


ISSN: 0973-7510
E-ISSN: 2581-690X
Prompt diagnosis of coronavirus disease 2019 (COVID-19) is requisite due to the upsurge of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) cases globally. Real-time reverse-transcription polymerase chain reaction (rRT-PCR) remains as the gold standard for the diagnosis of SARS-CoV-2 due to its higher sensitivity and specificity. Regardless, due to its longer turnaround time and expertise, bed side testing rapid antigen based tests were developed in order for portable, rapid diagnosis of the disease. The present study delineates the utility of Rapid Antigen Testing (RAT) screening among symptomatic and asymptomatic patients in a tertiary care hospital. This is a retrospective data collection study from Indian Council of Medical Research (ICMR) portal by exporting the excel sheet from March 2021 to March 2022 who undergone COVID testing in a tertiary care diagnostics facility. The demographic and vaccination details of the individuals were extracted using ICMR Sample referral form (SRF) from all patients who are tested for RAT. Of the total 9898 patients tested for RAT, 392 and 9506 were vaccinated and unvaccinated, respectively. Among them, number of positives was 3% and 15% respectively. The odds ratio showed that the vaccinated individuals had 81.4% reduced risk of getting infection compared to unvaccinated individuals (OR-0.186; p=0.001). A significant difference was observed between the type of vaccine used and COVID infection, majority of them had taken Covishield (83.5%) followed by Covaxin (16%) [p=0.0005]. Males showed a marginally significant p trend with COVID infectivity (OR=1.114, p=0.073) too. RAT is useful as a screening test for rapid diagnosis of infection in patients who are more prone to spread the disease. As RAT is cost effective and had short-turnaround time, it can be recommended in areas with upsurge in SARS-CoV-2 cases to administer isolation and infection control measures.
Rapid Antigen Test, Breakthrough Infections, COVID-19, SARS-CoV-2, Vaccines
The SARS-CoV-2 pandemic started in January 2020 and caused social and economic burden in the community. Till date, it has affected about 110 million people globally. The upsurge of SARS-CoV-2 prompts the rapid detection of SARS-CoV-2 infection. Among the various available diagnostic tests to confirm the clinical diagnosis of COVID-19 infection, nucleic acid amplification test and serological tests are generally used for the diagnosis.1,2 The Real-Time reverse transcriptase PCR (rRT-PCR) is considered as the ‘gold standard’ test for the diagnosis of COVID-19. It demands manpower, technical expertise, time, more cost, laboratory setting with proper biosafety measures.3 For the rapid detection and isolation of positive patients, directions have been made to take on the use of rapid diagnostic test for rapid diagnosis and infection control. The Rapid Antigen Test (RAT) is found to be cheaper, fast, and easy to perform on bed side.4 RAT is useful in case of screening in emergency before the patients are triaged and shifted to respective departments, emergency surgery or invasive procedures, endoscopy, etc. According to Indian Council of Medical Research (ICMR) guidelines using RAT as a screening test in symptomatic individuals needs confirmation by rRT-PCR if the initial screening is negative. And in case of asymptomatic screening of the individual in an area of low prevalence may give a low positive predictive value which has to be further confirmed with rRT-PCR.5 Data from previous research has shown the detection of SARS-CoV-2 with RAT compared to RT-PCR.6,7 There are certain pitfalls in using RAT like most of the kits require nasopharyngeal swab which is quite difficult to collect in pediatric age group and in mentally challenged individuals, a meta analysis study shown an average sensitivity and specificity of RAT as 56.2% and 99.5% respectively.8 There are various RAT kits approved by ICMR for the diagnostic use. The performance of RAT in vaccinated individuals were not previously explored completely. This study shows the utility of RAT screening in symptomatic and asymptomatic patients.
This study was an observational retrospective data collection study conducted in the Department of Microbiology, Mahatma Gandhi Medical College & Research Institute (MGMCRI), Puducherry, a tertiary care hospital in Southern India. The data was collected from the Indian Council of Medical Research (ICMR) COVID-19 data entry portal by exporting the excel sheet from March 2021 to March 2022. ICMR provide the data entry portal of COVID-19 testing which mainly consists of data pertained to COVID-19 RT-PCR and Rapid Antigen test (RAT). This is collected by the Government of India with the help of authorized collection Centre persons throughout the country.9 In our centre, there are separate data entry operators who enter all the required patients details, category under which they were tested, symptoms, kit used and the result. These datas were collected by using ICMR Sample Referral Form (SRF) from all patients who are tested for RAT. The study was approved by Institute Human Ethics Committee (IHEC)-MGMCRI/IRC/24/2021/04/IHEC/41 and obtained waiver for patients consent. The demographic details, hospitalization status, vaccine status, COVID-19 infection among vaccinated (after one and two doses) and unvaccinated individuals, frequency of infection in different types of vaccines were the data collected and analysed. Most patients included were from emergency, ward or outpatients who got screened for various reasons like suspected SARS-CoV-2 infection, screening for invasive or non-invasive procedures, international travelers, self-testing, contacts with lab confirmed cases etc and they were isolated accordingly. The extracted data was then consolidated as vaccinated and unvaccinated individuals.
Statistical analysis
The data collected from ICMR COVID-19 data entry portal was exported to MS Excel and analyzed in SPSS version 17.090 (IBM Corp., Armonk NY, USA). All categorical variables were presented as frequencies and percentages. Chi-square test was used for the comparison of proportions and regression analysis (Odds Ratios [ORs] with 95% confidence intervals) was performed. For comparisons, all p-values were two-sided and P-value <0.05 was considered statistically significant.
During the study period from March 2021 to March 2022, the total number of patients screened by RAT was 9898. Of the subjects included in the study, 520 (7.8%) were symptomatic, 6149 (92.2%) were asymptomatic. Among the vaccinated individuals (n=392) and unvaccinated individuals (n=9506), the number of positives were 3% and 15%, respectively. The breakthrough infection after single and double dose of vaccine is analysed and observed no significant difference in breakthrough infection between them (p>0.05).
The details were shown in Figure & Table 1. Individuals who are screened positive for SARS-CoV-2 virus even after primary or booster vaccination are considered as “vaccine breakthrough infection”. The symptom status, whether symptomatic or asymptomatic has been mentioned based on the data from sample referral form containing patients details.
Table (1):
Frequency of infection among vaccinated, unvaccinated individuals and post vaccination infection after single and double dose of vaccine
Total N (%) |
Positives N (%) |
Negatives N (%) |
|
|---|---|---|---|
Vaccinated individuals |
392 (100%) |
12 (3%) |
380 (97%) |
Unvaccinated individuals |
9506 (100%) |
1377 (15%) |
8129 (85%) |
Post vaccination infection after single dose of vaccine |
392 (100%) |
4 (1%) |
388 (99%) |
Post vaccination infection after double dose of vaccine |
163 (100%) |
10 (6%) |
153 (94%) |
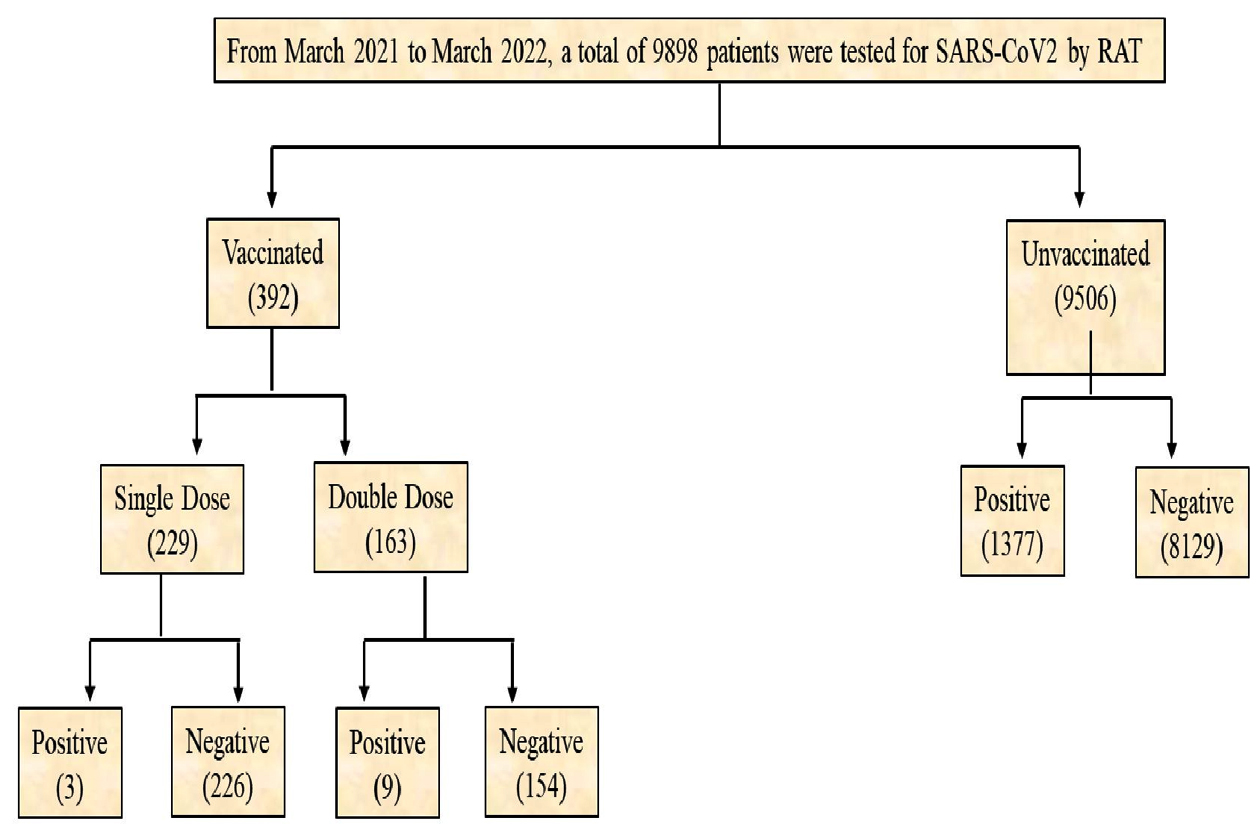
Figure. Frequency of infection among vaccinated and unvaccinated individuals
Table 2 depicts the breakthrough infection status after different types of vaccine. It was observed that, majority of them had taken Covishield (83.5%) followed by Covaxin (16%). The association between breakthrough infection rate and type of vaccines was also examined. We observed significant difference between the type of vaccine used and COVID infection (c2=15.28, p=0.0005).
Table (2):
Breakthrough infection after different types of vaccine
| Types of vaccine | Total N (%) | Positive N (%) | Negative N (%) | χ2 | p-value |
|---|---|---|---|---|---|
| Covaxin | 62 (16%) | 1 (1.6%) | 61 (98.4%) | 15.28 | 0.0005 |
| Covishield | 328 (83.5%) | 10 (3.05%) | 318 (96.95%) | ||
| Others | 2 (0.5%) | 1 (50%) | 1 (50%) | ||
| Total | 392 | 12 | 380 |
When regression analysis was performed, it was found that the vaccinated individuals have 81.4% reduced risk of getting COVID infection compared to unvaccinated individuals (OR: 0.186, p=0.001) (Table 3), this strengthens importance of vaccinations in COVID infections.
Table (3):
Odds ratio among vaccinated and unvaccinated individual
| Positive | Negative | Odds ratio (OR) | p-value | |
|---|---|---|---|---|
| Vaccinated | 12 (3%) | 380 (97%) | 0.186 | 0.001 |
| Unvaccinated | 1377 (14.5%) | 8129 (85.5%) |
OR: Odds Ratio
Gender-wise analysis on COVID positives with vaccination was also analyzed and it was found that 2.7% of the male and 4% of female were infected. When regression analysis was performed, there observed no association between sex and COVID infection (Table 4).
Table (4):
Gender wise analysis among vaccinated individuals
| Vaccinated Positive | Vaccinated Negative | Odds ratio (OR) | p-value | |
|---|---|---|---|---|
| Male | 8 (2.7%) | 285 (97.3%) | 0.666 | 0.751 |
| Female | 4 (4%) | 95 (96%) |
Gender-wise analysis on COVID positives without vaccination was also analyzed and it was found that 15% of the male and 13.7% of female were infected. Surprisingly, when regression analysis was performed, male sex shown a marginally significant p trend with the COVID infectivity (OR=1.114, p=0.073) (Table 5).
Table (5):
Gender wise analysis among unvaccinated individuals
| Unvaccinated Positive | Unvaccinated Negative | Odds ratio (OR) | p-value | |
|---|---|---|---|---|
| Male | 806 (15%) | 4544 (85%) | 1.114 | 0.073 |
| Female | 571 (13.7%) | 3585 (86.3%) |
Among the positive cases of COVID, subgroup analysis was performed based on the vaccination status and gender. It was found that among the male, 1.7% of the positive cases were vaccinated while 1.2% among female were vaccinated. The COVID positives were very high in both male and female when they are not vaccinated (Table 6).
Table (6):
Infection among vaccinated and unvaccinated individuals
| Positive | χ2 | Odds ratio (OR) | p-value | ||
|---|---|---|---|---|---|
| Vaccinated | Unvaccinated | ||||
| Male | 14 (1.7%) | 806 (98.3%) | 0.279 | 1.417 | 0.598 |
| Female | 7 (1.2%) | 571 (98.8%) | |||
OR: Odds Ratio
Since the rapid surge of COVID-19, more attention had been on the accessibility of rapid, accurate, and affordable diagnostic test. Early detection is of more focus in health care settings to execute appropriate infection control measures to prevent the disease transmission. The high sensitive real-time RT-PCR is considered as the gold-standard laboratory diagnostic test and also remain as a widely used confirmatory test for COVID-19. Rapid, cost effective laboratory tests are stand in need to curb the spread and management of SARS-CoV-2 infection. In a populated country like India, SARS-CoV-2 testing by RT-PCR is an uphill battle since it can detect non infectious as well as dead viral paricles which lasts as positive for long period of time.10 In this scenario, RAT can be used as SARS-CoV-2 detection point-of-care test for rapid and massive testing, despite its lower sensitivity than RT-PCR.11 Since January 2020, three consecutive waves occurred, in Puducherry Union territory (UT) the cases started increasing since March 2020. This rapid surge of cases in the UT made the government for the emergency training of health care workers and preparedness towards the outbreak management. In our hospital setting, we tested surveillance samples, outpatient, and in-patient samples.
In our present study, the positivity rate was 14% (1389/9898). We observed this during the second and third wave of SARS-CoV-2 pandemic. Also, about 3% among vaccinated and 15% among unvaccinated individuals had breakthrough infection. This observations are similar to earlier studies which reported breakthrough infection ranging from 4 to 31%.12-16 Also, a recent study from Pune, India, reported that 16.8% of the vaccinated had breakthrough infections.17 In our study, there is no significant difference in breakthrough infections after different intervals of post vaccinations. This might be explained by the efficient immune response provided by vaccination in vaccinated individuals. To date, more than 10 billion doses have been delivered as per the approval of vaccines by various regulatory systems.18
Besides, we also examined a significant difference between the type of vaccine used and COVID infection, with majority taken Covishield (83.5%) followed by Covaxin (16%). The infection rate was higher in both vaccines. It is plausible that the mutant strains perhaps be resistant to the available vaccines apart from the reports about the efficacy against the variant strains. Additionally, in our study vaccinated individuals had 81.4% reduced risk of getting infection compared to unvaccinated individuals showed the reduced infection rate in vaccinated patients.19 Parallel results of increased proportion of developing severe infections among unvaccinated individuals were observed in other studies.20-22 Similarly, a recent study of breakthrough infections among healthcare workers from Sikkim reported less severe infections in vaccinated individuals.23 Hence, this suggests that vaccines reduce COVID-19 associated emergency hospitalization and disease severity. Similarly, male sex depicted a marginal sex specific variance in COVID-19 virulence. Previous studies shown that male gender overrepresented in COVID-19 infectivity in various populations, in line with our results.24,25 This may be due to gender related behaviors, hormonal, genetic factors and differential expression of Angiotensin converting enzyme-2 (ACE-2) receptors in males and females.26 and needs more attention. Hence in our scenario, RAT results found to be primarily based on the viral load of the samples. The identified difference in RAT results between vaccinated and unvaccinated individuals showed higher viral load in unvaccinated individuals.
In conclusion, we observed no variations in breakthrough infections between the full vaccinations which might be due to the efficient immune response imparted through vaccinations. Also, it appears that vaccinated individuals had 81.4% reduced infection rate compared to unvaccinated which inturn showed these vaccines are still protective against severe infectivity. Meanwhile, our study depicted a marginal sex specific variance in COVID infection, hence gender specificity should be considered while elucidating the COVID data. Hence RAT can be useful as a screening tool in curbing the COVID-19 pandemic through rapid diagnosis of infection in vaccinated individuals who are more likely to spread the disease. As RAT is cost effective and had short-turnaround time, it can be recommended in areas with upsurge in SARS-CoV-2 cases to administer isolation and infection control measures. However, it may be ascertained by COVID RT-PCR.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
The study was approved by the Institute Human Ethics Committee (IHEC), Mahatma Gandhi Medical College & Research Institute, Puducherry, India, with reference number MGMCRI/IRC/24/2021/04/ IHEC/41.
- Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25(3):2000045.
Crossref - Wan Y, Shang J, Graham R, Baric RS, Li F. Receptor recognition by the novel coronavirus fromWuhan: an analysis based on decadelong structural studies of SARS coronavirus. J Virol. 2020; 94(7):e00127-e00120.
Crossref - Albert E, Torres I, Bueno F, et al. Field evaluation of a rapid antigen test (Panbio COVID-19 Ag Rapid Test Device) for COVID-19 diagnosis in primary healthcare centres. Clin Microbiol Infect. 2021;27(3):472.e7-472.e10.
Crossref - Alejandro F-M, Argemi J, Rodriguez, JA, Arino AH, Moreno-Galarraga L. Validation of a Rapid Antigen Test as a Screening Tool for SARS-CoV-2 Infection in Asymptomatic Populations. Sensitivity, Specificity and Predictive Values.Clin Med. 2021;37:100954.
Crossref - Menchinelli G, De Angelis G, Cacaci M, et al. SARS-CoV-2 Antigen Detection to Expand Testing Capacity for COVID-19: Results from a Hospital Emergency Department Testing Site. Diagnostics. 2021;11(7):1211.
Crossref - Turcato G, Zaboli A, Pfeifer N, et al. Rapid antigen test to identify COVID-19 infected patients with and without symptoms admitted to the Emergency Department. Am J Emerg Med. 2022;51:92-97.
Crossref - Morishima M, Kimura M, Sakoh T, et al. Universal admission screening for COVID-19 using quantitative antigen testing and questionnaire screening to prevent nosocomial spread. PLoS One. 2022;17(11):e0277426.
Crossref - Dinnes J, Deeks JJ, Adriano A, et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst Rev. 2020;8(8):CD013705.
Crossref - Kaur J, Kaur J, Dhama AS, Kumar V, Singh H. Management of COVID-19 Pandemic Data in India: Challenges Faced and Lessons Learnt. Front Big Data. 2021;4:790158.
Crossref - Peng B, Zhou W, Pettit RW, et al. Optimal test-assisted quarantine strategies for COVID-19. medRxiv. 2021;11.06.20222398.
Crossref - Hong KH, Lee SW, Kim TS, et al. Guidelines for laboratory diagnosis of coronavirus disease 2019 (COVID-19) in Korea. Ann Lab Med. 2020;40(5):351-360.
Crossref - Singh CM, Singh PK, Naik BN, Pandey S, Nirala SK, Singh PK. Clinico-epidemiological profile of breakthrough COVID-19 Infection among vaccinated beneficiaries from a COVID-19 vaccination Centre in Bihar, India. Ethiop J Health Sci. 2022; 32(1):15-26.
- Teran RA, Walblay KA, Shane EL, et al. Post vaccination SARS-CoV-2 Infections among Skilled Nursing Facility Residents and Staff Members – Chicago, Illinois, December 2020-March 2021. Am J Transplant. 2021;21(6):2290-2297.
Crossref - Niyas VKM, Arjun R. Breakthrough COVID-19 infections among health care workers after two doses of ChAdOx1 nCoV-19 vaccine. QJM. 2021;114(10):757-758.
Crossref - Krishna B, Gupta A, Meena K, et al. Prevalence, severity, and risk factor of breakthrough infection after vaccination with either the Covaxin or the Covishield among healthcare workers: A nationwide cross-sectional study. J Anaesthesiol Clin Pharmacol. 2022;38(Suppl 1):S66-S78.
Crossref - Rahi M, Yadav CP, Ahmad SS, et al. Vaccination coverage and breakthrough infections of COVID-19 during the second wave among staff of selected medical institutions in India. PLOS Glob Public Health. 2023;3(4):e0000946.
Crossref - Doke PP, Mhaske ST, Oka G, et al. SARS-CoV-2 breakthrough infections during the second wave of COVID-19 at Pune, India. Front Public Health. 2023;10:1040012.
Crossref - Mathieu E, Richie H, Ortiz-Ospina E, Macdonald B, Hasell J, Beltekian D, et al. “Coronavirus Pandemic (COVID-19)”. Our World in Data. March 2020. Retrieved from: ‘https://ourworldindata.org/coronavirus
- Muthukrishnan J, Vardhan V, Mangalesh S, et al. Vaccination status and COVID-19 related mortality: A hospital based cross sectional study. Med J Armed Forces India. 2021;77(Sup 2):S278-S282.
Crossref - Balachandran S, Moni M, Sathyapalan DT, et al. A comparison of clinical outcomes between vaccinated and vaccine-naive patients of COVID-19, in four tertiary care hospitals of Kerala, South India. Clin Epidemiol Glob Heal. 2022;13:100971.
Crossref - Butt AA, Nafady-Hego H, Chemaitelly H, et al. Outcomes Among Patients with Breakthrough SARS-CoV-2 Infection After Vaccination. Int J Infect Dis. 2021:110:353-358.
Crossref - Wichaidit M, Nopsopon T, Sunan K, et al. Breakthrough infections, hospital admissions, and mortality after major COVID-19 vaccination profiles: A prospective cohort study. Lancet Reg Health Southeast Asia. 2023;8:100106.
Crossref - Gurung S, Tewari E, Pradhan P, et al. Vaccine Breakthrough Infections Among Healthcare Workers in a COVID-19-Designated Tertiary Care Government Hospital in Sikkim. Cureus. 2023;15(10):e46752.
Crossref - Pijls BG, Jolani S, Atherley A, et al. Temporal trends of sex differences for COVID-19 infection, hospitalisation, severe disease, intensive care unit (ICU) admission and death: a metaanalysis of 229 studies covering over 10M patients. F1000Research. 2022;11:5.
Crossref - Kharroubi SA, Diab-El-Harake M. Sex-differences in COVID-19 diagnosis, risk factors and disease comorbidities: A large US-based cohort study. Front Public Health. 2022;17;10:1029190.
Crossref - Mariappan V, Rao SR, Pillai AB. Angiotensin-converting enzyme 2: A protective factor in regulating disease virulence of SARS-COV-2. IUBMB Life. 2020;72(12):2533-2545.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.