


ISSN: 0973-7510
E-ISSN: 2581-690X
Hisham Altayb8 and Abdelbagi Alfadil1
Bacterial infections continue to pose a significant global health threat, further intensified by the increasing prevalence of antibiotic resistance. Methicillin-resistant Staphylococcus aureus (MRSA) poses significant threats, especially in healthcare settings around the world. Conventional treatments face some limitations due to development of antimicrobial resistance, emphasizing the urgent need to explore alternative treatment strategies. In this study, we propose the potential synergistic activity of thymoquinone and 3-hydrazinoquinoxaline-2-thiol (3HT) to combat MRSA infections. The minimum inhibitory concentrations (MICs) of both thymoquinone and 3HT were assessed across twenty-two clinical MRSA strains. Thymoquinone demonstrated the minimum inhibitory concentration (MIC) values range between 8 and 128 µg/ml., while 3HT exhibited MIC levels varying from 16 to 32 µg/ml. Moreover, the checkerboard-assay was utilized to evaluate the integration of the following antimicrobial agents; thymoquinone and 3HT. Thymoquinone and 3HT bind to PBP2a leading to reduction in MRSA antimicrobial resistance via significantly disrupting its structure and function. Our study reveals an in-vitro synergistic interaction between these compounds with a fractional inhibitory concentration index (FICI) less than 0.5 against different isolated MRSA strains. While further research is necessary, our findings offer a promising approach for developing new effective MRSA treatments.
MRSA, AMR, 3HT, Thymoquinone, Antimicrobial Agents, FICI
The global menace of bacterial infections persists, standing as a significant contributor to mortality and a continuing challenge amplified by the escalating problem of antibiotic resistance.1,2 MRSA is a major cause of hospital-acquired infections, leading to increased illness, longer hospital stays, and higher treatment costs. MRSA infections are classified into healthcare-associated (HA-MRSA), community-associated (CA-MRSA), and livestock-associated (LA-MRSA) types.1,3,4 Each year, 150,000 European patients contract MRSA, costing 380 million Euros; in the United State, MRSA affects 94,000, causing 18,000 deaths.4,5 Saudi Arabia faces MRSA challenges, particularly in healthcare. In Riyadh, 18% of 200 healthcare workers tested were MRSA carriers.5,6
b-lactam antibiotics are widely used, effective, and low-toxicity antimicrobials.7,8 b-lactam antibiotics act by disrupting penicillin-binding proteins in bacterial cell walls.8 MRSA resists b-lactams by acquiring the mecA gene, which encodes a low-affinity penicillin-binding protein, PBP2a.9,10
Addressing MRSA infections is challenging due to limited therapeutic options.11 Current MRSA treatments include daptomycin, linezolid, and vancomycin, each with limitations and increasing resistance reports.12-14 The resistance profile markedly reduces the available effective treatments, complicating the management of MRSA infections.11
Developing new antibiotics encounters challenges such as regulatory hurdles, financial constraints, and extensive time requirements.15,16 Urgent solutions are needed for antibiotic resistance, including new resistance targets, small molecule inhibitors, and synergistic combinations of older antibiotics.10,17,18 Combining antibiotics and repurposing old drugs are cost-effective strategies that can expedite treatment for resistant bacterial infections, saving time and money.16,19,20
Thymoquinone (Figure 1), a bioactive compound naturally found in the seeds of Nigella sativa, known as black cumin or black seed, is a naturally occurring substance.21 It has been shown that thymoquinone exhibits notable effectiveness a bactericidal effect against multiple clinical strains of MRSA.22,23 Moreover, thymoquinone displayed notable bactericidal effects against most tested bacteria, particularly against Gram-positive cocci such as Staphylococcus aureus and Staphylococcus epidermidis. Additionally, thymoquinone showed supplementation affected the cells’ oxidative activity and effectively inhibited cell adhesion to glass surfaces.24
Figure 1. Chemical structure of thymoquinone a bioactive compound extracted from the seeds of Nigella sativa
Quinoxaline derivatives have demonstrated significant antibacterial, antifungal, and antitubercular activities in various studies. Additionally, quinoxaline compounds exhibit antifungal activity against a range of pathogenic fungi, making them valuable in combating fungal infections. Moreover, these derivatives have shown promise in antitubercular activity, effectively inhibiting the growth of Mycobacterium tuberculosis. The multifaceted therapeutic potential of quinoxalines underscores their importance in developing new treatment strategies for infectious diseases.25,26 In a prior study carried out by Elfadil et al., the significant effectiveness of quinoxaline derivatives, specifically 3-Hydrazinoquinoxaline-2-Thiol (3HT) (Figure 2) was demonstrated against a wide variety of clinical strains linked to MRSA.27,28
Figure 2. The figure illustrates the chemical structure of 3-Hydrazinoquinoxaline-2-Thiol (3HT), a quinoxaline derivative
Building on this, we suggest that using quinoxaline derivatives in Combination therapy could enhance the effectiveness of 3HT targeting different clinical strains of MRSA. This innovative way builds upon previous research, offering a potential solution to the difficulties posed by MRSA infections, paving the way for more effective treatment alternatives. This paper aims to assess the in vitro efficacy of the 3HT in combination with thymoquinone against different MRSA clinical strains. The focus is on discovering potential synergy between the two antimicrobial compounds and their impact on treatment efficacy, contributing to new approaches for combating MRSA infections.
Bacterial strains, growth media and condition
This investigation comprised of the analysis of 22 MRSA bacteria obtained from King Abdulaziz University Hospital, Jeddah, Saudi Arabia. These bacteria were kept in glycerol and maintained at minus eighty centigrade. Initially, a thawing process was carried out and the tested bacteria were grown on blood agar (provided by HiMedia, India) and incubated for 20 hours at 37°C in aerobic conditions. The collection of the bacteria was adhered to the ethical guidelines set forth by the ethics and research committee of the Faculty of Applied Medical Sciences at King Abdulaziz University (No. 38-712-456) and was in accordance with the Declaration of Helsinki.
Antibacterial agents
This study evaluated drugs with a specific focus on MRSA. Among these, a 3HT compound was sourced from Fluorochem Ltd. in the UK, while thymoquinone powder was obtained from (Sigma, UK). The two agents were then dissolved in the chemical DMSO.
Antibiotic sensitivity testing (AST)
To evaluate antibiotic sensitivity, we performed a broth microdilution test. This comprises of making a serial of two-fold dilution of the antimicrobial agents being tested in MHB (Sigma-Aldrich, United States). Next, one hundred microliter of the prepared antimicrobial mixture was added to each well of 96-well plates. The bacterial suspension diluted to 0.5 McFarland utilizing a Biosan Densitometer DEN-1B to measure turbidity. Following this, 5 µl of the inoculum was introduced into each well supplemented with different antibiotic concentrations. The plates were incubated for 20 hours at 37°C. The antibiotic susceptibility tests were carried out in three times, and the average values were documented.29 The MIC is the minimum concentration of a drug that can effectively inhibit the visible growth of a microorganism. The MIC values for the 2 antibacterial agents were assessed via the broth microdilution assay and interpreted based on the standards set by the Clinical Laboratory Standards Institute (CLSI).30,31
Checkerboard-assay
In order to determine the interactions among the antimicrobial drugs, the checkerboard-assay was employed. In this method, a twofold serial dilution of each compound was prepared in MHB sourced from the company. Subsequently, fifty microliters of each dilution were added to the 96-well plates. The prepared bacteria were carefully adjusted to 0.5McFarland through a Biosan Densitometer DEN-1B for turbidity detection. Subsequently, 5 microliters of the diluted bacteria were added to the corresponding 96-wellplates.2
When assessing the synergy between the compounds 3HT and thymoquinone, the Fractional Inhibitory Concentration (FIC) was determined using the formula FIC = [MIC (3HT in combination) divided by MIC (3HT alone)] + [MIC (thymoquinone in combination) divided by MIC (thymoquinone alone)]. This computation involves comparing the MIC of the solely drugs when combined with those utilized separately. This method allows for a thorough assessing of the combined) inhibitory effect.32 The checkerboard test was conducted three times, and the average values documented for subsequent analysis.
Assessment of the interactions between the tested antimicrobial agents
Combination studies using a checkerboard design were applied to construct a matrix covering all potential dose combinations of the prepared drugs with the calculated concentration range. The interaction among the 2 drugs was quantitatively analyzed using the fractional inhibitory concentration index (FICI), computed with the formula: FICI = [(MIC A in combination) divided by MIC A] + [(MIC B in combination) divided by MIC B].
The interpretation of FICI results can be determined if the values less than or equal to 0.5 indicate synergy, those greater than 0.5 but not exceeding 1 signify an additive effect, values above 1 but not exceeding 2 suggest indifference, and values surpassing 2 indicate antagonism. In practice, synergy according to this calculation means a reduction in the MIC of each drug by at least two dilution levels when the two drugs are used together.33
Molecular docking
Docking studies were conducted using Maestro, protein structure of penicillin G acyl-PBP2a from MRSA (PBP2a) was acquired from PDB database (https://www.rcsb.org/structure/1MWT). Thymoquinone and 3-hydrazinoquinoxaline-2-thiol compounds, were obtained from PubChem database.34 Prior docking process both protein and compounds were prepared, then SiteMap tool within the Maestro suite that identifies and characterizes potential binding sites on the surface of a protein. The binding is determined according to previous publication.35,36 The best docking configuration was chosen based on the docking pose with the lowest binding free energy between the ligand and receptor.
Evaluating the MICs of both 3HT and thymoquinone
Determining the MICs of both 3HT and thymoquinone is crucial before proceeding with the checkerboard-assay. The MIC levels for thymoquinone, as presented in Table 1, range from 8 to 128 µg/ml. Similarly, the MIC levels for 3HT range from 16 to 32 µg/ml (Table 1). Once these MICs were obtained, a checkerboard test was then devised, blending varying amounts of thymoquinone and 3HT.
Table (1):
The MICs of 3HT and thymoquinone (μg/ml) for a variety of MRSA strains
MRSA strain number |
MIC of 3HT |
MIC of thymoquinone |
|---|---|---|
1 |
32 |
16 |
2 |
32 |
16 |
3 |
32 |
16 |
80 |
32 |
16 |
95 |
32 |
32 |
93 |
32 |
16 |
90 |
16 |
32 |
92 |
32 |
32 |
91 |
32 |
32 |
100 |
32 |
32 |
101 |
16 |
32 |
96 |
32 |
32 |
98 |
16 |
8 |
97 |
16 |
32 |
107 |
16 |
32 |
102 |
32 |
32 |
105 |
32 |
128 |
106 |
32 |
32 |
104 |
32 |
32 |
72 |
32 |
64 |
73 |
16 |
32 |
75 |
32 |
16 |
Synergy of 3HT and thymoquinone against different MRSA clinical strains
A checkerboard-test was carried out to examine the efficacy of combining 3HT and thymoquinone against various MRSA clinical strains. Thymoquinone on its own was shown to be inadequate in suppressing MRSA growth. Nonetheless, a significant monitoring was made when thymoquinone was joined with 3HT: the MICs of thymoquinone significantly decreased, with decreases ranging from 4 to 128 folds across all tested MRSA strains. Similarly, the MICs of 3HT notably decreased in combination with thymoquinone, showing reductions of 4 to 64-fold against the tested MRSA strains (Figure 3). This suggests that 3HT can enhance the effectiveness of thymoquinone against MRSA strains (Table 2).
Table (2):
The interaction between 3HT and thymoquinone against various MRSA clinical strains in vitro. The FICI values less than or equal to 0.5 indicate synergy, those greater than 0.5 but not exceeding 1 signify an additive effect, values above 1 but not exceeding 2 suggest indifference, and values surpassing 2 indicate antagonism
MRSA strain |
FIC of 3HT |
FIC of thymoquinone |
FICI of 3HT+thymoquinone |
|---|---|---|---|
MRSA 1 |
0.125 |
0.25 |
0.375 synergy |
MRSA 2 |
0.25 |
0.031 |
0.281 synergy |
MRSA 3 |
0.125 |
0.25 |
0.375 synergy |
MRSA 80 |
0.25 |
0.062 |
0.312 synergy |
MRSA 95 |
0.145 |
0.208 |
0.353 synergy |
MRSA 93 |
0.208 |
0.114 |
0.322 synergy |
MRSA 90 |
0.125 |
0.167 |
0.292 synergy |
MRSA 92 |
0.25 |
0.124 |
0.374 synergy |
MRSA 91 |
0.167 |
0.125 |
0.292 synergy |
MRSA 100 |
0.114 |
0.208 |
0.322 synergy |
MRSA 101 |
0.25 |
0.187 |
0.437 synergy |
MRSA 96 |
0.25 |
0.146 |
0.396 synergy |
MRSA 98 |
0.27 |
0.145 |
0.415 synergy |
MRSA 97 |
0.208 |
0.169 |
0.377 synergy |
MRSA 107 |
0.333 |
0.065 |
0.398 synergy |
MRSA 102 |
0.208 |
0.073 |
0.281 synergy |
MRSA 105 |
0.25 |
0.054 |
0.304 synergy |
MRSA 106 |
0.208 |
0.105 |
0.313 synergy |
MRSA 104 |
0.016 |
0.25 |
0.266 synergy |
MRSA 72 |
0.093 |
0.123 |
0.216 synergy |
MRSA 73 |
0.25 |
0.008 |
0.258 synergy |
MRSA 75 |
0.08 |
0.12 |
0.2 synergy |
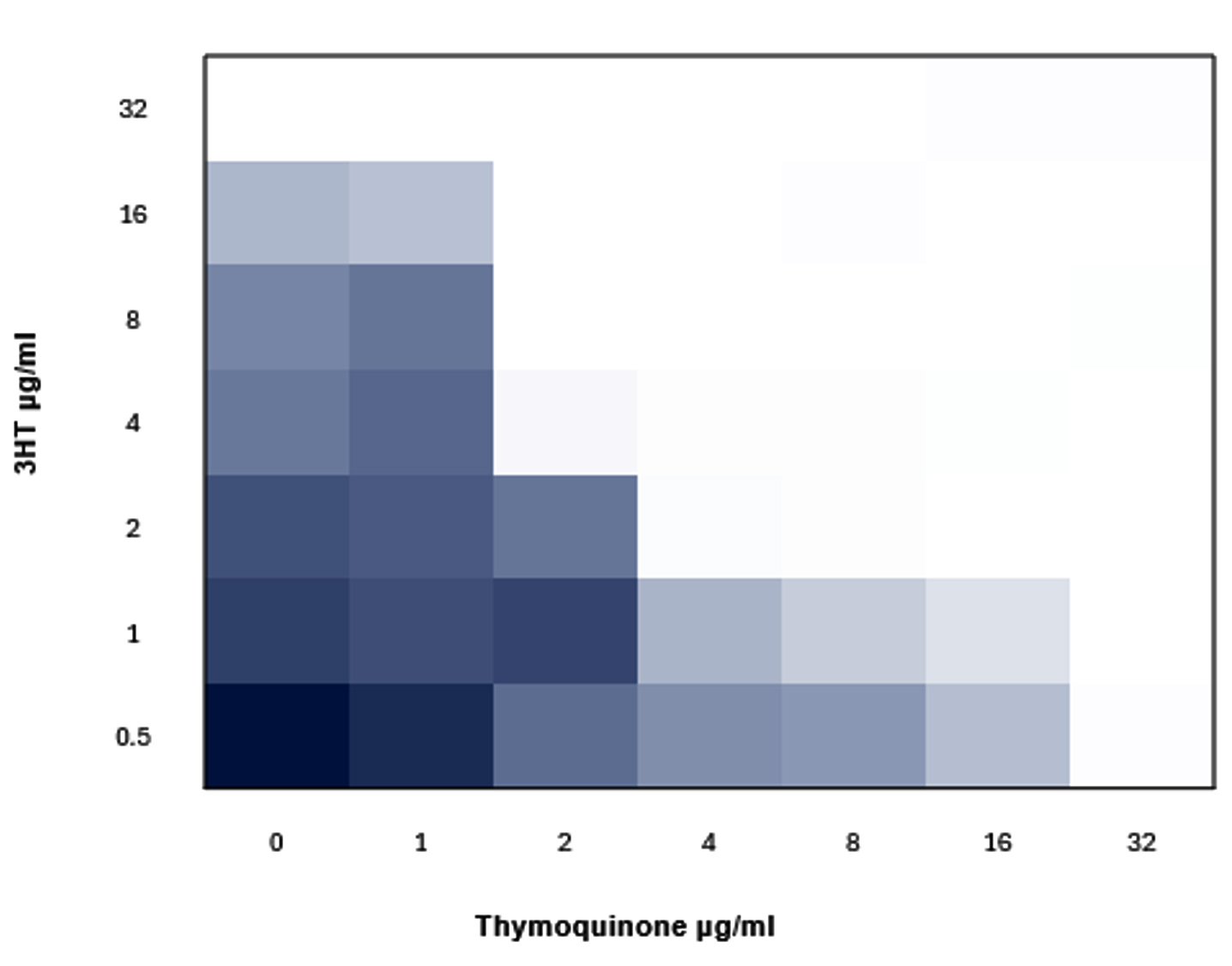
Figure 3. Checkerboard-assay illustrates the synergism action of 3HT combined with thymoquinone against MRSA 91. The blue color indicates growth and the white color represent no growth
Binding potential of thymoquinone and 3HT to PBP2a
Both thymoquinone and 3-hydrazinoquinoxaline-2-thiol have been examined for their potential to bind to PBP2a, a protein known to cause antibiotic resistance in MRSA. The XP scores, which indicate docking efficacy, are -3.8 for Thymoquinone and slightly higher at -4.1 for 3-hydrazinoquinoxaline-2-thiol, indicating a slightly stronger docking interaction for the latter. Both compounds had the same MMGBSA score of -16 (Table 3), indicating a similar binding energy and possible stability of the complex formed with PBP2a. This implies that both compounds could be regarded possible inhibitors of PBP2a, contributing to efforts against MRSA infections.
Table (3):
Docking and binding energy generated from the interaction of Thymoquinone and 3HT with PBP2a from methicillin resistant S. aureus (MRSA)
Compound |
PubChem ID |
Structure |
XP score |
MMGBSA |
|---|---|---|---|---|
Thymoquinone |
10281 |
 |
-3.8 |
-16 |
3-HT (hydrazinoquinoxaline-2-thiol) |
781248 |
 |
-4.1 |
-16 |
Thymoquinone and 3-hydrazino-quinoxaline-2-thiol administration causes considerable structural changes in PBP2a, a protein linked to methicillin resistance in S. aureus. PBP2a’s pocket volume was initially reported at 442.470 ų. Docking 3-hydrazinoquinoxaline-2-thiol alone results in a volume drop to 390.334 ų, indicating a significant occupancy and probable modification in the protein structure. Docking both compounds at the same time results in a significant decrease in pocket volume to 66.199 ų (Table 3, Figures 4-6).
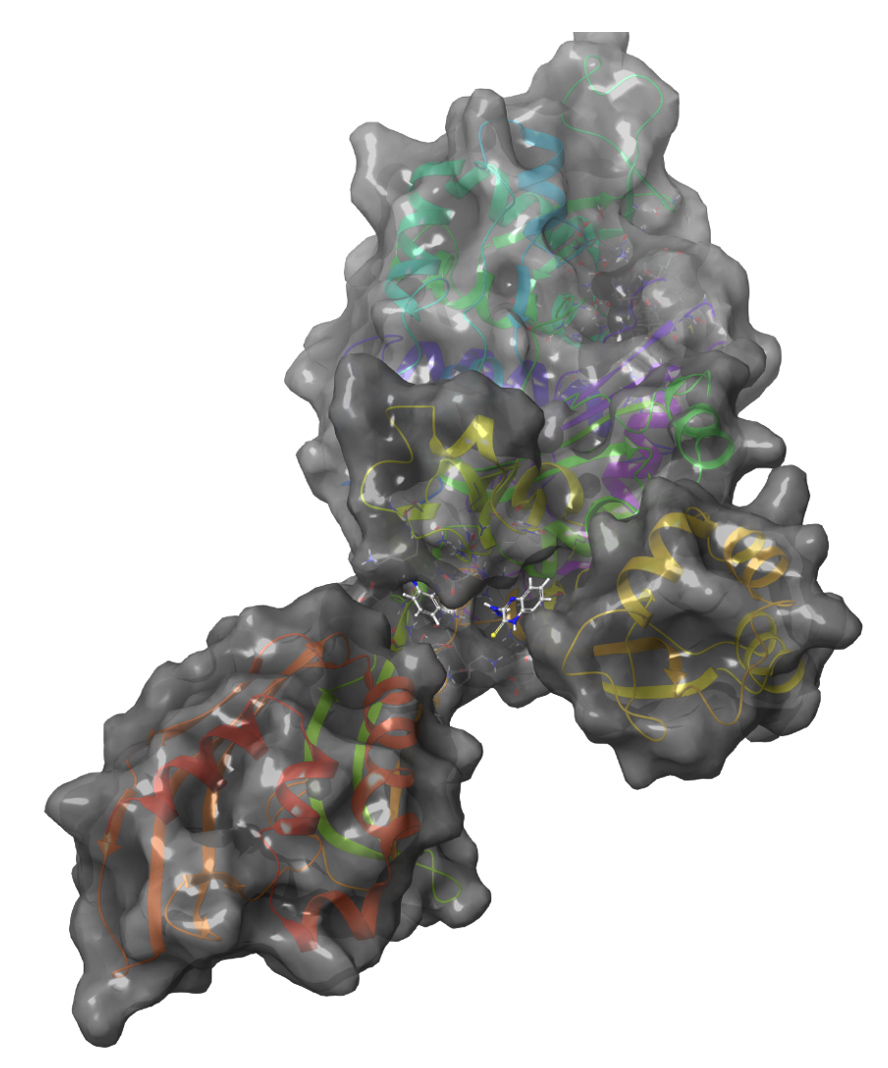
Figure 4. 3D structure of PBP2a from MRSA, showing the binding site blocked by the Thymoquinone (left) and 3-hydrazinoquinoxaline-2-thiol (right)
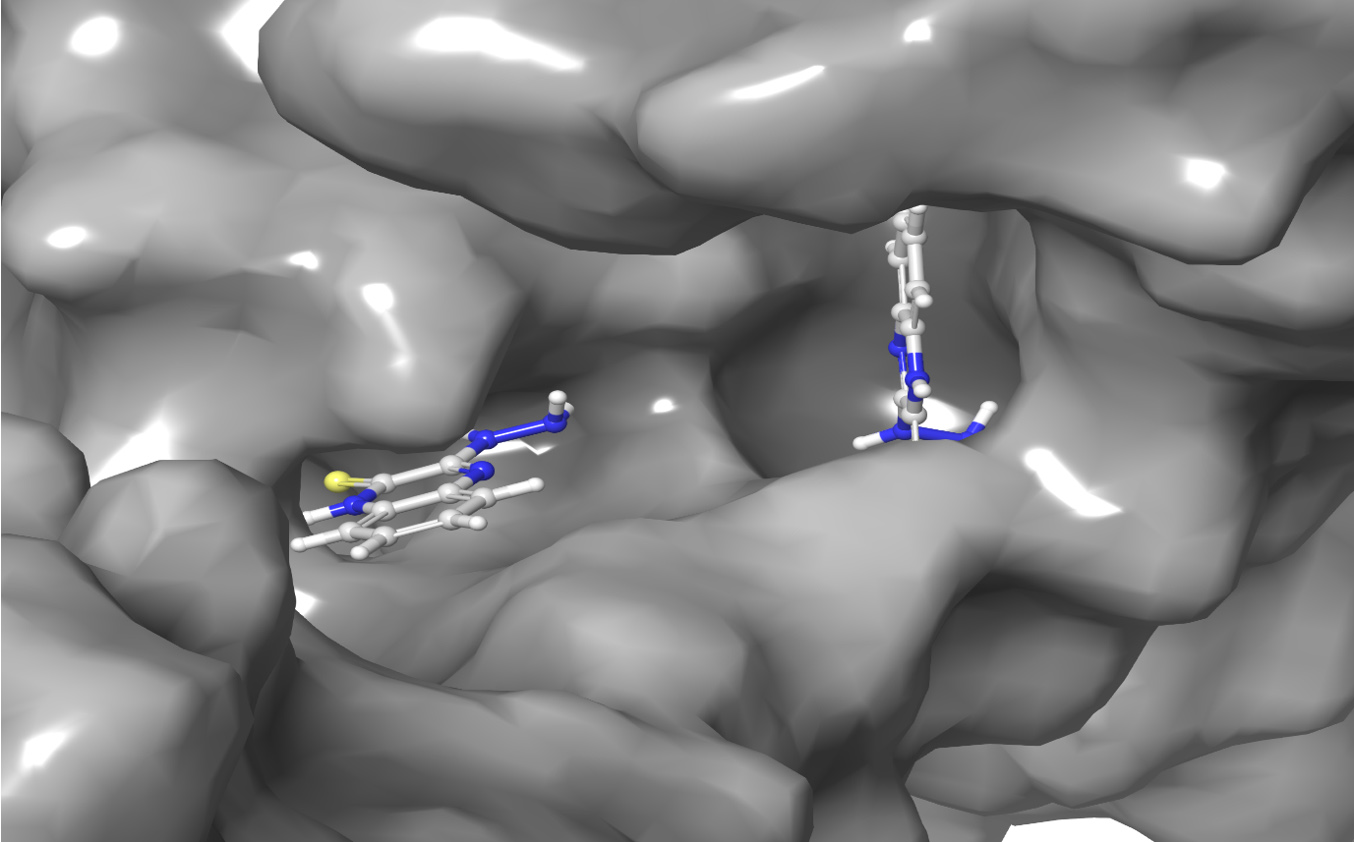
Figure 5. Enlarged view of the interaction of 3HT (left) and Thymoquinone (right), with PBP2a from methicillin resistant S. aureus (MRSA)

Figure 6. Detailed interaction of 3HT (A) and Thymoquinone (B), with PBP2a from methicillin resistant S. aureus (MRSA). Showing the hydrogen bonds in blue and hydrophobic bonds in grey
This significant drop shows a synergistic effect of the compounds, which could lead to a strong suppression of PBP2a functionality. Such a large change may impair the protein’s capacity to connect with natural substrates or other compounds that promote bacterial resistance, thereby re-sensitizing MRSA to methicillin. The findings highlight the therapeutic potential of these chemicals, implying that they could play an important role in overcoming bacterial resistance. Further research, such as kinetic studies and molecular dynamics simulations, would be advantageous in fully understanding binding kinetics and experimentally validating computational predictions. This could pave the door for new antibacterial techniques to combat resistant bacterial strains.
Table (4):
Hydrogen Bonds generated from interaction of 3HT and Thymoquinone with PBP2a
| Compound | Index | Residue | AA | Distance H-A | Distance D-A | Donor Angle | Donor Atom | Acceptor Atom |
|---|---|---|---|---|---|---|---|---|
| 3-hydrazinoquinoxaline-2-thiol | 1 | 277A | VAL | 2.98 | 3.89 | 157 | 8194 [O3] | 20438 [N3] |
| 2 | 277A | VAL | 1.86 | 2.86 | 176.47 | 8188 [N3] | 20423 [O2] | |
| 3 | 292A | GLN | 2.08 | 3.02 | 152.52 | 20437 [Npl] | 8726 [O2] | |
| 4 | 292A | GLN | 2.99 | 3.47 | 112.1 | 8731 [O3] | 20438 [N3] | |
| 5 | 293A | HIS | 2.9 | 3.85 | 165.04 | 8755 [O3] | 20438 [N3] | |
| 6 | 293A | HIS | 2.07 | 2.97 | 146.52 | 20438 [N3] | 8762 [N3] | |
| 7 | 293A | HIS | 2.75 | 3.21 | 108.19 | 8762 [N3] | 20423 [O2] | |
| 8 | 293A | HIS | 2.75 | 3.21 | 108.19 | 8768 [N3] | 20423 [O2] | |
| 9 | 294A | GLU | 3.09 | 3.94 | 147.17 | 8794 [O3] | 20435 [Nam] | |
| 10 | 294A | GLU | 3.12 | 3.94 | 139.04 | 20435 [Nam] | 8794 [O3] | |
| 11 | 295A | ASP | 2.04 | 2.85 | 134.91 | 8813 [N3] | 20422 [O2] | |
| 12 | 295A | ASP | 1.89 | 2.85 | 159.41 | 8814 [N3] | 20422 [O2] | |
| Thymoquinone | 1 | 277A | VAL | 1.86 | 2.86 | 176.47 | 4094 [Nam] | 10213 [O2] |
| 2 | 295A | ASP | 1.89 | 2.85 | 159.41 | 4407 [Nam] | 10212 [O2] |
Tables 3 and 4 provide specific information about the molecular interactions of 3-hydrazinoquinoxaline-2-thiol, thymoquinone, and the PBP2a enzyme. Table 4 details the hydrogen bonds produced during these interactions, demonstrating how each drug interacts with specific amino acids in PBP2a. For example, 3-hydrazinoquinoxaline-2-thiol forms several hydrogen bonds with residues such as VAL, GLN, HIS, and GLU (Figure 6A), indicating strong contact locations that may impair the protein’s functionality. The hydrogen bonds’ distances range from 1.86 Å to 3.12 Å, with donor angles indicating successful binding. Thymoquinone, although interacting through fewer hydrogen bonds, exhibits a comparable pattern of significant contact with VAL and ASP residues (Figure 6B), indicating a particular interaction that could affect the protein’s activity. These contacts are distinguished by identical distances and angles, indicating a precise docking orientation suitable for efficient binding. Table 3 shows the hydrophobic interactions that contribute to the stability of compound-protein complexes. Both compounds interact primarily with residues such as LYS, ALA, GLU, and ASP. These hydrophobic bonds are close together, with distances ranging from 3.18 Å to 3.92 Å, potentially contributing to binding affinity (Table 5).
Table (5):
Hydrophobic bonds generated from interaction of 3HT and Thymoquinone with PBP2a
| Compound | Index | Residue | AA | Distance | Ligand Atom | Protein Atom |
|---|---|---|---|---|---|---|
| 3-hydrazinoquinoxaline-2-thiol | 1 | 273A | LYS | 3.91 | 20426 | 8085 |
| 2 | 273A | LYS | 3.18 | 20427 | 8084 | |
| 3 | 275A | ASP | 3.92 | 20444 | 8152 | |
| 4 | 276A | ALA | 3.89 | 20426 | 8175 | |
| 5 | 276A | ALA | 3.65 | 20429 | 8169 | |
| 6 | 293A | HIS | 3.75 | 20430 | 8761 | |
| 7 | 294A | GLU | 3.68 | 20424 | 8785 | |
| 8 | 294A | GLU | 3.85 | 20442 | 8792 | |
| 9 | 295A | ASP | 3.68 | 20446 | 8821 | |
| Thymoquinone | 1 | 273A | LYS | 3.91 | 10216 | 4044 |
| 2 | 273A | LYS | 3.18 | 10217 | 4043 | |
| 3 | 276A | ALA | 3.89 | 10216 | 4088 | |
| 4 | 294A | GLU | 3.78 | 10214 | 4396 |
To our knowledge, this paper represents the initial documentation of a synergistic interaction between thymoquinone and 3HT derivatives against various MRSA clinical strains. Notably, different MRSA strains showed varied MIC in response to thymoquinone or 3HT. Uncovering this remarkable interaction not only enhances our knowledge of MRSA therapeutics but also suggests an encouraging pathway for mitigating antibiotic resistance in this specific context. Previous study has demonstrated that the combining of thymoquinone and Augmentin exhibits a synergistic effect versus different clinical strains of MRSA. Our findings are consistent with these observations, as they also indicate that thymoquinone can enhance the effectiveness of antibiotic Augmentin.37 However, this study expands upon this by revealing that thymoquinone similarly synergizes with 3HT, suggesting its chance to enhance the activity of beta-lactam antibiotics and other compounds possessing antimicrobial properties.
The concurrent administration of thymoquinone and 3HT led to a remarkable decrease in MIC, with decreases of up to 128-fold observed. Similarly, a clear effect was noticed when thymoquinone was administered alongside 3HT, resulting in a notable reduction in the MIC of the 3HT derivatives themselves. This robust synergistic interaction between 3HT and thymoquinone was consistently demonstrated across experiments involving various clinical MRSA strains. These results may strongly suggest that the combination of therapeutic approach with thymoquinone and 3HT can provide a significant antimicrobial response against MRSA strains; however, in vivo studies are required to further investigate the synergistic effect of 3HT and thymoquinone.
The addition of a second antibiotic to the treatment regimen could overcome the shortcomings of the initial antibiotic, as proposed in earlier studies.38 Our research aligns with this idea and presents strong evidence. When given alone, thymoquinone was ineffective at inhibiting the growth of MRSA at a lower MIC. However, in combination with 3HT, it exhibited can inhibit MRSA growth with lower MIC. This outcome highlights the synergistic interaction between thymoquinone and 3HT, emphasizing its potential as a combination therapy for addressing challenges associated with MRSA infections.
Given the potential toxicity linked to elevated concentrations of 3HT, thymoquinone, and other drugs, there is an emerging strategy to address this concern by utilizing reduced doses of each drug synergistically.33 Our study demonstrated that while thymoquinone alone needed 64 µg/ml in inhibiting the growth of certain MRSA strains, only 4 µg/ml of thymoquinone displayed effective in inhibiting the growth of the same MRSA strain when used in combination with 3HT. This finding indicates that similar therapeutic results can be attained with reduced drug doses, which may help lower of seriousness of the side effects. However, more investigations are crucial to confirm and expand upon this encouraging observation. Our findings align with previous studies demonstrating that thymoquinone has the potential to boost the anti-staphylococcal effects of oxacillin, penicillin, and tetracycline, particularly against specific strains.39 The effectiveness of thymoquinone has been demonstrated against Klebsiella pneumoniae and Proteus vulgaris.40,41 We suggest that combining antimicrobial therapies may broaden the spectrum of coverage, although additional tests are requisite to substantiate this claim.
Our research demonstrates the synergistic impact of the 3HT and thymoquinone combination on diverse clinical MRSA strains. This observed synergy can be attributed to various mechanisms that involve the suppression through distinct signaling pathways. Thymoquinone can inhibit the bacteria by producing unreversible harm to bacterial morphology, including the disruption of cell membrane intactness, protein loss, and interference with intracellular proteins.42 On the other hand, 3HT has been revealed to act an essential function in inhibiting DNA synthesis.43 By impeding the synthesis of DNA, 3HT adds another layer of effectiveness in controlling the proliferation and survival of MRSA strains. The interaction of mechanisms of action in combination therapy is considered as a comprehensive approach to addressing MRSA infections. Hence, we propose that the observed synergistic effect emerges from simultaneously addressing MRSA through different pathways.
A different reason for the heightened effectiveness of the thymoquinone and 3HT combination against diverse MRSA strains might be attributed to the enhanced creation of reactive oxygen species (ROS). The ROS interfere with cellular electron transport, resulting in sustained oxidative stress and eventual cell demise. Numerous studies support the notion that thymoquinone can induce ROS formation, playing a pivotal role in eliminating bacterial cells.44,45 Conversely, there is a suggestion that thymoquinone could potentially inhibit PBPs, known for staphylococcal resistance.40 Therefore, we propose that the reduction in b-lactam resistance factors, such as PBP2A in MRSA using antibiotic combination, potentially implies a modulation in protein expression. This modulation may render MRSA more susceptible to the combined antibiotic effect. A proteomic study will be helpful to confirm this speculation.
Thymoquinone and 3HT were evaluated for their ability to bind to PBP2a, a protein associated with MRSA resistance. The docking efficacy scores were -3.8 for thymoquinone and -4.1 for 3-hydrazinoquinoxaline-2-thiol, with both compounds showing similar binding energy (-16 MMGBSA score). These compounds cause significant structural changes in PBP2a, with a notable reduction in pocket volume from 442.470 ų to 66.199 ų when both compounds are docked simultaneously, indicating a synergistic effect. Such a large change may impair the protein’s capacity to connect with natural substrates or other compounds that promote bacterial resistance, thereby re-sensitizing MRSA to methicillin. This suggests that they could be effective inhibitors of PBP2a, potentially re-sensitizing MRSA to methicillin. The current findings highlight the therapeutic potential of these chemicals, implying that they could play an important role in overcoming bacterial resistance. Further research, such as kinetic studies and molecular dynamics simulations, are recommended and advantageous in fully understanding binding kinetics and experimentally validating computational predictions. This could pave the door for new antibacterial techniques to combat antimicrobial resistant bacteria.
Additional assays and tests are imperative to deepen our understanding of the synergistic interaction between thymoquinone and 3HT against MRSA. This includes the need for a mechanistic study to uncover the fundamental mechanisms through which these agents collaborate against diverse clinical MRSA strains. Such insights would pave the way for the development of further effective combinations. Additionally, it is crucial to evaluate whether the synergistic interaction between thymoquinone and 3HT against MRSA can be extrapolated to other organisms such as Staphylococcus epidermidis, Pseudomonas aeruginosa, Klebsiella pneumoniae, and other resistant strains, or if its efficacy is specific to MRSA. Notably, the antibiofilm activity of thymoquinone was most pronounced against P. aeruginosa ATCC 14886.45 This observation prompts further investigation into the combined efficacy of thymoquinone and 3HT against MRSA-producing biofilm. A set of crucial experiments is imperative. Initially, performing a Time-Kill assay is vital to thoroughly scrutinize the bactericidal effects of the thymoquinone and 3HT in combination, offering insights into its chance as a therapeutic way over a specified duration.2 On the other hand, a resistance assay is crucial to evaluate the probability of bacteria evolving resistance to the combination, ensuring its sustained effectiveness.33 The inclusion of an in vivo model becomes essential to investigate the combination’s efficacy in a living organism, providing valuable insights into its behavior within the body in terms of pharmacokinetics and pharmacodynamics and its interaction with bacteria.46,47
Our study provides the initial evidence of synergy between 3HT and thymoquinone against diverse MRSA strains. While the findings indicate possible clinical applications, more assays and experiments, including biofilm assay, time-kill assay, mechanistic study and in vivo studies, are essential to optimize dosing, guarantee safety and evaluate the effectiveness of new treatment products under real-life conditions.
ACKNOWLEDGMENTS
The authors would like to acknowledge and appreciate the dedicated team at the Department of Clinical Microbiology Laboratory, King Abdulaziz University Hospital, for their indispensable support in supplying the bacterial isolates crucial for our study.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Ethics and Research Committee of the Faculty of Applied Medical Sciences at King Abdulaziz University (No. 38-712-456) and was in accordance with the Declaration of Helsinki.
- Lee AS, de Lencastre H, Garau J, et al. Methicillin-resistant Staphylococcus aureus. Nat Rev Dis Prim. 2018;4(1):18033.
Crossref - Hu Y, Liu Y, Coates A. Azidothymidine produces synergistic activity in combination with colistin against antibiotic-resistant Enterobacteriaceae. Antimicrob Agents Chemother. 2019;63(1):e01630.
Crossref - Cuny C, Wieler LH, Witte W. Livestock-Associated MRSA: the Impact on Humans. Antibiotics. 2015;4(4):521-543.
Crossref - Kock R, Becker K, Cookson B, et al. Methicillin-resistant Staphylococcus aureus (MRSA): burden of disease and control challenges in Europe. Euro Surveill. 2010;15(41):19688.
Crossref - Frana TS, Beahm AR, Hanson BM, et al. Isolation and Characterization of Methicillin-Resistant Staphylococcus aureus from Pork Farms and Visiting Veterinary Students. PLoS One. 2013;8(1):e53738.
Crossref - Zowawi HM. Antimicrobial resistance in Saudi Arabia: An urgent call for an immediate action. Saudi Med J. 2016;37(9):935-940.
Crossref - Thakuria B, Lahon K. The Beta Lactam Antibiotics as an Empirical Therapy in a Developing Country/ : An Update on Their Current Status and Recommendations to Counter the Resistance against Them. J Clin Diagnostic Res. 2013;7(6):1207-1214.
Crossref - Bush K, Bradford PA. b-Lactams and b-lactamase inhibitors: an overview. Cold Spring Harb Perspect Med. 2016;6(8):a025247.
Crossref - Reygaert WC. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018;4(3):482-501.
Crossref - Lee SH, Wang H, Labroli M, et al. TarO-specific inhibitors of wall teichoic acid biosynthesis restore b-lactam efficacy against methicillin-resistant staphylococci. Sci Transl Med. 2016;8(329):329ra32.
Crossref - Meyer E, Schwab F, Gastmeier P. Nosocomial methicillin resistant Staphylococcus aureus pneumonia-epidemiology and trends based on data of a network of 586 German ICUs (2005-2009). Eur J Med Res. 2010;15(12):514-524.
Crossref - Kristich CJ, Rice LB, Arias CA. Enterococcal Infection – Treatment and Antibiotic Resistance, Enterococci From commensals to Lead. causes drug Resist. Enterococci: From Commensals toLeading Causes of Drug Resistant Infection. 2014:1-62.
- Nguyen HM, Graber CJ. Limitations of antibiotic options for invasive infections caused by methicillin-resistant Staphylococcus aureus: is combination therapy the answer?. J Antimicrob Chemother. 2009;65(1):24-36.
Crossref - Davis JS, van Hal S, Tong SYC. Combination antibiotic treatment of serious methicillin-resistant Staphylococcus aureus infections. Semin Respir Crit Care Med. 2015;36(1):3-16.
Crossref - Ventola CL. The Antibiotic Resistance Crisis Part 1: Causes and Threats. Pharm Ther. 2015;40(4):277-283, 2015.
- Boyd NK, Teng C, Frei CR. Brief Overview of Approaches and Challenges in New Antibiotic Development: A Focus On Drug Repurposing. Front Cell Infect Microbiol. 2021;11:1-12.
Crossref - Ba X, Harrison EM, Lovering AL, et al. Old drugs to treat resistant bugs: Methicillin-resistant Staphylococcus aureus isolates with mecC are susceptible to a combination of penicillin and clavulanic acid. Antimicrob Agents Chemother. 2015;59(12):7396-7404.
Crossref - Farha MA, Leung A, Sewell EW, et al. Inhibition of WTA synthesis blocks the cooperative action of pbps and sensitizes MRSA to b-lactams. ACS Chem Biol. 2013;8(1):226-233.
Crossref - Ramo-Garcia S, Ng C, Anderson H, et al. Synergistic drug combinations for tuberculosis therapy identified by a novel high-throughput screen. Antimicrob Agents Chemother. 2011;55(8):3861-3869.
Crossref - Safavi A, Sabourian R, Foroumadi A. Treatment of Helicobacter pylori infection: Current and future insights. World J Clin Cases. 2016;4(1):5.
Crossref - Amin B, Hosseinzadeh H. Black Cumin (Nigella sativa) and Its Active Constituent, Thymoquinone: An Overview on the Analgesic and Anti-inflammatory Effects. Planta Med. 2016;82(1-2):8-16.
Crossref - Hariharan P, Paul-Satyaseela M, Gnanamani A. In vitro profiling of antimethicillin-resistant Staphylococcus aureus activity of thymoquinone against selected type and clinical strains. Lett Appl Microbiol. 2016;62(3):283-289.
Crossref - Mouwakeh A, Kincses A, Nove M, et al. Nigella sativa essential oil and its bioactive compounds as resistance modifiers against Staphylococcus aureus. Phyther Res. 2019;33(4):1010-1018.
Crossref - Chaieb K, Kouidhi B, Jrah H, Mahdouani K, Bakhrouf A. Antibacterial activity of Thymoquinone, an active principle of Nigella sativa and its potency to prevent bacterial biofilm formation. BMC Complement. Altern. Med. 2011;11:29.
Crossref - Carta A, Paglietti G, Nikookar MER, Sanna P, Sechi L, Zanetti S. Novel substituted quinoxaline 1,4-dioxides with in vitro antimycobacterial and anticandida activity. Eur J Med Chem. 2002;37(5):355-366, 2002.
Crossref - Bazuhair MA, Alsieni M, Abdullah H, et al. The Combination of 3-Hydrazinoquinoxaline-2-Thiol with Thymoquinone Demonstrates Synergistic Activity Against Different Candida Strains. Infect Drug Resist. 2024;17:2289-2298.
Crossref - Elfadil A, Alzahrani AM, Abdullah H, et al. Evaluation of the Antibacterial Activity of Quinoxaline Derivative Compound Against Methicillin-Resistant Staphylococcus aureus. Infect Drug Resist. 2023;16:2291-2296.
Crossref - Elfadil A, Ibrahem K, Abdullah H, Mokhtar JA, Al-Rabia MW, Mohammed HA. Synergistic Activity of 3-Hydrazinoquinoxaline-2-Thiol in Combination with Penicillin Against MRSA. Infect Drug Resist. 2024;17:355-364.
Crossref - Mikkelsen K, Sirisarn W, Alharbi O, et al. The Novel Membrane-Associated Auxiliary Factors AuxA and AuxB Modulate b-lactam Resistance in MRSA by stabilizing Lipoteichoic Acids. Int J Antimicrob Agents. 2021;57(3):106283.
Crossref - Tan CM, Therien AG, Lu J, et al. Restoring methicillin-resistant Staphylococcus aureus susceptibility to β-lactam antibiotics. Sci Transl Med. 2012;4(126):126ra35.
Crossref - Clinical and Laboratory Standards Institute. 2018. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; approved standard—10th ed. M07-A11. Clinical and Laboratory Standards Institute, Wayne, PA.
- Liu X, Pai PJ, Zhang W, et al. Proteomic response of methicillin- resistant S . aureus to a synergistic antibacterial drug combination/ : a novel erythromycin derivative and oxacillin. Sci Rep. 2016;25(6):1-12, 2016.
Crossref - Gonzales PR, Pesesky MW, Bouley R, et al. Synergistic, collaterally sensitive b-lactam combinations suppress resistance in MRSA. Nat Chem Biol. 2015;11(11):855-861.
Crossref - Kim S, Thiessen PA, Bolton EE, et al. PubChem substance and compound databases. Nucleic Acids Res. 2016;44(D1):D1202-D1213.
Crossref - Otarigho B, Falade MO. Computational Screening of Approved Drugs for Inhibition of the Antibiotic Resistance Gene mecA in Methicillin-Resistant Staphylococcus aureus (MRSA) Strains. BioTech. 2023;12(2):1-14.
Crossref - Mahmood F, Jan MS, Ahmad S, et al. Ethyl 3-oxo-2-(2,5-dioxopyrrolidin-3-yl)butanoate derivatives: Anthelmintic and cytotoxic potentials, antimicrobial, and docking studies. Front Chem. 2017;5:1-11.
Crossref - Badger-Emeka LI, Emeka PM, Ibrahim HIM. A Molecular Insight into the Synergistic Mechanism of Nigella sativa (Black Cumin) with b-Lactam Antibiotics against Clinical Isolates of Methicillin-Resistant Staphylococcus aureus. Appl Sci. 2021;11(7):3206.
Crossref - Mulani MS, Kamble EE, Kumkar SN, Tawre MS, Pardesi KR. Emerging strategies to combat ESKAPE pathogens in the era of antimicrobial resistance: A review. Front Microbiol. 2019;10(4):539.
Crossref - Rondevaldova J, Novy P, Urban J, Kokoska L. Determination of anti-staphylococcal activity of thymoquinone in combinations with antibiotics by checkerboard method using EVA capmatTM as a vapor barrier. Arab J Chem. 2017;10(4):566-572.
Crossref - Dera AA , Ahmad I, Rajagopalan P, et al. Synergistic efficacies of thymoquinone and standard antibiotics against multi-drug resistant isolates. Saudi Med J. 2021;42(2):196-204.
Crossref - Qureshi KA, Imtiaz M, Parvez A, et al. In vitro and In silico Approaches for the Evaluation of Antimicrobial Activity, Time-Kill Kinetics, and Anti-Biofilm Potential of Thymoquinone (2-Methyl-5-propan-2-ylcyclohexa-2, 5-diene-1,4-dione) against Selected Human Pathogens. Antibiotics. 2022;11(1):79.
Crossref - Fan Q, Yuan Y, Jia H, et al. Antimicrobial and anti-biofilm activity of thymoquinone against Shigella flexneri. Appl Microbiol Biotechnol.2021;105(11):4709-4718.
Crossref - Cheng G, Sa W, Cao C, et al. Quinoxaline 1,4-di-N-oxides: Biological activities and mechanisms of actions. Front Pharmacol. 2016;7:64.
Crossref - Adegbeye MJ , Elghandour MMMY, Faniyi TO, et al. Antimicrobial and antihelminthic impacts of black cumin, pawpaw and mustard seeds in livestock production and health. Agrofor Syst. 2020;94(4):1255-1268.
Crossref - Goel S, Mishra P. Thymoquinone inhibits biofilm formation and has selective antibacterial activity due to ROS generation. Appl Microbiol Biotechnol. 2018;102(4):1955-1967.
Crossref - Nang SC, Lin YW, Fabijan AP, et al. Pharmacokinetics/pharmacodynamics of phage therapy: a major hurdle to clinical translation. Clin Microbiol Infect. 2023;29(6):702-709.
Crossref - Duan L, Zhang J, Chen Z, et al. Antibiotic combined with epitope-specific monoclonal antibody cocktail protects mice against bacteremia and acute pneumonia from methicillin-resistant staphylococcus aureus infection. J Inflamm Res. 2021;14:4267-4282.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.