


Carbapenem-resistant Acinetobacter baumannii (CRAB) poses a significant healthcare challenge worldwide because of its role in bloodstream infections, wound infections, and ventilator-associated pneumonia. A particularly concerning trait is its ability to develop multidrug-resistance and its unique capacity to endure extreme conditions that other microorganisms cannot withstand. This review delves into the microbiology of Acinetobacter spp., exploring their characteristics, molecular classification, and mechanisms of carbapenem-resistance, including the production of carbapenem-hydrolyzing β-lactamases (notably Oxacillinase (OXA-type), efflux pump activity, alterations in porin channels, and horizontal gene transfer. This paper emphasizes the rapid global dissemination of Acinetobacter spp. due to antibiotic misuse and improper treatment methods. Research also reveals that treatment options for these infections are severely limited, necessitating the development of new and innovative treatment strategies. To curb the spread of Acinetobacter spp., there is a pressing need to focus on advancements in diagnostics, control measures, antimicrobial stewardship programs, and new therapies such as vaccines and phage therapy. It is crucial to enhance disease diagnostics, invest in research and development of effective new drugs, and collaborate internationally to share knowledge about CRAB.
Hospital-acquired Infections, β-lactamases, Carbapenem-resistance, Acinetobacter baumannii, Multidrug-resistance, Antimicrobial Stewardship
Resistance to carbapenems among Acinetobacter spp., especially Acinetobacter baumannii, poses a global threat to healthcare systems due to the wide variety of antimicrobial agent resistance. Acinetobacter spp. are pathogens found in hospital settings; they pose a significant threat to hospital patients, employees, and the general public via their ability to cause pneumonia, bloodstream infections, and potentially lethal wounds. These pathogens cause infections with high mortality rates due to the presence of less effective drugs against these pathogens. Carbapenems are not effective against CRAB, and because of horizontal gene transfer (HGT), these CRAB are empowered with various carbapenem-resistant mechanisms, such as beta-lactamase production. CRAB can readily mutate, thereby developing multidrug resistance (MDR). CRAB can undergo HGT and mutations in genes involved in the production of carbapenem-hydrolyzing beta-lactamases, which are termed metallo-beta-lactamases (MBLs) and OXAs. Finally, they fortify the bacterial cell by changing the outer membrane porins in a way that renders carbapenem entry very difficult.1 Moreover, efflux pumps limit the amount of medications that bacteria may store in their bodies. The intricate process of carbapenem-resistance involves multiple genetic alterations, making it challenging to overcome.2
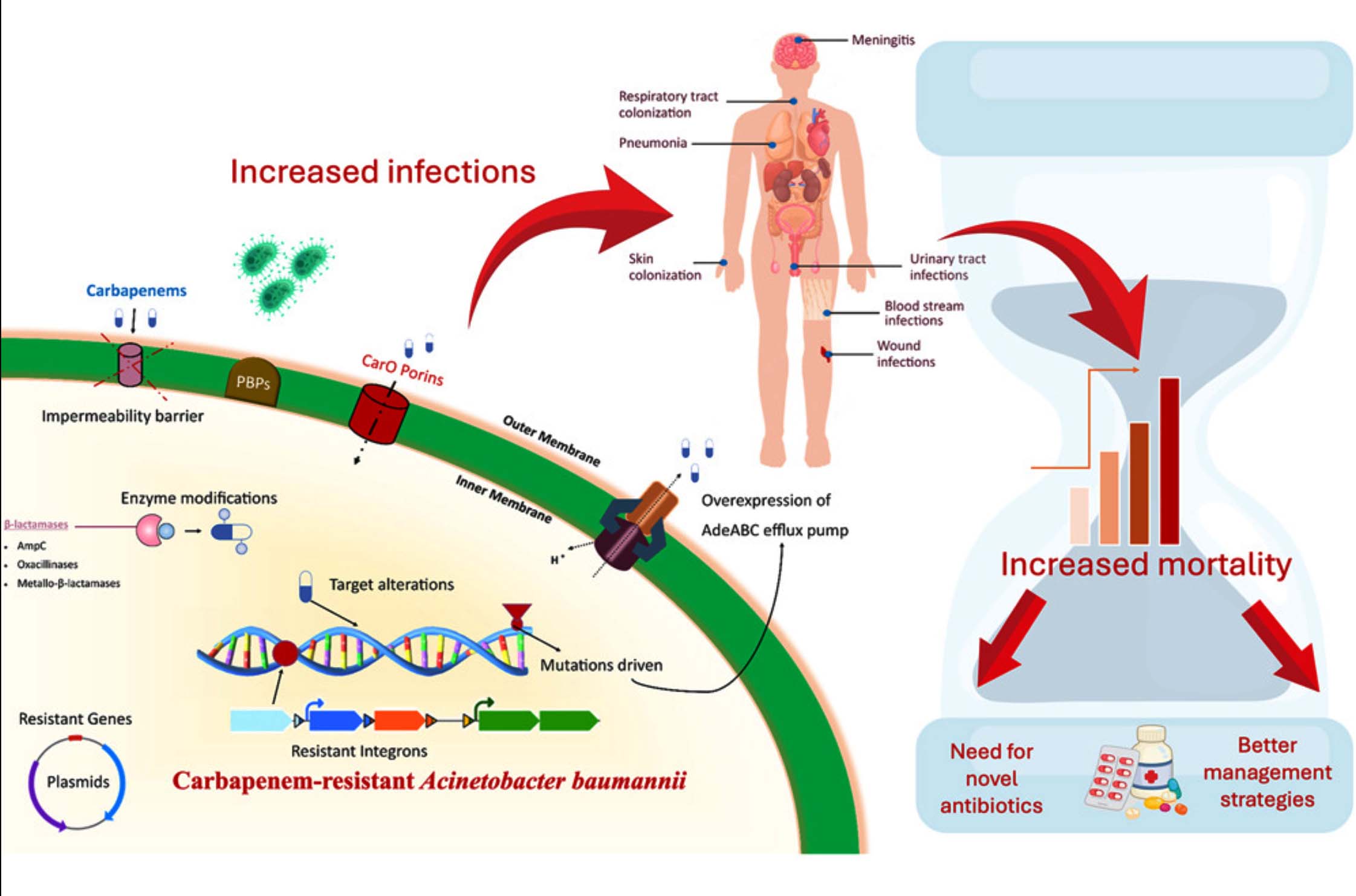
Figure 1. Carbapenem-resistant Acinetobacter baumannii3
Figure 1 shows the processes that lead to infections caused by CRAB.3 This emphasizes the role of genetic resistance factors in causing infections and deaths. Therefore, novel drugs and improved treatment techniques are urgently needed.4 Because of widespread reports of CRAB resistance, the presence of this microbe in intensive care units (ICUs) has prompted grave concerns about the spread of MDR pathogens, particularly CRAB. Anyone from the most developed nations to the least developed ones may find CRAB. The misuse of antibiotics, due to lack of knowledge on how to use them correctly, is a leading source of multidrug-resistant bacteria. The spread of CRAB is also a major concern worldwide because the resistance patterns are also found in communities and places other than hospitals.5 Hence, research on CRAB and how to address it has become very important before it becomes a major threat to the human race. Because carbapenem-resistant Acinetobacter is present in most of the public places, it can easily infect a person or worsen a sick person’s condition, incurring high medical bills. Once CRAB develops MDR, it can worsen a patient’s condition because of ineffective medications. Shortage of effective drugs against CRAB makes treatment difficult for the patients. Due to the lack of an effective vaccine, controlling and eradicating this Acinetobacter is difficult.6 To prevent MDR, effective research is needed on preventing the spread of CRAB.
Overview of Acinetobacter spp.
Soil, water, and healthcare facilities can host Acinetobacter spp. Acinetobacter spp. are aerobic coccobacilli that are oxidase-negative, non-motile, Gram-negative, and prevalent in the Earth’s ecosystem. Among the Acinetobacter spp., A. baumannii is the most hazardous. It is commonly isolated in healthcare facilities. The presence of this substance in the hospital environment poses a significant risk to patients who have already been hospitalized for other medical conditions are listed in Table 1. A. baumannii causes ventilator-associated pneumonia (VAP) and may infect the bloodstream, urinary tract, or wounds. Only a small fraction of the over 50 species with names pose any real threat to humans. The Acinetobacter baumannii, complex (ACB complex), which includes A. baumannii, Acinetobacter calcoaceticus, and Acinetobacter nosocomialis, is notoriously difficult to identify and halt mutations in using the standard and conventional procedures used by the vast majority of labs. Recently, species-level identification has been enhanced by molecular approaches, such as polymerase chain reaction (PCR) and mass spectrometry-based identification, Matrix-Assisted Laser Desorption/Ionization – Time of Flight. (MALDI-TOF). Their presence on dry surfaces and resistance to desiccation are the most harmful and spreadable traits. Thus, it can be concluded that this trait aids them during nosocomial epidemics. From the most dangerous (Acinetobacter baumannii) to the least dangerous (Acinetobacter lwoffii and Acinetobacter calcoaceticus), all Acinetobacter species are listed in Table 2, along with the illnesses they cause and their clinical relevance. This highlights their functions in healthcare-associated infections particularly in patients with impaired immune systems.
Table (1): General characteristics of Acinetobacter spp.
Characteristic |
Description |
|---|---|
Gram Stain |
Gram-negative coccobacilli |
Motility |
Non-motile |
Oxidase Reaction |
Oxidase-negative |
Catalase Reaction |
Catalase-positive |
Growth Conditions |
Aerobic, facultative anaerobic |
Habitat |
Environmental (soil, water); hospital settings |
Biofilm Formation |
Yes, often on medical devices |
Clinical Significance |
The major cause of hospital- acquired infections |
Table (2): Clinically relevant Acinetobacter species and associated infections
Acinetobacter |
Clinical Significance |
Common Infections |
|---|---|---|
A. baumannii |
Most pathogenic; major cause of HAIs |
Pneumonia, sepsis, wound infections |
A. nosocomialis |
Less virulent but still associated with infections |
UTIs, respiratory tract infections |
A. calcoaceticus |
Environmental; rarely pathogenic in humans |
Opportunistic infections in immuno- compromised |
A. lwoffii |
Generally non-pathogenic; occasional infections reported |
Skin, urinary tract |
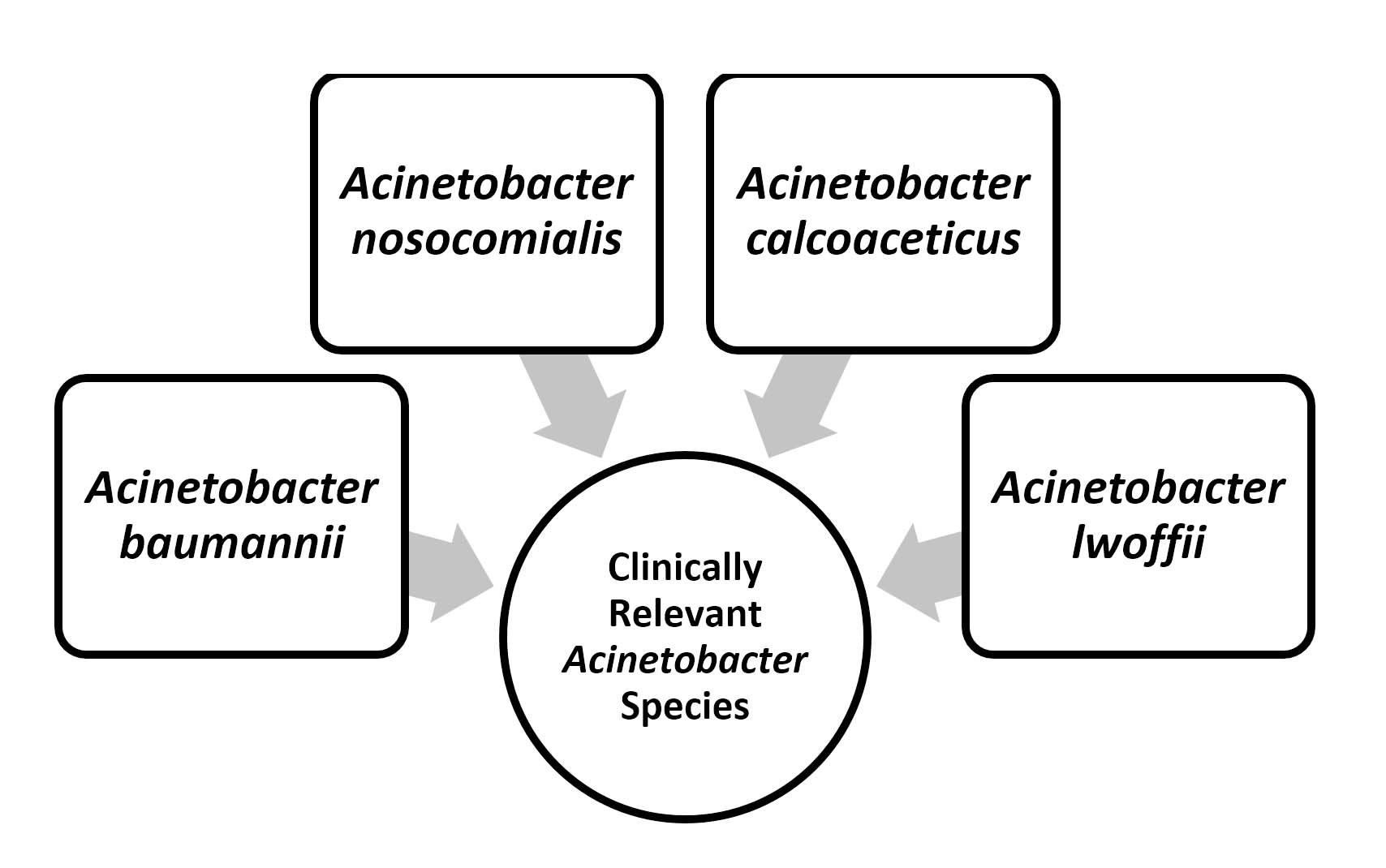
Figure 2. Clinically Relevant Acinetobacter species7
Figure 2 illustrates the clinically relevant Acinetobacter species, highlighting their varying levels of pathogenicity and the types of infections they cause, from severe hospital-acquired infections to opportunistic infections in immunocompromised patients.7
Importance of carbapenem-resistance in Acinetobacter
Acinetobacter infections are treated with carbapenem antibiotics, such as imipenem and meropenem. However, Acinetobacter has recently developed significant resistance to older and more rudimentary antibiotics, and this has become a great concern for communities worldwide. Due to alterations in membrane permeability and efflux pump overexpression, as well as the production of carbapenemases, namely OXA-type beta-lactamases and MBLs, Acinetobacter has evolved significant resistance against antibiotics.
Currently, CRAB leaves very little scope for treatment as it is nearly resistant to most of the available antibiotics on the market. The combination usually used for treatment is colistin and tigecycline, which can have many side effects and can be toxic. Due to the resistance shown by CRAB, the mortality rate, hospital expenses, and healthcare costs increase.8 Therefore, the World Health Organization (WHO) has identified CRAB as a global health concern and is allocating substantial resources to the research and development of novel antibiotics that may play a pivotal role in the eventual eradication of Acinetobacter.
For the removal and stoppage of Acinetobacter, the world must come and work together for global surveillance, enhanced diagnostic capabilities, and advanced methods to prevent the spread of infections. There is also a need to closely monitor day-to-day advancements in the resistance of CRAB and study the molecular mechanisms of CRAB for developing more effective drugs against Acinetobacter.
Objectives of the review
- To investigate the taxonomy, microbiological traits, and clinical relevance of Acinetobacter species, with an emphasis on A. baumannii and its function in healthcare-related illnesses.
- To investigate the biochemical and molecular processes underlying carbapenem-resistance in Acinetobacter species, including the functions of plasmid-mediated resistance genes, carbapenemases, efflux pumps, and porin mutations.
- To examine worldwide epidemiological trends and the transmission of Acinetobacter strains resistant to carbapenem, emphasizing geographical distribution, resistance patterns, and risk factors that contribute to the formation and spread of clones that are resistant to multiple drugs.
- To assess new therapeutic approaches, infection control procedures, antimicrobial stewardship, and future research directions, as well as existing and developing methods for the prevention, management, and treatment of carbapenem-resistant Acinetobacter infections.
Microbiology of Acinetobacter spp.
General characteristics of Acinetobacter
The bacterium Acinetobacter spp. is characterized by its lack of motility, aerobic metabolism, oxidase resistance, and catalase activity. The important characteristic of these bacteria is that they can adapt to environmental conditions, such as low temperature, high salinity, and desiccation. Due to these, Acinetobacter can live in the hospital environment of the ICU, which can prove fatal to hospital patients. There are almost 50 species of Acinetobacter, and the most common and devastating of them is A. baumannii, which has greater resistance to antibiotics and a high power to mutate itself according to the surroundings or antibiotics, thus causing a lot of infections to human beings than with any other Acinetobacter.
The Gram-negative outer membrane, which comprises the cell wall of Acinetobacter spp. aids in the development of resistance to several anti-bacterial medications. In addition to protecting catheters and ventilators from infection, CRAB (Acinetobacter spp.) forms biofilms on these tools, thereby increasing the risk of infection in hospitalized patients. Acinetobacter acquires resistance capabilities as a consequence of the genetic material that contributes to the formation of antibiotic resistance genes, which in turn produce clinical pathogenicity.9
Identification and classification of Acinetobacter species
Using Gram staining, biochemical tests, and antimicrobial susceptibility patterns, the Acinetobacter species can be easily identified and classified. The aforementioned phenotypic methods are not effective for all species because many species have overlapping characteristics. Multiple molecular methods, including PCR tests, 16S rRNA gene sequencing, and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS), have been used to determine the species of these Acinetobacter bacteria are included in Figure 3.
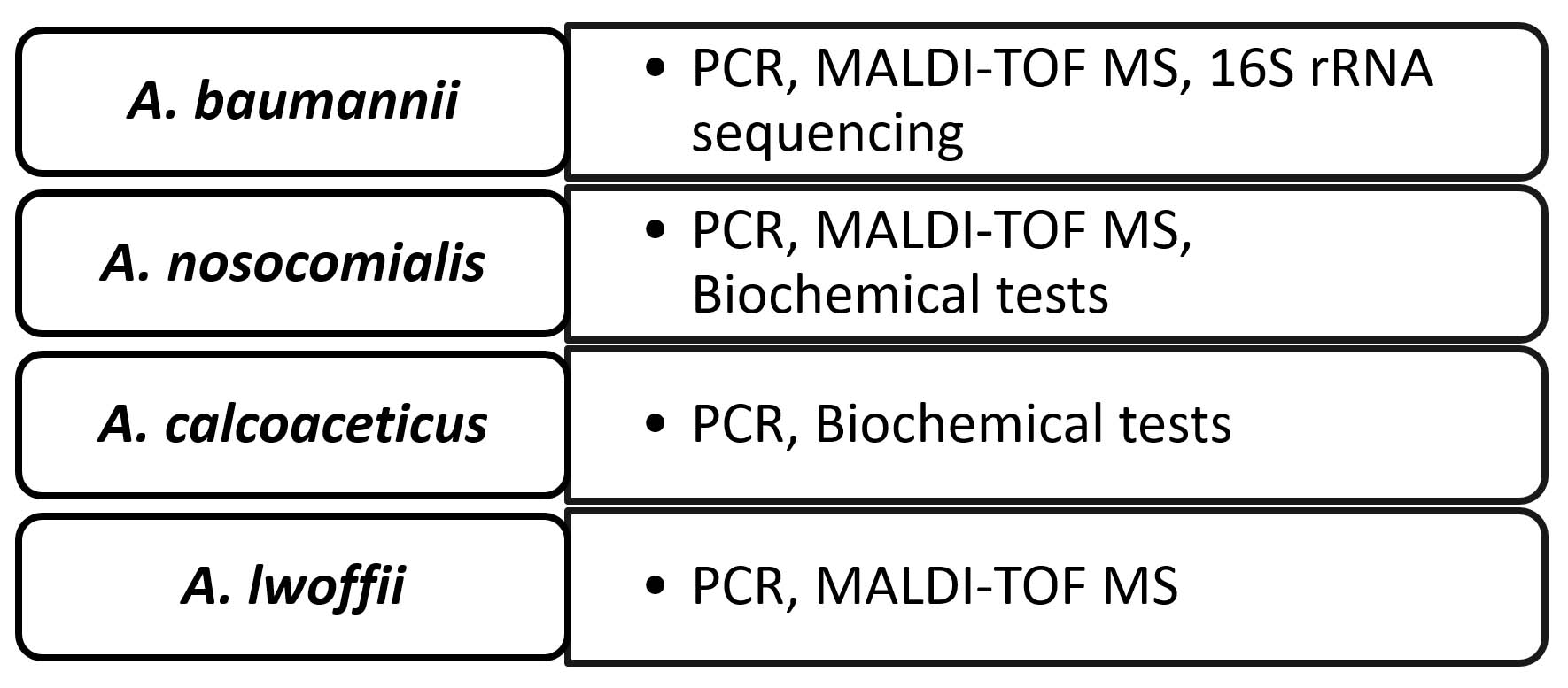
Figure 3. Key Acinetobacter Species and Identification Methods10
Differentiating between several species of Acinetobacter, most notably the Acinetobacter calcoaceticus-baumannii (ACB) complex, using conventional techniques is impossible.10 A. baumannii is the most common cause of illness because it is the most harmful Acinetobacter species. Although less dangerous, other ACB complex species, including Acinetobacter calcoaceticus and Acinetobacter nosocomialis, are important in clinical practice. Molecular typing methods such as pulsed-field gel electrophoresis and multilocus sequence typing (MLST) are used to monitor Acinetobacter strains that have developed resistance to many drugs and to obtain a better knowledge of the epidemiology of this bacterium. The key Acinetobacter species and the clinical importance of their identification techniques (e.g., PCR, MALDI-TOF MS, and biochemical assays) are included in Table 3 and Figure 4. Although Acinetobacter lwoffii is rarely pathogenic, A. baumannii is widely recognized as a significant nosocomial pathogen. This species causes opportunistic infections and infections in the respiratory system and urinary tract.11
Table (3): Key Acinetobacter species and identification methods
Abbrevation |
Identification Method |
Clinical Relevance |
|---|---|---|
A. baumannii |
PCR, MALDI-TOF MS, 16S rRNA sequencing |
Major nosocomial pathogen |
A. nosocomialis |
PCR, MALDI-TOF MS, Biochemical tests |
Urinary tract and respiratory infections |
A. calcoaceticus |
PCR, Biochemical tests |
Opportunistic infections in immunocompromised |
A. lwoffii |
PCR, MALDI-TOF MS |
Rarely pathogenic, occasional infections |
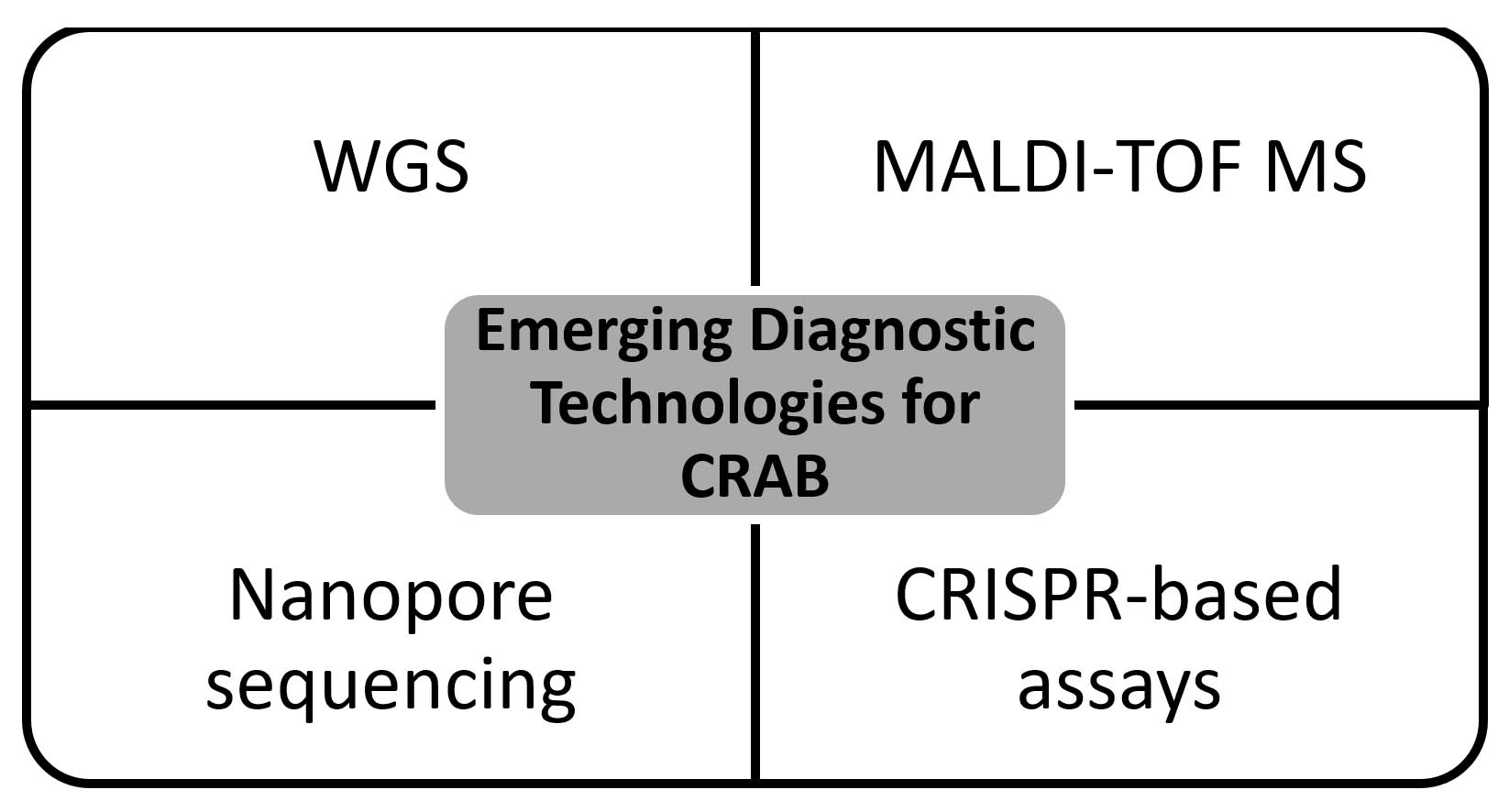
Figure 4. Emerging diagnostic technologies for CRAB11
Beta-lactamase production (Class A, B, C, and D)
A. baumannii can render carbapenems ineffective against most CARB by hydrolyzing their beta-lactam ring via the development of beta-lactamases. Serine beta-lactamases are classified into class A, MBLs into class B, ampC-type beta-lactamases into class C, and oxacillinases into class D. Class B MBLs and class D OXA-type beta-lactamases are the most prevalent kinds of beta-lactamases. Horizontal bacterial gene transfer occurs through plasmids or transposons. Most carbapenemases are of the OXA type. For example, the MBLs of the OXA-23, OXA-24, and OXA-58 varieties hydrolyze a variety of beta-lactams with relative ease. The presence of carbapenemases reduces the efficacy of antibiotics.12
OXA gene expression is facilitated by insertion sequence elements (ISs), such as ISAba1, ISAba4, and ISAba125, which provide strong promoters. CRAB contains virulence factors that affect disease progression. The global distribution of A. baumannii emerged in the 1970s through ‘international clones of high risk’ (ICs), with IC1 and IC2 first identified in nosocomial infections. GenBank data on the IC1-IC9 outbreaks show IC2 was the most prevalent CRAB clone. In South America, CRAB is linked to OXA-23 carbapenemases through clones IC1 (CC1), IC4 (CC15), IC5 (CC79), and IC7 (CC25), with IC2 (ST2) present across countries.
Intrinsic resistance occurs via bacterial outer membrane-blocking drugs and chromosomal AmpC β-lactamases. Acquired resistance includes: i) production of carbapenem hydrolyzing class D β-lactamases ii) metallo-β-lactamases (NDM 1) iii) aminoglycoside modifying enzymes within Figure 5. The RND family efflux pumps expel antimicrobials, whereas resistance develops through gyrA and parC mutations. These resistance determinants spread via HGT through plasmids, integrons, and transposons, leading to MDR organisms.13
Figure 5. Hydrolytic Mechanism of OXA-58 Enzyme, a Carbapenem-hydrolyzing Class D β-Lactamase from A. baumannii13
Porin channel mutations and reduced permeability
Porins were identified as the mechanisms responsible for carbapenem-resistance. The porin channels in the outer layer of Acinetobacter are highly permeable to small molecules and antibiotics. The Acinetobacter spp. makes the porin channels to reduce the influx of carbapenems and other antibiotics through various mutations, which causes antibacterial drug resistance and leads to a lot of infections in the human race.12 These mutations often occur in the carO gene, which encodes a major porin protein involved in carbapenem uptake. The reduction of these porins, which leads to increased resistance to MDR and carbapenems, is a direct result of the overuse and abuse of antibiotics.
Efflux pumps and their role in resistance
The antibiotic resistance in Acinetobacter is caused by efflux pumps. Due to efflux pumps, a large number of antibiotics and carbapenems are discharged or ejected from the bacterial cell body, thus making these antibiotics of no use. The Ade family of efflux pumps, particularly the AdeABC pump, plays a significant role in monitoring various antibiotics such as carbapenems, fluoroquinolones, and aminoglycosides.14
Genetic factors contributing to resistance
Some genetic factors, such as plasmids, transposons, and integrons, are responsible for carbapenem-resistance in Acinetobacter. Due to HGT, MDR strains are rapidly formed in bacteria, making them resistant to antibiotics. Mechanisms such as beta-lactamase production, efflux pump overexpression, and porin mutations are providing the power to Acinetobacter to develop multiple resistance mechanisms. These mechanisms enable Acinetobacter to adapt to various antimicrobial agents and to survive in different environments.
Role of HGT in resistance spread
HGT is the primary cause of MDR in Acinetobacter species. Conjugation, transformation, and transduction allow the rapid transmission of resistant genes from one species to another. The presence of HGT in hospitals is the main cause of the development of MDR Acinetobacter bacteria. The presence of OXA-type beta-lactamases or MBL in Acinetobacter or CRAB is responsible for the rapid transmission of these MDR strains.15
Global trends in carbapenem-resistant Acinetobacter infections
A. baumannii is a rising threat to Indian healthcare. In India, A. baumannii has become a major healthcare pathogen, with alarming antibiotic resistance rates. Infections are more prevalent in tertiary care hospitals and ICUs. An analysis of a North Indian tertiary care facility found that Gram-negative bacteria predominantly cause nosocomial infections. In India, from 307 clinical specimens, A. baumannii was mainly isolated from endotracheal tubes (44.95%). Biofilm formation occurred in 66.78% of the isolates, correlating with MDR status. International Clone II emerged as the predominant lineage in Indian hospitals in 2023, associated with high antibiotic resistance. A literature review assessed the prevalence, resistance trends, and risk factors of A. baumannii infection. In India, A. baumannii caused 22.3% of hospital-acquired pneumonia cases, with carbapenem-resistance exceeding 70%. New Delhi Metallo-β-lactamase (NDM)-producing strains have increased the challenge, with MDR strains rising to 74.7%. In China, A. baumannii accounts for 35.7%-52.7% of hospital-acquired pneumonia cases, with carbapenem-resistance above 70% and MDR strains reaching 63.8%.16
Epidemiology of CRAB
Nosocomial pathogens, such as CRAB, cause infections in hospitalized patients and are often discovered in ICUs. From various studies, we found that the incidence of CRAB in hospitalized patients has increased manyfold in Asia and Europe. For example, the carbapenem-resistance rate in A. baumannii surpassed 50% in many European nations, according to a surveillance report from the European Centre for Disease Prevention and Control (ECDC, 2022). In nations such as China and India, the prevalence of CRAB is above 60%.15
Infections of the urinary tract and bloodstream, as well as ventilator-associated pneumonia, are the most common CRAB infections. Patients with compromised immune systems are more likely to develop infections than healthy individuals. Patients often end up paying more for their healthcare because of the increased length of stay in the hospital.17 From 2021 to 2023, the prevalence of CRAB in India is 68%, followed by China with 63%, Italy with 54%, Brazil with 48%, and the USA with 34%.
Geographic distribution of resistance
The global distribution of CRAB depends on antimicrobial usage, infection control measures, and healthcare infrastructure. In Europe, the states and countries situated in the Eastern and Southern regions have a higher percentage of MDR cases than the Western and Northern regions. For example, the percentage of patients infected with CRAB is higher in Greece and Italy,18 while countries such as Sweden and Norway have lower percentages of MDR CRAB infections.
In the USA, the CRAB presence can be seen in hospitals and nursing homes (CDC, 2021). The Southeast Asian and Middle Eastern countries have more cases of MDR due to misuse and overuse of antibiotics and the presence of less effective laws.19 The WHO has classified CRAB as a “priority 1: critical pathogen” under its global priority.20
Information on the worldwide spread of CRAB is provided by the Global Antimicrobial Resistance and Use Surveillance System (GLASS), an international organization. In addition, this group has called on people worldwide to unite in the battle against CRAB.
Impact on healthcare systems and patient outcomes
The impact of CRAB on patients is increased hospital bills the length of stay in the hospital increases. Moreover, lives of patients infected with CRAB are at stake. Majority of mortality is due to the presence of CRAB in the bloodstream, accounting for almost 40% of mortality.21 More powerful antibiotics, such as colistin, are used for the treatment of the CRAB; however, they have various side effects associated with them.
The financial strain on patients and their families is significant, as hospital expenses increase with extended hospitalization. Mortality rates for CRAB are also elevated due to the absence of effective and safe antibiotics currently available to prevent or treat MDR. Hospitals facing CRAB outbreaks are required to implement costly infection-control measures, such as intensified disinfection, patient cohorting, and staff education, which further strain healthcare resources.22
Clinical implications of carbapenem-resistant Acinetobacter
Resistance in hospital and community settings
Previous studies have concluded that CRAB is a pathogen that is especially found in hospitals; however, recent research suggests that CRAB is also found in community settings. Hospital ICUs are best suited for their presence because of the various invasive devices and antibiotics. The rate of spread is higher in hospitals because of the presence of contaminated and used medical equipment with which healthcare workers are constantly in touch.23 In some of the cases, it was found that the CRAB cases are being found in individuals who do not have any hospital exposure, which suggests the presence of contamination in water and soil.24 These emerging cases outside the hospital setting pose significant challenges to containment and early diagnosis.
Associated infections (e.g., Pneumonia, bloodstream infections)
Infections of the wound, blood, urinary tract, and VAP are all possible complications of catheter-associated bloodstream infections (CRAB). The death and morbidity rates are higher in patients with VAP. Because of its ability to establish biofilms on endotracheal tubes, A. baumannii is difficult to eradicate.25 Some investigations have shown that CRAB infections in the bloodstream had a death rate of about 60%.26 Because of immune clearance mechanisms, CRAB develop a high degree of resistance to a wide variety of antibiotics, making it very difficult to treat infections caused by these bacteria.27
Table (4): Major infections caused by CRAB and clinical outcomes
Infection Type |
Common Sites |
Mortality (%) |
|---|---|---|
Ventilator-Associated Pneumonia (VAP) |
Lungs |
30-50 |
Bloodstream Infections (BSI) |
Blood |
40-60 |
Urinary Tract Infections (UTI) |
Urinary tract |
10-15 |
Wound Infections |
Skin, surgical sites |
15-25 |
Table 4 highlights major infections caused by CRAB, including VAP, BSI, UTI, and wound infections, along with their common sites. The associated mortality rates vary significantly, with bloodstream infections showing the highest fatality.28
Treatment challenges and therapeutic options
A. baumannii resistance to piperacillin/tazobactam has increased to 56.8%, consistent with studies from the Asia-Pacific and the Middle East reporting 50%-60% resistance rates. Ciprofloxacin resistance surged to 68%, reflecting a global trend of 65%-70%. Colistin, as a last-line defense against MDR organisms, showed a low resistance rate of 0.8%, although increased use may lead to higher resistance. Aminoglycoside resistance also increased. These patterns significantly affect clinical practice, necessitating greater reliance on current local resistance data and emphasizing the importance of antibiotic stewardship.29
Because very few antibiotics are available for the treatment of CRAB, there is an urgent need to conduct more research on CRAB and MDR. For the time being, we use colistin, tigecycline, and cefiderocol, all of which have various adverse effects associated with them. Colistin is a last-resort antibiotic; however, its nephrotoxicity limits its long-term use. Newer agents, such as cefiderocol, have shown promise; however, clinical data on their long-term efficacy remain limited.28
As a last resort, doctors may prescribe a combination medication that includes colistin and either meropenem or rifampin, in a specific ratio, to treat CRAB.30 In various cases, it was also found that all the methods used for the treatment of CRAB proved ineffective due to the strong resistance shown by CRAB.31 Some of the modes of treatment that are still in the experimental stage are bacteriophage therapy, antimicrobial peptides, and immunotherapies.32 Enhanced techniques for the elimination of illnesses caused by the Acinetobacter bacteria and other preventative measures will have to be used until a viable CRAB therapy is found.
Diagnostic approaches for carbapenem-resistant Acinetobacter
Conventional and molecular methods
Two methods are used: the conventional diagnostic approach and the molecular diagnostic approach. Under the traditional methods, we used MacConkey agar and biochemical tests (oxidase reactions and carbohydrate assimilation) for bacterial identification. The only real issue with automated systems, such as BD Phoenix and VITEK 2, is they may sometimes provide false positives when the species are very close, despite their high speed and accuracy for quick identification. Manual disc diffusion and broth microdilution are the techniques of choice for determining the minimum inhibitory concentrations against Acinetobacter spp.33 Resistance genes such as blaOXA-23, blaOXA-24, blaNDM, and blaVIM may be detected using molecular methods such as PCR, real-time PCR, and multiplex PCR. Compared to other approaches, such as phenotypic tests, which are used to identify carbapenemase genes, the aforementioned methods tend to be more sensitive and precise. Loop-mediated isothermal amplification (LAMP) and DNA microarrays, which are advanced molecular methods, are becoming popular owing to their simple and rapid results.34
According to a few studies, molecular analysis revealed a high prevalence of blaOXA-23 in 94.4% CRAB isolates, indicating its dominant role in carbapenem-resistance. blaNDM-1 was identified in 53% of the isolates, and all blaNDM 1-positive isolates also contained blaOXA-23, indicating the co-existence of multiple carbapenemase genes. These findings align with the evidence that OXA-type carbapenemases and MBLs are the principal mechanisms of carbapenem-resistance in A. baumannii, particularly in South/Southeast Asia. Similar co-occurrence has been reported in India, Nepal, and Algeria. Although MBLs are less common in developed countries, their prevalence in developing regions, often in combination with other carbapenemase genes, is well-documented. Since its identification in India, blaNDM-1 has spread globally, accounting for most cases in Asia.
Sequencing analysis confirmed accurate gene amplification with high sequence identity, validating the assay reliability. Minor mismatches and deletions in the non-coding regions indicated allelic variation among the isolates. High sequence conservation suggests evolutionary pressure to maintain the functional integrity of resistance determinants. Similar conservation patterns have been reported in other regions, highlighting the need for molecular surveillance to monitor variants and support infection control.35
Table (5): Comparison of diagnostic methods for crab
Method |
Principle |
Time Required |
Sensitivity |
Specificity |
Comments |
|---|---|---|---|---|---|
Culture + Biochemical Tests |
Phenotypic identification |
24-48 hours |
Moderate |
High |
Standard but time-consuming |
Automated Systems |
Biochemical profiling |
8-24 hours |
High |
Moderate |
Can misidentify some species |
PCR |
DNA amplification |
2-6 hours |
High |
High |
Detects specific resistance genes |
LAMP |
Isothermal DNA amplification |
High |
High |
Rapid, suitable for resource-limited labs |
|
Microarray |
Gene hybridization |
4-6 hours |
High |
High |
Expensive but highly multiplexed |
Table 5 compares various diagnostic methods for detecting CRAB based on principles, time, sensitivity, and specificity. Rapid molecular techniques, such as PCR and LAMP, offer high accuracy and speed, whereas traditional culture methods remain reliable but slow.34
Challenges in detection
Medical professionals encounter numerous obstacles when identifying CRAB. Phenotypic methods struggle to detect low-level or novel resistance, making this a significant challenge. Advanced techniques often fail to include all pertinent carbapenemase genes in databases, leading to inaccurate results. The use of heterogeneous expression can exacerbate mixed infections. Additionally, genotypic methods require specialized equipment and expertise, which limit their use in resource-poor areas. Another significant issue for contemporary medical teams is the absence of standardized molecular protocols that are crucial for the accurate diagnosis of infections. The ongoing mutation and emergence of new variants, such as blaOXA-235 and blaOXA-72, further complicate diagnostic processes.35 The medical community seeks diagnostic tools that are cost-effective, rapid, and capable of distinguishing between colonization and infection.
Advances in diagnostic technologies
Whole-genome sequencing (WGS) is essential to phylogenetic connections, resistance genes, and virulence factors. Because of high cost and lengthy processing time, WGS is only used for CARB monitoring and investigation.37 Because of the development of MALDI-TOF MS, the detection of bacterial infections has become much easier. It takes only a minute for it to recognize many different species. Modern applications include the identification of protein biomarkers associated with resistance.38 Rapid and accurate identification of resistance genes is being achieved using CRISPR-based diagnostics such as SHERLOCK and DETECTOR. Therefore, thermal cyclers are not necessary. As a portable and easily managed method, nanopore sequencing allows us to monitor CRAB in real time in hospitals.39
Table (6): Emerging diagnostic technologies for CRAB
Technology |
Key Features |
Advantages |
Limitations |
|---|---|---|---|
WGS |
Full genome sequencing |
Comprehensive, high-resolution |
Expensive, slow |
MALDI-TOF MS |
Protein-based identification |
Rapid, high throughput |
Cannot detect all resistance genes |
CRISPR-based assays |
Gene detection using Cas enzymes |
Highly specific, portable |
Experimental, not widely available |
Nanopore sequencing |
Real-time, portable DNA sequencing |
Fast, field-deployable |
High error rate, needs optimization |
Table 6 and Figure 4 outline40 emerging diagnostic technologies for CRAB, highlighting innovations such as WGS, MALDI-TOF MS, CRISPR-based assays, and nanopore sequencing. These methods offer advanced detection capabilities with varying advantages and limitations in terms of speed, accuracy, and accessibility.40
Control and prevention strategies
Infection control measures in healthcare settings
Medical professionals employ infection prevention and control (IPC) technologies to prevent CRAB infections in hospitals. In this strategy, hospital personnel maintain strict hygiene by cleaning their hands properly and at regular intervals, cleaning instruments and objects present in the hospital environment, using personal protective equipment, and separating the patient from the rest of the patients and hospital staff. MDR Acinetobacter spp. has the capability to stay and live on the dry surface for a long duration of time without being damaged; hence, to stop it from spreading, the hospitals should be cleaned properly with the use of sodium hypochlorite or hydrogen peroxide.40 Additionally, surveillance cultures and cohorting of patients help contain outbreaks effectively.41
The spread of nosocomial CRAB infections can be significantly decreased with the help of a strict precaution system and active screening. Hospital staff should be trained and educated to maintain strict hygiene within the ICU and hospital surroundings.42 Regular monitoring and audits of IPC adherence should further strengthen these efforts.
Antimicrobial stewardship programs
For the removal and stoppage of the infections, antimicrobial stewardship programs (ASPs) are also used. In these programs, medical professionals initially impose certain restrictions, then conduct audits and await feedback, and finally, propose prescribing based on the guidelines. During ASP, it is advised not to use carbapenems and cephalosporins, which can increase the rates of mutations and MDR in CRAB.43
Medical professionals use de-escalation of empirical therapy, which involves combining pharmacokinetic and pharmacodynamic (PK/PD) approaches to treat infections to increase therapeutic effectiveness. For crucial implementation, various teams of ASP have been formulated, which are a combination of infectious disease physicians, pharmacists, and microbiologists.44
Development of new antimicrobials and alternative therapies
Cefiderocol, a siderophore cephalosporin, is an essential component in the treatment of infections that are resistant to carbapenems.45 The medical experts are conducting clinical trials of some of the combinations, such as sulbactam-durlocactam and meropenem-vaborbactam, to overcome resistance caused by class D carbapenemas.46
Medical experts are investigating a range of alternative therapies, including bacteriophage therapy, antimicrobial peptides, and CRISPR. Bacteriophage therapies have shown significant effectiveness against A. baumannii.47 Additionally, immunomodulatory therapies that focus on host-pathogen interactions are being studied.
Role of vaccines in prevention
It is a fact that we do not have any vaccines against these CRAB; however, medical researchers are trying their best to discover a vaccine against these infections. Outer membrane proteins (OMPs), such as OmpA and OmpW, have provided very good results against these CRAB.48 To generate long-term immunity in patients and medical staff, scientists are also developing live-attenuated and conjugate vaccines.
The most important challenges faced by these vaccines are:
1) Antigenic variability and
2) Lack of strong immunity. With a successful vaccine, the rate of infection can be easily decreased.49
Future directions in combatting carbapenem-resistant Acinetobacter
Research on new resistance mechanisms
To protect the world from the threats of A. baumannii we must develop a mechanism that can better understand the resistance mechanism of CRAB. Various studies have shown the determination of new variants, blaOXA-235 and balOXA-72, which are better equipped with efflux pump overexpression and porin modifications.50 The medical experts and researchers can decode the unrecognized resistance determinants and mobile genetic elements with the help of WGS, which makes the method easy for horizontal gene transfer. These findings highlight the need for continuous molecular monitoring in diagnosis and therapy.
Novel therapeutic approaches and drug development
Cefiderocol and sulbactam-durlobactam are two antibiotics that have shown promising outcomes in preventing CRAB infections and are currently in the penultimate stage of clinical testing. Cefiderocol and sulbactam-durlobactam are part of the Therapeutic Innovation Approaches.51 The popularity of phage therapy is also reaching a new height because of its precision and ability to easily penetrate the defense resistance mechanism of CRAB. Moreover, antimicrobial peptides and immunotherapeutics, including monoclonal antibodies targeting virulence factors such as OmpA, are being studied as adjunctive or stand-alone therapies.52 These approaches, combined with PK/PD-based dosing strategies, offer promising avenues for treatment.
Global collaboration for surveillance and control
Global cooperation is essential for the effective control of CRAB. The entire world must come together and combat the infections caused by CRAB. The WHO introduced GLASS to enhance global data sharing. Medical researchers have initiated collaborative research networks and public private partnerships to develop robust mechanisms for detecting and curbing the spread of CRAB.53 Additionally, ensuring access to quality diagnostics and improved treatments is crucial for eradicating CRAB worldwide.
For medical science, one of the biggest challenges is CRAB. CRAB was once determined to be a low-virulence environmental contaminant; however, it has now become the most problematic and dangerous pathogen on Earth. It develops antibiotic resistance and is responsible for the illnesses and deaths worldwide. It is found in hospital environments, particularly in the ICU, and possesses resistance mechanisms against nearly all antibiotics. It also has a high mortality rate compared to other infections found in the environment. The most common CRAB infections include ventilator-associated pneumonia and blood and wound infections. Since the WHO has classified it as a “critical priority” infection, swift global action to eliminate it is of the utmost importance. One of the deadliest bacteria in the world, A. baumannii, can persist in the dry air of hospitals in combination with strong disinfectants. These bacteria may adapt to their environment using very few nutrients and may even develop resistance to antibiotics. These infections possess multidrug-resistant characteristics due to carbapenem-hydrolyzing β-lactamases, particularly OXA-type enzymes, porin mutations, and overexpression of efflux plasmids. Porin mutations provide a protective barrier that prevents antibiotics from penetrating the bacterial cell wall, whereas the overexpression of efflux plasmids removes these drugs from the bacterial cells. This bacterium has successfully developed resistance to several antibiotics through insertion sequences and the horizontal transfer of resistance genes.
CRAB has become a global issue in Asia, Southern Europe, the Middle East, and parts of Latin America, especially in countries with poor medical facilities and fewer infection control protocols. Due to poor healthcare facilities, patients’ stay in the hospital is prolonged, thus increasing medical bills. Moreover, the mortality rate of CRAB infections is very high. Therapeutically available antibiotics are generally not used against CRAB, as they develop resistance against old and weak antibiotics. The combination of cefiderocol and sulbactam-durlobactam is still in the clinical trial phase. Phage therapy and monoclonal antibodies represent exciting avenues but require further validation and regulatory approval before they can be implemented on a large scale. The detection and diagnosis of CRAB is very difficult in countries with fewer facilities. The molecular techniques have shown very good precision and accuracy in the determination of these bacteria; however, the high cost of these techniques has created a major problem in their adoption. With constant mutations, CRAB enables them to enhance their resistance capability; thus, it has become very important for world to update their diagnostic platforms to detect these pathogens. Early and accurate detection remains critical for guiding targeted therapy and implementing infection control measures swiftly.
Medical experts have employed multifaceted strategies to control these pathogens. The protocols suggested by the medical expert are as follows: 1) washing and cleaning of hands at regular intervals with soaps and sanitizers, 2) preventing physical and direct contact with pathogens, 3) constantly decontamination using strong disinfectants, and 4) keeping infected patients apart from the rest of the hospital’s patients and employees. Programs aimed at antimicrobial stewardship that encourage responsible antibiotic use and lessen the push for resistance are equally crucial. Global corporations must identify and eradicate CRAB. The world must fund the research and development (R&D) activities to develop a strong and updated database that can easily identify CRAB pathogens. Although still in the experimental stage, the development of vaccines holds promise for the prevention of infections in high-risk populations. From the above studies, it is clear that CRAB is intelligent and smart, as it has developed its own mechanism against antibiotics, which is becoming a difficult task for modern medical science to conquer. To control these pathogens, there should be constant R&D of antibiotics, and global corporations should increase. With a combination of microbiological insights, diagnostic advancements, clinical preparedness, and public health strategies, we can try to solve the issues of MDR in CRAB.
Recommendations for future research
Actively engaging in innovative research across various disciplines is essential to address the increasing threat of CRAB. Initially, gaining a deeper understanding of the mechanisms underlying the increase in resistance is crucial. Although β-lactamase production, efflux pumps, and porin loss have been thoroughly examined, further exploration of new resistance pathways, including those involving regulatory genes and epigenetic factors, is necessary to maintain bacterial adaptability. The development of new antimicrobial agents targeting CRAB is also a pressing concern. In addition to developing new antibiotics, exploring drug repurposing strategies and effective combination therapies is vital. Promising yet underexplored options that could bypass traditional resistance mechanisms include antimicrobial peptides, phage therapy, and nanoparticles.
Enhancing diagnostic tools is critical. Given the high prevalence of CRAB and limited laboratory capabilities in low- and middle-income countries, research should prioritize the development of rapid, sensitive, and cost-effective molecular diagnostics. WGS combined with AI-based prediction systems can revolutionize early detection and outbreak surveillance.
Globally, more data on the epidemiology of CRAB are needed, especially in less-studied regions. Supporting international surveillance networks is essential to understanding the spread of resistant strains. Finally, increased collaboration and funding should be directed towards the early stages of A. baumannii vaccine development, particularly for high-risk populations such as immunocompromised individuals and patients in the ICU.
In conclusion, future research should be multifaceted, collaborative, and centered on innovative approaches to tackle the clinical and public health challenges posed by CRAB.
ACKNOWLEDGMENTS
The authors thank the Department of Microbiology, Mamata Academy of Medical Sciences, for providing resources and facilities that enabled this study.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
ETHICS STATEMENT
Not applicable.
- Kazemian H, Karami-Zarandi M, Heidari H, Ghanavati R, Khoshnood S. Antimicrobial combination effects against multidrug-resistant Acinetobacter baumannii and Pseudomonas aeruginosa strains: A cross-sectional study. Health Sci Rep. 2024;7(5):e2061.
Crossref - Poirel L, Nordmann P. Carbapenem resistance in Acinetobacter baumannii: mechanisms and epidemiology. Clin Microbiol Infect. 2006;12(9):826-836.
Crossref - Thacharodi A, Vithlani A, Hassan S, Alqahtani A, Pugazhendhi A. Carbapenem-resistant Acinetobacter baumannii raises global alarm for new antibiotic regimens. iScience. 2024;27:111367
Crossref - Murray CJL, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629-655.
Crossref - Dolma KG, MD WM. Acinetobacter baumannii: An overview of emerging multidrug-resistant pathogen. Med J Malaysia. 2022;77(3):357.
- Giamarellou H, Karaiskos I. Current and potential therapeutic options for infections caused by difficult-to-treat and pandrug-resistant gram-negative bacteria in critically ill patients. Antibiotics. 2022;11(8):1009.
Crossref - Rahi AA, Al-Hasnaway HH. Multidrug resistance patterns, gene overexpression, and genetic diversity of Acinetobacter baumannii isolates from clinical specimens. 2025.
Crossref - Doi Y, Murray GL, Peleg AY. Acinetobacter baumannii: evolution of antimicrobial resistance—treatment options. Semin Respir Crit Care Med. 2015;36(1):85-98.
Crossref - Rokes AB, Santos-Lopez A, Cooper VS. History shapes regulatory and evolutionary responses to tigecycline in strains of Acinetobacter baumannii from the pre-and post-antibiotic eras. bioRxiv. 2025;2025-01.
Crossref - Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev. 2008;21(3):538-582.
Crossref - Orozco-Ochoa AK, González-Gómez JP, Quiñones B, Campo NCD, Valdez-Torres JB, Chaidez-Quiroz C. Bacteriophage Indie resensitizes multidrug-resistant Acinetobacter baumannii to antibiotics in vitro. Sci Rep. 2025;15(1):11578.
Crossref - Quyen TLT, Hsieh YC, Li SW, Wu LT, Liu YZ, Pan YJ. Molecular epidemiology of carbapenem-resistant Acinetobacter baumannii group in Taiwan. mSphere. 2025;10(1):e00793-24.
Crossref - Kuruva K, Koppala R, Naaz S, et al. Tracking Acinetobacter baumannii in Critical Care Units: Environmental Surveillance and One Health Strategies for AMR Prevention. Jordan Medical Journal. 2025;59(5).
Crossref - Tajer L, Paillart JC, Dib H, Sabatier JM, Fajloun Z, Khattar ZA. Molecular mechanisms of bacterial resistance to antimicrobial peptides in the modern era: an updated review. Microorganisms. 2024;12(7):1259.
Crossref - Jangid H, Kumar D, Kumar G, Kumar R, Mamidi N. Bibliometric examination of global scientific research about Carbapenem-resistant Acinetobacter Baumannii (CRAB). Antibiotics. 2023;12(11):1593.
Crossref - Pathoor NN, Ganesh PS, Gopal RK. Understanding the prevalence, antimicrobial resistance, and public health challenges of Acinetobacter baumannii in India and China. J Appl Microbiol. 2025;136(5).
Crossref - Dijkshoorn L, Nemec A, Seifert H. An increasing threat in hospitals: multidrug-resistant Acinetobacter baumannii. Nat Rev Microbiol. 2007;5(12):939-951.
Crossref - European Centre for Disease Prevention and Control (ECDC). Antimicrobial Resistance in the EU/EEA: Annual Epidemiological Report for 2022. 2022. https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2022. Accessed May 12, 2025.
- Mathu R, Diago-Navarro E, Lynch E, et al. Antibiotic resistance in the Middle East and Southern Asia: a systematic review and meta-analysis. JAC-Antimicrob Resist. 2024;7(1):dlaf010.
Crossref - World Health Organization (WHO). WHO bacterial priority pathogens list, 2024: Bacterial pathogens of public health importance to guide research, development and strategies to prevent and control antimicrobial resistance. https://www.who.int/publications/i/item/9789240093461″>Crossref
- Howard DH, Bach PB, Berndt ER, Conti RM. Pricing in the market for anticancer drugs. J Econ Perspect. 2012;26(1):27-50.
Crossref - Munoz-Price LS, Hayden MK, Lolans K, et al. Successful control of an outbreak of Klebsiella pneumoniae carbapenemase–producing Klebsiella pneumoniae at a long-term acute care hospital. Infect Control Hosp Epidemiol. 2015;29(1):139-162.
Crossref - Zhang X, Tian L, Wu J, et al. Risk factors for Carbapenem-resistant Acinetobacter baumannii contamination on hospital surfaces: a multi-year environmental monitoring study in Shanghai, China. Front Microbiol. 2025;16:1609148.
Crossref - Dadić B, et al. Carbapenem-resistant bacteria in the environment Arh Hig Rada Toksikol 2025;76:87−101
Crossref - Chukamnerd A, Saipetch N, Singkhamanan K, et al Association of biofilm formation, antimicrobial resistance, clinical characteristics, and clinical outcomes among Acinetobacter baumannii isolates from patients with ventilator-associated pneumonia. Clin Respir J. 2024;18:e13732.
Crossref - Lee BY, Bartsch SM, Wong KF, et al. The potential trajectory of carbapenem-resistant Enterobacteriaceae, an emerging threat to healthcare facilities, and the impact of the Centers for Disease Control and Prevention toolkit. Am J Epidemiol. 2016;183(5):471–479.
Crossref - Zarrilli R, Pournaras S, Giannouli M, Tsakris A. Global evolution of multidrug-resistant Acinetobacter baumannii clonal lineages. Int J Antimicrob Agents. 2013;41(1):11-19.
Crossref - Boutzoukas A, Doi Y. The global epidemiology of carbapenem-resistant Acinetobacter baumannii. JAC Antimicrob Resist. 2025;7(4)
Crossref - Ravella Venkatasubramanyam N, Easwaran S, Prabhakaran N. Retrospective Analysis of Antimicrobial Resistance Trends in Pseudomonas aeruginosa and Acinetobacter baumannii. Cureus. 2024;16(9):e69166.
Crossref - Katip W, Uitrakul S, Oberdorfer P. A Comparison of Colistin versus Colistin Plus Meropenem for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients: A Propensity Score-Matched Analysis. Antibiotics. 2020;9(10):647.
Crossref - Thacharodi A, Vithlani A, Hassan S, Alqahtani A, Pugazhendhi A. Carbapenem-resistant Acinetobacter baumannii raises global alarm for new antibiotic regimens. iScience. 2024;27(12):111367
Crossref - Hao Linga,Xinyu Loua, et al.Recent advances in bacteriophage-based therapeutics: Insight into the post-antibiotic era. Acta Pharmaceutica Sinica B 2022;12(12): 4348-4364
Crossref - Clinical and Laboratory Standards Institute (CLSI). M100: Performance Standards for Antimicrobial Susceptibility Testing. 33rd ed. Clinical and Laboratory Standards Institute; 2023.
- Hendriksen RS, Munk P, Njage P, et al. Global monitoring of antimicrobial resistance based on metagenomics analyses of urban sewage. Nat Commun. 2019;10(1):1124.
Crossref - Kannan KP, Girija ASS, Priyadaharsini JV. Co-occurrence of blaOXA-23 and blaNDM-1 Genes in Carbapenem-resistant Acinetobacter baumannii Isolated from Bloodstream Infections: A Cross-sectional Study. J Clin Diagn Res. 2026;20(4): DC22-DC27.
Crossref - Evans BA, Amyes SG. OXA b-lactamases. Clin Microbiol Rev. 2014;27(2):241-263.
Crossref - Quainoo S, Coolen JPM, Van Hijum S a. FT, et al. Whole-Genome Sequencing of Bacterial Pathogens: the Future of Nosocomial Outbreak Analysis. Clin Microbiol Rev. 2017;30(4):1015-1063.
Crossref - Elbehiry A, Abalkhail A. Spectral precision: recent advances in Matrix-Assisted laser Desorption/Ionization Time-of-Flight mass spectrometry for pathogen detection and resistance profiling. Microorganisms. 2025;13(7):1473.
Crossref - Wang Z, Wang Q, Zhang J, et al. CRISPR-driven diagnostics: Molecular mechanisms, clinical efficacy and translational challenges. Clin Transl Med. 2025;15(10):e70482.
Crossref - Morena R, Gullì SP, Serapide F, Russo A. Precision approaches to Carbapenem-Resistant infections in the ICU: integrating diagnostics, stewardship, and novel therapies. Diagnostics. 2026;16(7):1053.
Crossref - Siegel JD, Rhinehart E, Jackson M, et al. 2007 guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. Am J Infect Control. 2007;7;35(10):S65-S164.
Crossref - Vicentini C, Bussolino R, Kuczewski E, et al. Carbapenem-resistant Acinetobacter baumannii infections in intensive care units: incidence, infection prevention and control, and antimicrobial stewardship practices in the cross-border region between Italy and France, 2019–2022. Journal of Hospital Infection. 2026;170:174-183.
Crossref - Magesa B, Mwelange L, Sirili N, Mhame M. Barriers and facilitators for the implementation of Antimicrobial Stewardship Programs in Dar es Salaam Regional Referral Hospitals (RRHs). PLOS Global Public Health. 2026;6(3):e0006123.
Crossref - Bissantz C, Zampaloni C, David-Pierson P, et al. Translational PK/PD for the Development of Novel Antibiotics—A Drug Developer’s perspective. Antibiotics. 2024;13(1):72.
Crossref - Zhanel GG, Golden AR, Zelenitsky S, et al. Cefiderocol: A Siderophore Cephalosporin with Activity Against Carbapenem-Resistant and Multidrug-Resistant Gram-Negative Bacilli. Drugs. 2019;79(3):271-289.
Crossref - McLeod SM, Moussa SH, Hackel MA, Miller AA. In vitro activity of sulbactam-durlobactam against Acinetobacter baumannii-calcoaceticus complex isolates collected globally in 2016 and 2017. Antimicrob Agents Chemother. 2020;64(4):e02534-19.
Crossref - Schooley RT, Biswas B, Gill JJ, et al. Development and use of personalized bacteriophage-based therapeutic cocktails to treat a patient with a disseminated resistant Acinetobacter baumannii infection. Antimicrob Agents Chemother. 2017;61(10):e00954-17.
Crossref - Wu HJ, Xiao ZG, et al. Drug-resistant Acinetobacter baumannii: from molecular mechanisms to potential therapeutics (review). Exp Ther Med. 2023;25(5):209.
Crossref - Elbehiry A, Marzouk E, Moussa I, et al. The Prevalence of Multidrug-Resistant Acinetobacter baumannii and Its Vaccination Status among Healthcare Providers. Vaccines. 2023;11(7):1171.
Crossref - Roca I, Espinal P, Vila-Farres X, Vila J. The Acinetobacter baumannii oxymoron: commensal hospital dweller turned pan-drug-resistant menace. Front Microbiol. 2012;3:148.
Crossref - Nguyen M, Joshi SG. Carbapenem resistance in Acinetobacter baumannii, and their importance in hospital-acquired infections: a scientific review. J Appl Microbiol. 2021;131(6):2715-2738.
Crossref - Russo TA, Luke NR, Beanan JM, et al. The K1 capsular polysaccharide of Acinetobacter baumannii strain 307-0294 is a major virulence factor. Infect Immun. 2010;78(9):3993-4000.
Crossref - Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318-327.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.