.N., Marcit, S.K., Helle, B.K. Emergence of invasive serotype VIII group B streptococcal infections in Denmark. J. Clin. Microbiol., 2003; 41: 4442-4.
- Dutra, V.G., Alves, V.M.N., Olendzki, A.N., Dias, C.A.G., Bastos, A.F.A., Santos, G.O., et al. Streptococcus agalactiae in Brazil: serotype distribution, virulence determinants and antimicrobial susceptibility. BMC. Infec. Dis., 2014; 14:323, DOI: 10.1186/1471-2334-14-323
- Duarte, R.S., Bellei, B.C., Miranda, O.P., Brito, M.A., Teixeira, L.M. Distribution of antimicrobial resistance and virulence-related genes among Brazilian group B streptococci recovered from bovine and human sources. Antimicrob. Agents. Chemother .,2005; 49: 97-103.
- Simões, J.A., Alves, V.M., Fracalanzza, S.E.L., Camargo, R.P., Mathias, H.M., Brolazo, E.M. Phenotypical characteristics of group B Streptococcus in parturients. Braz. J. Infect. Dis., 2007, 11: 261-6.
- Palmeiro, J.K., Dalla-Costa, L.M., Fracalanzza, S.E.L., Botelho, A.C.N., Nogueira, K.S., Scheffer, M.C., et al. Phenotypic and genotypic characterization of group B streptococcal isolates in southern Brazil. J. Clin. Microbiol., 2010; 12: 4397-4403.
- Corrêa, A.B.A., Silva, G.L., Pinto, T.C.A., Oliveira, I.C.M., Fernandes, F.G., Costa, N.S., et al.The genetic diversity and phenotypic characterisation of Streptococcus agalactiae isolates from Rio de Janeiro, Brazil. Mem. Inst .Oswaldo .Cruz ., 2011, 106: 1002-6.
- Pinto, T.C.A., Costa, N.S., Souza, A.R.V., Silva, L.G., Corrêa, A.B.A., Fernandes, F.G., et al. Distribution of serotypes and evaluation of antimicrobial susceptibility among humam and bovine Streptococcus agalactiae strains isolated in Brazil between 1980 and 2006. Braz. J .Infect Dis., 2013, 17: 131-6.
- Verani, J.R., McGee, L., Schrag, S.J. Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC). Prevention of perinatal group B streptococcal disease revised guidelines from CDC 2010. MMWR. Recomm .Rep .,2010; 59: 1–36.
- Poyart, C., Tazi, A, Reglier-Poupet, H., et al. Multiplex PCR assay for rapid and accurate capsular typing of group B streptococci. J. Clin. Microbiol.2007; 45: 1985–1988.
- Imperi, M., Pataracchia, M., Alfarone, G., Baldassarri, L., Orefici, G., Creti, R. A multiplex PCR assay for the direct identification of the capsular type (Ia to IX) of Streptococcus agalactiae. J .Microbiol .Methods., 2010; 80: 212–4.
- Yao, K., Poulsen, K., Maione, D. et al. Capsular gene typing of Streptococcus agalactiae compared to serotyping by latex agglutination. J. Clin .Microbiol., 2013; 51: 503–7.
- Nagano, N., Nagano,Y., Toyama, M., Kimura, K., Tamura,T., Shibayama, K. , et al.Nosocomial spread of multidrug-resistant group B streptococci with reduced penicillin susceptibility belonging to clonal complex. J. Antimicrob. Chemother., 2011; doi:10.1093/jac/dkr546
- Khan, I.U., Hassan, A.A., Abdulmawjood, A., Lämmler, C., Wolter, W., Zschöck, M. Identification and epidemiological characterization of Streptococcus uberis isolated from bovine mastitis using conventional and molecular methods. J. Vet. Sci., 2003; 4(3): 213-24.
- Boswihi, S.S., Udo, E.E., Al-Sweih, N.Serotypes and Antibiotic Resistance in Group B Streptococcus Isolated from Patients at the Maternity Hospital, Kuwait. J .Med .Microbiol .,2012; 6: 126–131.
- Emaneini, M., Mirsalehian, A., Beigvierdi, R., Imani Fooladi, A.A., Asadi, F., Jabalameli, F., Taherikalani ,M. High Incidence of Macrolide and Tetracycline Resistance among Streptococcus agalactiae Strains Isolated from Clinical Samples in Tehran, Iran. J. Clin. Med .,2014; 9(2): 157-61.
- Hraoui, M., Boutiba-Ben Boubaker, I., Rachdi, M., Slim, A., Ben Redjeb, S. Macrolide and tetracycline resistance in clinical strains of Streptococcus agalactiae isolated in Tunisia. J. Med. Microbial .,2012; 61:1109-13.
- Acikgoz, Z.C., Almayanlar ,E., Gamberzade, S., Gocer, S .Macrolide resistance determinants of invasive and noninvasive group B Streptococci in a Turkish hospital. Antimicrob. Agents .Chemother., 2004; 48(4):1410-2.
- Gherardi, G., Imperi, M., Baldassarri, L., Pataracchia, M., Alfarone, G., Recchia, S.,et al. Molecular epidemiology and distribution of serotypes, surface proteins, and antibiotic resistance among group B Streptococci in Italy. J .Clin. Microbiol., 2007; 45(9):2909-16.
- Ueno, H., Yamamoto, Y., Yamamichi, A., Kikuchi, K., Kobori, S., Miyazaki, M.Characterization of group B Streptococcus isolated from women in Saitama city, Japan. Jpn. J. Infect .Dis .,2012; 65(6):516-21.
- Mansouri, S., Ghasami, E. , Shahabi Najad, N. Vaginal Colonization of Group B Streptococci During Late Pregnancy in Southeast of Iran: Incidence, Serotype Distribution and Susceptibility to Antibiotics. J. Med. Sci., 2008; 8: 574-578.
- Barcaite, E., Bartusevicius, A., Tameliene ,R., Kliucinskas, M. , Maleckiene, L., et al. Prevalence of maternal group B Streptococcal colonisation in European countries. Acta .Obstet. Gynecol. Scand .,2008; 87: 260-71.
- Motlova, J., Strakova, L., Urbaskova, P., Sak, P. , Sever, T. Vaginal and rectal carriage of Streptococcus agalactiae in the Czech Republic: Incidence, serotypes distribution and susceptibility to antibiotics. Indian. J. Med. Res., 2004; 119: 84-87.
- Uh, Y., Jang, I.H., Hwang, G.Y., Lee, M.K. , Yoon, K.J. ,et al. Serotypes and genotypes of erythromycin-resistant group B streptococci in Korea. J. Clin. Microbiol., 2004; 42: 3306-8.
- Savoia, D. , Gottimer, C., Crocilla, C., Zucca, M. Streptococcus agalactiae in pregnant women: Phenotypic and genotypic characters. J. Infect .,2008; 56: 120-5.
- Jannati, E., Roshani, M., Arzanlou, M., Habibzadeh, S. , Rahimi, G . , Shapuri, R .Capsular serotype and antibiotic resistance of group B streptococci isolated from pregnant women in Ardabil, Iran. Iran. J .Microbiol .,2012; 4(3): 130-135.
- Ippolito, D.L., James, W.A., Tinnemore, D., Huang, R.R., Dehart, M.J., Williams, J., et al. Group B streptococcus serotype prevalence in reproductive-age women at a tertiary care military medical center relative to global serotype distribution. BMC .Infect .Dis .,2010; 10: 336.
- Dhanoa ,A.,Karunakaran, R., Puthucheary, S.D. Serotype distribution and antibiotic susceptibility of group B streptococci in pregnant women. Epidemiol. Infect., 2010; 138: 979-981.
- Nahaei, M.R., Ghandchilar, N., Bilan, N., Ghahramani, P. Maternal carriage and neonatal colonization of Streptococcus agalactiae in Tabriz, Northwest Iran. Iranian. J .Med .Sciences 2007; 32: 177-181.
- Castor, M.L., Whitney, C.G., Como-Sabetti, K. , Facklam, R.R., Ferrieri, P., Bartkus, J.M., et al. Antibiotic resistance patterns in invasive group B streptococcal isolates. Infect. Dis. Obstet .Gynecol., 2008; http://dx.doi.org/10.1155/2008/727505
- Zhao, Z., Kong, F., Zeng, X. , Gidding, H.F. , Morgan, J., Gilbert, G.L. Distribution of genotypes and antibiotic resistance genes among invasive Streptococcus agalactiae (group B streptococcus) isolates from Australasian patients belonging to different age groups. Clin. Microbiol .Infect .,2008; 14: 260–7.
© The Author(s) 2017. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.