

Parth Goel1 ![]() , Dweepna Garg2
, Dweepna Garg2![]() and Amit Ganatra2
and Amit Ganatra2![]()
COVID-19 is one of the very contagious diseases from the family Coronaviridae and spreading at a faster rate in the community. In December 2019, the first case of COVID-19 was reported in Wuhan, China. An epidemic outbreak of COVID-19 was seen in India from March 2020. Epidemiological data of COVID-19 cases of the world and India have been analyzed in our study. We have utilized publicly available two databases from data repository by Johns Hopkins CSSE and covid19india.org. COVID-19 cases and case fatality rate (CFR) of the world have been summarized and compared with India from January 22, 2020 to April 15, 2020. Indian cases were analyzed among states of India and also compared with age and gender by performing statistical approaches such as central tendency, standard deviation and interquartile range. By April 15, 2020, Indian has reported 12,322 confirmed cases, 1,498 recovered cases and 405 death cases of COVID-19. In spite of India being a diverse country with the second-highest population, the deadly side of COVID-19 was comparatively far less as compared to the other countries. India has taken preemptive measures at an early stage to prevent transmission of COVID-19 outbreak and it is reviewed from our study by comparing India with other countries. Our study also summarizes that age also plays a vital role in the intervention of COVID-19 cases.
Coronavirus, COVID-19, Epidemic, Pandemic, India, Statistical analysis
The spread of coronavirus has shown an exponential growth all over the world and it has become uncontrollable. Twenty-seven cases of pneumonia of unknown etiology were detected on 31st December 2019, in Wuhan City, the capital of Hubei Province, with a population of 11 million1. It was widely considered that source of novel coronavirus may have been from the Wuhan’s Huanan Seafood Wholesale Market, and it also referred as zoonotic disease. The outbreak of coronavirus has affected around 250 countries as well, besides China. On January 31, 2020, the World Health Organization (WHO) declared the outbreak as an epidemic for concern of public health emergencies. Later, on March 11, 2020, it was announced as a pandemic by the WHO2. Scientists in China identified the etiological agent of the epidemic as a previously unknown coronavirus dated January 7, 2020, and it was labeled as 2019-nCoV (2019 novel coronavirus)3,4.
The novel coronavirus disease received an official name as Coronavirus Disease 19 (COVID-19) by the World Health Organization (WHO) on February 11, 20205 and the International Committee on Taxonomy of Viruses (ICTV) has proposed SARS-CoV-2, the name of the virus that causes COVID-196. At present, there is no effective drug to cure the disease and the vaccine is yet to be developed. However, many clinical trials are ongoing to evaluate the treatments. As of April 15, 2020, 19,18,137 confirmed cases and 1,23,126 death cases have been reported in the world (213 countries) by WHO7. Early detection, isolation, prompt treatment, and a robust system to trace contacts are the ways to interrupt the spread of COVID-198. The most common symptoms for COVID-19 infected patients are fever, dry cough, fatigue, dyspnea and headache. However, some cases have developed various fatal complications including organ failure, septic shock, pulmonary edema, severe pneumonia, and Acute Respiratory Distress Syndrome (ARDS)9. The incubation period of COVID-19 ranges from 2-14 days. However, the mean incubation period is 5.2 days and a median duration from the onset of symptoms to death is 14 days10,11. COVID-19 infected older people, infants and patients suffering from hypertension, diabetes, cardiovascular disease, chronic respiratory disease or cancer have been shown to require special treatment and might have complications during treatment12. The outbreak initiated and started infecting the rest of the world with its epicenter in Europe and the United States apart from China.
In India, the first case of the COVID-19 was reported on January 30, 2020. A total of 12,322 cases, 1,498 recoveries (including 1 migration) and 405 deaths have been confirmed by the Ministry of Health and Family Welfare till April 15, 202013. The main reason for the spread of COVID-19 in India was due to the international travel history found among the Indians. Before the initiation of the global pandemic in India, it had already spread to a great extent in other countries. Therefore people with a travel history to abroad were quarantined for 14 days to avoid spread of coronavirus in India. The spread of COVID-19 in India started in February 2020 and it has shown an exponential increase to date.
There are four stages of the spread of coronavirus. To date, India is affected by the second stage which is a local transmission. Indian government officials and rescue teams worked hard to identify people who have come in contact with coronavirus infected patients. India is one of the most diverse countries in the world by different religious, ethnic groups, different weather conditions with the second largest population in the world. If India reaches the third stage (community transmission), it will be really difficult to trace the person who is being contacted by an infected person. The Government of India announced the lockdown on 24th March 2020 for 21 days and on 14th April 2020, it was extended till 3rd May 2020. It was one of the world’s largest lockdowns wherein 1.35 billion of the population of India was asked to stay at home as social distancing is the best measure to overcome the spread of COVID-19. Indian Council of Medical Research (ICMR) approved 151 government laboratories, 68 private laboratories and 3 collection sites for conducting the test of COVID-19 across the country as on April 15, 2020.
Data Collection
In our study, we have used two available datasets in order to analyze the various aspects of the global pandemic caused due to coronavirus. Both datasets are publicly available. Johns Hopkins University Center for Systems Science and Engineering (JHU CSSE) collected worldwide data of COVID-19 cases in three categories such as confirmed case, death case, and recovered case15. We have considered data of 185 countries and have been analyzed from January 22, 2020 to April 15, 2020 for comparing the world data with India. The second dataset has been taken from covid19india.org16. Data has been crowdsourced from reliable sources on a daily basis. This dataset is used to study confirmed cases, recovered cases, death cases and CFR of India from March 14, 2020 to April 15, 2020. Moreover, age-wise, gender-wise and state-wise data have also been analyzed and visualized. Null values have been removed by ignoring tuples and a total of 1348 cases details have been considered for age and gender analysis. Death and recovered cases are also explored by considering 224 cases.
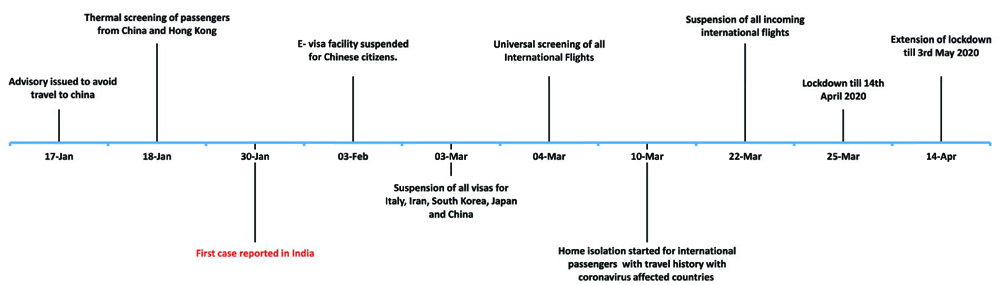
Fig. 1. the timeline of COVID-19 outbreak and the preventive measures to control the spread of COVID-19 in India from January 2020 to April 202014.
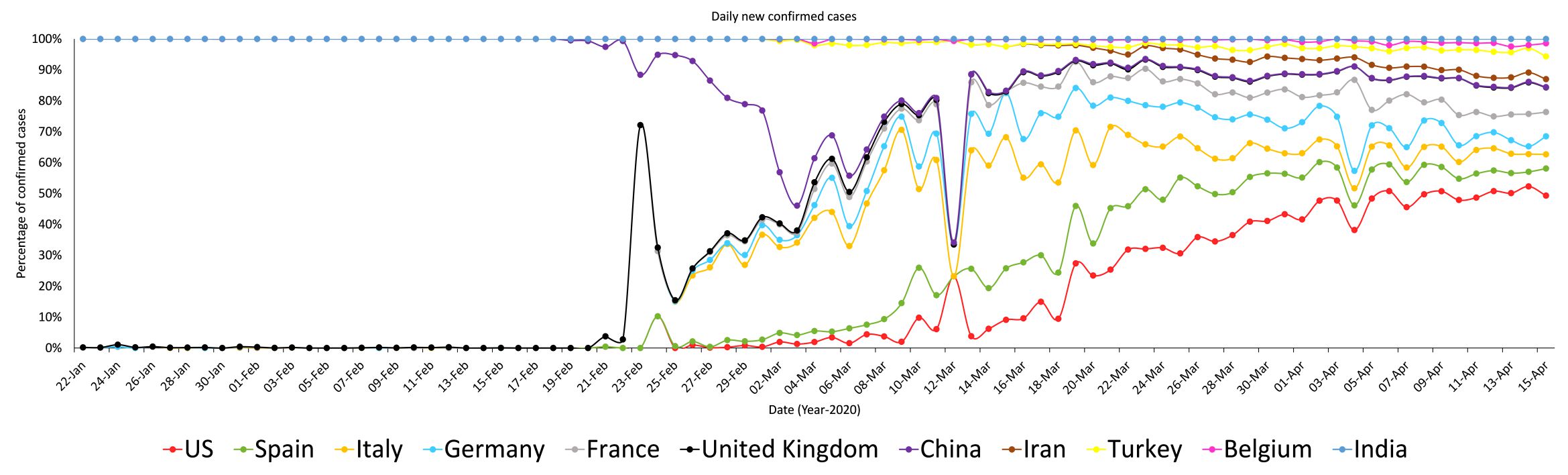
Fig. 2. Daily confirmed cases of top-10 countries in the world and India
Analysis of world COVID-19 data with India
The coronavirus has been affected epidemiologically over the world. 20,56,054 confirmed cases, 14,10,864 active cases, 5,11,019 recovered cases, 1,34,171 death cases and 6.53% CFR have been reported as of April 15, 2020, among 185 countries in the world. Fig. 2 illustrates the reported daily confirmed cases of top-10 countries in the world and India. Maximum cases were reported in China till 12th March 2020 and hence overall moderate growth is observed in the figure. Thereafter, coronavirus started spreading in the rest of the parts of the world, and then Italy became the second epicenter of this global pandemic after China. After March 19, 2020, an overall increase in the graph was observed as cases started increasing in the USA drastically. Fig. 3(A) shows the comparison of confirmed cases of India with the top-10 countries of the world as of April 15, 2020. The highest confirmed case reported by the USA were 6,36,350. Spain, Italy, France and Germany also got affected by the coronavirus severely and came in top-5 position in the world. In contrast, India reported 12,322 confirmed cases. The preemptive steps were not taken well in advance by top ten coronavirus affected countries like social distancing, lock-down, and suspension of flights from the countries affected with the deadly virus leading to the spread of COVID-19.
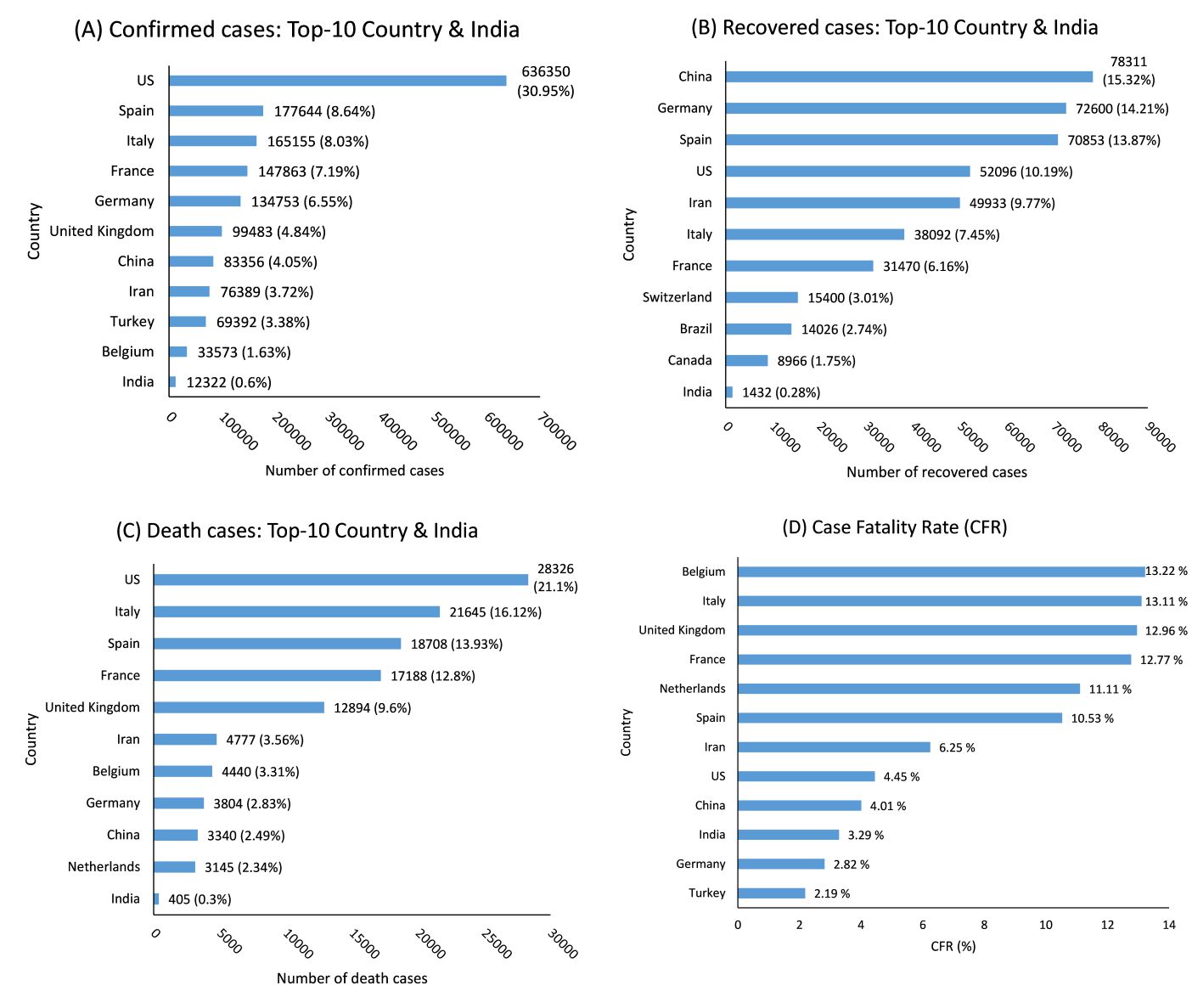
Fig. 3. Comparison of COVID-19 cases and CFR of top-10 country with India as of April 15, 2020; (A) confirmed cases, (B) recovered cases, (C) death cases, and (D) CFR.
Initially, China was the epicenter of the global pandemic. However, the recovery rate was comparatively high with respect to other countries. Medical treatment might have been excellent in Germany because it is at the fifth position in the list of top ten conformed cases as per fig. 3(A), but it was at the second position in recovery cases as per fig 3(B). India has a 0.28% recovery rate compared to the world recovery rate.
Fig. 3(C) summarizes the comparison of death cases between top-10 countries and India. India has reported only 405 death cases against its confirmed cases and the population too. COVID-19 originated from China but China has reported 3,340 death cases which is comparatively less to the top-5 counties. Total death cases of the USA (21.1%), Italy (16.12%), Spain (13.9%), France (12.8%) and UK (9.6%) have reported 73.5% compared to the total world death cases.
Case fatality rate (CFR) is the proportion of death cases by confirmed cases in a given period of time17. We have calculated the CFR rate of top-10 countries having the death cases and confirmed cases presented in fig. 3(D). Belgium and Netherlands have higher mortality compared to the number of confirmed cases in a given frame of time. Therefore, these countries are way ahead in top-10 comparison of CFR than death cases.
Analysis of COVID-19 data within India
The first case of COVID-19 in India was reported in Kerala dated 30th January 2020. The patient was a student who had a travel history from Wuhan, China. The cumulative 12,322 confirmed cases, 1,498 recovered cases, 10,419 active cases, 405 death cases and 3.29% CFR have been reported. There was a gradual increase in the number of confirmed cases till 29th March 2020 onwards in fig.4.
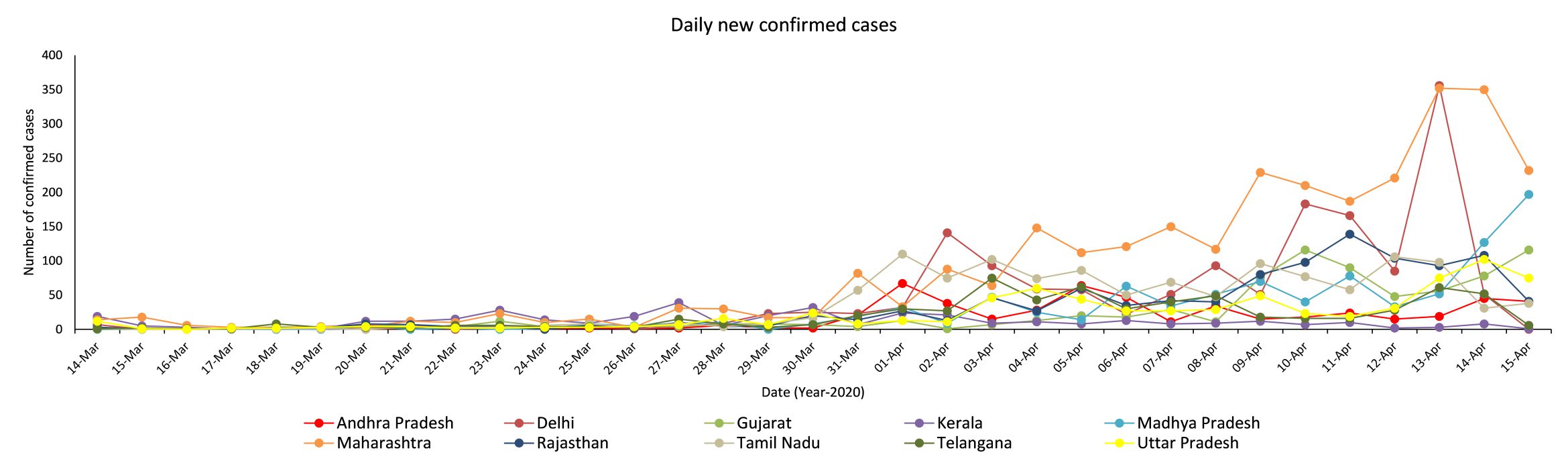
Fig. 4. Daily new confirmed cases of top-10 states of India from March 14, 2020 to April 15, 2020
After 30th March 2020, exponential growth in the number of confirmed cases was observed in India. Maharashtra, Madhya Pradesh and Delhi have reported more than 150 cases per day and after 4th April 2020, only Maharashtra reported more than 100 confirmed cases per day continually. Fig. 5(A) illustrates top-10 states of India having confirmed COVID-19 cases.
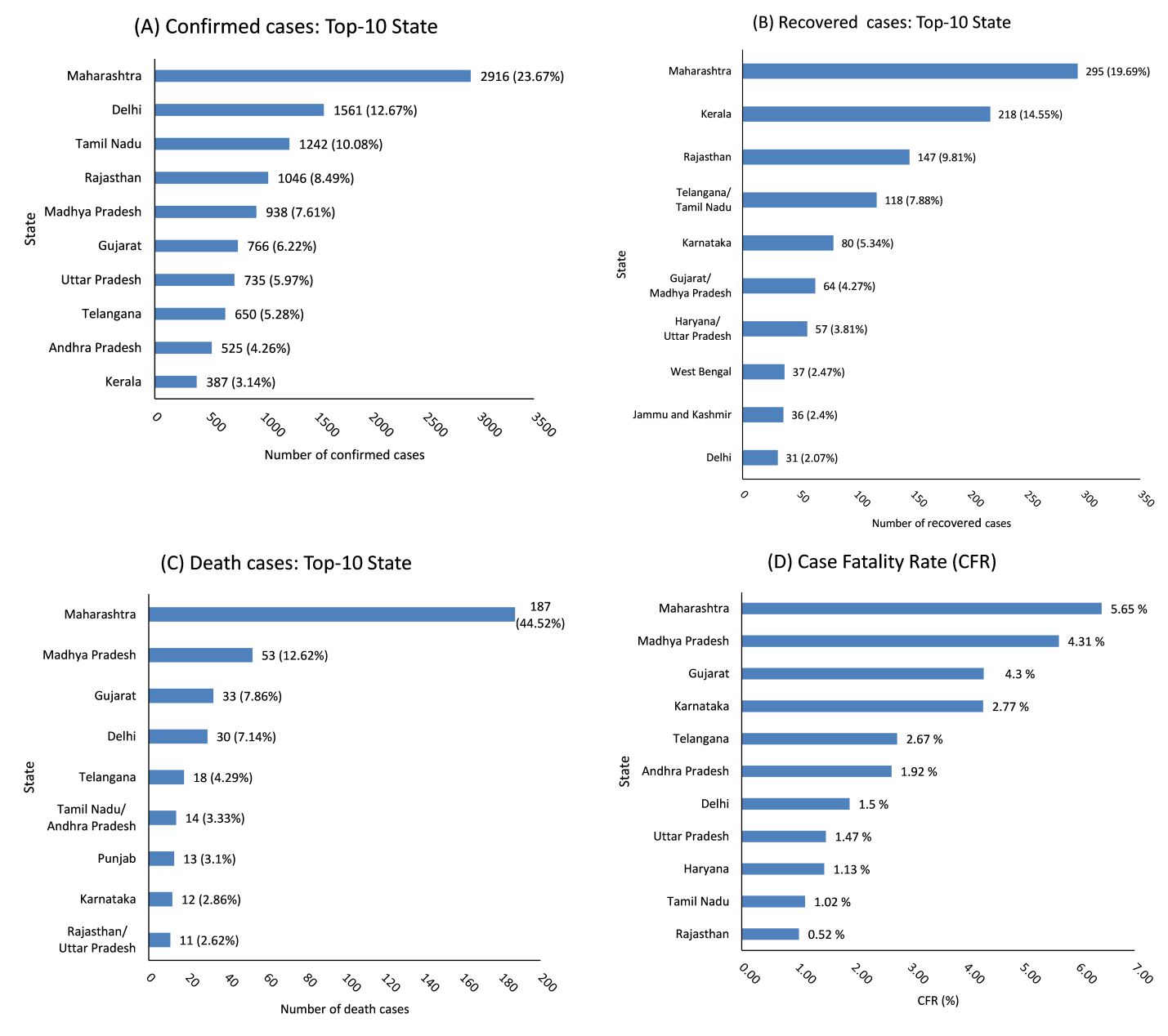
Fig. 5. Comparison of COVID-19 cases and CFR of top-10 state of India as of April 15, 2020; (A) confirmed cases, (B) recovered cases, (C) death cases, and (D) CFR.
Fig. 5(B) shows the recovered cases of the top-10 states in India. Haryana stands at 4th position in recovered cases state but it is not in top-10 states of the confirmed and death cases. Therefore, it can be regarded that Haryana did take proactive measures to prevent the spread of coronavirus.
Fig. 5(C) represents the top-10 states of India having death cases. Total death cases have been reported 405 as of April 15, 2020. Maharashtra has the highest deceased and confirmed cases in India. One possible reason could be high population density and oodles of international travelers in Mumbai compared to other cities. Fig. 5(D) represents the top-10 states of India in descending order of its CFR. Gujarat was at 10th position in the list of top ten states with confirmed cases but it was at 1st position in the list of top ten states with CFR rate in India.

Fig. 6. Age analysis; (A) Gender wise age analysis with confirmed cases, (B) Age analysis with deceased and recovered cases.
Fig. 6(A) shows the age analysis of COVID-19 confirmed cases by gender-wise. As the dataset is crowdsourced, it contains many null values. So, we have preprocessed data by eliminating rows which contain missing values in age field and remaining cases were 1,348 for gender analysis (i.e. Fig. 6(A)) and 166 cases for death and recovered analysis (i.e. Fig. 6(B)). Out of them, 952 male and 396 females have been infected by COVID-19. It is found that coronavirus infected people are more in between the age group of 26 to 52 (Q1 = 26 and Q3=52 from table. 1) and the number of infected males are greater than females. The reasons might be, this age group are mostly working people including labours who go out or migrate to other places for work and hence local transmission of the virus can be propagated. Looking after the male to female ratio in India, the males are more active and have wider social activities as compared to females.
Table (1):
Statistical analysis of COVID-19 cases for different groups.
Group |
Number of cases |
Mean ± S.D. |
Min |
P25 (Q1) |
Median |
P75 (Q3) |
Max |
Interquartile Range (IQR = Q3-Q1) |
Range |
|---|---|---|---|---|---|---|---|---|---|
Male |
952 |
39.86 ± 16.58 |
1 |
27 |
38 |
52 |
96 |
25 |
95 |
Female |
396 |
39.03 ± 19.30 |
1 |
24.5 |
36 |
53.75 |
85 |
29.25 |
84 |
All (Total of Male and Female) |
1348 |
39.66 ± 17.46 |
1 |
26 |
38 |
52 |
96 |
26 |
97 |
Deceased |
164 |
59.03 ± 13.86 |
1 |
52 |
60 |
67.5 |
86 |
15.5 |
85 |
Recovered |
60 |
40.15 ± 17.03 |
1 |
27 |
36.5 |
55 |
75 |
28 |
74 |
In our study, Table 1 summarizes the statistical analysis of different groups. One hundred twenty-five patients succumbed to diseases and 56 recovered out of 166 cases. As per the fig. 6(B), the chance of fatality is higher in geriatric people due to existing medical condition, for instance, hypertension, diabetes etc. and also due to lowered immunity when compared to younger people. It also represents that patients’ age above 81 caved into the deadly attack of coronavirus and they have a higher chance to decease.
An epidemic outbreak of COVID-19 is at the early stage in India and in a better position compared to other countries in the world. Our study shows India has reported 0.6% confirmed cases and 3.29% CFR which is a slower growth rate when compared to other countries in the world against its total population. Due to lockdown till April 14, 2020 in India, cases of community transmission were meagre and lockdown is extended till May 3, 2020, cases of local transmission will also decrease. Our study also summarizes COVID-19 cases state-wise. It has been observed that states having higher number of immigrants, were badly hit coronavirus and had maximum confirmed cases of COVID-19 such as Maharashtra, Delhi and Tamil Nadu. COVID-19 showed a higher effect on the young age group and females being less affected than male. Moreover, maximum deaths have been reported after the age of 52. The Government of India has taken the right decision of announcing lockdown at the right time of early-stage which is an appreciable and a bold step to prevent transmission of COVID-19 in India and saves so many lives in the second highest populated country in the world. Because social distancing is the only key solution to stop an outbreak of COVID-19. Finally, our analytical efforts may guide researchers for further interventions to prevent and control COVID-19 and may be helpful in preparing epidemiological models on COVID-19 data of India.
ACKNOWLEDGMENTS
We would like to thank Dr Dweepika Garg for her valuable assistance to proofread the manuscript.
CONFLICT OF INTEREST
The listed author(s) declare no conflict of interest in any capacity, including competing or financial.
AUTHORS’ CONTRIBUTION
All listed author(s) have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
ETHICS STATEMENT
This article does not contain any studies with human participants or animals performed by any of the authors.
AVAILABILITY OF DATA
Not applicable.
- H Lu, CW Stratton, Y Tang. Outbreak of pneumonia of unknown etiology in Wuhan China: the mystery and the miracle. J Med Virol. 2020;92(4):401-402.
Crossref - WHO Director-General’s opening remarks at the media briefing on COVID-19. https://www.who.int/dg/speeches/detail [ Accessed 12 April, 2020]
- Schwartz DA, Graham AL. Potential maternal and infant outcomes from (Wuhan) Coronavirus 2019-nCoV infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections. Viruses, 2020; 12(2):194.
Crossref - Ma K, Chen T, Han MF, Guo W, Ning Q. Management and clinical thinking of Coronavirus Disease 2019. Zhonghua Gan Zang Bing Za Zhi. 2020;28(0):E002. DOI: 10.3760/cma.j.issn.1007-3418.2020.0002
- World Health Organization. Coronavirus disease (COVID-19) outbreak. https://www.who.int/emergencies/diseases/novel-coronavirus-2019, Accessed 12 April, 2020.
- Gorbalenya AE, Baker SC, Baric RS et al. Severe acute respiratory syndrome-related coronavirus—the species and its viruses, a statement of the Coronavirus Study Group. BioRxiv. 2020:2020.02.07.937862.
Crossref - Coronavirus disease (COVID-19) Pandemic. https://www.who.int/emergencies/diseases/novel-coronavirus-2019, Accessed 13 April, 2020
- N Chen, M Zhou, X Dong, et al., Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet. 2020.
Crossref - C Rothe, M Schunk, P Sothmann, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N. Engl. J. Med. 2020;382:970-971.
Crossref - Wang W, Tang J, Wei F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J. Med. Virol. 2020;92:441-447.
Crossref - Coronavirus. https://www.who.int/health-topics/coronavirus, Accessed 13 April, 2020.
- Ministry of Health and Family Welfare, Government of India. https://www.mohfw.gov.in/, Accessed 14 April, 2020.
- India’s response to COVID outbreak. https://pib.gov.in/PressReleasePage.aspx?PRID=1608727 [ Accessed 14 April, 2020]
- CSSE COVID-19 Dataset. https://github.com/CSSEGISandData/COVID-19 [Accessed 10 April, 2020]
- COVID-19 India. https://covid19india.org [ Accessed 12 April, 2020]
- Case Fatality Rate. https://www.sciencedirect.com/topics/medicine-and-dentistry/case-fatality-rate [ Accessed 15 April, 2020]
© The Author(s) 2020. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.