


ISSN: 0973-7510
E-ISSN: 2581-690X
Uropathogenic Escherichia coli (UPEC) is the leading cause of urinary tract infections worldwide. ESBL-producing UPEC poses an escalating public health threat, yet its molecular epidemiology remains completely uncharacterized in Yemen. A cross-sectional study of 400 urine samples was conducted in Sana’a, Yemen. ESBL production was phenotypically screened. Multiplex PCR detected fimH and papC, confirmed by Sanger sequencing. Of 180 UPEC isolates, 75 (41.7%) were ESBL-producers. ESBL production was significantly associated with ICU admission, diabetes, and urinary tract abnormalities (P < 0.001). Resistance to third-generation cephalosporins exceeded 95%. Meropenem (96.0%), imipenem (92.0%), and amikacin (82.7%) were the most effective agents. fimH was detected in 89.3% and papC in 86.7% of ESBL-UPEC isolates; 84% co-harbored both genes. Sequencing confirmed high identity to reference sequences (99.37% and 98.25%, respectively). This first molecular study from Yemen reveals a high prevalence of multidrug-resistant ESBL-UPEC harboring fimH and papC in both hospital and community settings, underscoring an urgent public health threat.
Uropathogenic E. coli, Extended-Spectrum β-lactamase, Type 1 Fimbriae, P Fimbriae, Virulence Factors, Sequencing, Yemen
Urinary tract infections (UTIs) impose a substantial burden on global healthcare systems. Uropathogenic Escherichia coli (UPEC) is the leading cause of UTIs, responsible for nearly 80% of community-acquired and approximately 50% of hospital-acquired infections.1,2 The emergence of antibiotic resistance in UPEC, particularly via extended-spectrum β-lactamase (ESBL) production, has become a critical public health concern.3
ESBL enzymes (CTX-M, TEM, and SHV) confer resistance to penicillins and third-generation cephalosporins. These enzymes have driven the emergence of multidrug-resistant (MDR) superbugs harboring diverse resistance genes.3,4 The growing dissemination of ESBL-producing UPEC leads to prolonged illness, therapeutic failure, and substantially higher healthcare costs.5,6
Multiple virulence factors enable ESBL-UPEC to colonize and invade the urinary tract.4 Adhesion genes are particularly critical during the initial stages of infection. The fimH gene (type 1 fimbriae) mediates bacterial attachment to bladder cells through D-mannose binding, thereby initiating colonization and biofilm formation.6,7
The papC gene encodes the P fimbrial usher protein, which binds to receptors on kidney epithelial cells and is strongly associated with pyelonephritis.6,7 Co-carriage of both adhesion genes (fimH and papC) alongside multidrug-resistance complicates clinical management and limits therapeutic options.
Despite extensive global research on ESBL and virulence gene genetics in UPEC, no molecular data exist from Yemen. To date, no study has characterized virulence genes in ESBL-producing UPEC strains from this region. Given their well-established roles in UPEC pathogenesis and resource limitations, this pilot study focused on fimH and papC as representative adhesion factors, acknowledging that a broader panel of virulence genes (e.g., afa, sfa, hlyA, cnf1, and iron acquisition genes) remains to be investigated.
Therefore, this study represents the first comprehensive molecular investigation of ESBL-producing UPEC in Yemen. Our objectives were to determine the incidence and antimicrobial resistance profiles of ESBL-UPEC and to characterize the virulence genes fimH and papC.
Study Design, Study Population, and Eligibility Criteria
This cross-sectional study was conducted at Al-Kuwait University Hospital in Sana’a City, Yemen, between April 2024 and April 2025. Ethical approval was obtained from the Committee of the Biological Department, Microbiology Branch, Faculty of Science, Sana’a University (approval no. 825-9). A consecutive sampling technique was employed: all patients presenting with suspected urinary tract infections (UTIs) during the study period who met the eligibility criteria were invited to participate. A total of 180 E. coli isolates were recovered from 400 midstream urine samples collected at the hospital. Prior to collection, all patients received standardized verbal and written instructions for obtaining a clean-catch midstream urine specimen. Samples were immediately stored at 4 °C and processed for culture within 24 hours. Demographic and clinical data were collected from all participants using a structured questionnaire.
Inclusion criteria
Patients of all ages and genders who provided informed consent and from whose urine samples a significant growth of E. coli (³ 105 CFU/mL) was isolated.
Exclusion criteria
Individuals who declined to participate, samples with insufficient volume, and specimens showing mixed bacterial growth or insignificant bacteriuria (< 105 CFU/mL) were excluded.
Identification of uropathogenic E. coli
Urine samples were inoculated onto blood agar and MacConkey agar (HiMedia, India) using a calibrated loop and incubated aerobically at 37 °C for 18-24 hours. Presumptive E. coli isolates were confirmed by Gram staining (Gram-negative bacilli) and the IMViC biochemical profile (indole positive, methyl red positive, Voges-Proskauer negative, citrate negative).6
Phenotypic confirmation of ESBL production
Phenotypic ESBL confirmation was performed using the Double-Disk Synergy Test (DDST).8 A Mueller-Hinton agar plate was inoculated with a 0.5 McFarland bacterial suspension. An amoxicillin-clavulanic acid disk (20/10 µg) was placed centrally, with ceftazidime (30 µg), cefotaxime (30 µg), and aztreonam (30 µg) disks positioned 20 mm from the center. After incubation (35 ± 2 °C, 16-18 hours), a positive result was defined as a “keyhole” effect synergistic enhancement of any antibiotic inhibition zone toward the central disk.
Antimicrobial susceptibility testing and screening for ESBL producers
Antimicrobial susceptibility was determined using the Kirby-Bauer disk diffusion method following CLSI M100 guidelines.8 E. coli ATCC® 25922 served as the quality control strain in each run. Following incubation, inhibition zone diameters were measured, and isolates were categorized as susceptible, intermediate, susceptible-dose dependent, or resistant according to CLSI M100, 33rd edition (2023), breakpoints.8
Storage of bacterial isolates
To preserve the viability and genetic integrity of the confirmed ESBL- producing uropathogenic E. coli isolates for downstream molecular analyses, a cryopreservation protocol was implemented. Following daily confirmation, the isolates were resuspended in a cryoprotectant solution of nutrient broth (HiMedia, India) supplemented with 10% (v/v) glycerol. The suspensions were then aliquoted into cryovials and stored at -20 °C for short-term preservation.9
Molecular identification
All ESBL-producing UPEC isolates were screened for the fimH and papC genes using a multiplex polymerase chain reaction (PCR) assay.
DNA extraction genomic
Genomic DNA was extracted using the Bioneer Exgene™ Kit (K-3032G, Bioneer, Korea) according to the manufacturer’s protocol. DNA purity (A260/280 ratio = 1.8-2.0) was confirmed using a Genova Nano spectrophotometer.
Polymerase Chain Reaction (PCR)
A single-tube multiplex assay was performed to detect both fimH and papC adhesion genes. Each 20 µL reaction mixture contained 10 µL of 2 × master mix, 2 µL of primer mix (10 µM each; final concentration 1.0 µM per primer), 4 µL of DNA template, and 4 µL of nuclease-free water. Negative (nuclease-free water) and positive (E. coli ATCC® 25922) controls were included in each run. The primer sequences and target amplicon sizes are provided in Table 1.
Table (1): Characteristics of oligonucleotide primers for multiplex PCR
| Target Gene | Base Pair | Primer Sequence (5′ → 3′) | Stock (µM) | Ref. |
|---|---|---|---|---|
| fimH | 508 bp | F: TCGAGAACGGATAAGCCGTGG | 100 µM | 12 |
| R: GCAGTCACCTGCCCTCCGGTA | ||||
| papC | 200 bp | F: GTGGAGTATGAGTAATGACCGTTA | 100 µM | 12 |
| R: ATATCCTTTCTGCAGGGATGCAATA |
Note: F, forward; R, reverse. All primers were reconstituted with nuclease-free water (H2O) to obtain a 100 µM stock solution. The final concentration in the PCR reaction was 1.0 µM per primer
Thermal cycling
Initial denaturation at 95 °C for 5 minutes; 35 cycles of denaturation at 95 °C for 30 seconds, annealing at 54 °C for 30 seconds, and extension at 72 °C for 35 seconds; followed by a final extension at 72 °C for 5 minutes.
Electrophoresis
PCR products were resolved by electrophoresis on a 1% agarose gel stained with ethidium bromide. A 100 bp DNA ladder was used as a size marker, and amplicons were visualized under ultraviolet (UV) light.
DNA sequencing
Purified PCR products were submitted to Genome Medical Company (Amman, Jordan) and forwarded to Macrogen Europe (Milan, Italy) for bidirectional Sanger sequencing using the BigDye® Terminator v3.1 Kit on an ABI 3730xl DNA Analyzer. Sequence chromatograms and trimmed consensus sequences were provided by the sequencing facility. The obtained sequences were deposited in GenBank, and sequence identities were confirmed using NCBI BLASTn.
Statistical analyses
Data were analyzed using SPSS statistical software version 25 (IBM Corp., Armonk, NY, USA). Univariate analysis was performed using the chi-square (χ²) test. Odds ratios (OR) with 95% confidence intervals (CI) were calculated to assess associations between categorical variables. A P-value <0.05 was considered statistically significant.
Prevalence of uropathogenic E. coli
Of the 400 midstream urine samples processed, 180 (45.0%) yielded significant growth of E. coli and were confirmed as uropathogenic E. coli (UPEC). Among these 180 isolates, 105 (58.3%) were classified as non-ESBL producers, while 75 (41.7%) were confirmed as ESBL producers using the double-disk synergy test (DDST).
Association of ESBL-UPEC infections with demographic and clinical characteristics
Among the 180 UPEC isolates, 75 were ESBL producers. Inpatient status was associated with higher odds of ESBL production (odds ratio [OR] = 2.19; 95% confidence interval [CI]: 1.18-4.06); however, this association did not reach statistical significance (P = 0.059). No significant associations were observed between ESBL production and sex (P = 0.157) or age group (P = 0.209). Detailed demographic and clinical characteristics are presented in Table 2.
Table (2): Demographic and clinical characteristics of patients with ESBL-producing and non-ESBL UPEC infections
| Characteristic | Category | ESBL-UPEC (n = 75) | Non-ESBL UPEC (n = 105) | P-value | Chi-Square | Odds Ratio (95% CI) |
|---|---|---|---|---|---|---|
| Age Group (years) | <20 | 8 (10.7%) | 17 (16.2%) | 0.209 | 4.53 | – |
| 21-40 | 45 (60%) | 50 (47.6%) | ||||
| 41-60 | 17 (22.6%) | 23 (21.9%) | ||||
| >60 | 5 (6.7%) | 15 (14.3%) | ||||
| Sex | Male | 23 (30.6%) | 43 (40.6%) | 0.157 | 2.00 | 1.55 (0.83-2.89) |
| Female | 52 (69.3%) | 62 (59.1%) | ||||
| Patient Type | Inpatient | 35 (46.7%) | 30 (28.6%) | 0.059 | 3.56 | 2.19 (1.18-4.06) |
| Outpatient | 40 (53.3%) | 75 (71.4%) |
Note: Chi-square ≥3.84 (significant), P-value: ≤0.05 (significant)
Risk factors and ESBL-UPEC infections
As shown in Table 3, ICU admission, urinary tract deformity, heart disease, and diabetes were significantly associated with ESBL-UPEC infections (P < 0.001). History of surgery (P = 0.589) and prostatic disease (P = 0.747) were not significantly associated.
Table (3): Association of clinical risk factors for ESBL-producing UPEC infection
Risk Factor |
Non-ESBL UPEC (n = 105) (%) |
ESBL UPEC (n = 75) (%) |
P-value |
Odds Ratio (95% CI) |
|---|---|---|---|---|
Urinary Deformity |
15 (14.3%) |
30 (40%) |
4 (1.9 – 8.2) |
|
Diabetes |
32 (30.5%) |
41 (54.7%) |
2.7 (1.5 – 4.9) |
|
Heart Disease |
22 (21%) |
32 (42.7%) |
2.8 (1.5 – 5.3) |
|
ICU Admission |
2 (1.9%) |
19 (25.3%) |
17.1 (3.9 – 75.4) |
|
Surgery |
19 (18.1%) |
16 (21.3%) |
0.5890 |
1.2 (0.6 – 2.5) |
Prostatic Disease |
11 (10.5%) |
9 (12%) |
0.7470 |
1.2 (0.5 – 2.9) |
Antibiotic susceptibility profiles
ESBL-producing UPEC isolates demonstrated high levels of resistance to third-generation cephalosporins (³95%). The most effective antibiotics were meropenem (96.0% susceptible), imipenem (92.0%), and amikacin (82.7%). Nitrofurantoin exhibited only moderate activity (46.7% susceptible). The complete antimicrobial susceptibility profile is detailed in Table 4.
Table (4): Antimicrobial susceptibility profile of 75 extended-spectrum
| Antibiotic | ESBL Isolates (n = 75) | ||
|---|---|---|---|
| Susceptible (%) | Intermediate (%) | Resistant (%) | |
| Amikacin | 62 (82.7%) | 3 (4.0%) | 10 (13.3%) |
| Gentamicin | 48 (64.0%) | 3 (4.0%) | 24 (32.0%) |
| Tobramycin | 40 (53.3%) | 5 (6.7%) | 30 (40.0%) |
| Ampicillin | 0 | 1 (1.3%) | 74 (98.6%) |
| Amoxicillin-Clavulanate | 40 (53.3 %) | 2 (2.7%) | 33 (44.0%) |
| Cefepime (4th generation) | 2 (2.7%) | 1 (1.3%) | 72 (96.0) |
| Cefotaxime (3rd generation) | 0 | 1 (1.3%) | 74 (98.7) |
| Ceftazidime (3rd generation) | 0 | (4.0%)3 | 72 (96.0) |
| Cefoxitin (2nd generation) | 45 (60%) | 6 (6.7%) | 25 (33.3%) |
| Aztreonam | 0 | 4 (5.3%) | 71 (94.7%) |
| Meropenem | 72 (96.0%) | 2 (2.7%) | 1 (1.3%) |
| Imipenem | 69 (92.0%) | 4 (5.3%) | 2 (2.7%) |
| Ciprofloxacin | 25 (33.3%) | 5 (6.7%) | 45 (60.0%) |
| Levofloxacin | 35 (46.7%) | 6 (8.0%) | 34 (45.3%) |
| Nalidixic Acid | 3 (4.0%) | 2 (2.7%) | 70 (93.3%) |
| Chloramphenicol | 20 (26.7%) | 6 (8.0%) | 49 (65.3%) |
| Nitrofurantoin | 35 (46.7%) | 7 (9.3%) | 33 (44.0%) |
| Piperacillin-Tazobactam | 30 (40.0%) | 7 (9.3%) | 38 (50.7%) |
| Tetracycline | 14 (18.7%) | 2 (2.7%) | 59 (78.7%) |
Distribution of virulence genes in ESBL-producing UPEC
Among the 75 ESBL-UPEC isolates, 67 (89.3%) tested positive for the fimH gene, 65 (86.7%) tested positive for the papC gene, and 63 (84.0%) harbored both genes concurrently. Specifically, 4 isolates (5.3%) harbored fimH only, 2 isolates (2.7%) harbored papC only, and 6 isolates (8.0%) lacked both genes. A representative agarose gel image showing the amplification of fimH (508 bp) and papC (200 bp) is presented in Figure.
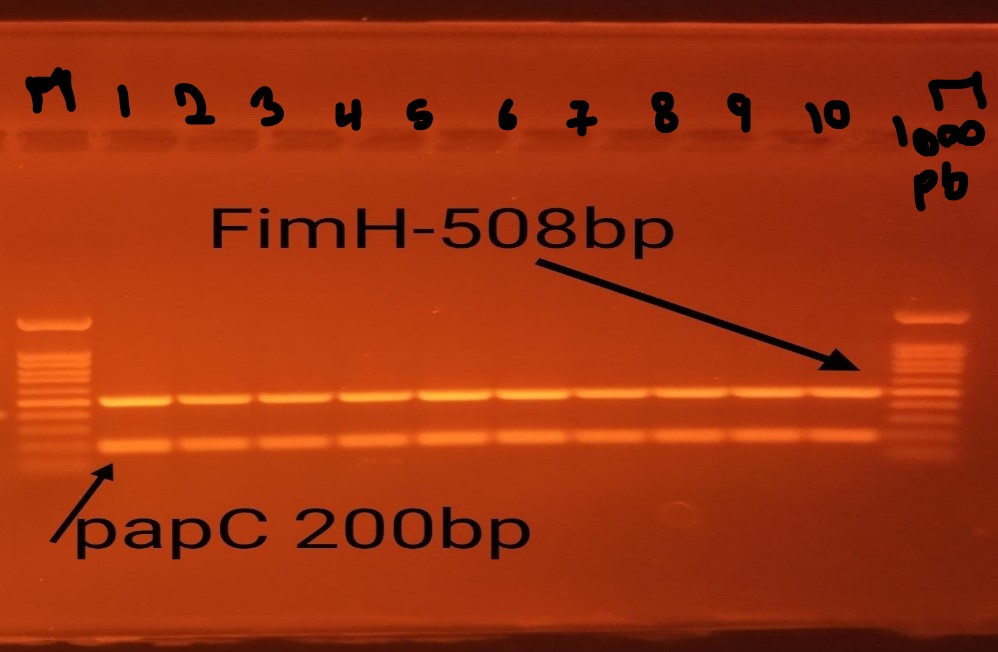
Figure. Agarose gel image showing the fimH (508 bp) and papC (200 bp) virulence genes in ESBL UPEC isolates
Association of virulence genes with clinical syndromes and clinical risk factors
Cystitis was significantly associated with the presence of both fimH (P = 0.01) and papC (P = 0.01). No significant associations were observed between either virulence gene and ICU admission, diabetes mellitus, heart disease, or urinary tract abnormalities. A non-significant trend was observed between papC carriage and post-surgical status (P = 0.083). Both genes were more frequently detected in outpatients than in inpatients, although this difference was not statistically significant.
Nucleotide sequencing and GenBank deposition
Bidirectional Sanger sequencing of the fimH and papC amplicons yielded high-quality chromatograms and trimmed consensus sequences. BLASTn analysis of the fimH sequence revealed 99.37% identity with the fimH gene located on the chromosomes of Escherichia coli strains 22AR0747, MLI109, and R12 (GenBank accession numbers CP195459.1, CP117008.1, and CP066740.1, respectively). The fimH DNA sequence generated in this study was deposited in GenBank under accession number PX893128.
The DNA sequence of both genes generated in this study was deposited in GenBank under the accession number as shown in Table 5.
Table (5): Determination of accession numbers by GenBank
Sequence_ID |
Identifier Organism GenBank accession number |
|---|---|
PX893128 |
fimH |
PZ454262 |
papC |
This study provides the first comprehensive analysis presenting molecular epidemiological data on ESBL-producing uropathogenic E. coli (UPEC) from Yemen, revealing a high prevalence of multidrug-resistant clones that are increasingly community-associated and harbor a potent combination of virulence genes.
The prevalence of ESBL-producing UPEC in Sana’a was 41.7%, and these isolates exhibited multidrug resistance. This rate is consistent with a report from Eastern India.10
Therefore, our demographic analysis showed increased infection rates among females and the 21-40 age group, consistent with global data where anatomical factors and sexual activity are well-known contributors.11-14 Community-driven spread of ESBL-UPEC has also been reported in Saudi Arabia15 and China.16 In our study, 60% of ESBL-UPEC infections were community-acquired, indicating widespread community dissemination.16
Also, analysis revealed significant associations between ESBL-UPEC and several risk factors, including ICU admission, diabetes, and urinary tract abnormalities. These conditions may create a vicious cycle: predisposing patients to recurrent infections, prompting repeated antibiotic use, and thereby driving further resistance selection and spread.17-20
Our susceptibility data reveal a critical treatment challenge in Yemeni clinics. Resistance rates reached 98.7% for cefotaxime and 60.0% for ciprofloxacin, rendering third-generation cephalosporins and fluoroquinolones unreliable for empirical UTI treatment. Consequently, clinicians have limited options, necessitating alternative agents such as amikacin (82.7% susceptible). These findings align with reports from Ethiopia18 and Egypt21 and are supported by studies from Iran and China advocating combination therapy.22,23
Polymerase chain reaction (PCR) analysis detected fimH in 89.3% and papC in 86.7% of ESBL-UPEC isolates. The high prevalence of fimH is expected, as this gene is commonly found in both pathogenic and commensal E. coli. In contrast, papC is more specifically associated with uropathogenic strains.23-28 No association was found between fimH or papC and clinical syndrome, a finding possibly attributable to the limited sample size. This contrasts with a Colombian study that reported a significant association between fimH-positive ESBL-UPEC and ICU admission (OR 5.63; 95% CI 1.92-16.53; P = 0.002).28 In the present study, virulence genes were most prevalent among outpatients, but no association was found with inpatient or outpatient status. This agrees with a Peruvian study reporting a higher fimH prevalence among outpatients (68.9%) than inpatients (31.1%).15
In addition, sequencing confirmed that the amplified product was the type 1 fimbrial adhesin gene (fimH) from Escherichia coli, showing high identity to known sequences (e.g., XNP_02010.1)29. The fimH sequence was deposited in GenBank under accession number PX893128. Furthermore, BLASTN and BLASTX analyses identified the 174 bp amplicon as a fragment of the papC gene, which encodes the P fimbrial usher protein – a critical virulence factor in uropathogenic E. coli.30 The papC sequence was deposited in GenBank under accession number PZ454262.
This study reveals a critical public health concern in Sana’a, Yemen. Among UPEC isolates, 41.7% were ESBL producers and demonstrated resistance to commonly used antibiotics. Notably, the majority of ESBL-UPEC cases (60%) occurred in outpatients, indicating that antimicrobial resistance is now a community-wide problem. Furthermore, most isolates harbored the adhesion genes fimH (89.3%) and papC (86.7%), which may contribute to pathogenicity. These findings underscore the urgent need for enhanced antimicrobial stewardship, routine surveillance, and infection control measures in both hospital and community settings in Yemen.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
Both authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Committee of the Biological Department, Microbiology Branch, Faculty of Science, Sana’a University (no. 825-9).
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Gaviria L, Montsant L, Azuaje C, et al. A descriptive analysis of urinary ESBL-producing Escherichia coli in Cerdanya Hospital. Microorganisms. 2022;10(3):488.
Crossref - Pandey A, Khandait M, Sandhya. To study the prevalence of extended-spectrum β-lactamase (ESBL)- producing uropathogenic Escherichia coli(UPEC) and its antibiotic sensitivity pattern around the semi-urban region of Gurugram. J Neonatal Surg. 2025;14(16):317-326.
- Naziri Z, Derakhshandeh A, Borchaloee AS, Poormaleknia M, Azimzadeh N. Treatment failure in urinary tract infections: a warning witness for virulent multi-drug resistant ESBL-producing Escherichia coli. Infect Drug Resist. 2020;13:1839-1850.
Crossref - Whelan S, Lucey B, Finn K. Uropathogenic Escherichia coli(UPEC)-associated urinary tract infections: the molecular basis for challenges to effective treatment. Microorganisms. 2023;11(9):2169.
Crossref - Gupta S, Kumar P, Rathi B, et al. Targeting of uropathogenic Escherichia coli papG gene using CRISPR-dot nanocomplex reduced the virulence of UPEC. Sci Rep. 2021;11(1):17801.
Crossref - Hasan SM, Ibrahim KS. Molecular characterization of extended spectrum β-lactamase (ESBL) and virulence gene factors in uropathogenic Escherichia coli(UPEC) in children in Duhok City, Kurdistan Region, Iraq. Antibiotics. 2022;11(9):1246.
Crossref - Matsukawa M, Igarashi M, Watanabe H, et al. Epidemiology and genotypic characterization of dissemination patterns of uropathogenic Escherichia coli in a community. Epidemiol Infect. 2019;147:e148.
Crossref - Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. 33rd ed. CLSI supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute. 2023.
- Tuttle AR, Trahan ND, Son MS. Growth and maintenance of Escherichia coli laboratory strains. Curr Protoc. 2021;1(1):e20.
Crossref - Behera B, Debbarma M, Rout B, et al. Prevalence of ESBL-producing bacteria in community-acquired UTI from the eastern part of India. J Pure Appl Microbiol. 2022;16(3):1682-1688.
Crossref - Razaq L, Uddin F, Ali S, Ali S, Kausar R, Sohail M. Extended-spectrum β-lactamase variants in Escherichia coli, Klebsiella pneumoniae and Proteus mirabilis from community- and hospital-acquired urinary tract infections. Gene Rep. 2024;37:102065.
Crossref - Ghazvini H, Taheri K, Edalati E, Miri A, Sedighi M, Mirkalantari S. Virulence factors and antimicrobial resistance in uropathogenic Escherichia coli strains isolated from cystitis and pyelonephritis. Turk J Med Sci. 2019;49(1):361-367.
Crossref - Moubayed N, Ghazzawi R, Mitri C, Khalife S. Recent data characterizing the prevalence and resistance patterns of fimH-producing uropathogenic Escherichia coli isolated from patients with urinary tract infections in North Lebanon. Arch Clin Infect Dis. 2023;18(4):e135782.
Crossref - Alghamdi SAA, Mir SS, Alghamdi FS, Banghali MAMMAA, Almalki SSR. Evaluation of extended-spectrum beta-lactamase resistance in uropathogenic Escherichia coli isolates from urinary tract infection patients in Al-Baha, Saudi Arabia. Microorganisms. 2023;11(12):2820.
Crossref - Jia P, Zhu Y, Li X, et al. High prevalence of extended-spectrum beta-lactamases in Escherichia coli strains collected from strictly defined community-acquired urinary tract infections in adults in China:a multicenter prospective clinical microbiological and molecular study. Front Microbiol. 2021;12:663033.
Crossref - Ahn ST, Lee HS, Han DE, et al. What are the risk factors for recurrent UTI with repeated ESBL-producing Enterobacteriaceae? A retrospective cohort study. J Infect Chemother. 2023;29(1):72-77.
Crossref - Vachvanichsanong P, McNeil EB, Dissaneewate P. Extended-spectrum beta-lactamase Escherichia coli and Klebsiella pneumoniae urinary tract infections. Epidemiol Infect. 2021;149:e12.
Crossref - Omar MH, Kilale AM, Rashid HK, Mwakapeje ER, Onoka IM, Gimbi AA. Prevalence and risk factors for extended-spectrum β-lactamase- producing antimicrobial-resistant E. coli in urinary tract infections among inpatients in the tertiary hospitals in Zanzibar. Pan Afr Med J. 2024;47:193.
Crossref - Aworh MK, Kwaga J, Okolocha E, Mba N, Thakur S. Prevalence and risk factors for multidrug-resistant Escherichia coli among poultry workers in the Federal Capital Territory, Abuja, Nigeria. PLoS One. 2019;14(11):e0225379.
Crossref - Alharazi T, Alhoot MA, Alzubiery TK, et al. Increasing resistance of nosocomial and community-acquired Escherichia coli in clinical samples from hospitals and clinics in Sana’a City. J Pure Appl Microbiol. 2024;18(3):1741-1751.
Crossref - Khater ES, Sherif HW. Association between virulence factors and antibiotic resistance in E. coli isolated from urinary tract infection patients in Banha University Hospitals, Egypt. Merit Res J Microbiol Biol Sci. 2021;9(1):1-8.
Crossref - Memar MY, Vosughi M, Saadat YR, et al. Virulence genes and antibiotic susceptibility patterns of Escherichia coli isolated from nosocomial urinary tract infections in the northwest of Iran during 2022-2023:a cross-sectional study. Health Sci Rep. 2024;7(11):e70149.
Crossref - Zhong Z, Cui Z, Li X, et al. Nitrofurantoin combined with amikacin:a promising alternative strategy for combating MDR uropathogenic Escherichia coli. Front Cell Infect Microbiol. 2020;10:608547.
Crossref - Zhang L, Li F, Li X. Studies on virulence and extended-spectrum β-lactamase-producing uropathogenic Escherichia coli isolates and therapeutic effect of fosfomycin in acute pyelonephritis mice. Biomed Res Int. 2022;2022:8334153.
Crossref - Nivetha RM, Mariappan S, Sekar U, Aishwarya KV. Detection of virulence determinants of uropathogenic Escherichia coli. Cureus. 2025;17(2):e79116.
Crossref - Matta-Chuquisapon J, Valencia-Bazalar E, Marocho-Chahuayo L, Gonzales-Escalante E, Sevilla-Andrade C. Presence of fimH and afa genes in urinary isolates of extended-spectrum beta-lactamase – producing Escherichia coli in Lima, Peru. Rev Peru Med Exp Salud Publica. 2020;37(2):282-286.
Crossref - Mitsui M, Sekito T, Maruhashi M, et al. Distribution of fimbrial genes and their association with virulence and levofloxacin resistance/extended-spectrum beta-lactamase production in uropathogenic Escherichia coli. Antibiotics. 2025;14(5):468.
Crossref - Camargo-Mendoza J, Ariza-Rodrםguez D. Risk factors for health care-associated infections by ESBL-producing germs in an intensive care unit of a public hospital in Bogota, D.C., Colombia. Rev Fac Med. 2022;70(4):e92755.
Crossref - Sadredinamin M, Hakemi Vala M, Talebi G. FimH, partial [Escherichia coli]. National Center for Biotechnology Information. Published 2024.
- Huang Y, Smith BS, Chen LX, Baxter RH, Deisenhofer J. Insights into pilus assembly and secretion from the structure and functional characterization of usher PapC. Proc Natl Acad Sci USA. 2009;106(18):7403-7407.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.