


ISSN: 0973-7510
E-ISSN: 2581-690X
Improper waste management practices are a serious problem that involves not only the hospital staff but society at large. To improve biomedical waste (BMW) management, it is important to evaluate the current practices in BMW management (BMWM), identify the gaps, and address them. With this backdrop, this research was done to assess the awareness of BMW management practices among the healthcare professionals in a teaching hospital. This is a hospital-based observational study with assessment of 112 doctors, 230 nurses, and 158 waste handlers. The healthcare workers (HCW) were evaluated regarding awareness, and different practices of BMWM with a self-structured questionnaire. An overall score of ≥50% in each section was considered satisfactory regarding awareness and practices for BMWM. Data were analyzed statistically using SPSS Ver.21 software. Regarding the awareness on various aspects of BMWM, doctors had maximum level of awareness at 68.6% (60.0% – 77.2%), followed by nurses at 69.3% (63.3%-75.3%) and waste handlers at 55.9% (48.2% – 63.6%). Overall nurses showed maximum awareness of existing practices at 74.0% followed by doctors at 70.2% and waste handlers were at 53.8%. To optimize BMWM, it is important to raise awareness on best practices while evaluating the current practices. Gaps in knowledge and skills need to be identified and closed. Ongoing information, education and communication for health care professionals are pivotal in improving BMWM practices.
Biomedical waste (BMW), Biomedical waste management (BMWM), Biomedical waste team, Infection Control, Healthcare workers (HCW)
Biomedical waste is the waste that is generated during investigation, treatment, or vaccination of humans or animals, or that is produced during manufacture or testing of biologicals.1 For this study it applied to the above and covers the Biomedical waste (BMW) as described in schedule – 1 of the government of India rules, 1998. About 85% of waste generation in relation to health related activities is non hazardous. The remaining 15% of waste generated out of healthcare activities is considered hazardous. These hazardous material might be infectious, toxic, or radioactive and have potential to cause injury.2 Although, the quantity of the infectious waste produced is less as compared to the overall healthcare waste, the poor waste management practices by healthcare workers lead to the mixing of the infectious waste with non-infectious waste and thereby contaminating the whole waste.3 BMW waste production increased manifold during the Covid pandemic which further compounded the situation.4
Improper disposal of BMW has many adverse and harmful effects on the environment & human health.5 High risk activities like the reuse of syringes and multi-dose vials augments the chances of blood borne diseases manyfold.6 Needles used by drug abusers lead to further spread of infection.7 Repacking of used needles/cotton etc. can be done by unscrupulous elements. Air pollution due to incineration of improperly segregated waste produces toxic gases while water pollution is a problem due to improper liquid waste management.8 Increasing antibiotic resistance is a potential threat due to the spread of resistant strains.9
Any carelessness in the management of waste generated in a hospital tends to spread infections and contaminate the entire environment. Thus, improper waste management practices are a serious problem that involves not only the hospital staff but society at large. However, in developing countries, biomedical waste management (BMWM) have not received sufficient attention and hence it remains a major biosafety threat.10
There are numerous myths and misperceptions regarding BMWM among healthcare professionals, health administrators and the public. Lack of awareness, non- ownership, unstructured training, and lax implementation are the factors largely influencing poor BMWM in India. To improve BMWM, it is important to assess current awareness on proper BMWM. It is imperative to understand and evaluate the current practices in BMWM with gap analysis.11 With this backdrop, this research was done to assess the awareness regarding BMWM practices among the healthcare personnel in a teaching hospital. Further, suitable recommendations to improve BMW practices among healthcare personnel based on study findings were given.
The objectives of this study were to evaluate the level of awareness and existing practices regarding BMWM amongst the HCW. The study compared the level of awareness of BMWM among doctors, nursing staff, and waste handlers. Existing practices of BMWM among doctors, nursing staff, and waste handlers was also compared. Reasons behind inadequate BMWM were evaluated with a thorough assessment of the gaps in knowledge and practices among the HCWs.
A hospital-based observational study was conducted at Career Institute of Medical Sciences and Hospital, Lucknow from October to December 2019. Ethical clearance was taken from the Institutional Ethical committee to conduct the study. Using the purposive sampling method, 500 Health Care Workers (HCWs) dealing with BMW were included for the study comprising 112 doctors, 230 nurses, and 158 waste handlers. Study groups were based on their designation as faculty, junior/senior residents, medical interns, nurses, and waste handlers. Informed consent was taken from the health care workers after explaining to them the purpose of the study. Confidentiality of the participants and data was maintained.
Our hospital has a BMWM Team that regularly conducts training programs on BMWM. The HCW were evaluated regarding awareness, and practices of biomedical waste management via a self-structured questionnaire. Question set was designed in English and then modified to the local language (Hindi) to make it easily understandable across all the classes of HCP. The questionnaire comprised twenty close-ended questions and was divided into two sections. The first section consisted of ten questions of one mark each and assessed the awareness regarding BMWM. The second section consisting of 10 questions included questions related to practical implications and practices. An overall score of ≥ 50% in each section was considered as the satisfactory score on awareness and practices for BMWM.
Data were analyzed statistically using SPSS Ver.21 software. Chi-square test was undertaken to find association between the HCP groups regarding their knowledge and practices towards BMWM. The p value was applied on the generated data.
A total of 500 HCWs participated in our study. Out of the 500, 112 (22.4%) were doctors, 230 (46%) were nurses and 158 (31.6%) were waste handlers. A total of 77.8% of healthcare personnel had received training on BMWM (Table 1).
Table (1):
Health care workers who underwent BMWM Training.
HCW category (n=500) |
HCW those who underwent training |
|---|---|
Doctors (112) |
89 (79.4%) |
Nurses (230) |
191 (83%) |
Waste handlers (158) |
109 (68.9%) |
Total |
389 (77.8%) |
Analyzing the awareness about various aspects of BMWM, doctors had maximum level of awareness at68.6% (60.0% – 77.2%), followed by nurses at 69.3% (63.3%-75.3%) and waste handlers at 55.9% (48.2% – 63.6%) (Table 2, Fig. 1).
Table (2):
BMWM awareness among health care personnel.
| Awareness of Bio Medical Waste Management as per 2016 guidelines. | Satisfactory Awareness | chi sq | p-value | |||
|---|---|---|---|---|---|---|
| Doctors (N=112) | Nurses (N=230) | Waste Handlers (N=158) | ||||
| A1 | Salient guidelines of BMWM Rules | 80 (71.4%) | 164 (71.3%) | 101 (63.9%) | 2.78 | 0.249 |
| A2 | Significance of Biohazard Symbol | 82 (73.2%) | 170 (73.9%) | 96 (60.8%) | 8.55 | 0.014 |
| A3 | Percentage of Infectious waste among total waste in hospital | 71 (63.4%) | 144 (62.6%) | 76 (48.1%) | 9.70 | 0.008 |
| A4 | Hazards associated with improper BMWM | 88 (78.6%) | 167 (72.6%) | 102 (64.6%) | 6.61 | 0.037 |
| A5 | Description of PPE while handling BMW | 74 (66.1%) | 149 (64.8%) | 104 (65.8%) | 0.07 | 0.964 |
| A6 | Segregation of BMW at Source | 79 (70.5%) | 158 (68.7 %) | 82 (51.9%) | 14.30 | 0.001 |
| A7 | Color coding of BMW as per 2016 guidelines | 75 (67.0%) | 169 (73.5%) | 73 (46.2%) | 30.80 | <0.001 |
| A8 | Storage of BMW beyond 48 hours | 82 (73.2%) | 162 (70.4%) | 87 (55.1%) | 13.10 | 0.001 |
| A9 | Transportation rules including GPS system in BMW Vehicles | 62 (55.4%) | 146 (63.5%) | 67 (42.4%) | 16.80 | <0.001 |
| A10 | Proper final disposal of waste | 75 (67.0%) | 164 (71.3%) | 96 (60.8%) | 4.71 | 0.095 |
| Overall awareness | 68.6% (60.0%-77.2%) |
69.3% (63.3%-75.3%) |
55.9% (48.2%-63.6%) |
|||
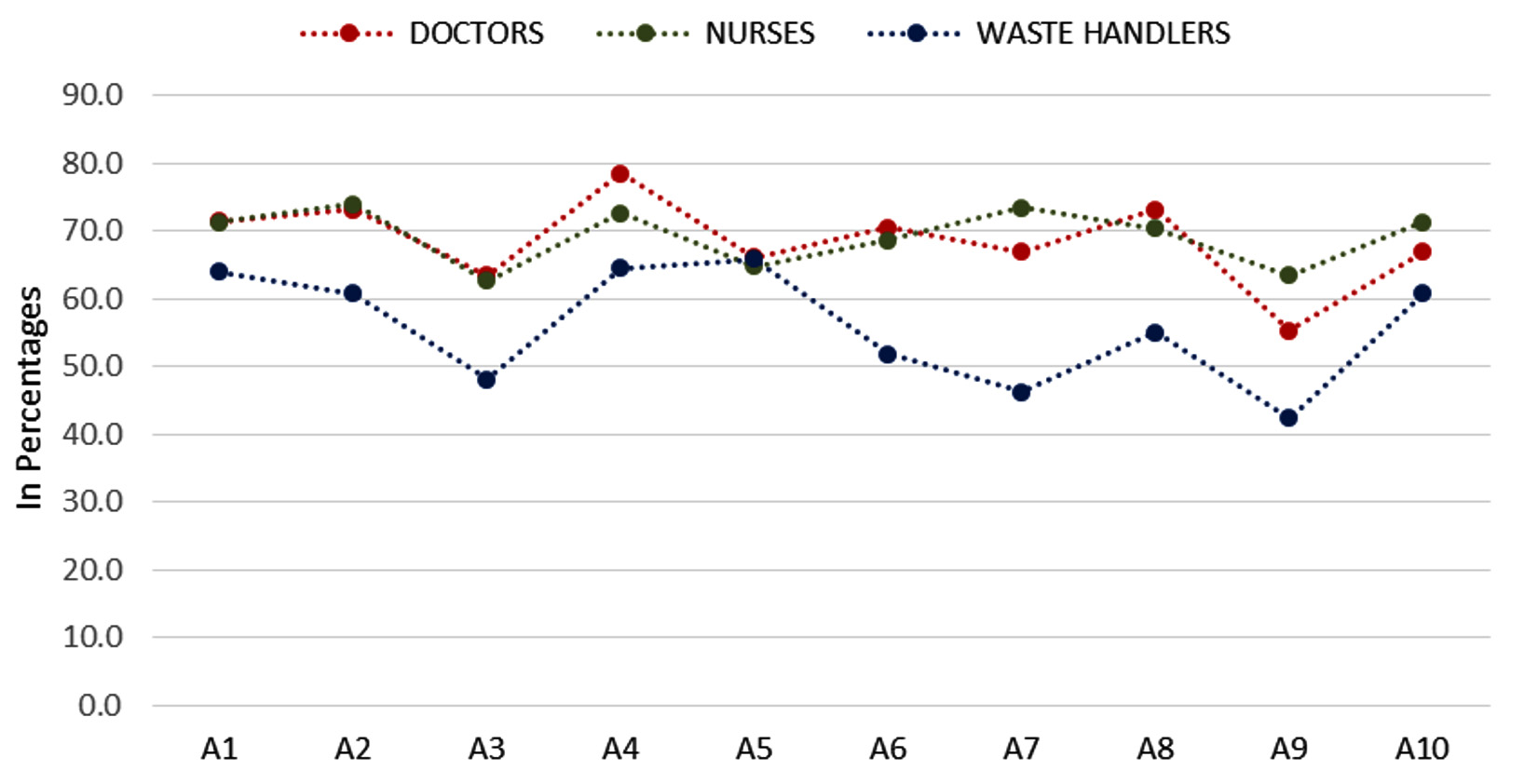
Fig. 1. Level of BMWM awareness among health care personnel.
The difference in level awareness among doctors, nurses, and waste handlers about various aspects of BMWM was found statistically significant with a p-value <0.05 (Table 2).
Overall nurses showed maximum adequacy level of existing practices at 74.0% followed by doctors at 70.2% and waste handlers at 53.8% (Table 3, Fig. 2).
Table (3):
BMWM awareness of existing practices among healthcare personnel.
| Assessment of BMWM Practices as per 2016 guidelines | Satisfactory Practices | chi sq | p-value | |||
|---|---|---|---|---|---|---|
| Doctors (112) | Nurses (230) |
Waste Handlers (158) | ||||
| P1 | Method for segregating collecting human anatomical waste | 71 (63.4%) | 180 (78.3%) | 91 (57.6%) | 20.2 | <0.001 |
| P2 | Method for segregating contaminated linen, casts, cotton gauze | 72 (64.3%) | 166 (72.2%) | 98 (62.0%) | 4.93 | 0.085 |
| P3 | Method for segregating infected plastic wastes | 79 (70.5%) | 195 (84.8%) | 87 (55.1%) | 41.4 | <0.001 |
| P4 | Method for segregating general wastes | 86 (76.8%) | 182 (79.1%) | 111 (70.3%) | 4.1 | 0.129 |
| P5 | Method for segregating metallic sharp wastes | 81 (72.3%) | 177 (77.0%) | 89 (56.3%) | 19.3 | <0.001 |
| P6 | Method for discarding infectious liquid waste | 76 (67.9%) | 161 (70.0%) | 78 (49.4%) | 18.6 | <0.001 |
| P7 | Method for discarding used disposable needles/ Use of Needle Cutter | 88 (78.6%) | 171 (74.3%) | 77 (48.7%) | 36.3 | <0.001 |
| P8 | How to dispose Intact or broken glassware | 77 (68.8%) | 167 (72.6%) | 76 (48.1%) | 25.8 | <0.001 |
| P9 | Practices of reporting of injuries resulting from improperly disposed biomedical waste | 77 (68.8%) | 148 (64.3%) | 62 (39.2%) | 31.7 | <0.001 |
| P10 | Correct management of Spills | 79 (70.5%) | 156 (67.8%) | 81 (51.3%) | 14.4 | 0.001 |
| Overall (Average) Satisfactory Practices | 70.2% (61.7% – 78.7%) | 74% (68.3% – 79.7%) | 53.8% (46.0% – 61.6%) | |||
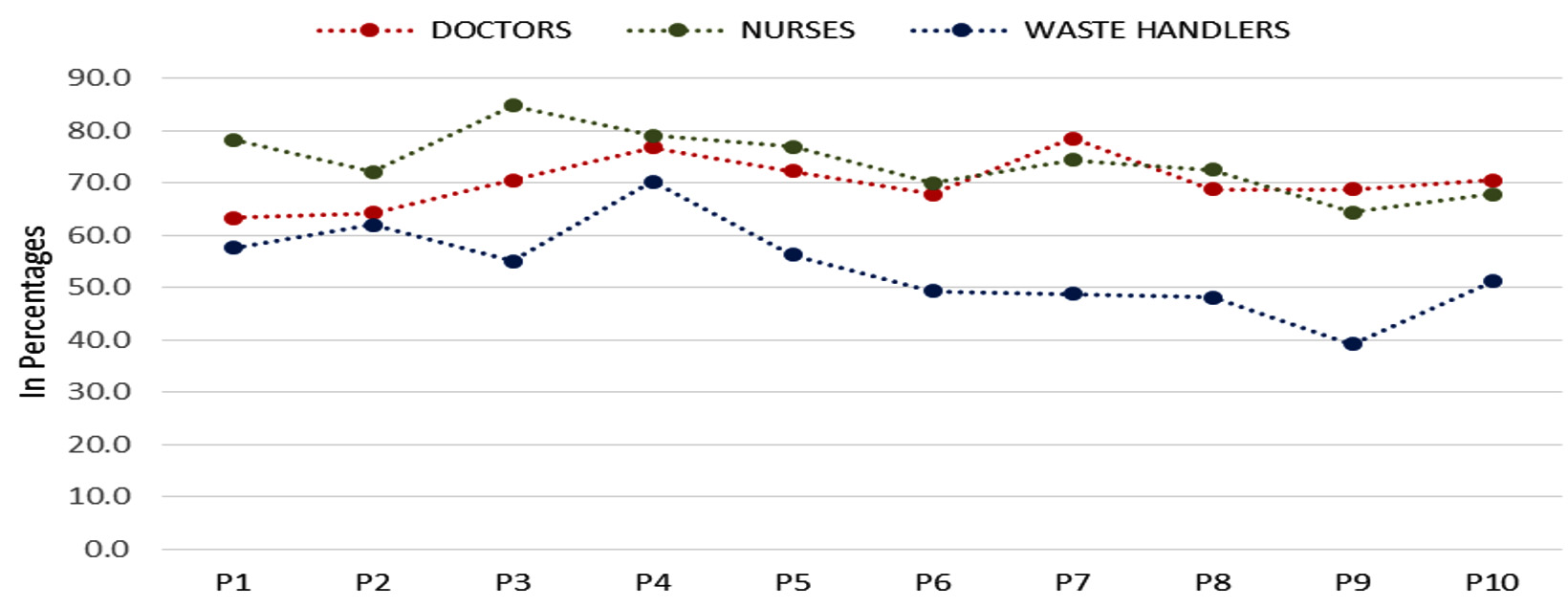
Fig. 2. BMWM adequacy of existing practices among healthcare personnel.
On comparing the existing practices among doctors, nurses, and waste handlers, the significant difference in the level of existing practices was found for all the aspects except entities like methods for segregating infective non-plastic waste (p=0.085) and method for segregating general wastes (p=0.129).
Faculties showed the maximum level of awareness at 83.4% and interns showed the minimum level of awareness at 52.0% (Table 4, Fig. 3). On comparing the awareness among faculty, residents, and interns, the significant difference in awareness was found in various aspects.
Table (4):
Level of awareness regarding BMWM among faculty, residents and interns.
Questionnaire |
Faculty (38) |
Senior residents (23) |
Junior residents (26) |
Interns (25) |
Total (112) |
chi sq |
p-value |
|
|---|---|---|---|---|---|---|---|---|
A1 |
Salient guidelines of BMWM Rules |
34 (89.5%) |
17 (73.9%) |
21 (80.8%) |
19 (76.0%) |
91 (81.3%) |
2.96 |
0.398 |
A2 |
Significance of biohazard symbol |
35 (92.1%) |
18 (78.3%) |
17 (65.4%) |
12 (48.0%) |
82 (73.2%) |
16.1 |
0.001 |
A3 |
Percentage of infectious waste among total waste in hospital |
30 (78.9%) |
17 (73.9%) |
14 (53.8%) |
10 (40.0%) |
71 (63.4%) |
12 |
0.007 |
A4 |
Hazards associated with improper BMWM |
33 (86.8%) |
19 (82.6%) |
20 (76.9%) |
16 (64.0%) |
88 (78.6%) |
4.96 |
0.175 |
A5 |
Description of PPE while handling BMW |
32 (84.2%) |
12 (52.2%) |
12 (46.2%) |
10 (40.0%) |
74 (66.1%) |
15.9 |
0.001 |
A6 |
Segregation of BMW at source |
34 (89.5%) |
15 (65.2%) |
16 (61.5%) |
14 (56.0%) |
79 (70.5%) |
10.4 |
0.015 |
A7 |
Color coding of BMW as per 2016 guidelines |
29 (76.3%) |
17 (73.9%) |
15 (57.7%) |
14 (56.0%) |
75 (67.0%) |
4.37 |
0.224 |
A8 |
Storage of BMW beyond 48 hours |
34 (89.5%) |
18 (73.3%) |
17 (65.4%) |
13 (52.0%) |
82 (73.2%) |
12 |
0.007 |
A9 |
Transportation rules including GPS system in BMW Vehicles |
28 (73.7%) |
14 (60.9%) |
12 (46.2%) |
8 (32.0%) |
62 (55.4%) |
11.9 |
0.008 |
A10 |
Proper final disposal of waste |
28 (73.7%) |
17 (73.9%) |
16 (61.5%) |
14 (56.0%) |
75 (67.0%) |
2.98 |
0.394 |
Overall awareness (%) |
83.4% (71.6%-95.2%) |
71.3% (52.8% -89.8%) |
61.5% (42.8% – 80.2%) |
52.0% (32.4% – 71.6%) |
69.6% (61.1% – 78.1%) |
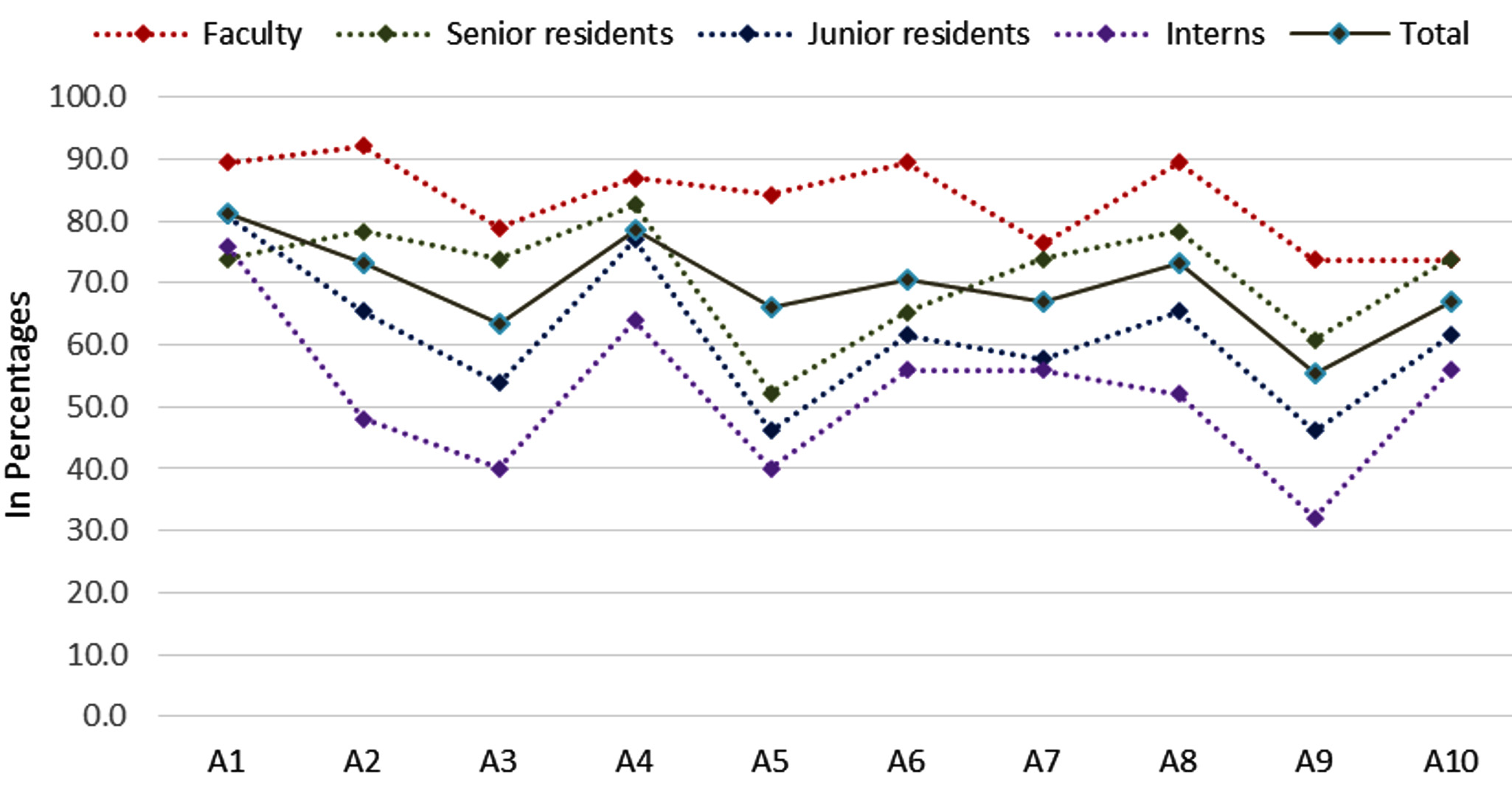
Fig. 3. Level of awareness to BMWM among faculty, residents and interns.
Overall faculty showed maximum compliance with existing practices with an overall rate of 79.2% while interns’ showed an overall 58.8% practice level. (Table 5, Fig. 4)
Table (5):
Adequacy of BMWM practices awareness amongst and among faculty, residents and interns.
| Satisfactory practices | ||||||||
|---|---|---|---|---|---|---|---|---|
| Assessment of adequacy of BMWM practices as per 2016 guidelines | Faculty (38) | Senior residents (23) | Junior residents (26) | Interns (25) |
Total (112) |
chi sq | p-value | |
| P1 | Method for segregating collecting human anatomical waste | 30 (78.9%) | 17 (73.9%) |
12 (46.2%) |
12 (48.0%) | 71 (63.4%) | 10.9 | 0.012 |
| P2 | Method for segregating contaminated linen, casts, cotton gauze | 29 (76.3%) | 19 (82.6%) |
13 (50.0%) |
11 (44.0%) | 72 (64.3%) | 12.6 | 0.006 |
| P3 | Method for segregating infected plastic wastes | 32 (84.2%) | 19 (82.6%) | 15 (57.7%) | 13 (52.0%) | 79 (70.5%) | 11.2 | 0.011 |
| P4 | Method for segregating general wastes | 34 (89.5%) | 19 (82.6%) | 17 (65.4%) | 16 (64.0%) | 86 (76.8%) | 8.06 | 0.045 |
| P5 | Method for segregating metallic sharp wastes | 29 (76.3%) | 18 (78.3%) |
15 (57.7%) |
19 (76.0%) | 81 (72.3%) | 3.66 | 0.301 |
| P6 | Method for discarding infectious liquid waste | 30 (78.9%) | 17 (73.9%) |
17 (65.4%) |
12 (48.0%) | 76 (67.9%) | 7.12 | 0.068 |
| P7 | Method for discarding used disposable needles/ Use of Needle Cutter | 32 (84.2%) | 20 (87.0%) |
17 (65.4%) |
19 (76.0%) | 88 (78.6%) | 4.46 | 0.216 |
| P8 | How to dispose Intact or broken glassware | 27 (71.1%) | 16 (69.6%) |
17 (65.4%) |
17 (68.0%) | 77 (68.8%) | 0.245 | 0.97 |
| P9 | Practices of reporting of injuries resulting from improperly disposed BMW | 30 (78.9%) | 19 (82.6%) |
15 (57.7%) |
13 (52.0%) | 77 (68.8%) | 8.64 | 0.034 |
| P10 | Correct management of Spills | 28 (73.7%) | 18 (78.3%) | 18 (69.2%) | 15 (60.0%) | 79 (70.5%) | 2.2 | 0.532 |
| Overall awareness (%) | 79.2% (66.3% – 92.1%) | 79.1% (62.5% – 95.7%) | 60% (41.2% – 78.8%) | 58.8% (39.5% – 78.1%) | 70.2% (61.7% – 78.7%) | |||
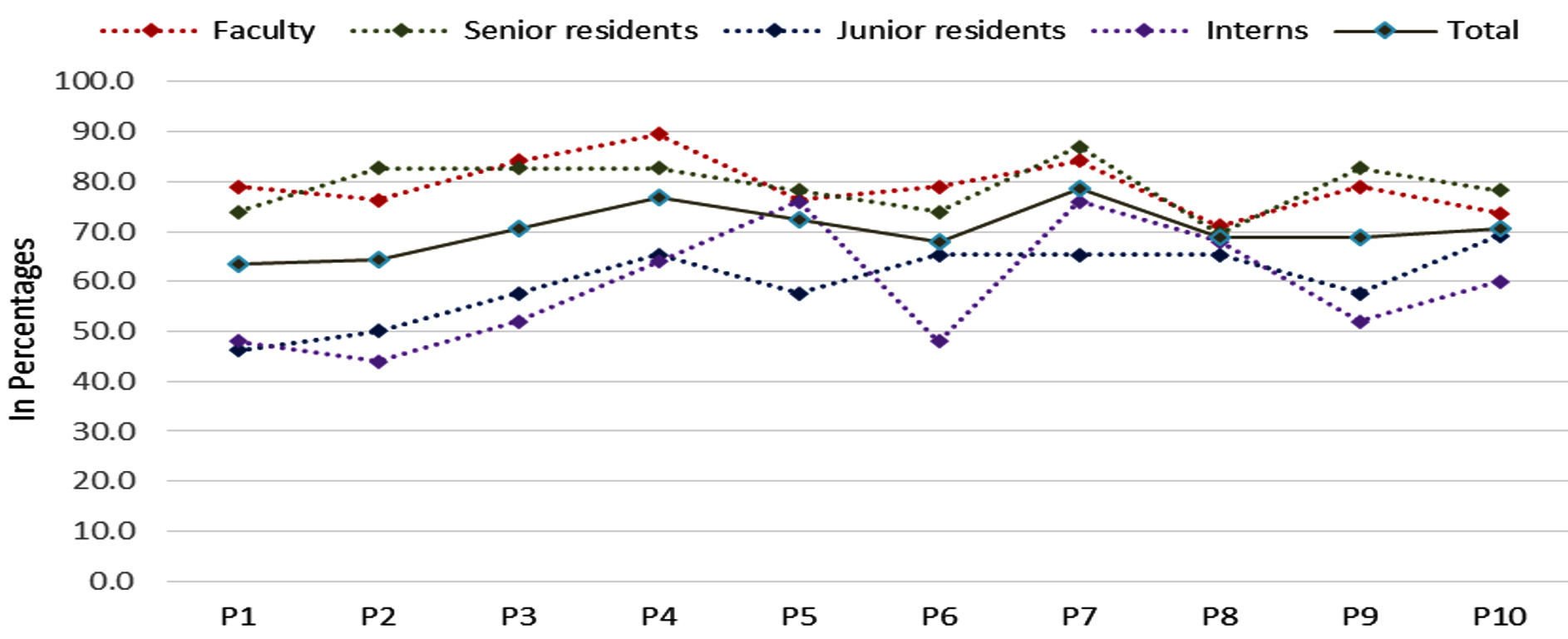
Fig. 4. Level of practices to BMW among faculty, residents and interns.
BMWM practices are far from optimal in India. The issues in segregation, transport and disposal are major biosafety threats. Inappropriate disposal techniques have reached alarming levels in respect to environmental safety and public health.
India generates about three million tons of medical waste every year. 10 to 35% of this BMW is potentially hazardous. Inappropriate separationism at point of generation and desultory mingling with non-hazardous waste create a bigger load of hazardous waste.12
Various studies in the past have shown that health care workers in our country are still not fully aware of proper BMW handling and disposal. Although globally there is heightened awareness about proper BMW handling and disposal.13 A report by the Indian Institute of Management, Lucknow depicted that about 50 -55% of the BMW generated in India is managed properly at all levels of disposal chain while the remaining mostly ends up mixing with the general waste.14 Thus heightened awareness, stringent processes, and appropriate skills among health care workers are essential for the adequate management of biomedical waste. Various studies conducted across India revealed gaps in the knowledge, behavioral void, and inconsistent practice which are major roadblocks in proper BMWM.15-16
Overall, most groups of HCP scored fairly on BMWM practices awareness. The awareness about BMW among doctors and nurses was relatively better (68.6% and 69.3% respectively), followed by that of waste handlers (59.9%).
The findings are consistent with the study done by a french study, where 62.6% of HCWs were having adequate knowledge regarding BMWM.17 An Indian study found that 64% of nurses had satisfactory knowledge and awareness regarding BMWM.18
The findings in our study could be attributed to the fact that regular BMW training is compulsorily imparted to all doctors, nurses, and waste handlers in the hospital. Additionally, onsite training is giving to all HCWs in the wards by the BMWM team. Online and hybrid modes of training were used during the pandemic.
Need to focus on all categories of healthcare workers are of utmost importance. In our study, we found that 79.4% of HCWs have attended the BMWM training program of which 79.4% were doctors and 83% were nurses. However, only 68.9% of waste handlers attended the training program. This reflects the low level of awareness and teaching opportunities among the waste handlers.
The gaps in knowledge were seen in BMW aspects regarding segregation, color coding, storage and transport and significance of biohazard symbol and the findings were statistically significant. As these HCWs are regularly engaged in the process of BMWM, therefore there is an urgent need to sensitize.19
Lesser knowledge amongst sanitary staff is mainly attributed to relatively lesser educational qualifications. Kapoor et al in their systematic review concluded that the level of knowledge in the study population regarding BMW was low and continuous training programs were needed to enhance it.20
On comparing the awareness and existing practices among faculty, residents, and interns, the level of awareness was higher among faculties as compared to the other doctors.21 This could be due to the greater number of training and onsite programs attended by the faculty and senior residents. As most of the interns and junior residents were recently recruited they had missed some of the training programs. Hence continuous training for all newly recruited doctors needs to be organized periodically. There is also a need for online recurrent training on BMWM with short refresher courses.
Though a greater number of doctors and nurses owned BMWM practices, nurse’s engagement to best practices was noteworthy.22 This could be because of the regular on-site training programs for nursing staff on segregation and transportation. Practices of segregation of plastic waste, metallic waste, and proper use of needle cutters were considerably better in nurses as compared to doctors. Proper discarding of liquid waste and broken glassware was also better known to nurses than doctors. Higher practice compliance scores amongst nursing colleagues could be attributed to better discipline, ownership on BMWM process, answerability and the responsibility bestowed upon them. Injury reporting from improperly disposed of BMW were higher among doctors in comparison to nurses.
Sanitation workers were largely ignorant about most of the aspects of BMWM practices. Most of these sanitation workers were placed on ad hoc jobs and were less aware about biohazard risk from BMW.
Every step involving biomedical waste generation, segregation, storage, transport and disposal need to be closely monitored. A surveillance system needs to be set for ensuring integrity of the whole process. Information, Education and communication (IEC) activities need to be contextual, ongoing and assessment based.
BMWM training program is essential to sensitize and raise awareness among HCWs. It also emphasizes the importance of the segregation of BMW. The training program also educates about the hazards associated with poor BMWM with special emphasis on sharp injuries.
Training should emphasize on empowering the health professionals on all theoretical and practical aspects of BMWM. Political will, ownership of BMWM, stringent implementation and IEC activities are pivotal in the program. The ramifications of best practices regarding BMWM go beyond realms of biosafety, injury prevention, vaccination, universal precautions. Novel and contextual strategies need to be adapted. Road shows, posters, handouts, stickers, charts and dedicated theme days will raise the awareness.23 Active surveillance, checklists and regular audits can enhance accountability in BMWM.
Improper disposal of BMW has many adverse and harmful effects on the environment & human health. To improve BMWM, it is important to be aware of its proper management and understand and evaluate the current practices in BMWM, to identify the gaps and to address them. Multipronged approach for education and implementation needs to be contextualized utilizing routine and novel tools. Advanced surveillance and checklist based pathways need to be utilized at every level of BMWM.
ACKNOWLEDGMENTS
I would like to thank Infection Control Nurses for their logistical support. I would also like to express my gratitude towards the BMW team, hospital administration & staff for their relentless support.
FUNDING
None.
ETHICS STATEMENT
It is an observational and non-interventional study. Principles of research ethics have been followed. No human or animal experimentation was involved.
AVAILABILITY OF DATA
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
INFORMED CONSENT
Informed consent was obtained for experimentation and that it confirms to the standards currently applied in India. The privacy rights of participants were observed.
- Safe Management of Wastes from Health-Care Activities. Second Edition. Edited by Chartier Y, Emmanuel J, Pieper U, et al. WHO. 2014. https://www.euro.who.int/__data/assets/pdf_file/0012/268779/Safe-management-of-wastes-from-health-care-activities-Eng.pdf
- Bio-Medical Waste (Management and Handling, 1998) Rules. New Delhi: Government of India Publications; Ministry of Environment and Forests Notification; 1998:276-284.
- Revised Draft Guidelines on Best Available Techniques and Provisional Guidance on Best Environmental Practices of the Stockholm Convention on Persistent Organic Pollutants. Geneva: Secretariat of the Stockholm Convention. Secretariat of the Stockholm Convention. 2006.
- Anwer M. Solid Waste Management in India Under COVID19 Pandemic: Challenges and Solutions. Int J Eng Res Technol. 2020;9(06):368-373.
Crossref - WHO. Review of Health Impacts from Microbiological Hazards in Health-Care Wastes. Geneva: World Health Organization. 2004.
- Corrao Crn, Mazzotta A, LA Torre G, De Giusti M. Biological Risk and Occupational Health. Industrial Health. 2012;50(4):326-337.
Crossref - Rachiotis G, Papagiannis D, Markas D, Thanasias E, Dounias G, Hadjichristodoulou C. Hepatitis B virus infection and waste collection: Prevalence, risk factors, and infection pathway. Am J Ind Med. 2012;55(7):650-655.
Crossref - Mattiello A, Chiodini P, Bianco E, et al. Health effects associated with the disposal of solid waste in landfills and incinerators in populations living in surrounding areas: a systematic review. International Journal of Public Health. 2013;58(5):725-735.
Crossref - Khan FA, Soderquist B, Jass J. Prevalence and Diversity of Antibiotic Resistance Genes in Swedish Aquatic Environments Impacted by Household and Hospital Wastewater. Front Microbiol. 2019;10:688.
Crossref - Padmanabhan KK, Barik D. Health Hazards of Medical Waste and its Disposal. Energy from Toxic Organic Waste for Heat and Power Generation. 2019;99-118.
Crossref - Imchen T, Kumari R, Singh JV, Srivastava K, Singh A. Study of biomedical waste management among healthcare personnel at a Tertiary hospital in Lucknow district. Int J Community Med Public Health. 2017;4(5):1483-1487.
Crossref - Datta P, Mohi G, Chander J. Biomedical waste management in India: Critical appraisal. J Lab Physicians. 2018;10(1):6-14.
Crossref - INCLEN Program Evaluation Network (IPEN) study group, New Delhi, India. Bio-medical waste management: situational analysis & predictors of performances in 25 districts across 20 Indian States. Indian J Med Res. 2014;139(1):141-153.
- Mor RS, Sarbjit S, Bhardwaj A, Osama M. Exploring the awareness level of biomedical waste management: Case of Indian healthcare. Management Science Letters. 2017;7:467-478.
Crossref - Dudi M, Sharma R, Sharma S, Jain M. Assessment of the knowledge, attitude and practices regarding Biomedical Waste Management amongst Paramedical Staff in a Tertiary Level Health Care Facility. Int J Med Sci Public Health. 2016;5(4):615-619.
Crossref - Rajput A, Deshpande K, Chakole SV, Mehta SC. Is Biomedical Waste Management Knowledge Adequate in Paramedics & Sanitary Workers in Hospitals of Ujjain City. Natl J Community Med. 2016;7(3):151-154
- Ndiaye P, Fall C, Diedhiou A, Tal-Dial A, Diedhiou O. Gestion des déchets biomédicaux (DBM) au Centre hospitalier régional (CHR) de Ziguinchor [Biomedical waste management in the Regional Hospital Center of Ziguinchor]. Sante. 2003;13(3):171-176.
- Sharma A, Sharma V, Sharma S, Singh P. Awareness of biomedical waste management among health care personnel in jaipur, India. Oral Health Dent Manag. 2013;12(1):32-40.
- Hakim SA, Mohsen A, Bakr I. Knowledge, attitudes and practices of health-care personnel towards waste disposal management at Ain Shams University Hospitals, Cairo. East Mediterr Health J. 2014;20(5):347-354.
Crossref - Kapoor D, Nirola A, Kapoor V, Gambhir R-S. Knowledge and awareness regarding biomedical waste management in dental teaching institutions in India- A systematic review. J Clin Exp Dent. 2014;6(4):e419-e424.
Crossref - Sharma P, Jais M, Gupta P, Randhawa V. Adequacy of awareness regarding biomedical waste management among health care workers in a tertiary care hospital in Delhi. Journal of Patient Safety & Infection Control. 2015;3(2)98.
Crossref - Mathur V, Dwivedi S, Hassan M, Misra R. Knowledge, Attitude, and Practices about Biomedical Waste Management among Healthcare Personnel: A Cross-sectional Study. Indian J Community Med. 2011;36(2):143-145.
Crossref - Ministry of Environment, Forest, and Climate Change, Biomedical Waste Management Rules, New Delhi; 2016:1-63.
© The Author(s) 2021. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.