

ISSN: 0973-7510
E-ISSN: 2581-690X
Helicobacter pylori infection is ubiquitous. Endoscopic Rapid urease test [RUT] is sensitive and specific for diagnosing H. pylori organism during endoscopy. Retrospective analysis of the pattern of RUT performance by endoscopists in Southeast Bengal region in patients evaluated for upper gastrointestinal disorders was performed. The gastroscopy reports of consecutive patients from South-eastern Bengal attending a gastroenterology clinic were studied. The data along with relevant treatment history were entered into a questionnaire and the data was analyzed. Data of 151 patients were analyzed. 16 patients with reflux oesophagitis and growth in duodenum were excluded. Out of 135 patients, 47.4 % and 52.6% had peptic ulcers and non ulcer dyspepsia [NUD] respectively. Rapid urease test (RUT) was positive in 40.62% and 33.80% of peptic ulcer and NUD patients respectively (p = 0.477). However 32.45% patients on “premedication” and 62% without “premedication’ ’were RUT positive, which was statistically significant (p= 0.014). There is also no difference (P >0.05) in endoscopic diagnosis or result of RUT performed by gastroenterologists or nongastroenterologists. 81.25% of RUT positive NUD patients who received Triple therapy for H. pylori did not respond; but all [100%] responded to antidepressants. RUT was performed routinely in all patients undergoing gastroscopy irrespective of diagnosis. The RUT was routinely performed without cognizance of pre-endoscopy treatment. “Pre-treatment” results in erroneous underestimation of H. pylori infection. Antidepressants were superior to triple therapy for NUD even in H. pylori infected patients.
Helicobacter pylori, Rapid urease test, Non-ulcer dyspepsia.
Helicobacter pylori infection is ubiquitous in both developing as well as developed countries. It is a gram negative, curved, microaerophilic and motile organism with multiple polar flagella having extraordinary ability to establish infections in human stomachs for years or decades. More than 50% of the world population is colonized with H.pylori1, 2. Exposure occurs in childhood and approximately 80% of adults have been infected at some time. Sero-surveys indicate a seroprevalence of 22%-57% in children under the age of five, increasing to 80%-90% by the age of 20, and remaining constant thereafter3-6 H. pylori commonly causes peptic ulcer, presenting as recurrent abdominal pain and is associated with 90% of duodenal ulcers and 80% of gastric ulcers7. H. pylori is also associated with gastric mucosa associated lymphoid tissue (MALT) lymphomas and gastric adenocarcinoma. There is an ambiguous between non-ulcer dyspepsia and infection with H pylori. The pathophysiology of dyspepsia with H. pylori infection is unclear, but may include changes in acid secretion, abnormal motility, or altered visceral perception8 The prevalence of H pylori is higher in patients with non-ulcer dyspepsia than in healthy controls9
Various methods to diagnose H. pylori infection are grouped as (a) Invasive methods and (b) Non invasive methods. The invasive methods are based on collection of endoscopic gastric biopsy specimens that are subjected to urease test, staining, culture, histology and molecular diagnostic techniques. The non invasive methods comprise urea breath test, serology and stool antigen test. Among invasive tests, Rapid urease test is a rapid, inexpensive, sensitive and specific diagnostic modality, which can identify H. pylori organism and can be also used for monitoring therapy. In the presence of H. pylori infection, urea is hydrolyzed to ammonia and carbon dioxide (CO2) due to release of urease enzyme. The change in colour of the broth from pale yellow to deep pink is taken as a positive result. Bacteria other than H. pylori that produce urease in a small amount cannot survive in the gastric mucosa.
Our study is aimed to audit the pattern of RUT performance by endoscopists and audit of the response to treatment, in Southeast Bengal region in patients evaluated for upper gastrointestinal disorders.
Retrospective analysis of records of consecutive patients attending a gastroenterology clinic for upper G.I. disorder with a past upper UGI endoscopy report was performed over a period of 7 Years from 05.11.03 to 24.06.10. During this period a total of 151 patients with dyspeptic symptoms were studied with their previous report. The records of these patients including endoscopic findings, RUT report and details of pre-procedure PPI/H2RA therapy within 2 weeks, and post UGIE treatment were analyzed. As Rapid urease Test (RUT) has a high sensitivity, specificity, positive predictive value in the order of > 98%, >99 %,> 99% respectively10, positive RUT was considered as presence of H. pylori in the gastric mucosa in the above patients. The patients having “peptic ulcer disease’’ (gastric ulcer and duodenal ulcer) and normal or near-normal endoscopies (including findings of questionable clinical significance such as gastritis or duodenitis) categorized as “nonulcer dyspepsia’’ on endoscopy were included in the study. Presence of reflux oesophagitis, any growth in stomach or duodenum, and any disease outside the stomach were excluded from this study. Peptic ulcer disease (PUD) group and nonulcer dyspepsia (NUD) group were again subdivided into two categories based on prior premedication or no premedication with PPI/H2RA before endoscopy.
Results of rapid urease test in all categories were analyzed. An audit of treatments used for H. pylori positive NUD patients and also the subjective [symptomatic] response to anti H. pylori treatment / anti-depressants was also analyzed during the current visit.
Definitions
Non ulcer dyspepsia (NUD) is defined as patients with central upper abdominal pain or discomfort for at least 12 weeks but a normal endoscopic appearance. Premedication means intake of proton pump inhibitors (PPIs) or histamine 2-receptor antagonists (H2RAs) [within 2 weeks] prior to rapid urease testing.
Statistical Analysis
Data was entered and analyzed in Statistical Package for Social Sciences (SPSS) ver17.0. Chi square test/Fisher’s Exact Test was used for nominal values.
Out of 151 patients, 128 were males and 23 were females with M: F ratio 5.6:1. Diagnosis by endoscopic findings is shown in Figure 1. Majority of patients had nonulcer dyspepsia (47%) followed by duodenal ulcer (31%) and gastric ulcer (11%). To prevent confounding in this study, sixteen were excluded due to presence of reflux oesophagitis in 15 patients and duodenal growth in one patient. Rest 135 patient i.e. 64 patients with peptic ulcer disease (47 duodenal ulcer, 17 gastric ulcer) and 71 patients of nonulcer dyspepsia (NUD) were included in the study (Fig 2).
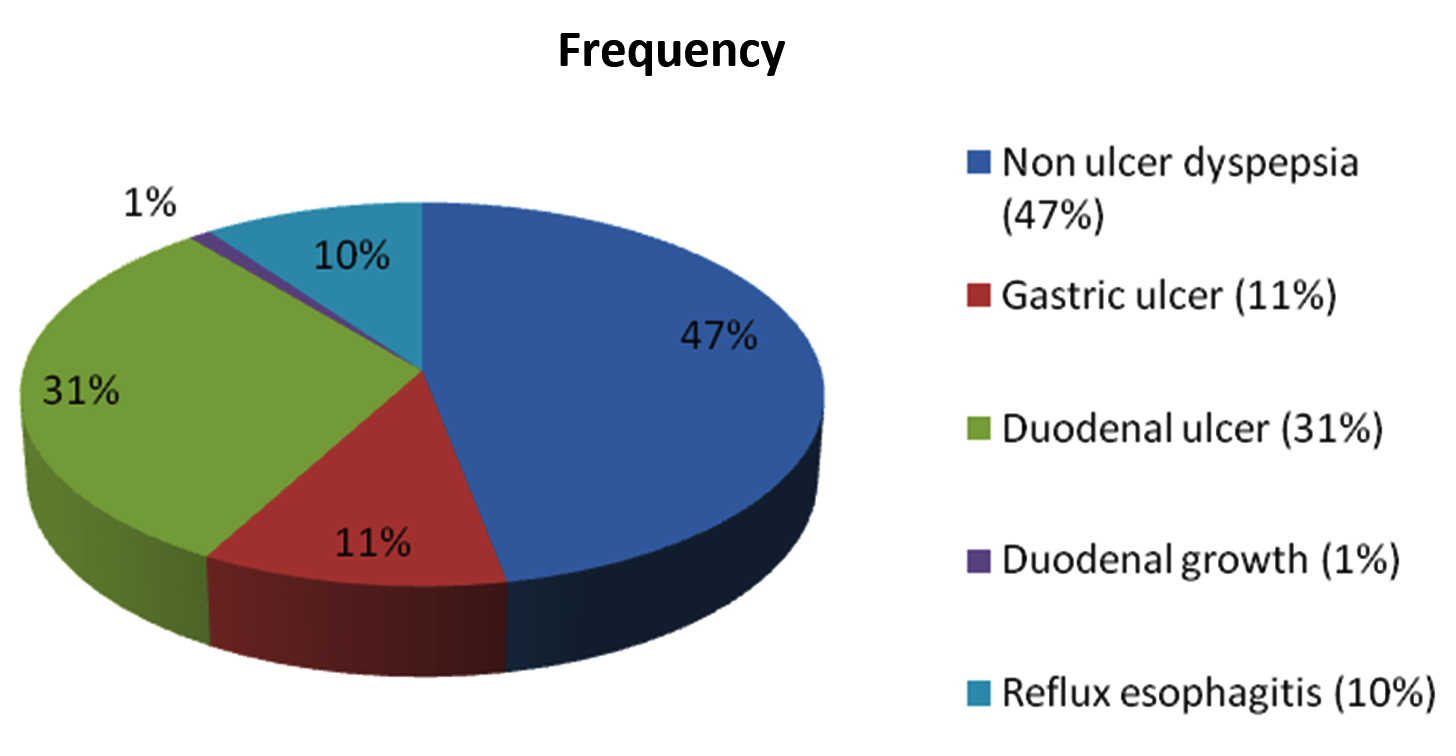
Fig. 1. Endoscopic findings
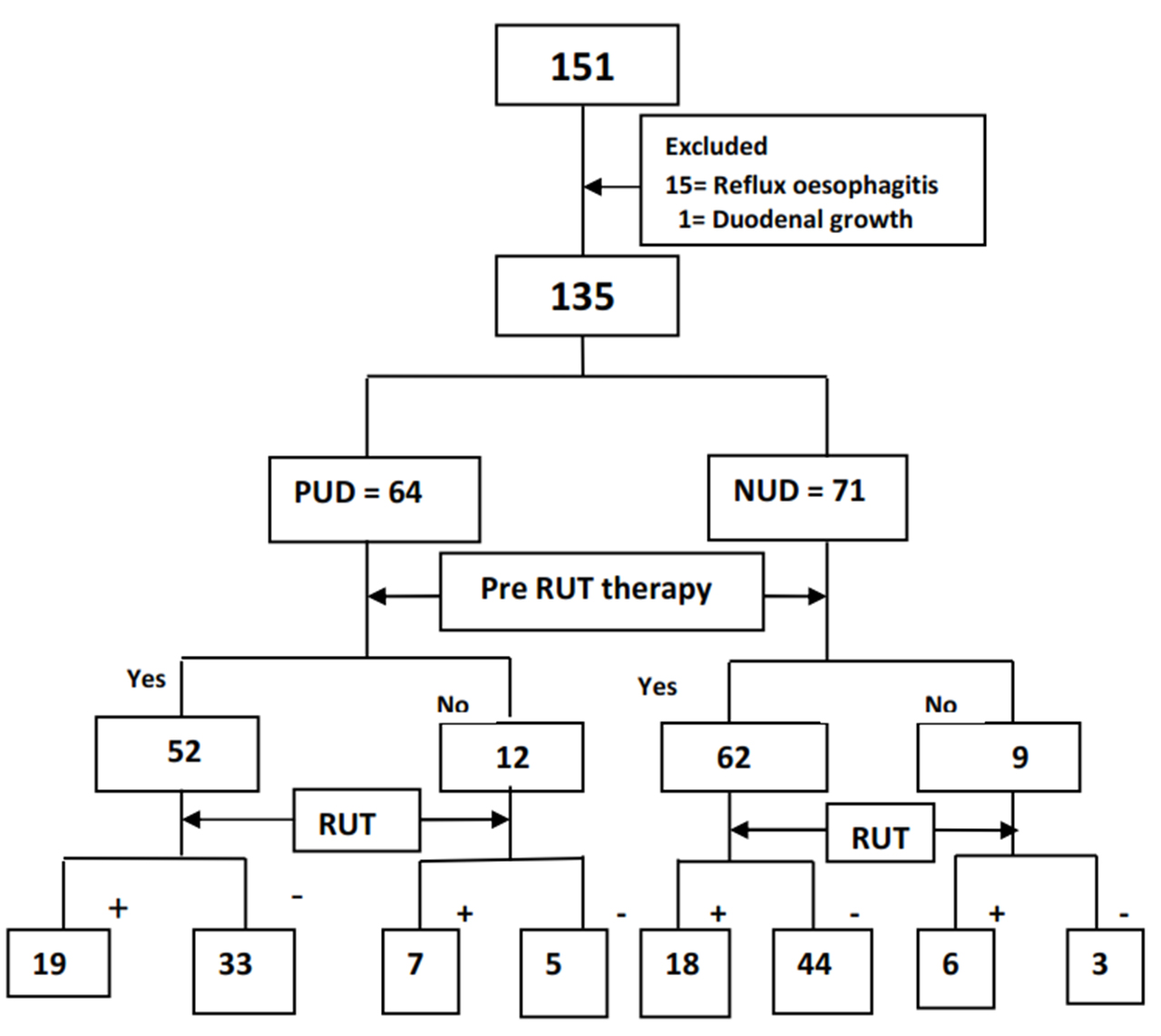
Fig. 2. Flow chart of study population
Peptic ulcers were found to be more common in males (53.04%) than females (15%). On the contrary females suffered more from nonulcer dyspepsia than males (p= 0.002) as shown in Figure 3. Rapid urease test was negative in 62.6% of males and 65% of females respectively (p=1.000) shown in Table 2. There was positivity no gender difference in rapid urease test positivity. Rapid urease test was positive in 40.62% and 33.80% of peptic ulcer and NUD patients respectively (p =0.477). Further subgroup analysis was done with premedication and without premedication to find out any differences. In peptic ulcer group, 36.5% with premedication and 58.3% without premedication were RUT positive (p=0.165). In NUD patients 29% with premedication and 66.6% without premedication were RUT positive (p=0.053). As premedication [PPIs or antibiotics prior to endoscopy] can influence the rapid urease test, further analysis was done in patients of both groups without premedication. In patients without premedication (Fig 2), positive rapid urease test was found only 58.3 % in peptic ulcer and 66.6% of NUD patients respectively (p=1.000). Overall out of 135 patients (Table-1), RUT positivity was seen in 32.45% and 61.9% patients on premedication and without premedication respectively (p = 0.014).
Table (1):
Factors associated with rapid urease test result
| RUT +VE(50) | RUT –VE(85) | p value | |
|---|---|---|---|
| Males | 43(37.4%) | 72(62.6%) | 1.000 |
| Females | 7(35%) | 13(65%) | |
| Premedication | 37(32.45%) | 77(67.54%) | 0.014 |
| No premedication | 13(61.9%) | 8(38.1%) | |
| Peptic ulcer | 26(40.62%) | 38(59.38%) | 0.477 |
| NUD | 24(33.80%) | 47(66.2%) |
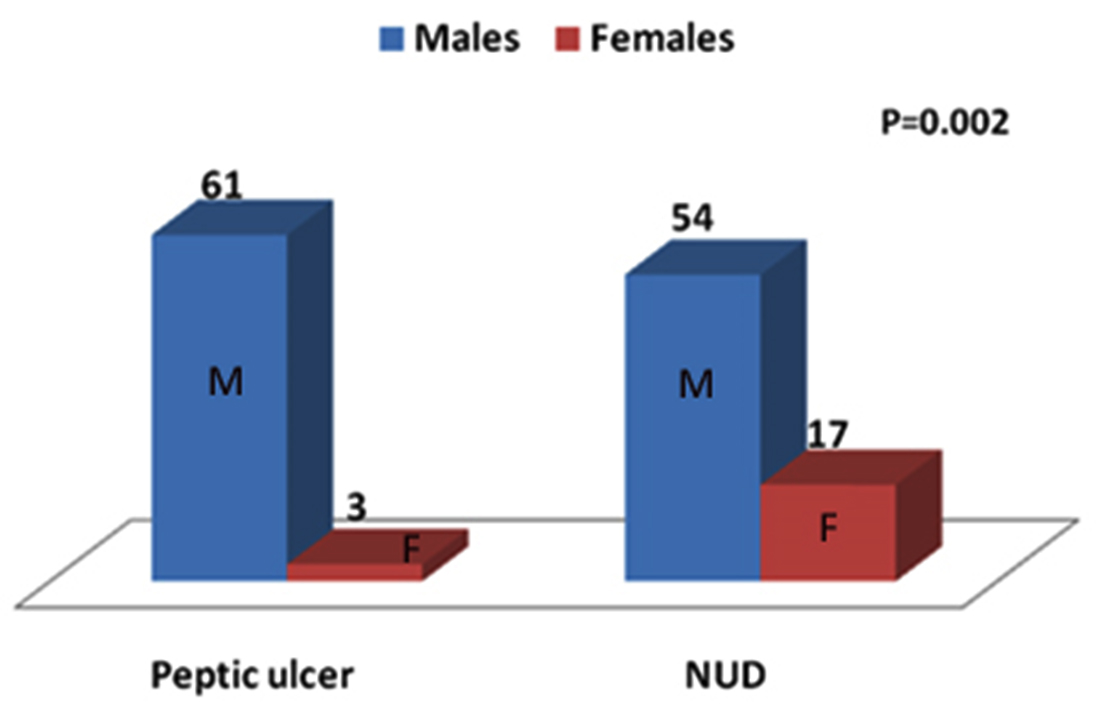
Fig. 3. Diagnosis according to gender
An Analysis of endoscopic pattern was done according to type of physicians (Table 2). Comparison of endoscopic diagnostic yield between untrained physicians [non-gastroenterologists] and trained physicians [gastroenterologists] showed that there was no difference in the proportion of patients having duodenal ulcer and nonulcer dyspepsia [NUD] (p=0.575).Similarly there was no difference in results of RUT (p=0.570) performed by different types of physicians (Table 2).
Table (2):
Diagnosis according to type of physicians
| Gastroenterologists | Nongastroenterologists | ||
|---|---|---|---|
| Peptic ulcer | 20(31.25%) | 44(68.75%) | 0.575 |
| NUD | 19(26.76%) | 52(68.42%) | |
| RUT +VE | 13(26%) | 37(74%) | 0.570 |
| RUT –VE | 26(30.59%) | 59(69.41%) |
Since we considered positive RUT as evidence of H. pylori infection, percentage of positive RUT without prior therapy can be extrapolated as prevalence of H. pylori infection in peptic ulcers patients (58.3%), NUD (66.6%) and total patients (61.9%).
The results of analysis of response to triple therapy in RUT positive NUD patients has been shown in Figure 4. Out of 71 NUD patients, 24 patients had positive RUT. Of these positive RUT patients, 18 patients were given triple therapy and 6 patients were given PPI or other medications. Two patients, who had taken triple therapy, did not come for follow up. The 16 patients of NUD, taking triple therapy, were assessed for symtomatical improvement after one month. Thirteen (81%) RUT positive NUD patients who received triple therapy for H. pylori did not respond, but all of the thirteen [100%] patients not responding to triple therapy responded to antidepressants (Figure -5). Using Fisher’s exact test, antidepressants are extremely effective than triple therapy regimen for non ulcer dyspepsia (p value=<0.0001), even in Helicobacter pylori infected patients. However response to anti-H. pylori triple regimen was significant (p=0.0011) in RUT positive peptic ulcer (80%) patients compared to NUD (18.75%) patients.
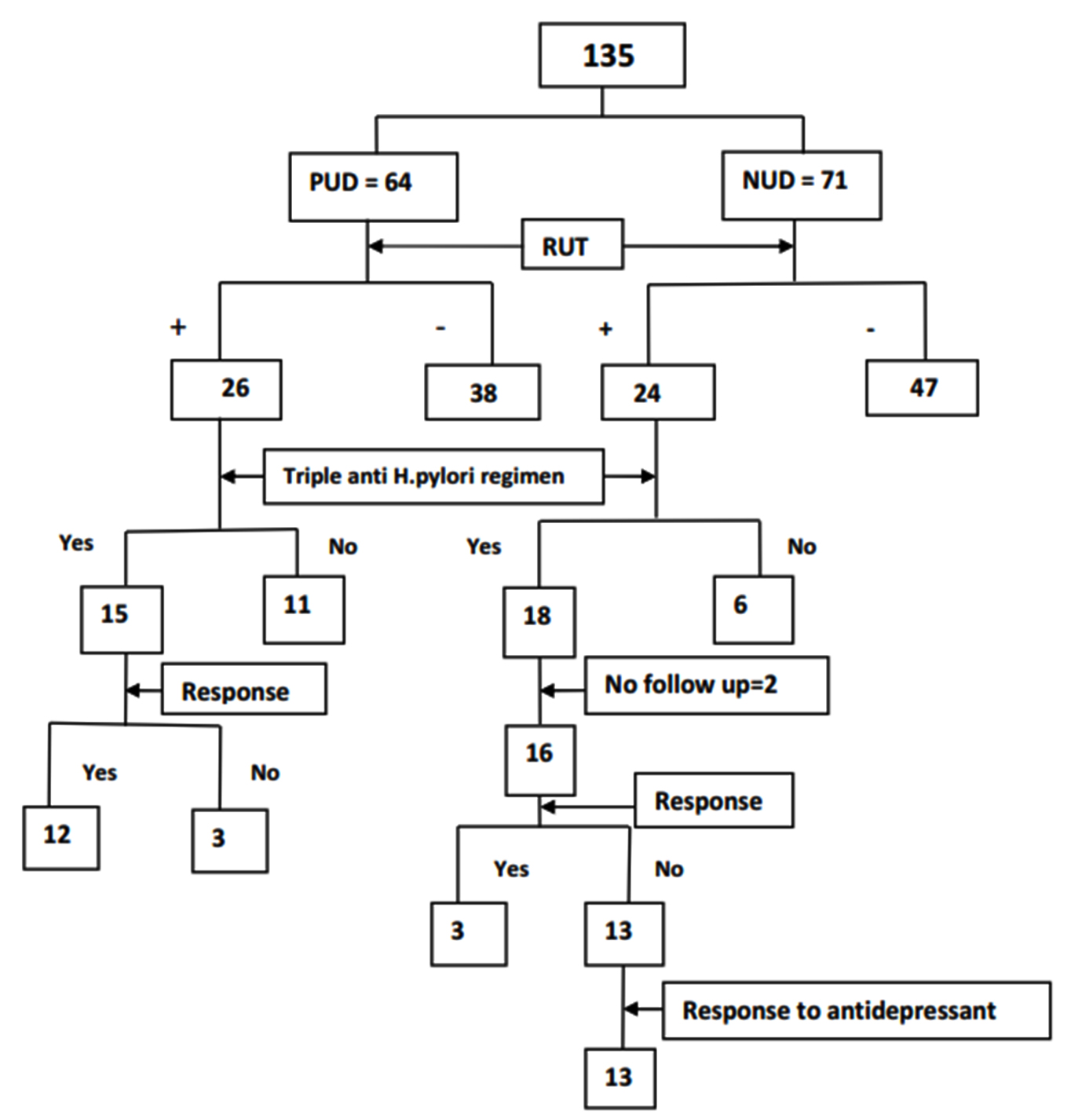
Fig. 4. Study flow chart of treatment
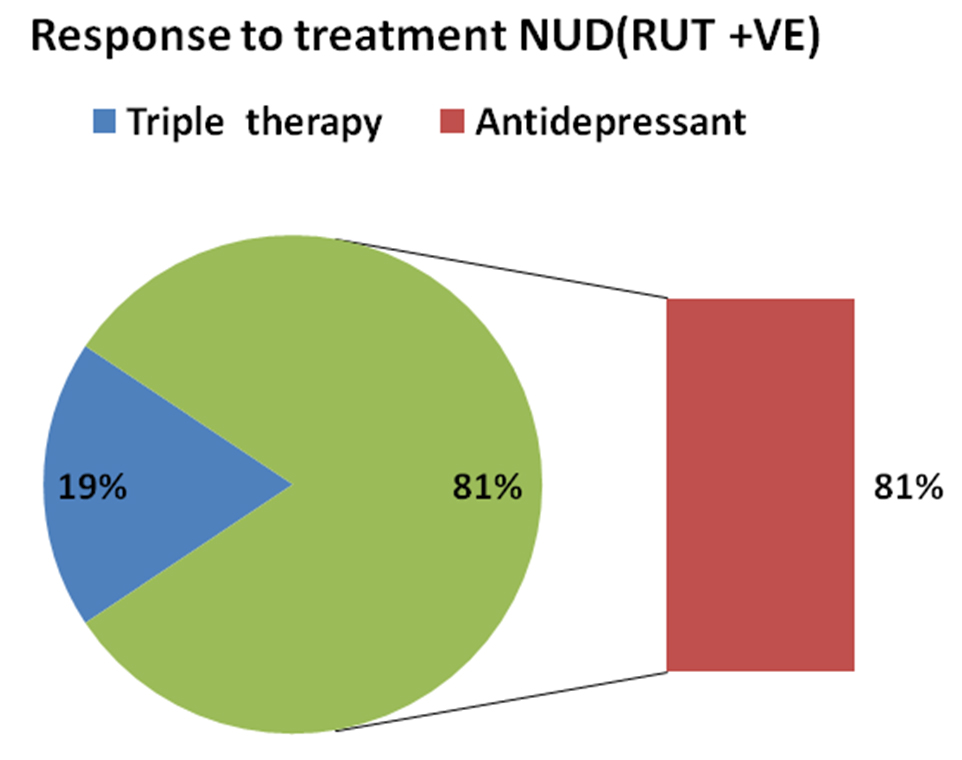
Fig. 5. Treatment response in rapid urease test positive NUD patients
Endoscopic findings of patients with upper gastrointestinal disorders from Southeast Bengal region revealed varied diagnosis. Non ulcer dyspepsia (47%) was the commonest diagnosis followed by peptic ulcers (42%) and reflux oesophagitis (10%). However an endoscopic review of four series of dyspeptic patients in U.K. revealed NUD 34% followed by GERD 24% and peptic ulcers 20%11,12 High prevalence of peptic ulcers in our study may be due to increased prevalence of causative factor like H. pylori infection, low hygienic environment and overcrowding.
In our study, males suffered more from peptic ulcers than females, which may be due to more proneness for stress and strain as well as addiction for alcohol and smoking in males. Females seek medical attention for functional dyspepsia (85%) more often than for ulcers (47%). Endoscopy is done by both trained and untrained physicians throughout the country due to lack of sufficient number of trained doctors as well as proximity of patients to untrained physicians, however there was no difference in diagnosing peptic ulcers and performance of rapid urease test.
There are limited studies in literature comparing response of rapid urease test with premedication in peptic ulcers or non ulcer dyspepsia. In our study, there was no significant difference in result of rapid urease test in peptic ulcer and non ulcer dyspepsia patients with regards to premedication, which may be due to small samples size and noneradication of H. pylori with respect to premedication. However, Overall analysis in 135 patients, demonstrated that prior PPI/H2 RA therapy resulted in decrease in positivity of rapid urease Test (RUT) significantly, compared to the group who had not received prior PPI, as found in other studies13, 14.
There are a number of studies15-18 on the effectiveness of triple therapy in peptic ulcer Patients, similar to our study. However, there are controversies regarding treatment of NUD patients. In our study, symptoms of 82% of NUD patients did not respond to anti H. pylori therapy, where as all NUD patients responded to anti-depressants, contrast to other studies16-18 Meta-analysis of twelve trials by Moayyedi19 showed H. pylori eradication treatment was significantly superior to placebo in treating non-ulcer dyspepsia (relative risk reduction 9% (95% confidence interval 4% to 14%), one case of dyspepsia being cured for every 15 people treated. H. pylori eradication cost £56 per dyspepsia-free month during first year after treatment. Canadian Helicobacter pylori consensus conference also favours the H. pylori eradication to prevent development of ulcer or cancer as the lifetime risk of developing ulcers for people who are infected with H. pylori is 5-15%20 A recent randomized clinical trial of 294 patients with uninvestigated dyspepsia in Canada found that treatment resulted in a sustained improvement in symptoms at 12 months in 50% of the patients treated to eradicate H. pylori compared with 36% in the placebo group21 This result was significant, and seven patients needed to be treated to cure one patient. The trial also showed that treatment was cost effective18 However another meta-analysis by Laine et al provided little support for the use of H. pylori eradication therapy in patients with nonulcer dyspepsia22. A study by Singh et al from Odisha also showed that antipsychotics rather than anti H. pylori treatment had a definite role in symptomatic amelioration of NUD patients23. Another small randomized controlled trial by Mertz et al. demonstrated benefit for symptoms of non-ulcer dyspepsia treated with amitryptiline 50 mg once daily at night24. Another prospective study on sixty patients (seropositive) found no benefit in-patients in dysmotility like NUD with anti H. pylori treatment with comparison to ulcer variety25. Thus most studies favour the effectiveness of antidepressants over H. pylori treatment for NUD. First, rampant use of antibiotics like amoxicillin, clarithromycin and metronidazole for other diseases sometimes with inadequate doses, may be responsible for resistance to these drugs used for H. pylori treatment. Further, our study population may have pre-dominant psychosomatic features, contributing to the pathophysiology of NUD. Besides, time to response measured after H. pylori treatment might be too short to get effective response from H. pylori treatment, compared to other studies15.
Our study on peptic ulcers showed 58% prevalence of H. pylori in contrast to an older study showing prevalence of H. pylori infection between 95% and 100%,3 which might be because of few small sample size. However, in a recent study from Kolkata, 70.04% patients were H. pylori –positive, which is similar to our study26 In our study prevalence of H. pylori in NUD was found to be 67%, similar to other studies from different parts of India (South India 74%,27 and New Delhi 54%28).
Various studies have demonstrated the role of H. pylori in the pathophysiology of peptic ulcer, MALT, and gastric carcinoma. This raises the question whether eradication of H. pylori is a practically feasible or necessary in developing countries like India? According to Ramakrishna, eradication of H. pylori in NUD is not justifiable in India29 Prevalence of H. pylori in normal population varies from 60 -80% in different studies in from various parts of India3, 27, 30 – 33 To eradicate the innocuous bacteria from our gastric flora, which is present since times immemorial34 we have to treat nearly 70-80 crores of people, which is not possible as recurrence of infection occurs in around 60% of patients according to reports published in various Indian publications35 In an Indian study of 45 patients followed up following eradication of H. pylori, recurrence of infection was detected in only one patient (2.4%) after one year36. There are also other arguments against the eradication of H. pylori infection. All strains inhabitating the gastric mucosa are not virulent. Besides, Production of increased acidic environment in the stomach and other immune factors may be a barrier to other ingested pathogens37, 38. In addition, the Possibility of protection from allergic and autoimmune diseases including asthma and Crohn’s disease due to H. pylori infection compared to developed countries may favour against treatment of this organism in developing countries like India39 Various consensus statements regarding treatment of H. pylori in India have ruled out anti H. pylori therapy for NUD patients, as this may aggravate the symptoms instead of amelioration40-43
RUT was performed routinely in all patients undergoing gastroscopy irrespective of diagnosis and without cognizance of pre-endoscopy treatment. Functional dyspepsia patients seek advice of untrained gastroenterology physicians more than qualified gastroenterologists. “Prior treatment” results in erroneous underestimation of H. pylori infection by RUT alone. RUT performed in general practice (irrespective of recent drug therapy) can be fallacious for detecting H. pylori infection and deciding about institution of eradication therapy. Antidepressants were superior to triple therapy for NUD even in H. pylori infected patients. There is no rationale for performing RUT in NUD Patients or treating these patients with anti H. pylori therapy. There is a need for developing rational guidelines for performing RUT.
- Mitchell HM. The epidemiology of Helicobacter pylori. Curr Top Microbiol Immunol 1999; 241:11-30.
- Brown LM. Helicobacter pylori. Epidemiology and Transmission, Epidemiol Rev Vol. 2000; 22: 283-297.
- Graham DY, Adam E, Reddy GT, Agarwal JP, Agarwal R, Evans DJ Jr, et al. Seroepidemiology of Helicobacter pylori infection in India. Comparison of developing and developed countries. Dig Dis Sci 1991; 36: 1084-8.
- Gill HH, Majumdar P, Shankaran K, Desai HG. Age-related prevalence of H. pylori antibodies in Indian subjects. Indian J Gastroenterology 1994; 13: 92-4.
- Kang G, Rajan DP, Patra S, Chacko A, Mathan MM. Use of serology, the urease test and histology in diagnosis of Helicobacter pylori infection in symptomatic and asymptomatic Indians. Indian J Med Res 1999; 110:86-90.
- Jais M, Barua S. Seroprevalence of anti Helicobacter pylori IgG/IgA in asymptomatic population from Delhi. J Commun Dis 2004; 36:132-5.
- Aroori S. Helicobacter pylori. Gastroenterology Today 2001; 5: 131-33.
- Talley NJ, Hunt RH. What role do H. pylori play in dyspepsia and non-ulcer dyspepsia: Arguments for and against H. pylori being associated with dyspeptic symptoms? Gastroenterol. 1997; 113:S67–S77.
- Armstrong D. H. pylori and dyspepsia. Scand J Gastroenterology. 1996; 31:38 47.
- Said RM, Cheah PL, Chin SC, Goh KL. Evaluation of a new biopsy urease test: Pronto Dry for the diagnosis of Helicobacter pylori infection. Eur J Gastroenterol Hepatology 2004; 16:195- 199.
- Richter J. Organic causes and differential characteristics from functional dyspepsia. Scand J Gastroenterol 1991; 26:11.
- AGA Technical Review: Evaluation of Dyspepsia, Table 1 p. 583, Gastro 1998;114:582-595.
- Megraud F.How should Helicobacter pylori infection be diagnosed? Gastroenterology. 1997; 113:S93-8.
- Yakoob J, Jafri W, Abid S, Jafri N, Abbas Z, Hamid S, Islam M, Anis K, Shah HA, Shaikh H.Role of rapid urease test and histopathology in the diagnosis of Helicobacter pylori infection in a developing country. BMC Gastroenterology 2005, 5.
- Ford A, Delaney B, Forman D, Moayyedi P. Eradication therapy for peptic ulcer disease in Helicobacter pylori positive patients. Cochrane Database Syst Rev 2004; 4:CD003840.
- Dayal VM, Kumar P, Kamal J, Shahi SK, Agrawal BK. Triple-drug therapy of Helicobacter pylori infection in duodenal ulcer disease. Indian J Gastroenterol 1997; 16:46-8.
- Forbes GM, Glaser ME, Cullen DJ, Warren JR, Christiansen KJ, Marshall BJ, et al. Duodenalulcer treated with Helicobacter pylori eradication: seven-year follow-up Lancet. 1994; 343:258–60.
- Graham DY, Lew GM, Klein PD, Evans DG, Evans DJ Jr, Saeed ZA, et al. Effect of treatment of Helicobacter pyloriinfection on the long-term recurrence of gastric or duodenal ulcer. Ann Intern Med. 1992; 116: 705–8.
- Moayyedi P, Soo S, Deeks J, Delaney B, Harris A, Innes M, et al. Eradication of Helicobacter pylori for non-ulcer dyspepsia. Cochrane Database Syst Rev. 2001; 1:CD002096.
- Hunt RH, Thomson ABR. consensus conference participants. Canadian Helicobacter pylori consensus conference. Can J Gastroenterol. 1998; 12: 31–41
- Chiba N, Veldhuyzen van Zanten SJO, Sinclair P, Ferguson RA, Escobedo SR. the Cadet-Hp Study Group. Beneficial effect of H. pylori eradication therapy on long term symptom relief in primary care patients with uninvestigated dyspepsia: the cadet-Hp study [abstract] Gastroenterology. 2000; 118:A2390.
- Laine L, Schoenfeld P, Fennerty MB. Therapy for Helicobacter pylori in patients with nonulcer dyspepsia. A meta-analysis of randomized, controlled trials. Ann Intern Med. 2001; 134:361–9.
- Singh SP, Thatoi PK, Mohanty CBK, Das S, Mallik RN, Rout N. The role of Helicobacter pylori in nonulcer dyspepsia (NUD) [Abstract]. Indian J Gastroenterol 1997; 16 (suppl 2):A25.
- Mertz H et el, Effect of Amitryptiline on Symptoms, Sleep, and Visceral Perception in Patients With Functional Dyspepsia. Am J Gastroenterol 1998; 93:160-165.
- Babu V, Kate V, Ananthakrishnan N. Role of eradication of Cag A Helicobacter pylori in nonulcer dyspepsia.Trop Gastroenterol. 2005; 26:211-4
- Goenka MK, Majumder S, Sethy PK, Chakraborty M, Helicobacter pylori negative, non-steroidal anti-inflammatory drug-negative peptic ulcers in India. Indian J Gastroenterol. 2011; 30:33-7.
- Kate V, Ananthakrishnan N, Badrinath S, Ratnakar C. Prevalence of Helicobacter pylori infection in disorders of the upper gastrointestinal tract in south India. The National Medical Journal of India 1998; 11: 5-8.
- Mukhopadhyay DK, Tandon RK, Dasarathy S, Mathur M, Wali JP. A study of Helicobacter pylori in north Indian subjects with non-ulcer dyspepsia. Indian J Gastroenterol. 1992; 11:76-9.
- B.S.Ramakrishna, Helicobacter pylori infection in India: the case against eradication. Indian Journal of Gastroenterology 2006; 25: 25-8.
- Prasad S, Mathan M, Chandy G, Prasanna Rajan 0, Venkateswaran S,Ramakrishna BS, et al. Prevalence of Helicobacter pylori in southern Indian controls and patients with gastro duodenal disease. J Gastroenterol HepatoI 1994; 9: 501-6.
- Dore SP, Krupadas S, Borgonha S, Knipad AV. The 13C urea breath test to assess Helicobacter pylori infection in school children. Natl Med J India 1997; 10:57-60.
- Singh V, Trikha B, Nain CK, Singh K, Vaiphei K. Epidemiology of Helicobacter pyloriand peptic ulcer in India. Journal of Gastroenterology and Hepatology 2002; 17:659-65.
- Mishra S, Singh V, Rao GRK, Dixit VK, Gulati AK, Nath G. Prevalence of Helicobacter pyloriin asymptomatic subjects—A nested PCR based study. Infection, Genetics and Evolution 2008: 8: 815–819.
- Blaser MJ. Not all Helicobacter pylori strains are created equal: should all be eliminated? Lancet 1997; 349:1020–2
- Nanivadekar SA, Sawant PD, Patel HD, Shroff CP, Popat UR, Bhatt PP. Association or pepticulcer with Helicobacter pylori and the recurrence rate. A three years follow up study. J Assoc Physicians India 1990; 38:703-6.
- Bapat MR, Abraham P, Bhandarkar PV, Phadke AY, Joshi AS. Acquisition of Helicobacter pylori infection and reinfection after its eradication are uncommon in Indian adults. Indian J Gastroenterol 2000; 19:172-4.
- Blaser MJ. Helicobacter pylori eradication and its implications for the future. Aliment Pharmacol Ther 1997; 11:103-7.
- Blaser MJ, Atherton JC. Helicobacter pylori persistence: biology and disease. J Clin Invest 2004; 113:321-33.
- Bach JF. The effect of infections on susceptibility to autoimmune and allergic diseases. N Engl J Med 2002; 347:911-20.
- Kang JY, Folk KM, Ng HS, Ho KT, Chee A. Working party report of the Gastroenterological Society of Singapure. Part II- Helicobacter pylori and non-ulcer dyspepsia in Singapure. Singapure Med J 1996; 37: 428-429
- Bhatia SJ , Bhandarkar P V , Aggarwal R, Sawant P D. Eradication of Helicobacter pylori in nonulcer dyspepsia. Indian Journal of Gastroenterology 2000; 19(Suppl 1): S16-S19.
- Abraham P, Bhatia SJ,Position paper on Helicobacter pylori in India. Indian Society of Gastroenterology. Indian J Gastroenterol. 1997; 16 (Suppl 1): S29-33.
- Peura DA. The report of the Digestive Health Initiative International Update Conference on Helicobacter pylori. Gastroenterology 1997; 113(suppl 1):S4-S8.
© The Author(s) 2017. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.