

ISSN: 0973-7510
E-ISSN: 2581-690X
Urinary tract infections (UTI) are the most common bacterial infections among women in both pregnant and non pregnant states, among which asymptomatic bacteriuria is the commonest .Symptomatic bacteriuria includes cystitis and pyelonephritis. UTI is a disease of multiple etiology and is known for its recurrence despite the treatment. Every woman has a 20% life time risk of developing UTI. A sincere effort has been put to understand the local epidemiology of the organism and its susceptibility pattern so as to initiate an effective treatment. 1. To study the bacterial isolates of Urinary tract infection in pregnant women. 2. To study the antibiogram of the bacterial isolates. The study was conducted among 100 pregnant women who attended Obstetrics and Gynecology (OBG) outpatient department at a tertiary care centre, Bangalore, India, over a period of six months. For isolating the bacteria, standard conventional method of isolation and identification was followed. Antibiotic susceptibility of the isolates were determined using Kirby Bauer disk diffusion method. The data was analyzed using standard statistical package. Majority of the isolates were Escherichia coli (33.98%) followed by Klebsiella species (19.41%), Coagulase negative staphylococcus (16.50%) and Enterococcus fecalis (13.59%), Acinetobacter species (7.76%), Staphylococcus aureus (3.88%), Pseudomonas and Enterobacter species were 1.9% each. Proteus being the least(0.97%). The isolates were sensitive to Aminoglycosides (97.08%) and Nitrofurantoin (97.08%). The study suggests that the common etiological agent for UTI in pregnant women was Escherichia coli and was sensitive to Aminoglycosides and Nitrofurantoin.
Urinary tract infection, Pregnant women, Bacterial isolates, Antibiotic susceptibility.
Urinary tract infections (UTI’s) are the most common bacterial infections in women, in both the pregnant and non-pregnant states among which the asymptomatic bacteriuria (ASB) is most common. Symptomatic infection includes cystitis and pyelonephritis.1
The outer one-third of the female urethra, the urinary tract is normally sterile. Urinary tract infection includes both asymptomatic microbial colonization of the urine and symptomatic infection.2. Colony counts of >105/mL of mid-stream clean catch urine sample refers to significant bacteriuria3.
Urinary tract infections can be unresolved bacteriuria during the drug therapy, recurrent urinary infections which can be reinfection or relapse.4 The disease is exceeded in frequency among ambulatory patients by respiratory and gastrointestinal infections 4. Every woman has a 20% life time risk of coming down with a UTI. In children approximately 5% of girls and 1% of boys have a UTI by 11 years of age. 6,7
Asymptomatic Bacteriuria (ASB) is a state in which the patient has no symptoms of a UTI but a culture of a ‘clean catch’ midstream sample of urine reveals 1,00,000 colonies or more in per millilitre of urine of a single organism in two consecutive urine samples 8. And it affects 2-10% of pregnancies. It may be wiser to treat even when the colony count is lesser, as pyelonephritis can develop in women with lesser concentrations. It is important to diagnose and treat this condition, as symptomatic UTI will develop in nearly 40% of the cases and pyelonephritis will develop in 30% of untreated asymptomatic patients with bacteriuria 9. ASB is also associated with preterm labour and Foetal growth retardation(FGR)10. Recognition and therapy can eliminate 70% of acute UTls in pregnancy. The most common aetiological agent of the UTIs is Escherichia coli which usually responds to broad-spectrum antibiotics such as Aminoglycosides and Cephalosporins. In cases of suppression of bacterial persistence or recurrence Nitrofurantoin, 100 mg at bedtime for rest of pregnancy is the choice.11
Cystitis and Urethritis may occur. Cystitis is characterized by dysuria, urgency and frequency. Some women may have systemic findings, pyuria, bacteriuria and microscopic haematuria. Occasionally, there may be gross haematuria from hemorrhagic cystitis. With prompt treatment, cystitis may resolve without complications but in undiagnosed or untreated cases, the upper urinary tract may get involved in ascending infection 12Pyelonephritis is a condition characterized by an inflammation of the renal parenchyma and the collecting system (renal calyces and pelvis) within the kidney. It is generally seen in 1-2% of pregnancies. UTIs are not uncommon during pregnancy. ASB affects about 8% of pregnancies. If left untreated, it leads to symptomatic disease in more than a third of the affected individuals. Pathogens from the vagina and rectum ascends9,11 . E. coli is the principal offending organism. Others include Klebsiella, Pseudomonas, Enterococcus 8,13. Mechanical obstruction includes (i) ureteropelvic junction, (ii) ureteral urethral stenosis and (iii) calculi. Functional obstruction includes (i) pregnancy (progesterone induces relaxation of smooth muscle walls of the pelvicalyceal and ureteric systems, and reduces peristaltic activity) and (ii) vesicoureteral reflux. UTIs left unattended can predispose to preterm labour, enhanced adverse perinatal outcome, gram-negative septicaemia and disseminated vascular coagulation. Risk factors for UTIs in pregnancy include diabetes mellitus, sickle cell disease and vesicourethral reflex. 13,14.
Objectives
- To study the bacterial isolates in pregnant women with UTI.
- To study the antibiotic susceptibility pattern of the isolates.
The present study was done at a tertiary care centre, Bangalore, India for a period of 6months .A total of 100 patients who attended OBG OPD’s during the period were included in the study.The mid- stream clean catch urine sample was collected under aseptic precautions in a sterile wide mouthed screw capped container. These specimens were subjected to wet mount to look for pus cells and organisms. The urine samples were streaked onto Blood agar, Cystiene-Lactose-Electrolyte defecient agar and Mac conkey agar by a wire loop that can deliver 0.001ml of urine sample. Plates were then incubated at 370C and checked for significant bacteriuria by estimating the colony count by Kass concept. The isolates were identified by colony morphology and standard biochemical tests. Antibiotic susceptibility testing of the isolates was done by Kirby Bauer disc diffusion guidelines.6
For Antibiogram testing,the antibiotics used were Amikacin (30mcg), Ceftazidime (30mcg), Cefepime, Cefuroxime (30mcg), Cotrimoxazole, Amoxiclave (20/10mcg), Gentamicin (10mcg), Nalidixicacid (30mcg), Nitrofurantoin (100mcg), Piperacillin Tazobactam (100/10mcg), Ciprofloxacin (5mcg), Cefoxitin (30mcg)
Statistical analysis:The data collected was entered onto Microsoft excel.It was analyzed using standard statistical package for descriptive statistics and chi-square test was done with P value<0.05 was set as level as significance.
Culture Positive Vs Culture Negative
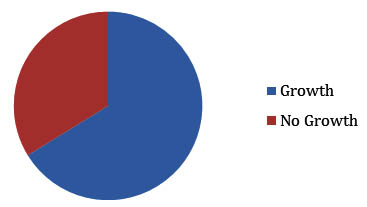
Fig. 1. Of the 100 cases examined for UTI,66.22% yielded growth and 33.78% showed no growth in culture
Culture Report
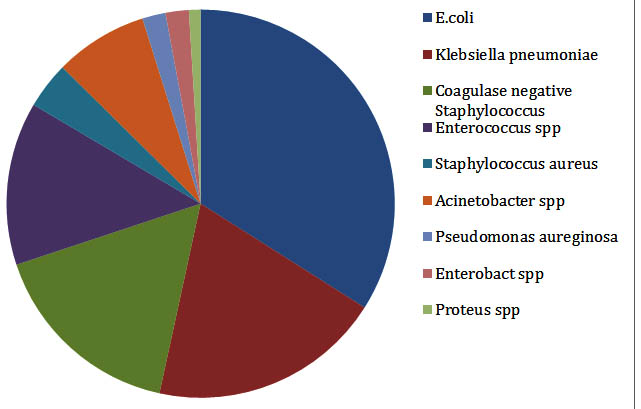
Fig. 2. Of the 103 isolates,68 isolates were gram negative organisms, among which E.coli predominated 33.98%,Klebsiellae pneumonia 19.41%, Acinetobacter species 7.76%, Pseudomonas aeruginosa and Enterobacter species with 1.94% and Proteus 0.97%.Of the gram positive organisms Coagulase negative staphylococcus showed 16.50%,Enterococcus fecalis 13.59% and Staphylococcus aureus 3.88%.Of the 4 isolates of Staphylococcus aureus none were MRSA
Antibiogram of the isolates
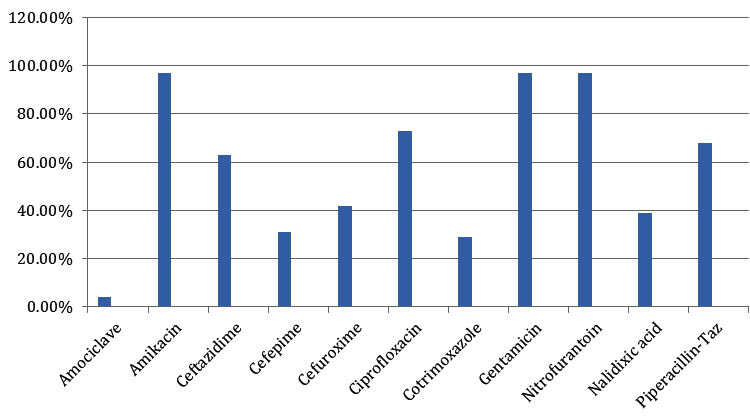
Fig. 3. Antibiotics susceptibility pattern was as follows. The isolates were highly susceptible to Amikacin, Gentamicin and Nitrofurantoin (97.08%), followed by Ciprofloxacin(72.81%), Piperacillin-tazobactam(67.96%), Ceftazidime(63.10%), Cefuroxime(41.74%), Nalidixic acid(38.83%), Cefepime(31.06%), Cotrimoxazole(29.1%), Amoxyclave(3.88%)
The incidence of bacteria isolated is 66.22% which has been reported to be only 8-16 % in western literature. Antibiotic prophylactic protocol recommendation by American Urological Association (AUA) and European Association of Urology(EAU) may not be relevant in indian population.4,7
Korets R et al and Dajani and Shehabi et al has reported the culture positives were 16% were as in the present study it was much higher ,66.22%.12,14.In similar study Escherichia coli was the most commonest organism isolated which coincides with the present study.Among the gram positive isolates Coagulase negative Staphylococcus was the commonest coincides with the study byDajani and Shehabi et al 14
The majority of etiological agents of UTI in the present study were gram negative bacilli.Similar findings were seen in the study by Shazia PS et al 9
According to Janifer J et al,the incidence of Enterococcus species were higher but in this study it was not so.This could be due to the use of MacConkey agar which is a selective medium for Gram negative organisms 8
Aminoglycosides and Nitofurantoin still remains the drugs effective in the treatment of UTI ,similar to Assefa A et al 11
The short female urethra and its close proximity to the vagina coupled with poor sanitary practices are responsible for the easy access of bacteria to the female urinary tract. Repeated catheterization to relieve retention either during pregnancy or during labour and puerperium commonly leads to urinary infection and pyelonephritis. The changes occurring in the kidney and the urinary tract during pregnancy are major factors in precipitating pyelonephritis and UTI 2,3. Progesterone mediated laxity in the smooth muscles of the collecting system enables its dilatation and thereby facilitating a reflux of urine up the ureters. The pressure exerted by the gravid uterus on the ureters impedes urine flow, thereby causing stasis of urine and sluggishness of urine flow. Aggravating factors are blood borne, lymphatic, direct infection. These changes are responsible for providing an ideal environment for bacterial growth and hence an enhanced frequency of this infection in pregnancy7,8, Pyelonephritis is seen more in primi gravidae. Previous History is seen in almost 50% of the cases. Abnormal tract is present in 25 percent of the cases and ASB is the cause in the remaining 25 percent. Pyelonephritis is usually preceded by either ASB or lower UTI (cystitis 0r urethritis). Stasis of urine will encourage multiplication of bacteria. Influx of infected urine into ureters and renal pelvis occurs due to laxity of vesicoureteric sphincters. Infection from renal pelvis spreads to parenchyma and depending on severity either suppurative pyelonephritis or perinephric abscess will develop. The most common aetiological agent (70-80%) is E. coli; Enterobacter Proteus species, Staphylococcus aureus, Klebsiellae pneumoniae, Pseudomonas are the other organisms.12,13,14. Endotoxins damage the alveoli and result in pulmonary oedema. Patients with pyelonephritis may have varying degrees of respiratory insufficiency. The patients usually present with systemic and local symptoms. The symptomatic manifestations are usually fever, malaise, nausea, vomiting and urgency of micturition along with tenderness at the renal angle on the affected side. In cases of cystitis, accompanying suprapubic discomfort may also be present. Clinical types include Acute (severe) and Chronic (mild). Pyelonephritis symptoms include onset is acute, usually appears after 16 weeks initiation of pregnancy. All patients must be screened for ASB, which if discovered must be appropriately treated. In established cases of infection, the following investigations are performed. Urine: The urinary sediment contains many leukocytes frequently in clumps and numerous bacteria, Urine for culture and antibiotic sensitivity, Hb (will be low), differential and total WB’C counts 5 leukocytosis), C-reactive protein will be high, Blood culture (bacteraemia present in 15-20%) . Renal function tests (shows high urea and creatinine)3. Effect on pregnancy include abortions, FGR, Preterm labour and IUFD. Symptomatic cases of infection are admitted to the hospital for intravenous fluids and antibiotic therapy. Following are the guidelines of management: Complete bed rest, Intravenous fluids, Intravenous antibiotics for the first 48 h. Patients are started empirically on cephalosporins. Later it may be changed when the antibiotic sensitivity is received. If aminonoglycosides are administered, it is very important to establish the renal function status and to titrate the dose accordingly. Antipyretics should be given. The treatment should be continued with oral antibiotics for at least 2 weeks to ensure eradication of the bacteria from the system. Criteria for cure is 3 consecutive weekly urines cultures are sterile. Complications includes, septicaemia, Adult respiratory distress syndrome, Renal abscess and scarring, which may lead to loss of renal function in the affected kidney in severe cases, Preterm labour and delivery, Increased perinatal morbidity and mortality, Disseminated intravascular coagulation (DIC).1,3,15
There is a higher than initially reported incidence of bacteria (66.22%) in patients who never had any evidence of Urinary tract infection. The common etiological agent was found to be Gram negative bacilli-Escherichia coli.Among the gram positive isolates majority was Coagulase negative staphylococcus.Most were highly sensitive to Aminoglycosides and Nitrofurantoin.
Follow-up includes, Urine cultures must be performed monthly to detect relapses, which can then be appropriately treated. Long-term antibiotic suppression is often advised. Frequent relapses may mandate an intravenous urogram which can be performed only after the delivery in the puerperium. Reevaluation should be done 4 months after delivery. Chronic Pyelonephritis may be because of chronic process from the beginning or due to sequelae of acute UTI. ASB may be a resting stage. Diagnosis is difficult, as pus cells may be absent. Chronic hypertension and anaemia may be a consequence. Usually nitrofurantoin 100 mg twice daily may be continued for longer periods
- Bailey RR. Urinary Tract Infection. In: Oxford Textbook of Medicine on CD-ROM. Oxford University Press and Electronic Publishing B. V; 1996 Section 20.8.1
- Calvin M. Cunin. Urinary Tract Infections and Pyelonephritis. In: Goldman E. editor. Cecil Textbook of Medicine 21st edition. W. B. Saunders Company; 2000. p. 138
- Stamm EW. Urinary Tract Infections and Pyelonephritis. In: Harrison’s Principles of Internal Medicine 15th Edition on CD-ROM. Mc-Graw and Hill Companies Inc; 2001
- Levi ME, Redington J Barth L. The Patient With Urinary Tract Infection. In: Schrier RW editor. Manual of Nephrology, 6th Edition. Lippincott Williams & Wilkins, 2005.
- David Howes. Urinary Tract Infection. eMedicine April 25 2005 (online).
- Miles RS,Amyes SGB.Laboratory control of antimicrobial therapy.p.151-78.In Collee JG,Fraser AG,Marmion BP,Simmons A.Mackie and Mc Cartney practical medical microbiology.14th ed.Delhi:Elsevier,2008.
- Ozumba UC. Increasing incidence of bacterial, resistance to antibiotics by isolates from the urinary tract. Niger J Clin Pract. 2005; 8(2):107-9.
- Janifer J,Geethalakshmi S,Satyavam K.Prevalence of Lower urinary tract infection in South India. Indian Journal of Nephrology. 2009; 19(3):107
- Shazia PS,Sharada VR,Rama RMV,Janardhan RR.Uropathogens and their drug susceptibility patterns among pregnant women in a tertiary hospital. Ann Biol Res. 2011; 2(5);516-521.
- Jenson BH, Baltimore RS. Infectious Diseases.In: Kleigman RM, Marcdante KJ, Jenson BH, Berhman RE editors. Nelson Essentials of Paediatrics 5th edition. Philadelphia: Elsevier Inc; 2006. p. 522.
- Assefa A,Asrat D,WolderamanuelY,Abdulla A.Bacterial profile and drug susceptibility pattern of urinary tract infection in pregnant women. Etiop Med J. 2008; 46(3):227-235.
- Korets R et al Risk Factors of Infectious Complications after Flexible Ureterorenoscopy with laser lithotripsy J Urol. 2011; 186:1899–1903.
- Gault MH, Longerich LL, Crane G, et al. Bacteriology of urinary tract stones. J Urol. 1995; 153:1164 1170.
- Dajani AM, Shehabi AA (1983) Bacteriology and composition of infected stones. Urology 21: 351–353
- Park K.Infectious disease.In:Park K,Bankot B,editors.Parks Text Book of Preventive and Social Medicine.18th ed.Jabalpur.Banarsidas Bhanot Publications; 2005.pp311-315.
© The Author(s) 2018. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.