

ISSN: 0973-7510
E-ISSN: 2581-690X
The 2022 Monkeypox Disease (MPOX) outbreak was declared a pandemic after detecting multiple human-to-human monkeypox cases in ‘non-endemic’ nations. The index case of MPOX has been reported in Nepal. Also, the disease burden in neighboring countries and international travel and tourism could increase the MPOX burden in Nepal. This study recruited 443 study participants between August 25 and September 10, 2022, using the snowball technique and using descriptive statistics to assess the awareness and knowledge of MPOX. Approximately 82% (n=361) of the study participants were young adults aged between 18-29 years and were undergoing or holders of tertiary education degrees (72.2%, n=320). Our findings showed that 76.5% (n=339/443) of the respondents were aware of the 2022 MPOX outbreak and obtained information about the disease from their local radio and television stations (20.6%, n = 70), as well as from other sources such as social media platforms (70.5%, n=239), and other internet sources (61.6%, n=209). The mean knowledge score of the respondents was 3.95±1.26, with a range of 0.5 to 7. Approximately three-quarters (72.3%, n=245) of the study participants were graded to have a good knowledge of the MPOX. Of the listed symptoms, study participants correctly identified high fever (62.2%, n=339), rashes (51.0%, n=173), swollen lymph nodes (34.5%, n=117), and sores around the mouth, vagina, and anus (26.8%, n=91). A higher number of participants were aware that vaccination could confer protection against the disease (70.8%, n=240). However, less than one third of the participants (30%, n=102) were aware that safe sex practices can be a preventive strategy against the disease. Finally, none of the sociodemographic variables were associated with increased knowledge of MPOX among the study participants. The knowledge of MPOX among the study population was above average. We advocate that public enlightenment campaigns in Nepal should address wrong perceptions of MPOX.
Monkey Pox, MPOX, Knowledge, Nepal, Awareness, Perception, Young Adults, Online Survey
The monkeypox virus (double-stranded DNA pox virus) causes monkeypox (MPOX), a re-emerging zoonotic disease that can be transmitted both directly between humans and indirectly through the environment.1 Humans infected with MPOX typically experience two weeks of fever, headache, muscle and back discomfort, swollen lymph nodes, and low energy, followed by two weeks of rashes.2 Non-human primates, rats, antelope, and squirrels are just a few of the animals that can spread this virus to humans through direct contact or the consumption of raw or undercooked meat.1,2 Intercourse with infectious wounds, scabs, or body fluids, including sexual intercourse, is the primary transmission mode of the monkeypox virus (MPXV).3 There is a high risk of social stigma and prejudice for those with MPOX because of the disease’s association with sexual intercourse and the high number of documented cases among gay males. In addition to the above-mentioned symptoms, skin lesions in MPOX may continue for up to four weeks, and lymphadenopathy separates MPOX from smallpox.4,5
An unexpectedly high number of cases of monkeypox have been reported throughout multiple countries in Europe, the Americas, Australia, and Asia since the first case was reported in the UK on May 13, 2022.6 The spread of monkeypox was labeled a “public health emergency of international concern” (PHEIC) based on the detection of multiple human-to-human monkeypox cases in ‘non-endemic’ high-income nations.7 On May 10, 2023, the PHEIC status of MPOX was lifted by the IHR emergency committee. As of March 5th, 2024, confirmed cases totaled 94,274, with 178 fatalities recorded across 118 nations, with 1 case and 0 death in Nepal.8 Looking at the global cases of MPOX, the disease is mostly identified in men who are gay or bisexual and among men population who tend to have sex with men (MSM), suggesting the spread of the disease through sexual networks.8,9 The high frequency of cases can evidently increase the risk of social discrimination towards bisexual or gay males and, more broadly, the LGBTQI+ community. However, stigmatizing the LGBTQI+ community during the MPOX epidemic will have detrimental effects on disease control and prevention.10 The increasing number of human instances of MPOX emphasizes the need to track the progression of the disease, make precise diagnoses, and create efficient vaccines, treatments, and cures. Campaigns to educate the public about MPOX risk factors and preventative interventions are highly effective in reducing the incidence of the disease.8,11 Preventative measures may be hampered by a lack of MPOX understanding, especially among the general people.12-14
The index case of MPOX was reported in Nepal on the 16 of June 2023.15 The index patient was a frequent traveler. The presence of wild animals, including monkeys, in nearly every temple and park in Kathmandu may contribute to the outbreak of MPOX in Nepal.16 This is due to several factors, including the high number of foreign workers visiting from the United Arab Emirates, India, and other countries, the increased activity and mobility of people due to festivals and elections, and the prevalence of wild animals, including monkeys.8,12 Assessing disease knowledge can help in countries with a deficient healthcare system by shedding light on health-seeking behavior and the importance of preventative actions. A major threat to human health and safety is posed by the global resurgence and spread of MPOX, especially in non-endemic nations.13,17,18 The WHO claims that a lack of public awareness is a major barrier to stopping the spread of MPOX.18 The community’s collective knowledge significantly impacts the spread of diseases; therefore, adhering to preventative and control activities is crucial. The survey findings may help government public health officials improve regulations, raise awareness of the MPOX outbreak, and plan upcoming public health campaigns. As a result, we decided to run an online poll in Nepal to gauge the level of MPOX awareness among young adults there.
Study design and study participants
This study was conducted as an online cross-sectional survey, open to participants from diverse socio-economic backgrounds. Participants were required to be at least 18 years old, reside in Nepal, and provide informed consent to participate. Assuming that 50% of respondents would have an adequate understanding of MPOX, with 95% Confidence level and 5% margin of error, a sample size of 385 was determined. We added 10% for contingency, so the total number of sample size required was 433. 443 responses were collected during the survey’s active period. Participants were enlisted with the help of a snowball sampling technique that relied on preexisting relationships established through social media platforms like Facebook Messenger and WhatsApp. Data utilized in this analysis was collected between August 25, 2022 (when the survey was first distributed), and September 10, 2022.
Questionnaire design
We designed a survey instrument and used Microsoft Forms to deliver the pre-validated questionnaire (https://forms.office.com/r/YvPWVv90m5) to assess the level of MPOX awareness and knowledge among a representative sample of Nepalese. Two additional independent reviewers pre-validated the revised questionnaire19 to ensure the validity of the questions, and pilot research with 20 participants from two provinces in Nepal was conducted. In addition, we used the Cronbach Alpha test to determine the reliability of the survey instrument and found that its overall reliability was 0.73, which is within the acceptable range. The survey had 27 questions broken up into four different parts. The first part of the survey collected respondents’ demographics, while the second part tested how well respondents understood the MPOX condition. Data on preventative measures and attitudes about the global health crisis were the goals of Sections C and D, respectively.
Data analysis
The statistical package Minitab v.17 (Pennsylvania, USA) was used to analyze the data. We utilized descriptive statistics to report qualitative variables as frequencies and proportions. The quantitative data were presented as mean and standard deviation. As previously reported, we employed a numerical scoring method to assess the respondents’ in-depth knowledge of the MPOX.13 Correct responses got a score of 1, whereas an incorrect response received a score of 0. For questions with several valid answers, the weighted score for each correct option was between 0.125 and 0.25, depending on how many possibilities there were. Subsequently, using a 7-item measure, we calculated the sum of each respondent’s scores and categorized them as having a “Satisfactory” or “poor” understanding of MPOX. This grade was obtained by categorizing scores based on 50% of the highest possible score (n=7). As a result, respondents with a cumulative score of fewer than 3.5 points were rated as having a poor (inadequate) understanding of MPOX, while those with a Score of 3.5 to 7 were rated as having good (satisfactory) knowledge. Finally, we used Univariable logistic regression analysis with a p<0.05 and a 95% Confidence Interval (CI) to test for all significant associations between the independent variables (socio-demographic factors) and the outcome variable (knowledge of MPOX).
Respondent demographics
This online survey was attempted by 451 persons, out of which 443 consented to participate (response rate was 98.2%). The study participants included more male respondents (54.4%, n=241) than the female gender (45.6%, n=202). Most of the respondents were between 18 and 29 years old (81.5%, n=361), and 72.2% of the respondents (n=320) were in university education or had a bachelor’s degree (Table 1). More than three-quarters (76.52%, n=339) of the study participants identified as heterosexual, whereas 15.6% (n=69) of them identified as homosexuals. More responses were received from the Bagmati province (49.7%, n=225).
Table (1):
Sociodemographic profiles of study participants (n=443)
| Variables | Frequency (%) |
|---|---|
| Age (Years) | |
| 18-29 | 361 (81.5) |
| 30-39 | 42 (9.5) |
| 40-49 | 35 (7.9) |
| 50-59 | 4 (0.9) |
| >60 | 1 (0.2) |
| Gender | |
| Female | 202 (45.6) |
| Male | 241 (54.4) |
| Sexual orientation | |
| Bisexual | 31 (7) |
| Heterosexual | 339 (76.5) |
| Homosexual | 69 (15.6) |
| Prefer not to say | 4 (0.9) |
| Level of education | |
| College/University degree | 320 (72.2) |
| High School or lower | 70 (15.8) |
| Master/professional fellowships or PhD | 53 (12) |
| Geo-political region (Province) | |
| Bagmati | 220 (49.7) |
| Lumbini | 124 (28) |
| Gandaki | 57 (12.9) |
| Madhesh | 29 (6.5) |
| Koshi | 13 (2.9) |
Awareness and knowledge of monkeypox disease
Most of the study participants (76.5%, n=339/443) were aware of the 2022 MPOX outbreak and obtained information about the MPOX from their local radio and television stations (20.6%, n=70), as well as from other sources such as social media platforms (70.5%, n=239), and other internet sources (61%, n=207). Similarly, most of those (85.8%, n=291/339) who were aware of the disease knew that it was declared a public health emergency of international concern due to its widespread occurrence in countries where it was initially never reported. The mean knowledge score of the respondents was 3.95±1.26, with a range of 0.5 to 7. Approximately three-quarters (72.3%, n=245) of the study participants had above the cut-off score of 3.5 (50% of the maximum obtainable score) and were deemed to have a good knowledge of the MPOX.
Around half of the study participants (49%, n=166) didn’t know about the incubation period, while most knew that anyone could be affected (90%, n=305). Approximately half of the study participants (45.7%, n=155) were aware that proper hand hygiene was extremely important in reducing the spread of the MPXV. In addition, our study participants knew that vaccination against MPOX (70.8%, n=240) and practicing safe sex (30%, n=102) could be protective against the MPOX (Table 2). On the mode of transmission, study participants opined that close contact with people who have the virus (60.5%, n=205), contact with contaminated surfaces (42.2%, n=143), and sexual contact (26.8%, n=92) were the most common routes of transmission. In our study, there were some wrong perceptions, which included the notion that antibiotics could be protective of the MPOX (25.4%, n=86), the disease can be transmitted via air droplets (45.4%, n=154), and mosquito/insect bites (16.2%, n=55). Also, only 21.8% (n=74) of them knew that MPOX can present as symptomatic infections with no obvious clinical symptoms. Of the listed symptoms, study participants correctly identified high fever (62.2%, n=339), rashes (51.0%, n=173), swollen lymph nodes (34.5%, n=117), and sores around the mouth, vagina, anus (26.8%, n=91) (Figure).
Table (2):
Knowledge of monkeypox disease among respondents in Nepal (n=339)
| Variables | Frequency (%) |
|---|---|
| 1. Have you heard of the 2022 monkeypox outbreak? | |
| No | 104 (23.5) |
| Yes | 339 (76.5) |
| 1b. Source of information on MPOX? | |
| TV | 70 (20.6) |
| Radio | 70 (20.6) |
| Internet sources | 207 (61) |
| Social media platforms | 239 (70.5) |
| Newspaper | 37 (10.9) |
| Friends/Family | 67 (19.8) |
| WHO website | 53 (15.6) |
| 2. Did you know that MPOX was declared a PHEIC? (n = 339) | |
| No | 48 (14.2) |
| Yes | 291 (85.8) |
| 3. Is it possible for MPOX-positive persons to show no symptoms? | |
| No | 91 (26.8) |
| Yes | 74 (21.8) |
| I don’t know | 174 (51.4) |
| 4. How long does it take to incubate the MPXV? | |
| 1-14 days | 58 (17.1) |
| 1-3 months | 3 (0.88) |
| 5-21 days | 112 (33) |
| I don’t know | 166 (49) |
| 5. Who can be infected with the MPOX? | |
| Anyone can be infected | 305 (90) |
| Teenagers | 14 (4.1) |
| People with chronic diseases | 13 (3.8) |
| Only those who practice unsafe sex | 22 (6.5) |
| Only old people | 1 (0.3) |
| 6. How does the virus spread? | |
| Air droplets | 154 (45.4) |
| Mosquito/Insect bites | 55 (16.2) |
| Contact with contaminated surfaces | 143 (42.2) |
| Sexual intercourse | 91 (26.8) |
| Close contact with people that have the virus | 205 (60.5) |
| Hunting and contact with wildlife | 47 (13.9) |
| Processing & consumption of inadequately cooked animal products | 0 (0) |
| I don’t know | 47 (13.9) |
| 7. How can we protect ourselves against MPOX? | |
| Use of antibiotics | 86 (25.4) |
| Proper hygiene such as handwash | 210 (61.9) |
| Practicing safe sex | 102 (30) |
| Vaccination against MPX | 240 (70.8) |
| None of the above | 0 (0) |
| I don’t know | 33 (9.7) |
| 8. Do you think hand hygiene is important to reduce the spread of viruses? | |
| Not important | 114 (33.6) |
| Averagely important | 70 (20.6) |
| Extremely important | 155 (45.7) |
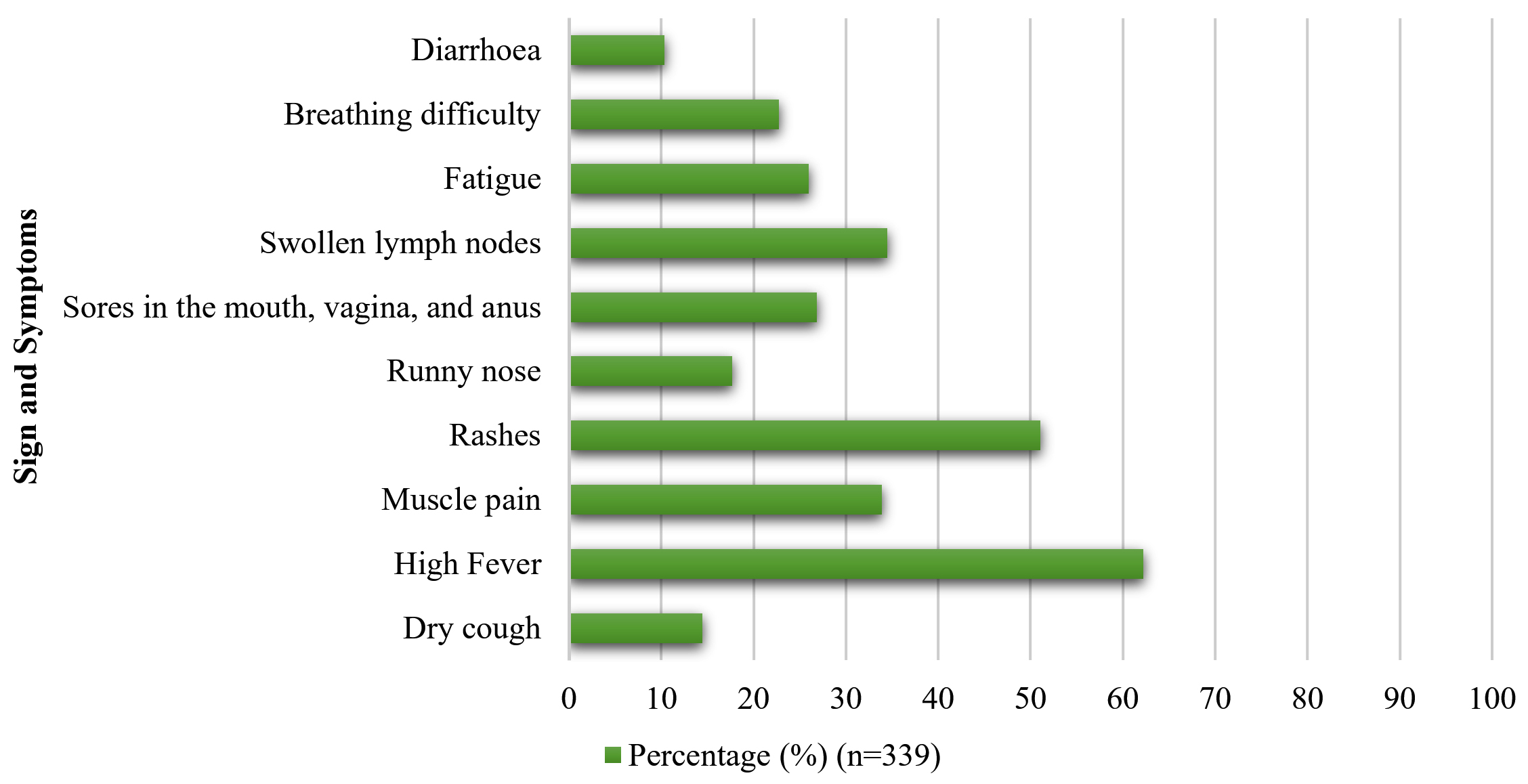
Figure. Awareness of signs and symptoms of MPOX among study participants (n=339)
Perception of the monkeypox disease
Although 72.2% (n=320/443) respondents had college or university degrees, less than half (36.8%, 163/443) of the respondents were aware that the MPXV can be transmitted through sexual intercourse. Most of the respondents (71.5%, 317/443) claimed that they knew the recommendations of the health ministry or government, but only 16.1% (51/443) of respondents followed all of the recommendations. Only 16.9% of the respondents (75/443) thought that health authorities have/are doing enough to safeguard public health, while around half of the respondents (52.6%, 233/443) believed that we can prevent such a global pandemic in the future. Regarding satisfaction with the media/social coverage of the monkeypox outbreak, 15.3% (68/443) respondents were very satisfied, 32.3% (143/443) were satisfied, and 30% (133/443) were averagely satisfied (Table 3).
Table (3):
Perception of monkeypox disease among respondents in Nepal (n=443)
| Variables | Frequency (%) |
|---|---|
| 1. Are you aware that the MPXV can be transmitted through sexual intercourse? | |
| I don’t know No Yes |
175 (39.5) 105 (23.7) 163 (36.8) |
| 2. Do you know the recommendations of your health ministry or government? | |
| Maybe No Yes |
93 (20.9) 33 (7.4) 317 (71.5) |
| 3. To which extent do you apply them? | |
| I follow all the recommendations. I follow most of them. I follow some but not all I do not follow any of the recommendations. |
51 (16.1) 173 (54.6) 87 (27.4) 6 (1.9) |
| 4. Are you currently on lockdown in your country (or your region of the country)? | |
| No Yes |
432 (97.5) 11 (2.5) |
| 5. Have you been vaccinated against monkeypox? | |
| No Yes |
435 (98.2) 8 (1.8) |
| 6. Do you think that your health authorities have/are doing enough to safeguard your health? | |
| Maybe No Yes |
167 (37.7) 201 (45.4) 75 (16.9) |
| 7. Do you think we can prevent such a global pandemic in the future? | |
| Maybe No Yes |
190 (42.9) 20 (4.5) 233 (52.6) |
| 8. How satisfied are you with the media/social coverage of the monkeypox outbreak? | |
| Very satisfied Satisfied Averagely satisfied Not satisfied Very dissatisfied |
68 (15.3) 143 (32.3) 133 (30.0) 65 (14.7) 34 (7.7) |
Bivariate logistic regression study did not find statistically significant relationships between age, sexual orientation, gender, education level, geographic location, and knowledge of MPOX (Table 4).
Table (4):
Analysis of sociodemographic variables as factors influencing the public knowledge of respondents towards the 2022 monkeypox outbreak
| Variables | Univariable analysis | ||||
|---|---|---|---|---|---|
| Satisfactory | Unsatisfactory | OR (95% CI) | p-value | ||
| Age (years) | 18 – 29 | 193 | 80 | 1.00 | – |
| 30 – 39 | 28 | 7 | 1.66 (0.69, 3.95) | 0.390 | |
| 40 – 49 | 18 | 5 | 1.49 (0.53, 4.15) | ||
| Gender | Male | 125 | 52 | 1.00 | – |
| Female | 114 | 40 | 1.18 (0.73, 1.92) | 0.490 | |
| Sexual orientation | Bisexual | 15 | 6 | 1.00 | – |
| Heterosexual | 189 | 60 | 1.11 (0.41, 2.98) | 0.356 | |
| Homosexual | 31 | 18 | 0.69 (0.23, 2.09) | ||
| Education | High School | 35 | 9 | 1.00 | – |
| College (Bachelor) | 173 | 74 | 0.60 (0.26, 1.31) | 0.300 | |
| Masters/Fellowship/PhD | 31 | 9 | 0.88 (0.31, 2.51) | ||
|
Geopolitical region |
Bagmati | 123 | 42 | 1.00 | – |
| Gandaki | 35 | 13 | 0.92 (0.44, 1.90) | 0.952 | |
| Lumbini | 71 | 29 | 0.84 (0.48, 1.46) | ||
| Madhesh | 10 | 5 | 0.68 (0.22, 2.11) | ||
| Koshi | 8 | 3 | 0.92 (0.23, 3.59) | ||
The global impact of the COVID-19 epidemic has been felt over the past three years.4,20 Not only did the COVID-19 epidemic have devastating health effects, but it also had widespread economic repercussions.4,21,22 Therefore, the announcement of the re-emergence of MPOX, its declaration of a global health emergency, and continuously rising cases may have harmful effects on societies regarding worry and anxiety,23,24 which coincides with the recent recovery of international systems from the pandemic’s consequences and the loosening of strict measures and restrictions on travel and personal communications. The increasing occurrence of epidemics and pandemics provide significant health difficulties for most resource-limited countries. Their ability to respond effectively to such situations might be negatively impacted by a lack of knowledge, which often leads to a casual attitude. The widespread consequences of outbreaks and pandemics may have a significant impact on the mental health of a population. The dread and anxiety that people feel in the face of a pandemic or epidemic have a significant impact on their actions and their emotions.25,26 This cross-sectional study aimed to gauge how well young people in Nepal understand the current MPOX pandemic. Previous research in other nations such as China,17,26 Bangladesh,27 Pakistan,28 Nigeria,29,30 and Iraq31 showed the knowledge gap of MPOX. It highlighted the need for health risk communication and educational awareness programs. To our knowledge, this is the first survey in Nepal among youths to focus on awareness and knowledge of MPOX.
The high awareness (76.5%) of MPOX among our study participants might be because of the high education level of the respondents and the widespread availability of internet public health advisories. Despite having high awareness, only 21.8% of respondents knew that MPOX could have asymptomatic cases, and around half of them didn’t know about the incubation period. Public enlightenment campaigns in Nepal should address wrong perceptions, including the notion that the disease can be transmitted via air droplets, mosquito/insect bites, and antibiotics, which could protect the MPOX. This poor perception could be due to the low burden of MPOX in Nepal while writing this manuscript. Similar to our study, university students in UAE had low knowledge of epidemiology, symptoms, and treatments of MPOX.32 Some 45.7% of our study participants regarded hand hygiene as highly significant in mitigating the transmission of MPXV, while 20.6% considered it moderately important. This trend could be attributed to the impact of COVID-19 campaigns and increased awareness, which have emphasized the significance of regular handwashing.
The knowledge that MPXV can be transmitted through sexual interaction is also largely unknown (26.8%). MPOX infections have been the subject of international discussion on whether or not they should be recognized as a sexually transmitted disease (STD). The MPOX disease is not an STD, even though it can be spread through intimate contact such as sexual activity.28,30 Since few people are aware that MPXV can be spread between people through sexual contact, this may lead to an inaccurate assessment of the danger posed by the virus and an increase in its spread. Reducing one-time sexual encounters by 40%, according to one study,33 could delay the spread of MPOX and lower the number of infected people by 20-31%. 61% of persons with confirmed cases of MPX also have MPXV in their blood.3,34 Most cases of human-to-human transmission in international clusters had preexisting conditions, especially human immunodeficiency virus (HIV/AIDS), which may have contributed to the false belief that only people who engage in unsafe sex or who have underlying conditions could be affected. According to research, 84% of participants with MPXV were either people living with HIV (PLWH) or users of HIV pre-exposure prophylaxis (PrEP).35,36
Impacts on efforts to contain other infectious diseases, such as MPOX, have arisen from the current COVID-19 pandemic. The public’s impression of the government’s response to the 2022 MPOX pandemic may be influenced by their view of how the government handled the COVID-19 epidemic. As a result, only 16.9% of respondents believed that Nepalese health officials were doing enough to protect public safety, and only 16.1% of respondents followed all of the health ministry’s recommendations and public health advisories. Lastly, it was encouraging to see that respondents were generally optimistic (52.6% positive) about the likelihood of averting the next global health crisis. The Nigerian public was likewise optimistic that we can stop or at least contain the next international health crisis.29 Increased contact with wildlife (especially due to population explosion), the capture, processing, sale, and consumption of game animals, and inadequate diagnostic infrastructure in resource-limited settings are all potential causes of the re-emergence of zoonotic diseases.17,30,31,37 Thus, it may be possible to slow the spread of the MPXV by investing in integrated surveillance at the interface between humans, animals, and ecosystems through a One Health approach. The recent discovery of MPXV reverse transmission from humans to animals (dogs) highlights the urgency of this issue.38
The limitation of this is that the participants were not chosen randomly, which makes the p-value less reliable. For this reason, it would be inappropriate to extrapolate our results to the entire Nepali people. In contrast, respondents’ sexual orientation and other socially undesirable background factors are less likely to influence the results of online polls.
The results of our study showed that MPOX awareness and knowledge are both above average. The mode of transmission, symptoms, and prevention methods of the disease were identified as major areas of poor knowledge. Nepal needs an effective preparedness plan to counteract any rise in MPOX cases. In addition, the introduction and spread of MPXV must be halted in Nepal, necessitating the strengthening of the country’s One-Health integrated disease surveillance system.
ACKNOWLEDGMENTS
The authors would like to acknowledge all the study participants.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to data collection, data analysis, manuscript preparation, and revision of the manuscript and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
ETHICS STATEMENT
The study was conducted in accordance with the Declaration of Helsinki and approved by Chitwan Medical College’s Institutional Review Committee (IRC) (CMC-IRC/077/078-031).
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Reynolds MG, Doty JB, McCollum AM, Olson VA, Nakazawa Y. Monkeypox re-emergence in Africa: a call to expand the concept and practice of One Health. Expert Rev Anti Infect Ther. 2019;17(2):129-139. doi
Crossref - CDC. Signs and Symptoms | Mpox | Poxvirus | CDC. 2023. https://www.cdc.gov/poxvirus/mpox/symptoms/index.html. Accessed November 23, 2023.
- Heskin J, Belfield A, Milne C, et al. Transmission of monkeypox virus through sexual contact – A novel route of infection. J Infect. 2022;85(3):334-363.
Crossref - Ahmed SK, Mohamed MG, Dabou EA, et al. Monkeypox (mpox) in immunosuppressed patients. F1000Res. 2023;12:127.
Crossref - Chakraborty S, Chandran D, Mohapatra RK, et al. Clinical management, antiviral drugs and immunotherapeutics for treating monkeypox. An update on current knowledge and futuristic prospects. Int J Surg. 2022;105:106847.
Crossref - Lai CC, Hsu CK, Yen MY, Lee PI, Ko WC, Hsueh PR. Monkeypox: An emerging global threat during the COVID-19 pandemic. J Microbiol Immunol Infect. 2022;55(5):787-794.
Crossref - ECDC. Risk assessment: Monkeypox multi-country outbreak. 2022. https://www.ecdc.europa.eu/en/publications-data/risk-assessment-monkeypox-multi-country-outbreak. Accessed November 23, 2023.
- WHO. 2022-23 Mpox (Monkeypox) Outbreak: Global Trends. 2023. https://worldhealthorg.shinyapps.io/mpx_global/. Accessed November 23, 2023.
- Dimitrakoff J. Monkeypox Virus Infection in Humans across 16 Countries – April-June 2022. N Eng J Med. 2022;387(25):e69.
Crossref - Bragazzi NL, Khamisy-Farah R, Tsigalou C, Mahroum N, Converti M. Attaching a stigma to the LGBTQI+ community should be avoided during the monkeypox epidemic. J Med Virol. 2023;95(1):e27913.
Crossref - Sah R, Mohanty A, Siddiq A, et al. Monkeypox reported in India – South East Asia Region: Health and economic challenges. Lancet Reg Health – Southeast Asia. 2022;4:100063.
Crossref - CDC. 2022 Mpox Outbreak Global Map | Mpox | Poxvirus | CDC. 2023. https://www.cdc.gov/poxvirus/mpox/response/2022/world-map.html. Accessed November 23, 2023.
- Bell DM. World Health Organization Working Group on Prevention of International and Community Transmission of SARS. Public Health Interventions and SARS Spread, 2003. Emerg Infect Dis. 2004;10(11):1900.
Crossref - Abdel Fattah FAM, Dahleez KA, Mohamed AHHM, Okour MK, AL Alawi AMM. Public health awareness: knowledge, attitude and behaviors of the public on health risks during COVID-19 pandemic in sultanate of Oman. Global Knowledge Memory and Communication. 2021;71(1-2):25-25.
Crossref - Berdida DJE. Population-based survey of human monkeypox disease knowledge in the Philippines: An online cross-sectional study. J Adv Nurs. 2023;79(7):2684-2694.
Crossref - Subedi D, Acharya KP. Risk of monkeypox outbreak in Nepal. Travel Med Infect Dis. 2022;49:102381.
Crossref - Ren F, Liu J, Miao J, et al. Public awareness, specific knowledge, and worry about mpox (monkeypox): A preliminary community-based study in Shenzhen, China. Front Public Health. 2023;11:1077564.
Crossref - WHO. Monkeypox – United Kingdom of Great Britain and Northern Ireland. 2022. https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON381. Accessed November 23, 2023.
- Harapan H, Setiawan AM, Yufika A, et al. Knowledge of human monkeypox viral infection among general practitioners: a cross-sectional study in Indonesia. Pathog Glob Health. 2020;114(2):68-75.
Crossref - PAHO. Mpox outbreak – PAHO/WHO | Pan American Health Organization. 2022. https://www.paho.org/en/mpox. Accessed November 23, 2023.
- Chandran D, Dhama K, Muhammad AMK, et al. Monkeypox: An Update on Current Knowledge and Research Advances. J Exp Biol Agric Sci. 2022;10(4):679-688.
Crossref - Ajman F, Alenezi S, Alhasan K, et al. Healthcare Workers’ Worries and Monkeypox Vaccine Advocacy during the First Month of the WHO Monkeypox Alert: Cross-Sectional Survey in Saudi Arabia. Vaccines (Basel). 2022;10(9):1408.
Crossref - Lounis M, Bencherit D, Abdelhadi S. Knowledge and awareness of Algerian healthcare workers about human monkeypox and their attitude toward its vaccination: An online cross-sectional survey. Vacunas. 2023;24(2):122-127.
Crossref - Alrasheedy AA, Aldawsari AH, Alqasir MI, et al. Knowledge of Community Pharmacists in Saudi Arabia Regarding Human Monkeypox, Its Management, Prevention, and Vaccination: Findings and Implications. Vaccines. 2023;11(4):878.
Crossref - Youssef D, Abboud E, Kawtharani M, Zheim Z, Abou Arrage N, Youssef J. When a neglected tropical zoonotic disease emerges in non-endemic countries: need to proactively fill the unveiled knowledge gaps towards human monkeypox among the Lebanese population. J Pharm Policy Pract. 2023;16(1):39.
Crossref - Zheng M, Qin C, Qian X, et al. Knowledge and vaccination acceptance toward the human monkeypox among men who have sex with men in China. Front Public Health. 2022;10:997637.
Crossref - Nath SD, Islam AMK, Majumder K, et al. Assessment of Knowledge on Human Monkeypox Virus among General Population in Bangladesh: A Nationwide Cross-sectional Study. medRxiv. 2022.
Crossref - Kumar N, Ahmed F, Raza MS, et al. Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan. Vaccines (Basel). 2022;11(1):97.
Crossref - Al-Mustapha AI, Ogundijo OA, Sikiru NA, et al. A cross-sectional survey of public knowledge of the monkeypox disease in Nigeria. BMC Public Health. 2023;23(1):591.
Crossref - Awoyomi OJ, Njoga EO, Jaja IF, et al. Mpox in Nigeria: Perceptions and knowledge of the disease among critical stakeholders-Global public health consequences. PLoS One. 2023;18(3):e0283571.
Crossref - Ahmed SK, Abdulqadir SO, Omar RM, et al. Knowledge, Attitude and Worry in the Kurdistan Region of Iraq during the Mpox (Monkeypox) Outbreak in 2022: An Online Cross-Sectional Study. Vaccines. 2023;11(3):610.
Crossref - Jairoun AA, Al-Hemyari SS, Abdulla NM, et al. Awareness and preparedness of human monkeypox outbreak among university student: Time to worry or one to ignore? J Infect Public Health. 2022;15(10):1065-1071.
Crossref - Spicknall IH, Pollock ED, Clay PA, et al. Modeling the Impact of Sexual Networks in the Transmission of Monkeypox virus Among Gay, Bisexual, and Other Men Who Have Sex with Men – United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(35):1131-1135.
Crossref - Raccagni AR, Mileto D, Canetti D, et al. Monkeypox and pan-resistant Campylobacter spp infection in Entamoeba histolytica and Chlamydia trachomatis re-infection in a man who have sex with men. J Infect. 2022;85(4):436-480.
Crossref - Jenness SM, Goodreau SM, Rosenberg E, et al. Impact of the Centers for Disease Control’s HIV Preexposure Prophylaxis Guidelines for Men Who Have Sex With Men in the United States. J Infect Dis. 2016;214(12):1800-1807.
Crossref - Raccagni AR, Candela C, Mileto D, et al. Monkeypox infection among men who have sex with men: PCR testing on seminal fluids. J Infect. 2022;85(5):573-607.
Crossref - Temsah MH, Aljamaan F, Alenezi S, et al. Monkeypox Disease (MPOX) Perceptions among Healthcare Workers versus General Population during the First Month of the WHO Alert: Cross-Sectional Survey in Saudi Arabia. Vaccines. 2022;10(12):2071.
Crossref - Seang S, Burrel S, Todesco E, et al. Evidence of human-to-dog transmission of monkeypox virus. Lancet. 2022;400(10353):658-659.
Crossref
© The Author(s) 2024. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.