


ISSN: 0973-7510
E-ISSN: 2581-690X
Antibiotic-resistant bacteria (ARB) in hospital wastewater pose serious environmental and public health risks due to their potential to persist through treatment processes and disseminate resistance genes. This study investigated the occurrence and persistence of ARB and antibiotic resistance genes (ARGs) in the wastewater treatment system of a teaching hospital in Malaysia. Samples were collected from five treatment stages across two sampling periods and analyzed using culture-based isolation, 16S rRNA gene sequencing, and antimicrobial susceptibility testing according to CLSI and EUCAST guidelines. A total of 28 isolates consisting of 11 different bacterial species were identified, including representative species such as Klebsiella pneumoniae, Acinetobacter baumannii, Aeromonas hydrophila, and members of the Stenotrophomonas maltophilia complex. K. pneumoniae exhibited multidrug-resistance and mutations in the gyrA gene (S83R, D87N), associated with fluoroquinolone resistance. Detected ARGs included blaSHV, blaCTX-M, blaTEM, blaNDM, and gyrA. The persistence of resistant bacteria and ARGs in the final effluent indicates incomplete elimination by tertiary treatment. These findings highlight hospital wastewater as a critical reservoir for antimicrobial resistance and underscore, from a One Health perspective, the need for integrated monitoring and improved wastewater treatment strategies to limit environmental dissemination of resistance determinants.
Hospital Wastewater, Drug-resistance, Antibiotic-resistant Bacteria, Antibiotic Resistance Genes
Wastewater treatment facilities, particularly those managing hospital effluents, are considered hotspots for the spread of ARB, posing a risk to the public’s health when water is reused.1 This has serious effects for the long-term viability of antibiotic use in humans.2 Hospital wastewater contains significant levels of antibiotic residues, which impose selective pressure on the development of resistance. As a result, hospital wastewater plays a crucial role in the establishment and dissemination of ARB.3 Hospital wastewater may introduce and select resistant bacteria in the environment while suppressing susceptible microorganisms’ growth.4 The extensive use of antibiotics in human and animal medicine has led to the presence of antibiotic residues in wastewater and the emergence of ARB, posing environmental and public health concerns. Due to their receipt of antibiotic-contaminated waste from hospitals, municipal sewage, and livestock, wastewater treatment plants (WWTPs) are hotspots for the propagation of antibiotic-resistant genes (ARGs). While disinfection techniques like chlorination can lower the bacterial load, they may allow ARB to survive and reactivate.5 The prevalence of extensively drug-resistant bacteria has increased, especially in aquatic epidemics, and these strains are more challenging to control and treat with efficient antimicrobial treatments.6 Therefore, water sources may serve as a vital reservoir for infectious bacterial diseases and may raise the risk of illness for people who consume seafood or engage in recreational activities that expose them to water.7 Hospital wastewater has a crucial function as a reservoir and conduit for ARBs and ARGs, according to recent studies.8 In Malaysia, a cross-sectional study approach has been proposed to investigate antibiotic-resistant pathogenic bacteria and antibiotic residues in hospital effluents in Selangor, to establish baseline data on resistance prevalence and contaminant levels in effluent streams.9
Regional research, particularly studies in Malaysia, contextualises the incidence of resistant bacteria and the formation of AMR in hospital effluents, emphasising the importance of integrated surveillance systems that include phenotypic, molecular, and environmental data.10 Despite growing interest in hospital wastewater as a source of ARB and ARGs, data from Malaysia are scarce, and previous research seldom combined treatment-stage sampling, phenotypic resistance profiling, and molecular ARG identification in a single system.
This study fills these gaps by combining culture-based isolation, antimicrobial susceptibility testing, and targeted molecular detection of clinically relevant ARGs over multiple wastewater treatment stages and two sampling periods, resulting in a comprehensive picture of resistance persistence and dissemination within a hospital wastewater treatment system.
Specifically, this study aims to identify the resistance pattern in bacteria and their prevalence in hospital wastewater, as well as to highlight the potential risk to the environment and public health posed by untreated wastewater containing antibiotic-resistant bacteria.
Sample collection
This study employed a cross-sectional study, repeated-sampling design to investigate the occurrence, persistence, and resistance profiles of bacteria in a hospital wastewater treatment system. Sampling was performed during two separate time periods to capture temporal variation and improve the representativeness of the data.
Sampling was conducted during two distinct time periods. The first sampling campaign was carried out in July 2023, and the second in January 2024, with identical sampling locations and procedures in both periods. Each sampling campaign consisted of one complete sampling event across all five treatment stages of the wastewater treatment system. The same five locations (grit chamber, aeration tank, clarification tank, disinfection chamber, and discharge outlet) were sampled during both the first (July 2023) and second (January 2024) sampling periods.
Thus, each treatment stage was sampled twice in total, once in each sampling period, using identical sampling procedures, containers, and transport protocols. This design enabled temporal comparison between the two sampling periods while maintaining consistent spatial sampling across treatment stages.
The first sampling point was the grit chamber, where large solids and sediments are removed, followed by the aeration tank, where oxygen is introduced to stimulate the growth of microbial activity that degrades biological matter. The third stage is the clarification tank, which allows suspended biological sludge to settle. Subsequent treatment involves a disinfection chamber, which makes the treatment plant a conventional tertiary treatment where chlorination is used to reduce the microbial load. The final sampling was at the discharge outlet, where the treated effluent is released into the retention pond.
This hospital’s wastewater treatment system is an open system that receives both external water inputs and frequent inflows from hospital operations. All samples were taken during dry weather in order to reduce dilution effects and environmental variability. Sampling was not done after rainstorm occurrences. All samples were collected in sterile 500 mL standard laboratory glass bottles under sterile conditions to maintain sample integrity and to avoid contamination or microbial modification. Direct contact with external surfaces was avoided during collection, and containers were promptly sealed after filling. To reduce microbial growth and metabolic activity during transit, samples were brought to the lab in insulated containers at a temperature between 4 and 8 °C. To maintain microbial viability and resistance profiles, all samples were processed within two to four hours of collection, and no preservatives were used.
A schematic representation of the hospital wastewater treatment system, including treatment stages, sampling locations, flow direction, and treatment processes, is shown in Figure 1.
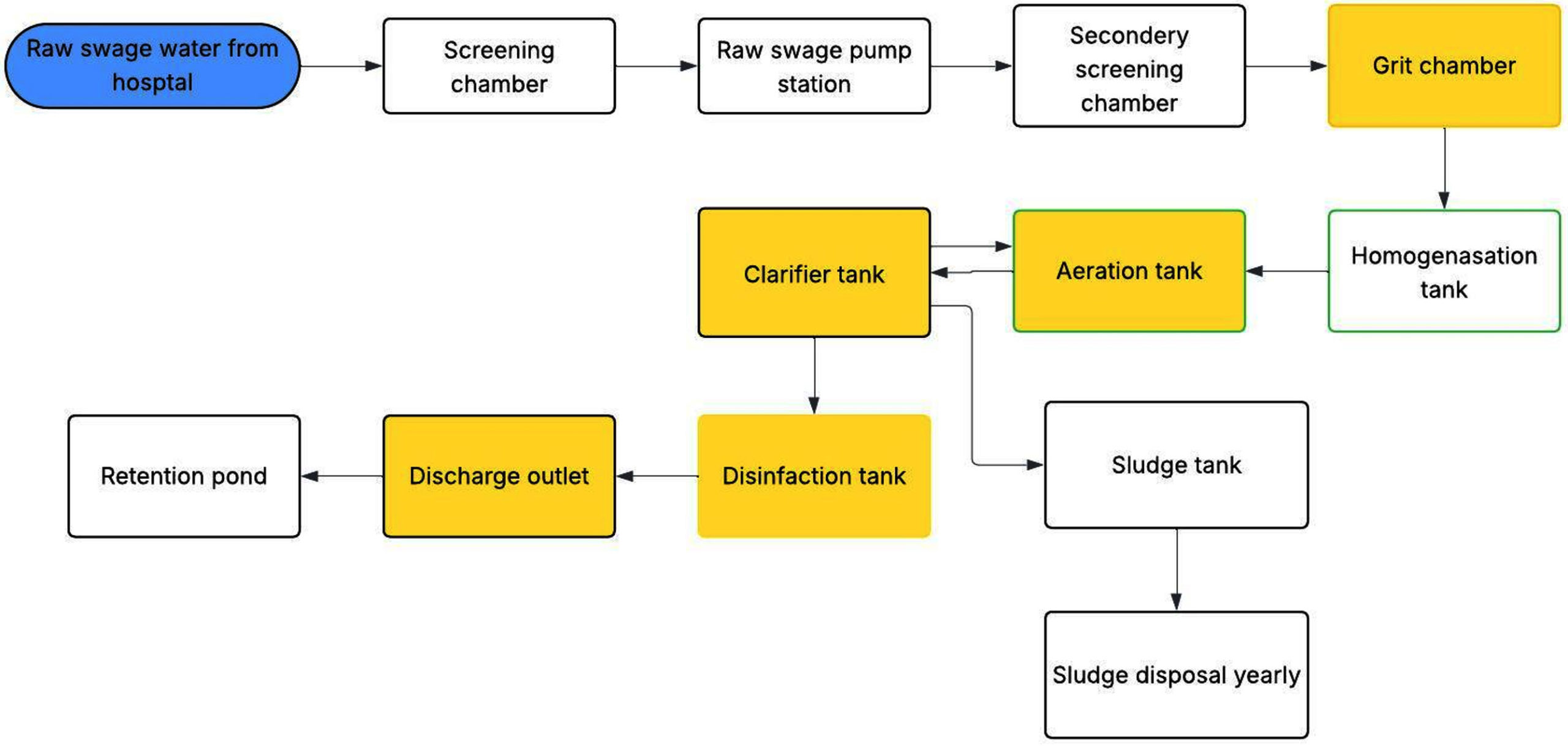
Figure 1. Schematic representation of the hospital’s wastewater treatment system showing flow direction and sampling points (S1-S5). Colours are used to indicate the sampling locations within the treatment system and do not represent treatment intensity or process differences
Bacteria isolation
A 5-fold serial dilution was performed to reduce the bacterial concentration, enabling the isolation of single colonies. One mL of the sample was diluted in 9 mL of sterile distilled water, and 100 µL of the diluted solution was spread onto nutrient agar (OXOID, United Kingdom) plates using the spread plate method for bacterial growth. Nutrient agar was used as a general-purpose, non-selective medium for the initial isolation of culturable bacteria from wastewater samples. While this medium is suitable for the growth and maintenance of a broad range of environmental and opportunistic bacteria and is appropriate for downstream cultivation and processing of isolates.
The plates were incubated at 37 °C for 24 hours under standard aerobic incubation conditions.
After incubation, colonies with different morphologies were selected and streaked onto fresh agar plates using the streak plate method to obtain pure cultures. Once single colonies were obtained, glycerol stocks were prepared by suspending the bacteria in a 20% glycerol solution and storing them at -40 °C to preserve the bacterial isolates for future analysis.
Colony Forming Units (CFU) Analysis
A colony count was conducted to determine the efficiency of the wastewater treatment plant. CFU analysis was performed independently of bacterial isolation procedures to quantify bacterial load and evaluate treatment efficiency across the wastewater treatment stages. Serial dilution was performed by diluting 1 mL of the sample in 9 mL of sterile nutrient broth to achieve an appropriate dilution factor for colony enumeration. Nutrient broth (OXOID, United Kingdom) was used as the diluent to maintain osmotic balance and bacterial viability during dilution, thereby preventing cell stress or lysis and ensuring accurate quantification of viable bacteria.
The final dilution factor was 1:100,000; 100 µL of the diluted sample was spread onto nutrient agar using an L-shaped spreader under sterile conditions. Plates were incubated at 37 °C for 24 hours under aerobic conditions. After incubation, visible colonies were counted manually. Duplicate colony counts were performed to ensure accuracy, and CFU values were calculated using the formula:
CFU/mL = (Number of colonies × Dilution factor) / Volume of plated sample.
Molecular Identification of Hospital Wastewater Isolates
Bacterial species in the samples were identified using molecular techniques, particularly 16S rRNA gene sequencing, a standard method11 for bacterial identification, due to the gene’s conserved yet variable nature.
PCR Amplification and Analysis of the 16S rRNA Gene
Genomic DNA was extracted from the isolated bacteria using the DNeasy Blood & Tissue Kit (QIAGEN, Hilden, Germany). The extracted DNA was subsequently used as a template for 16S rRNA gene amplification. The following primers were used:
- 27F Primer (5′-AGAGTTTGATCCTGGCTCAG-3′): Forward primer (Integrated DNA Technologies, United States of America).
- 1492R Primer (5′-CGGCTACCT TGTTACGACTT-3′): Reverse primer.
The PCR cycling conditions were as follows: initial denaturation at 94 °C for 30 seconds, denaturation at 94 °C for 30 seconds, annealing at 51 °C for 2 minutes, extension at 68 °C for 2 minutes, and final extension at 68 °C for 5 minutes in 30 cycles.
A portion of the PCR product was analysed using agarose gel electrophoresis to confirm successful amplification. A band at the expected size (~1,500 bp) confirmed the presence of the 16S rRNA gene. The PCR product was then purified and sequenced using Sanger sequencing.
The obtained nucleotide sequences were analyzed using the BLASTn tool against the NCBI GenBank database for taxonomic identification. Sequence similarity ≥97% was considered indicative of genus-level identification, while ≥99% was used to assign species-level identification.
Antimicrobial susceptibility testing
The antimicrobial susceptibility of the bacterial isolates was determined using disc diffusion testing following the Clinical and Laboratory Standards Institute guidelines (CLSI), 34th Edition.12 Commercial antibiotic discs containing known concentrations of antibiotics (Amikacin 30 µg, Meropenem 10 µg, Ceftriaxone 30 µg, Ertapenem 10 µg, Ceftazidime 30 µg, Imipenem 10 µg, Cefepime 30 µg, Gentamicin 10 µg, Ciprofloxacin 5 µg, Ampicillin 10 µg, Levofloxacin 5 µg, Minocycline 30 µg, Tetracycline 30 µg) (Liofilchem, Italy) were placed onto the inoculated agar plates. The antimicrobial susceptibility test (AST) was done once per isolate following CLSI/EUCAST standard procedures. The plates were incubated at 37 °C for 24 hours. After incubation, the zone of inhibition (a clear area around each disc where bacteria could not grow) was measured. Using E. coli ATCC 25922, quality control (QC) for antimicrobial susceptibility testing was performed in compliance with the Clinical and Laboratory Standards Institute 34th Edition (2024)(CLSI) criteria to ensure the accuracy and reliability of the AST results.
The results were interpreted in accordance with the Clinical and Laboratory Standards Institute (CLSI) Performance Standards of Antimicrobial Susceptibility, 2024 and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) Version 14.0, 2024 guidelines. Based on the size of the inhibition zone, bacteria were classified as susceptible, intermediate, or resistant to each antibiotic. For bacterial species lacking species-specific CLSI or EUCAST breakpoints, including Stenotrophomonas hibiscicola, antimicrobial susceptibility interpretation was guided by genus-level reference breakpoints and available EUCAST reference criteria for phylogenetically related taxa, including Pseudomonas spp.
Detection of the resistance genes
The targeted genes were selected based on the phenotypic resistance profiles observed in the AST results, with a focus on clinically relevant resistance mechanisms in hospital-associated bacteria, particularly ESBL production, carbapenem resistance, and fluoroquinolone resistance.
Multiplex PCR was used to detect the presence of blaSHV, blaCTX-M, blaTEM, blaNDM, blaKPC, blaOXA-48, and the quinolone-resistance gene gyrA using a Bio-Rad CFX 96 (United States of America) PCR machine. The reaction for multiplex PCR was performed using the following components: 2 µL of DNA template, 12.5 µl of AllTaq Master Mix (QIAGEN, Hilden, Germany) Composition (20 mM Tris-HCl, 1.8 mM MgCl2, 0.05% Tween® 20-, and 0.2- mM dNTPs), 0.5 µl of primers, and deionised sterile water for molecular purposes to achieve a final volume of 25 µl. Each PCR assay included a positive control consisting of genomic DNA extracted from previously characterised bacterial isolates confirmed to carry the target resistance genes. The primers used are detailed in Table 1.
Table (1): Primers are used for the polymerase chain reaction to detect genes responsible for resistance
| Primers | Sequence (5′ to 3′ Direction) | Amplicon Size | Ref. |
|---|---|---|---|
| TEM Forward | 5′-GAGACAATAACCCTGGTAAAT-3′ | 410 bp | 13 |
| TEM Reverse | 5′-AGAAGTAAGTTGGCAGCAGTG-3′ | 410 bp | |
| SHV Forward | 5′-GTCAGCGAAAAACACCTTGCC-3′ | 360 bp | |
| SHV Reverse | 5′-GTCTTATCGGCGATAAACCAG -3′ | 360 bp | |
| CTX-M Forward | 5′-GAAGGTCATCAAGAAGGTGCG-3′ | 550 bp | |
| NDM Forward | 5′-GCAGCACACTTCCTATCTCG-3′ | 190 bp | 14 |
| NDM Reverse | 5′-GTCCATACCGCCCATCTTGT-3′ | 190 bp | |
| KPC Forward | 5′-TGCAGAGCCCAGTGTCAGTTT-3′ | 620 bp | |
| KPC Reverse | 5′-CGCTCTATCGGCGATACCA-3′ | 620 bp | 15 |
| OXA_48 Forward | 5′-GCGTGGTTAAGGATGAACAC-3′ | 550 bp | |
| OXA_48 Reverse | 5′-CATCAAGTTCAACCCAACCG-3′ | 550 bp | |
| gyrA Forward | 5′-TACACCGGTCAACATTGAGG-3′ | 790 bp | 16 |
| gyrA Reverse | 5′-TTAATGATTGCCGCCGTCGG-3′ | 790 bp |
PCR conditions for the resistance genes
PCR was performed using primers (Bio Basic, United States of America) under the following conditions: initial denaturation at 94 °C for 30 seconds, denaturation at 94 °C for 30 seconds, annealing at 57 °C for 90 seconds, extension at 68 °C for 2 minutes, and final extension at 68 °C for 5 minutes over 25 cycles. These conditions were applied for TEM, CTX-M, SHV, NDM, GyrA, and OXA-48. For KPC, the annealing temperature was 55 °C. The size of the PCR products was detected using 1.2% agarose gel electrophoresis. PCR products were purified and sequenced by an external commercial sequencing facility using standard purification and Sanger sequencing protocols.
Bacterial load and distribution across wastewater treatment stages
Samples taken from HSAAS wastewater and plated on nutrient agar were used for colony counts. At each sampling site, the bacterial load varies. The grit chamber (S1) recorded (1.66 ± 0.11) × 108, followed by the Aeration tank (S2) (1.54 ± 0.11) × 108, the clarifier tank (S3) (1.43 ± 0.06) × 108, the disinfection tank (S4) (6.90 ± 0.06) × 107, and the discharge outlet (S5) (5.85 ± 0.05) × 107. Regardless of this decrease, bacterial growth was still detected in the disinfection tank and the v-notch discharge outlet that led to the retention pond, suggesting that microorganisms had not been completely removed. These variants are shown in Figure 2. The CFU/mL values presented in Figure 2 and Table 2 are derived from the same dataset. Figure 2 provides a graphical representation of bacterial load across treatment stages, while Table 2 presents the corresponding numerical values together with bacterial species distribution.
Table (2): Distribution of bacteria in the wastewater system plants
| Sampling Site | Bacteria Isolated | Mean ± SD (CFU/mL) |
|---|---|---|
| Grit chamber | Klebsiella pneumoniae (MDR) | (1.66 ± 0.11) × 108 |
| Stenotrophomonas hibiscicola | ||
| Acinetobacter baumannii | ||
| Aeromonas hydrophila | ||
| Stenotrophomonas maltophilia | ||
| Aeration tank | Stenotrophomonas geniculata | (1.54 ± 0.11) × 108 |
| Klebsiella pneumoniae | ||
| Pseudomonas putida | ||
| Pseudomonas stutzeri | ||
| Stenotrophomonas maltophilia | ||
| Bacillus altitudinis | ||
| Clarifier tank | Stenotrophomonas geniculata | (1.43 ± 0.06) × 108 |
| Klebsiella pneumoniae | ||
| Acinetobacter baumannii | ||
| Pseudomonas stutzeri | ||
| Bacillus cereus | ||
| Pseudomonas putida | ||
| Disinfection chamber | Stenotrophomonas geniculata | (6.90 ± 0.06) × 107 |
| Klebsiella pneumoniae | ||
| Acinetobacter baumannii | ||
| Aeromonas hydrophila | ||
| Bacillus altitudinis | ||
| Discharge outlet | Stenotrophomonas geniculata | (5.85 ± 0.05) × 107 |
| Klebsiella pneumoniae | ||
| Acinetobacter baumannii | ||
| Pseudomonas putida | ||
| Aeromonas hydrophila | ||
| Stenotrophomonas maltophilia |
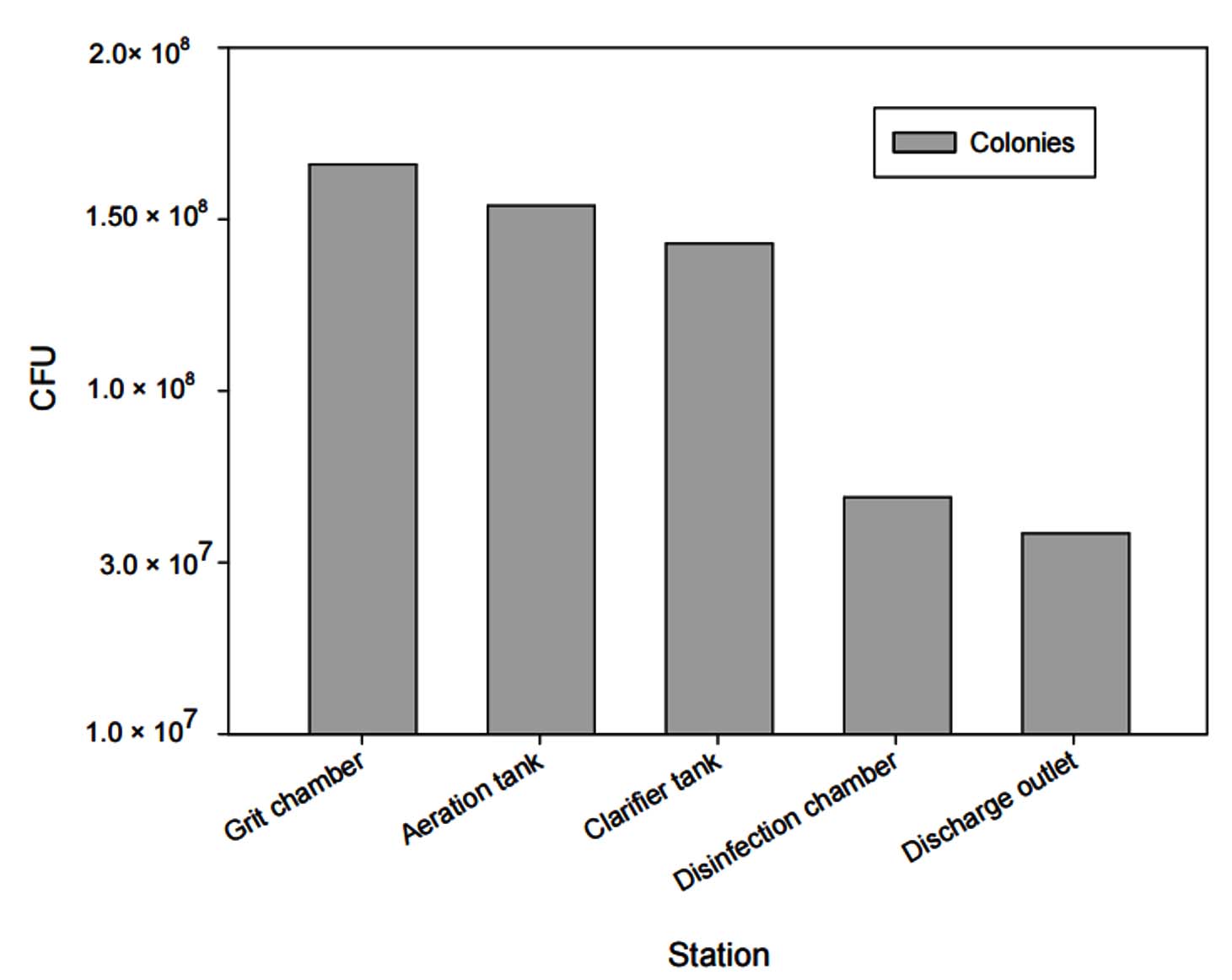
Figure 2. Number of bacteria (CFU/mL) across different stations
A total of 28 bacteria were isolated, representing 11 different species from the hospital wastewater system, and were identified as Stenotrophomonas geniculate, Klebsiella pneumoniae, and Stenotrophomonas hibiscicola (formerly Pseudomonas hibiscicola), while the second sampling revealed Klebsiella pneumoniae, Aeromonas hydrophila, Bacillus cereus, Acinetobacter baumannii, Pseudomonas putida, Pseudomonas stutzeri, Bacillus altitudinis, and Stenotrophomonas maltophilia, as Table 2.
Antimicrobial susceptibility test in bacteria from hospital wastewater
A total of 28 bacterial isolates were recovered from the wastewater treatment system. Of these, 22 isolates were subjected to AST. The remaining isolates were identified as Bacillus spp., which are classified as environmental bacteria and are not considered clinically relevant target organisms for standardized AST interpretation under CLSI and EUCAST guidelines. Therefore, these isolates were excluded from susceptibility testing and resistance profiling analyses.
Antimicrobial susceptibility profiles of the bacterial isolates are summarised in Table 3. Overall, Klebsiella pneumoniae showed the highest resistance levels, including multidrug- resistance in one isolate. Acinetobacter baumannii exhibited resistance to (ceftazidime and cefepime). Aeromonas hydrophila showed intermediate susceptibility to cephalosporins but remained susceptible to most antibiotics. Other isolates, including Stenotrophomonas maltophilia, Pseudomonas putida, and Pseudomonas stutzeri, were largely susceptible to the tested antibiotics. These findings indicate the persistence of antibiotic-resistant bacteria across different treatment stages (Supplementary Tables).
Table (3): Antimicrobial resistance profiles of bacterial isolates from hospital wastewater
| Antibiotics | Klebsiella pneumoniae N = 6 | S. hibiscicola N = 1 | Acinetobacter baumannii N = 4 | Aeromonashydrophila N = 3 | S. maltophilia N = 3 | P. putida N = 3 | P. stutzeri N = 2 | |
|---|---|---|---|---|---|---|---|---|
| Number of isolates (N = 22) | AMP | 6 | – | 0 | – | – | – | – |
| CN | 0 | – | 0 | 0 | – | – | – | |
| TE | 0 | – | 0 | 0 | – | – | – | |
| LEV | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| IMI | 1 | 1 | 0 | 0 | – | 0 | 0 | |
| AK | 0 | 0 | 0 | 0 | – | 0 | 0 | |
| CAZ | 1 | 0 | 4 | (3) INT | – | 0 | 0 | |
| FEP | 0 | 0 | 4 | 0 | – | 0 | 0 | |
| CIP | 1 | 0 | 0 | 0 | – | 0 | 0 | |
| CXT | 0 | – | 0 | 0 | 0 | – | – | |
| MRP | 0 | 0 | 0 | 0 | – | 0 | 0 | |
| CRO | – | – | 0 | (3) INT | – | – | – | |
| MN | 0 | – | 0 | 0 | 0 | – | – | |
| AUG | 0 | – | – | – | – | – | – | |
| CXM | 1 | – | 0 | 0 | – | – | – | |
| ETP | – | – | – | 0 | – | – | – |
(INT) Intermediate (-) Not tested, (AMP) Ampicillin, (CN) Gentamicin, (TE) Tetracycline, (LEV) Levofloxacin, (IMI) Imipenem, (AK) Amikacin, (CAZ) Ceftazidime, (FEP) Cefepime, (CIP) Ciprofloxacin, (CXT) Trimethoprim-sulfamethoxazole, (MRP) Meropenem, (ETP) Ertapenem, (CRO) Ceftriaxone, (MN) Minocycline, (AUG) Amoxicillin-Clavulanate, (CXM) Cefuroxime, (AUG) Amoxicillin-clavulanic acid
Detection of antibiotic resistance genes
For Klebsiella pneumoniae, the resistance gene identified was blaSHV. In the first batch of isolates, Klebsiella pneumoniae showed multidrug-resistance with the resistance genes blaCTX-M, blaSHV, and gyrA. For Acinetobacter baumannii, there were two resistance genes, which are blaSHV and blaCTX-M. For Aeromonas hydrophila, the resistance gene was blaSHV, while for Stenotrophomonas geniculata, the resistance genes were blaCTX-M and blaTEM. Lastly, for Stenotrophomonas hibiscicola, the resistance genes were blaSHV, blaCTX-M, and blaNDM. No resistance genes were detected in Pseudomonas putida, Pseudomonas stutzeri, and Stenotrophomonas maltophilia, as shown in Table 4.
Table (4): The detection of antibiotic resistance genes in the bacteria from the first sample isolate
Bacteria |
Resistance gene |
|---|---|
Klebsiella pneumoniae (MDR) |
blaSHV, blaCTX-M, gyrA |
Acinetobacter baumannii |
blaCTX-M, blaSHV |
Aeromonas hydrophila |
blaSHV |
Stenotrophomonas hibiscicola |
blaSHV, blaCTX-M, blaNDM |
Stenotrophomonas geniculata |
blaCTX-M, blaTEM |
Klebsiella pneumoniae |
blaSHV |
After analysing the sequence of the gyrA gene in Klebsiella pneumoniae from the hospital wastewater, the partial gyrA gene sequence was successfully amplified and submitted to GenBank under accession number PV948197. A point mutation was detected in the Quinolone Resistance-Determining Region (QRDR), especially at codon 83, where the wild-type serine was replaced by arginine, resulting in the S83R mutation, and at codon 87, aspartic acid was replaced with leucine, resulting in the D87L mutation. These mutations were identified through alignment against the gyrA gene of K. pneumoniae strain MGH 78578 (GenBank accession number: CP000647), a widely accepted international reference strain.
This study aims to assess the presence of antimicrobial-resistant bacteria in hospital wastewater at a teaching hospital in Malaysia. This study’s investigation included identifying the species and prevalence of bacteria isolated from hospital wastewater. A total of 28 isolates, representing 11 bacterial species, were recovered, including representative species such as Klebsiella pneumoniae, Acinetobacter baumannii, Aeromonas hydrophila, and members of the Stenotrophomonas maltophilia complex. The presence of these species in all stages of the treatment plant, even after disinfection, indicates that hospital wastewater has the potential to serve as a reservoir and a source of spreading antibiotic-resistant bacteria and antibiotic resistance genes.
A recent study in Malaysia reported the widespread occurrence of wastewater-borne ESKAPE pathogens and associated antimicrobial resistance genes in hospital effluents, highlighting hospitals as important contributors to environmental AMR dissemination. Like the findings of the present study, the study reported the persistence of clinically relevant resistant bacteria across wastewater treatment processes, underscoring the limitations of conventional treatment systems in fully removing antibiotic-resistant bacteria and resistance determinants. These findings are consistent with the resistance patterns and treatment-stage persistence observed in this study, further supporting the role of hospital wastewater as a significant reservoir of antimicrobial resistance in the Malaysian context.10
The prevalence and quantity of beta-lactam resistance genes in hospital wastewater and Enterobacterales isolates were studied in Indonesia. The results showed a high relative abundance of ESBL genes and recommended culture-independent monitoring as a method for early warning systems.17 The global consistency of hospital wastewater as an AMR reservoir has been shown by studies that highlight how hospital effluents act as hotspots for ARB and ARGs and may retain higher ARG abundances than regular municipal wastewater.18
The bacteria reflect both clinical and environmental origins, consistent with findings from other regions. Similar bacterial species such as Klebsiella pneumoniae, Enterobacter cloacae, Citrobacter freundii, Escherichia coli, and Pseudomonas spp. Acinetobacter spp. Aeromonas spp. and Elizabethkingia meningoseptica in Singapore’s hospital wastewater.19 In a study conducted in Indonesia, the following species were identified: Acinetobacter baumannii, Klebsiella pneumoniae, Pseudomonas stutzeri, and Stenotrophomonas maltophilia.20
This variation implies that hospital effluents share a core resistome but vary depending on hospital type, patient demographics, and wastewater management systems.21
Bacterial load was reduced gradually at every stage of wastewater treatment, peaking at the first grit stage and falling off at the outflow outlet. According to another study, there are the most colonies in the first collection tank, but the number drastically drops as the treatment process moves through the other stages. Findings from other hospital wastewater evaluation studies are consistent with the range of bacteria retrieved from the wastewater, which may represent bacterial illnesses throughout the research period.22
One of the Klebsiella pneumoniae isolates was found to be multidrug-resistant. Similar patterns of antibiotic resistance were documented in a Vietnamese hospital, where isolates showed resistance to ampicillin and carbapenems but remained susceptible to amikacin and gentamicin.23 The remaining Klebsiella pneumoniae isolates showed resistance only to ampicillin, which is inherently resistant due to the production of chromosomally encoded β-lactamases (specifically SHV β-lactamase), which can hydrolyze ampicillin and render it ineffective.24
Acinetobacter baumannii also showed resistance to ceftazidime and cefepime, aligning with a previous study in Bangladesh, where the Acinetobacter baumannii isolates tested were resistant to cefepime and ceftazidime, confirming the widespread resistance to third and fourth-generation cephalosporins, the isolates also show resistance to ciprofloxacin, levofloxacin, imipenem and meropenem which suggest there differential resistance mechanisms or selective pressure that effect the resistance of the bacteria.25,26
In contrast, Aeromonas hydrophila showed intermediate resistance to some cephalosporins but was not fully resistant. These findings highlight how resistance varies across and within species. In line with earlier reports of substantial multidrug-resistance in clinical isolates from the same hospital, cephalosporins and carbapenems were the most affected, even though no clear pattern was seen.27,28
The main resistance determinants detected were blaTEM, blaSHV, blaCTX-M, blaNDM, and gyrA. A study conducted in Slovakia and the Czech Republic has identified high levels of blaTEM and blaSHV genes in ESBL-producing E. coli isolated from urinary tract infections. A significant incidence of blaTEM-positive (ARB) has been observed in hospitals, indicating a possible reservoir for resistance genes.29
Our study shows that β-lactamase genes were the most detected resistance genes across all bacterial species isolated from hospital wastewater. The genetic diversity and high prevalence of antibiotic resistance genes, particularly β-lactamases, were also identified by a Singaporean study. These genes were frequently found to co-occur with clinically relevant pathogens.19
A study in Croatia found that certain genes can give resistance to various antibiotics, which is an important factor in the development of multidrug-resistance (MDR), and it also found that resistance genes, including blaCTX-M, blaKPC-2, blaTEM, and blaOXA-48, are linked to resistance to many antibiotic classes, especially β-lactams. Hospital wastewater typically contains high levels of antibiotic residues, creating selective pressure that promotes the survival and spread of resistant bacteria. This supports the discovery that resistance to third-generation cephalosporins can be conferred by the presence of just one resistance gene.30
Mutations in gyrA were linked to fluoroquinolone resistance, particularly ciprofloxacin, consistent with previous reports in clinical Klebsiella pneumoniae isolates, as was found in another study where a mutation in the gene that causes resistance to quinolones and fluoroquinolone antibiotics has grown, raising concerns about the spread of clinical strains of nalidixic acid and ciprofloxacin-resistant K. pneumoniae. A point mutation of the gyrA gene caused the resistance.31
Antibiotic resistance can be fuelled by even low dosages, which could have long-term negative effects on the environment. As demonstrated in Gaza, where Pseudomonas species were discovered in saltwater tainted by treated wastewater, these resistant bacteria can infiltrate natural water bodies.32
Hospital wastewater treatment plants vary in effectiveness, with removal rates of antibiotics and resistance genes ranging from 20.2%-100%. More stable antibiotics like quinolones, such as ofloxacin, are more difficult to remove, but beta-lactams are usually well eliminated.33
At HSAAS, tertiary wastewater treatment using chlorination is applied, which is considered a cost-effective method for reducing microbial loads.34 However, chlorination has limitations, such as forming harmful byproducts, biofilm resistance, and incomplete bacterial inactivation. Additionally, ARGs can still spread through horizontal gene transfer in treatment plants. Emerging hybrid disinfection methods using nanomaterials, natural biocides, and advanced oxidation processes show promise in improving the removal of resistant bacteria and genetic contaminants. These innovative approaches offer a more effective and sustainable solution for tackling antibiotic resistance in wastewater.35
Antibiotic-resistant microorganisms can enter hospital wastewater through patient excreta, contaminated medical devices, and discharges from wards, surgical theatres, and haemodialysis units.36 These factors lead to the introduction of resistant bacteria into the hospital sewage system. To address this, it’s essential to treat hospital waste before it enters the wastewater system. The need for better wastewater management is clear, as resistant bacteria can survive even after treatment, posing serious health risks. To combat the emergence of multidrug-resistant microorganisms, efficient wastewater treatment, ongoing monitoring, and stricter regulations on antibiotic use are crucial. Improved treatment technologies and reliable monitoring systems are key to protecting both human and environmental health.35
The findings of this study support the One Health approach, which acknowledges how the development and spread of antibiotic resistance are linked to the health of people, animals, and the environment. By acting as a pathway between clinical and environmental environments, hospital wastewater allows for the spread of resistance genes like gyrA mutations, blaSHV, blaCTX-M, blaTEM, and blaNDM all the way through the larger ecosystem. These ARGs’ potential to endure despite tertiary therapy highlights the possibility of horizontal gene transfer to environmental bacteria, which could re-enter animal and human populations through contaminated water sources. Therefore, integrating the One Health approach into wastewater monitoring programs may improve early detection and control methods, lowering the overall burden of AMR in community and clinical settings.
However, this study acknowledges several important limitations that represent the main weaknesses of the research. These include the limited number of hospitals involved, the relatively small sample collection, and the bacterial isolation method. Nutrient agar was used for culturing, which does not support the growth of all bacterial types, particularly fastidious, anaerobic, or intracellular bacteria that require special nutrients or conditions. Additionally, resistance gene detection was based only on primers selected according to the observed antibiotic resistance phenotypes. Also, it did not account for other mobile genetic elements such as plasmids, integrons, or transposons. This approach may miss resistance genes that are present but not expressed. Therefore, using whole-genome sequencing would provide a more comprehensive understanding of the resistance gene profile.
The findings of this study highlight the significant presence of antibiotic-resistant bacteria in hospital wastewater, demonstrating the role of hospital wastewater as a potential reservoir for MDR organisms. Given the growing concern over public health risks associated with antibiotic resistance, this study emphasises the need for effective wastewater treatment systems capable of reducing bacterial loads, including resistant strains, to safeguard both environmental and human health. Preventing the spread of antibiotic-resistant organisms requires an integrated approach that combines surveillance, timely detection, and stringent wastewater treatment protocols to mitigate the risks posed by untreated or inadequately treated hospital wastewater.
Additional file: Supplementary Tables.
ACKNOWLEDGMENTS
The authors are thankful to the hospital’s engineering department personnel for their expertise and assistance throughout this study.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
This study was funded by the Universiti Putra Malaysia Focused Grant (GP-F/JPAT/JMP/6307013-14001).
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript and/or in the supplementary files.
ETHICS STATEMENT
This article does not contain any studies on human participants or animals performed by any of the authors.
- Yuan T, Pian Y. Hospital wastewater as hotspots for pathogenic microorganisms spread into aquatic environment: A review. Front Environ Sci. 2023;10:1091734.
Crossref - Gaze WH, Krone SM, Larsson DJ, et al. Influence of humans on evolution and mobilization of environmental antibiotic resistome. Emerg Infect Dis. 2013;19(7):e120871.
Crossref - Tello A, Austin B, Telfer TC. Selective pressure of antibiotic pollution on bacteria of importance to public health. Environ Health Perspect. 2012;120(8):1100-1106.
Crossref - Alam MZ, Aqil F, Ahmad I, Ahmad S. Incidence and transferability of antibiotic resistance in the enteric bacteria isolated from hospital wastewater. Braz J Microbiol. 2013;44:799-806.
Crossref - Kumar A, Pal D. Antibiotic resistance and wastewater: Correlation, impact and critical human health challenges. J Environ Chem Eng. 2018;6(1):52-58.
Crossref - Reynolds D, Burnham JP, Guillamet CV, et al. The threat of multidrug-resistant/extensively drug-resistant Gram-negative respiratory infections: another pandemic. Eur Respir Rev. 2022;31(166):220068.
Crossref - Li S, Ondon BS, Ho S-H, Jiang J, Li F. Antibiotic resistant bacteria and genes in wastewater treatment plants: from occurrence to treatment strategies. Sci Total Environ. 2022;838(part 4):156544.
Crossref - Lymperatou D, Konstantopoulou R, Mentsis M, et al. Hospital Wastewater Surveillance and Antimicrobial Resistance: A Narrative Review. Microorganisms. 2025;13(12):2739.
Crossref - Bakon SK, Mohamad ZA, Jamilan MA, et al. Prevalence of antibiotic-resistant pathogenic bacteria and level of antibiotic residues in hospital effluents in Selangor, Malaysia: Protocol for a cross-sectional study. JMIR Res Protoc. 2023;12(1):e39022.
Crossref - Bakon SK, Zakaria NFS, Jamilan MA, Hashim H, Mohamad ZA. City or Suburb, Resistance Flows: Wastewater-Borne ESKAPE and AMR Genes in Malaysian Hospitals. Antibiotics. 2025;14(11):1058.
Crossref - Janda JM, Abbott SL. 16S rRNA gene sequencing for bacterial identification in the diagnostic laboratory: pluses, perils, and pitfalls. J Clin Microbiol. 2007;45(9):2761-4.
Crossref - Institute CaLS. Performance standards for antimicrobial susceptibility testing. 34 ed. Wayne, PA: Clinical and Laboratory Standards Institute; 2024.
- Sharma M, Pathak S, Srivastava P. Prevalence and antibiogram of Extended Spectrum -Lactamase (ESBL) producing Gram negative bacilli and further molecular characterization of ESBL producing Escherichia coli and Klebsiella spp. Journal of clinical and diagnostic research: JCDR. 2013;7(10):2173.
Crossref - Ravikant, Kumari P, Kumar M, Roy P, Jeya M. Detection of carbapenem-resistant Enterobacteriaceae by realtime pcr and assessment of hospitalization related risk factors associated with their fecal carriage: a casecontrol study. J Pure Appl Microbiol. 2022;16(2):1111-1121.
Crossref - Bhatt P, Tandel K, Das NK, Grover N, Ranjan P, Rathi K. Phenotypic detection and molecular characterization of carbapenem-resistant Enterobacteriaceae at a tertiary care center. Journal of Marine Medical Society. 2022;24(Suppl 1):S40-S6.
Crossref - Onseedaeng S, Ratthawongjirakul P. Rapid detection of genomic mutations in gyrA and parC genes of Escherichia coli by multiplex allele specific polymerase chain reaction. Journal of Clinical Laboratory Analysis. 2016;30(6):947-55.
Crossref - Santosaningsih D, Fadriyana AP, David NI, Ratridewi I. Prevalence and abundance of beta-lactam resistance genes in hospital wastewater and enterobacterales wastewater isolates. Trop Med Infect Dis. 2023;8(4):193.
Crossref - Zhang S, Huang J, Zhao Z, Cao Y, Li B. Hospital wastewater as a reservoir for antibiotic resistance genes: a meta-analysis. Front Public Health. 2020;8:574968.
Crossref - Haller L, Chen H, Ng C, et al. Occurrence and characteristics of extended-spectrum -lactamase-and carbapenemase-producing bacteria from hospital effluents in Singapore. Sci Total Environ. 2018;615:1119-1125.
Crossref - Budayanti NS, Aisyah DN, Fatmawati NND, Tarini NMA, Kozlakidis Z, Adisasmito W. Identification and distribution of pathogens in a major tertiary hospital of Indonesia. Front Public Health. 2020;7:395.
Crossref - Johar A, Salih MA, Abdelrahman HA, Al Mana H, Hadi HA, Eltai NO. Wastewater-based epidemiology for tracking bacterial diversity and antibiotic resistance in COVID-19 isolation hospitals in Qatar. J Hosp Infect. 2023;141:209-220.
Crossref - Kalaiselvi K, Mangayarkarasi V, Balakrishnan D, Chitraleka V. Survival of antibacterial resistance microbes in hospital-generated recycled wastewater. J Water Health. 2016;14(6):942-949.
Crossref - Nguyen TNT, Nguyen PLN, Le NTQ, et al. Emerging carbapenem-resistant Klebsiella pneumoniae sequence type 16 causing multiple outbreaks in a tertiary hospital in southern Vietnam. Microbial Genom. 2021;7(3):000519.
Crossref - Fu Y, Zhang F, Zhang W, et al. Differential expression of blaSHV related to susceptibility to ampicillin in Klebsiella pneumoniae. Int J Antimicrob Agents. 2007;29(3):344-347.
Crossref - Gu D, Wu Y, Chen K, et al. Recovery and genetic characterization of clinically-relevant ST2 carbapenem-resistant Acinetobacter baumannii isolates from untreated hospital sewage in Zhejiang Province, China. Sci Total Environ. 2024;916:170058.
Crossref - Hossain MA, Fatima NNE, Tushar JH, Mahmud H, Haque FKM. Isolation and characterization of Acinetobacter baumannii from environmental waters in Dhaka City, Bangladesh. BMC Microbiol. 2025;25(1):1-11.
Crossref - Labi A-K, Obeng-Nkrumah N, Addison NO, Donkor ES. Salmonella blood stream infections in a tertiary care setting in Ghana. BMC Infect Dis. 2014;14:1-10.
Crossref - Von Wintersdorff CJH, Penders J, Van Niekerk JM, et al. Dissemination of antimicrobial resistance in microbial ecosystems through horizontal gene transfer. Front Microbiol. 2016;7:173.
Crossref - Lepesova K, Olejnikova P, Mackulak T, Cverenkarova K, Krahulcova M, Birosova L. Hospital wastewater-Important source of multidrug resistant coliform bacteria with ESBL-production. Int J Environ Res Public Health. 2020;17(21):7827.
Crossref - Puljko A, Rozman SD, Barisic I, et al. Resistance to critically important antibiotics in hospital wastewater from the largest Croatian city. Sci Total Environ. 2023;870:161805.
Crossref - Ahmadi Z, Noormohammadi Z, Behzadi P, Ranjbar R. Molecular detection of gyrA mutation in clinical strains of Klebsiella pneumoniae. Iran J Public Health. 2022;51(10):2334.
Crossref - Elmanama AA, ElKichaoui AY, Mohsin MM. Contribution of hospital wastewater to the spread of antibiotic resistance in comparison to non-health. J AL-Aqsa Univ. 2006;10(1):108-121.
- Yao S, Ye J, Yang Q, et al. Occurrence and removal of antibiotics, antibiotic resistance genes, and bacterial communities in hospital wastewater. Environ Sci Poll Res. 2021;28(40):57321-57333.
Crossref - Zagklis DP, Bampos G. Tertiary wastewater treatment technologies: a review of technical, economic, and life cycle aspects. Processes. 2022;10(11):2304.
Crossref - Mandal TK. Nanomaterial-Enhanced Hybrid Disinfection: A Solution to Combat Multidrug-Resistant Bacteria and Antibiotic Resistance Genes in Wastewater. Nanomaterials. 2024;14(22):1847.
Crossref - Khan NA, Vambol V, Vambol S, et al. Hospital effluent guidelines and legislation scenario around the globe: A critical review. J Environ Chem Eng. 2021;9(5):105874.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.