


ISSN: 0973-7510
E-ISSN: 2581-690X
Neisseria gonorrhoeae (NG) is a sexually transmitted pathogen with increasing treatment challenges due to the rise in antimicrobial resistance. The emergence of drug-resistant strains necessitates the need for alternative and novel strategies for treatment. The aim of this research work was to assess the antimicrobial, bactericidal, and biofilm inhibitory potential of Nagarmotha, Basil, Sugandhmantri, Palmarosa, Eucalyptus, Lemongrass, Spearmint, Ginger, and Peppermint essential oils (EOs) against MDR clinical isolates of NG. The study was approved by the Institutional Ethics Committee, Indira Gandhi National Tribal University, Amarkantak, Madhya Pradesh, India. Endocervical/vaginal swab samples (n = 223) were collected from women aged 20-55 years, presenting with one or more symptoms of sexually transmitted infections (STIs). Clinical samples were cultured on specific media for the identification of NG. AST of standard antibiotics was performed using the Kirby-Bauer disc diffusion method. The antibacterial effect of selected EOs was assessed using agar well diffusion, and MIC and MBC were determined by broth microdilution methods. Biofilm inhibition was evaluated using a microtiter plate assay. Out of 223 swab samples, 100 (44.84%) were tested positive for NG. AST revealed that 36 isolates were MDR. Nagarmotha and Sugandhmantri essential oils exhibited the lowest MIC (20.83 µg/ml) and MBC (83.83 µg/ml) values for both. Nagarmotha and Sugandhmantri essential oils also showed high biofilm inhibition by 50.87% and 43.85% at 1/2 MIC concentration, respectively. GC-MS analysis indicated presence of Cyprene (45.64%) in Nargarmotha and Linalool (40.19%) in Sugandhmantri, as the major compounds. The findings suggest that Sugandhmantri and Nagarmotha essential oils, or their major phytochemicals may have promising applications in management of NG infections.
Neisseria Gonorrhoeae, Multidrug-resistance, Essential oil, Biofilm inhibition, Phytochemicals
Antibiotic resistance has become one of the major global health challenges. The rapid emergence and widespread dissemination of multidrug-resistant bacteria are increasingly compromising the effectiveness of existing treatments for common infectious diseases. According to the World Health Organization (WHO), infection with drug resistant microbes was directly responsible for an estimated 1.27 million deaths and was a contributing factor in nearly 4.95 million deaths worldwide, in 2019.1 Bacteria acquire resistance through multiple mechanisms including modification of drug binding targets, reduced drug influx, increased drug efflux, or enzymatic inactivation of antimicrobial agents.2 Addressing the growing crisis of antimicrobial resistance necessitates new therapeutic agents and drug targets.
Neisseria gonorrhoeae (NG) is a Gram-negative diplococcus bacterium that primarily infects the human urogenital tract and causes Gonorrhoea, a sexually transmitted disease associated with severe complications, such as pelvic inflammatory conditions, prostatitis, ectopic pregnancy, and impaired fertility in women.3 If left untreated, the infection may disseminate through bloodstream, leading to systemic conditions like arthritis and cardiac infections. Globally, infection caused by NG is actually one of the most common sexually transmitted infections. WHO estimated about 82.4 million new NG infections among adults aged 15-49 years, globally in 2020.4 Currently, antibiotics remain the only effective treatment option due to the absence of a reliable and effective vaccine.5 NG has developed resistance against most classes of antibiotics, including β-lactams, Tetracyclines, Macrolides, Fluoroquinolones, and Sulfonamides.6 Alarmingly, resistance to Cephalosporins, which was considered as the last line of defence, has been reported worldwide.7 Reports from 2007 to 2018 revealed rising resistance to Ceftriaxone, Cefixime, and other antibiotics across continents, prompting an urgent need for newer antibiotics or alternative treatments.8 Adding to the challenge, NG exhibits a significant ability to form biofilms, further contributing to its antimicrobial tolerance.3
In recent years, the search for alternative antimicrobial agents has intensified, especially extracts and phytochemicals of medicinal and aromatic plant origin. Their efficacy is attributed to the complex mixture of bioactive compounds present in the extracts, which act synergistically on multiple targets in bacterial cells, rather than relying on a single component or mechanism. Beyond direct antimicrobial effect, essential oils (EOs) have also been reported to inhibit toxin production, bacterial motility, biofilm formation, and quorum sensing, further supporting their use as antimicrobial agents.9-11 Recent studies have shown the antimicrobial and biofilm inhibitory effect of EOs of Pinus sylvestris, Citrus limon, and Origanum vulgare against NG and Streptococcus suis.12 Several ethnobotanical investigations have reported the traditional use of plants to manage STIs.13-16
In the present investigation, the antibacterial activity of nine EOs derived from different plant species was evaluated against multidrug-resistant clinical isolates of NG. Furthermore, the biofilm inhibitory potential of bioactive EOs was also assessed. The chemical composition of the bioactive EOs was further elucidated using GC-MS.
Collection of clinical samples
Endocervical /vaginal swab samples were collected from 223 symptomatic women (aged 20 to 55 years) attending the outpatient departments of the District Hospital, Anuppur, and Birsamunda Government Medical College, Shahdol, Madhya Pradesh, India. The samples were transported to the Infection Biology and Molecular Toxicology Laboratory for further processing.
Ethical approval
Ethical approval for the present research was obtained from the Institutional Ethics Committee, Indira Gandhi National Tribal University (Ref. No. IGNTU/IEC/2025/05A). Written informed consent was obtained from the participants before enrolling in the study.
Collection of essential oil
Nagarmotha (Cyperus scariosus), Basil (Ocimum basilicum), Palmarosa (Cymbopogon martini), Eucalyptus (Eucalyptus globulus), Spearmint (Mentha spicata) and Peppermint (Mentha piperita) essential oils were gifted by Ori Oils Pvt. Ltd., Kadamtola, Industrial Area, Anuppur, Madhya Pradesh. Sugandhmantri (Homalomena aromatica), Lemongrass (Cymbopogon flexuosus) and Ginger (Zingiber officinale) EOs were obtained from the Department of Horticulture, Aromatic and Medicinal Plants, Mizoram University, Aizawl, Mizoram, India.
Culture of NG
The clinical samples were cultured on chocolate agar and Thayer Martin selective media, enriched with vitamin growth supplement, haemoglobin, and VCNT (Vancomycin, Colistin, Nystatin, and Trimethoprim), and incubated overnight at 37 °C at 5% CO2, using modified protocol adapted from Juhi et al.17
Biochemical test
Confirmatory biochemical tests were conducted using the HiNeisseria™ Identification Kit (KB008) to verify the presence of NG. The kit includes 12 biochemical tests: Urease, ONPG, Voges-Proskauer, Oxidase, Catalase, Nitrate Reduction, Glucose, Maltose, Lactose, Sucrose, Fructose, and Mannose. Cultures that passed at least 8 of these tests were confirmed as NG.
Molecular confirmation of NG
To further verify species identification, confirmed culture positive isolates were analyzed by real-time PCR targeting the species specific orf1 gene. Each amplification run included appropriate positive and negative controls to ensure the reliability and accuracy of the test.
Anti-microbial susceptibility test (AST)
The NG was cultured on Muller-Hinton agar and the AST was performed by disc diffusion method. A total of 9 commonly used antibiotic discs {Tetracycline (TE), Ceftriaxone (CTR), Azithromycin (AZM), Ciprofloxacin (CIP), Levofloxacin (LE), Cefixime (CFM), Erythromycin (E), Doxycycline (DO) and Ofloxacin (OF)} at different concentrations were used to test the resistance pattern of NG. The antibiotics were considered sensitive, moderately sensitive, or resistant based on their inhibition zones in accordance with the Clinical and Laboratory Standards Institute (CLSI, 2024) guidelines. Strains exhibiting resistance to at least three antibiotics were classified as multidrug-resistant (MDR) and selected for subsequent analysis.
Antibacterial activity of EOs against NG
The antibacterial effect of the EOs against MDR clinical isolates (CIs) of NG was determined using an agar well diffusion method. EOs were dissolved in dimethyl sulfoxide (DMSO) to prepare stock solutions. Mueller-Hinton agar plates were inoculated with standardized bacterial inoculum (0.5-1 McFarland) to prepare a lawn culture. Wells of 7 mm diameter were punched in petri plates and each well was loaded with 50 µL of EO solution diluted with DMSO at 50% v/v concentration. Plates were incubated overnight at 37 °C under 5% CO2 for the growth of the bacteria. The antibacterial activity of EOs was measured in terms of zones of growth inhibition formed around each well.
Minimal inhibitory concentration (MIC) and minimal bactericidal concentration (MBC)
MIC and MBC of EOs and antibiotics were assessed through the microdilution method as per CLSI, 2024 guidelines. EOs were mixed with DMSO and subjected to two-fold serial dilutions in a 96-well microtiter plate to obtain final concentrations ranging from 166.6-0.39 µg/mL (v/v). Each well was inoculated with standardized bacterial suspensions and the plates were incubated overnight. MIC was considered as the minimum concentration of EO that completely inhibited the visible growth of NG, while the MBC was the minimum concentration required to reduce 99.9% of the bacterial population.
Biofilm inhibition
The microtiter plate assay was employed to assess the effects of EOs on biofilm formation at various sub-MIC levels, with minor modifications to previously reported methods. 9,18 Biofilms were grown at 37 °C, 5% CO2 for 24-72 hours in the presence of EOs, at various sub MICs. To remove planktonic cells, the wells were properly drained the following day and rinsed three times with sterile Phosphate-buffered saline (PBS). For biofilm staining, 150 μL of 0.8% crystal violet solution was added to each well, and the plate was incubated at room temperature for 20 minutes. The excess stain was removed subsequently by washing the wells with sterile PBS, and the plate was left to air-dry. To release the dye bound to the biofilm cells, 150 μL of 30% (v/v) glacial acetic acid was added into each well. The extent of biofilm inhibition was then quantified by recording the absorbance of treated and control groups at 600 nm. All experiments were performed in triplicate to ensure reproducibility. Mueller-Hinton broth served as the medium control, distilled water as the untreated (blank) control, DMSO as the solvent control, and antibiotic treated wells were used as the positive control. Optical density values were normalized by subtracting the corresponding blank values. Sub MIC concentrations of all EOs were screened for their ability to inhibit biofilm formation, and active EOs were selected for further investigations.
Phytochemical analysis of active EOs using Gas Chromatography-Mass Spectrometry (GC-MS)
The GC-MS analysis of EOs was conducted using a Perkin Elmer Clarus 680 GC system, coupled with a PE SQ-8 C mass analyzer. The analysis was carried out using an Elite-5MS capillary column (30 m × 0.25 mm, 0.25 µm). Helium was employed as the carrier gas at a steady flow rate of 1 mL/min. The oven temperature was initially set at 40 °C for 5 minutes, then gradually increased to 260 °C with programme rate of 12 °C/min. The oven was kept for an additional 5 minutes at final temperature. The injector temperature was set at 250 °C, operating in split mode (1:50) with a 1 µL injection volume using a Programmable Split Splitless Injector (PSSI). The ion source was operated at 180 °C, while the transfer line temperature was set at 200 °C. Electron ionization was applied at 70 eV, and mass spectra were recorded over a scan range of m/z 50-1000 amu. Identification of compounds was achieved by matching the obtained spectra with standard reference libraries, including NIST and Wiley, in accordance with established protocols.19
Statistical analysis
SPSS version 20.0 was used for statistical analysis. The mean, standard deviation, and P-values at 95% confidence intervals (CIs) were calculated for MICs and biofilm inhibition (OD and %). One way ANOVA was performed to compare the MIC values among the EO treated groups and the standard antibiotic. Additionally, two-way ANOVA was applied to determine the influence of different EOs and sub-MIC concentrations on biofilm inhibition percentage.
Out of the 223 swab samples, 100 (44.84%) were culture + ve exhibiting a grey coloured colony on Chocolate agar and Thayer-Martin agar, indicative of NG growth. The remaining 123 samples (55.15%) were culture-ve for NG (Figures 1A and B). For further confirmation of NG, all 100 culture-positive samples were subjected to 12 biochemical tests. Out of the 100 samples, 63 samples were positive for 10 biochemical tests, 17 samples were positive for 9 tests, and the remaining 20 samples were positive for 8 biochemical tests. The phenotypic and biochemical identification of NG was further confirmed by real-time PCR.
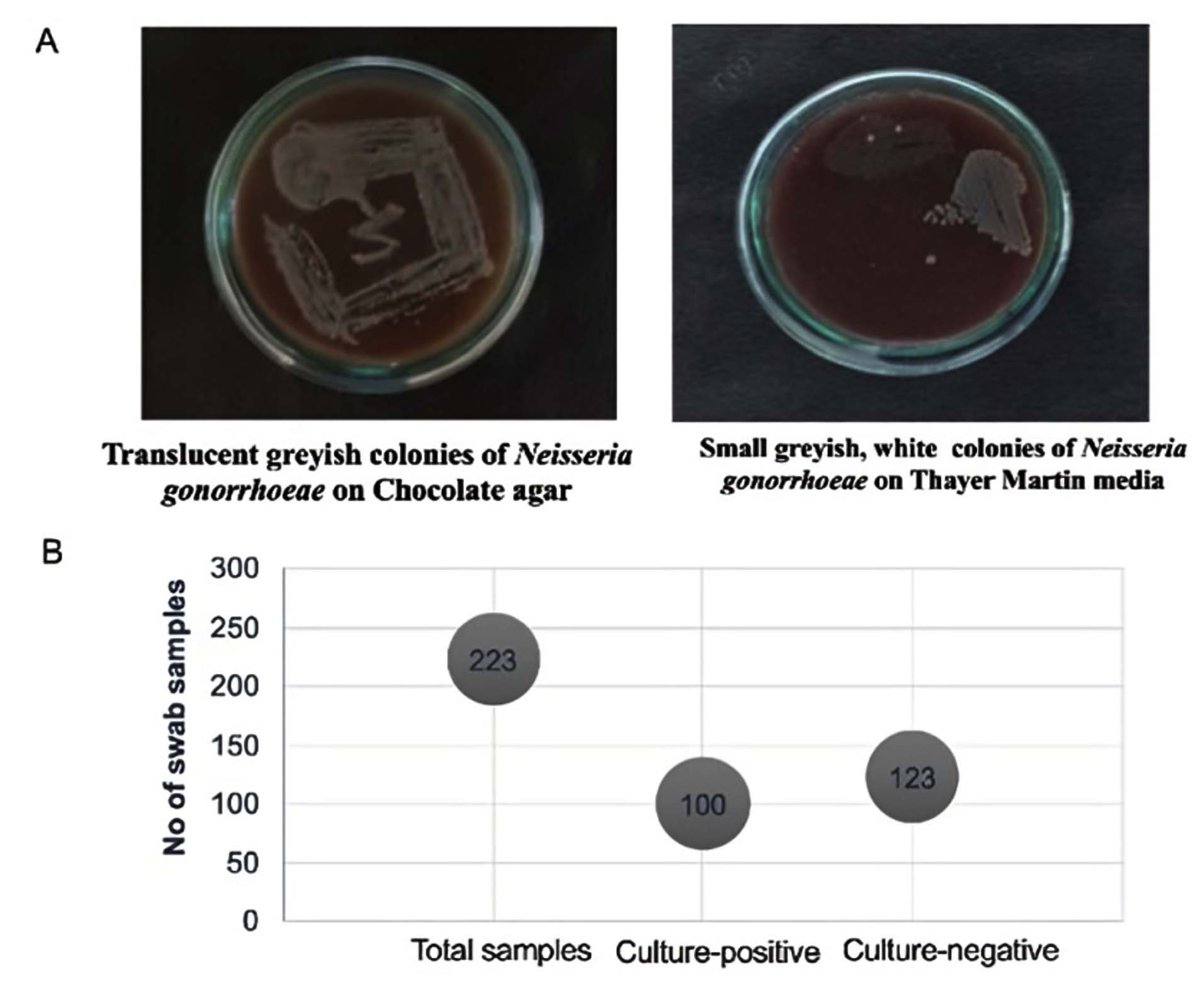
Figure 1. Growth of NG on chocolate and Thayer-Martin culture media
Antibiotic susceptibility test
AST revealed varied resistance profiles of NG against nine commonly used antibiotics. Among the 100 culture-positive swab samples from STI patients, 36 strains were identified as MDR. The resistance patterns of these MDR strains, as shown in Figures 2A and 2B indicate clinical isolates resistant to one, two, three, or four antibiotics. Figure 2C represents the heatmap of antibiotic resistance profiles, where blue indicates resistant strains and white indicates sensitive strains. Most of the samples were resistant to four or more antibiotics, with a notable rise in the number of highly resistant isolates. The highest resistance against nine antibiotics was observed in 16, highlighting a significant spread of MDR-NG.
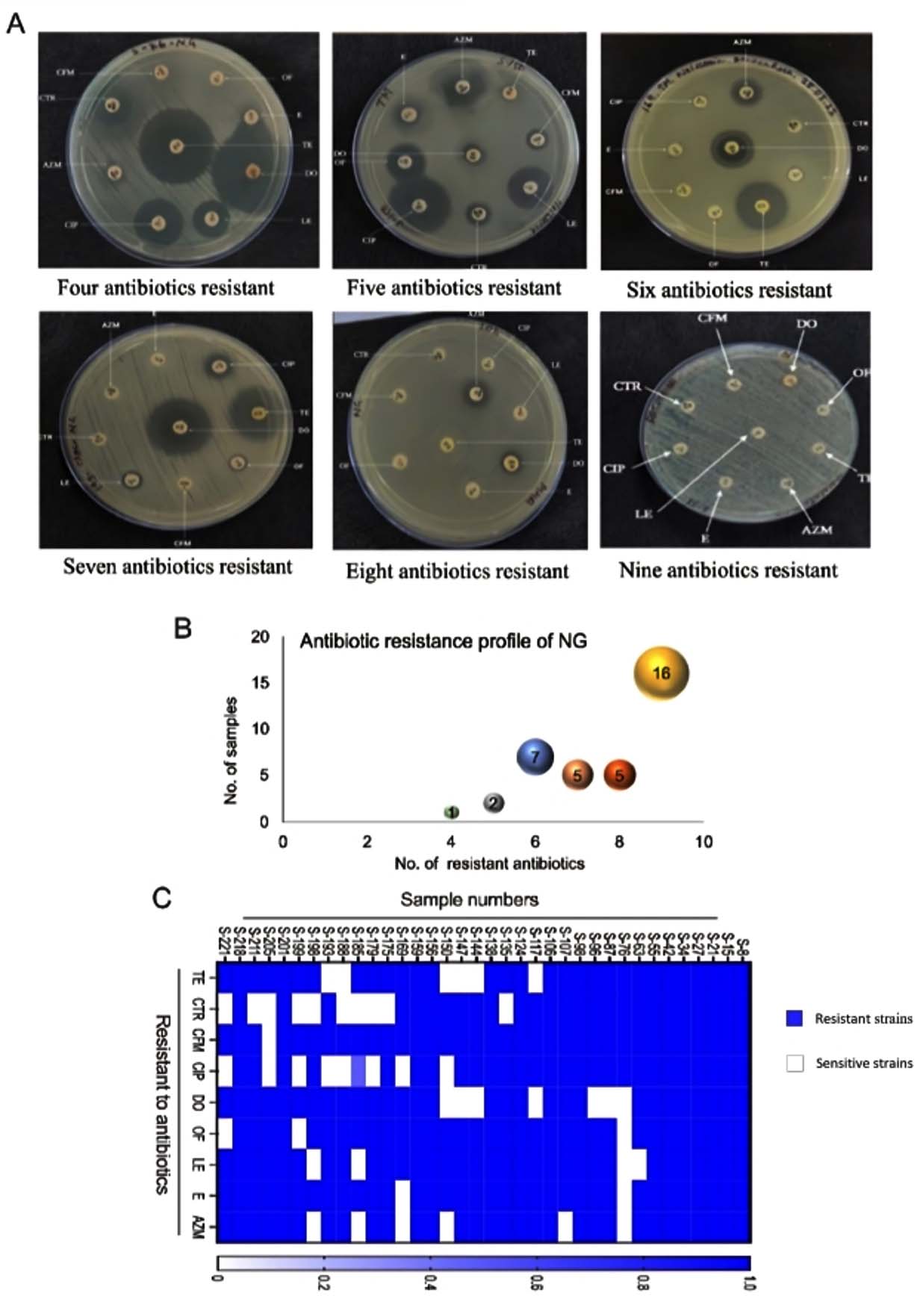
Figure 2. (A) AST pattern of NG positive samples. (B) Antibiotic resistance profile of NG. (C) Sample wise data (Heatmap) showing resistant and sensitive antibiotics against NG
Antimicrobial activity of EOs
The antimicrobial activity of EOs against NG was shown in Figure 3A. Nagarmotha displayed the highest inhibitory effect against all the MDR isolates, with the highest inhibition zone of (20 ± 0.20 mm), followed by Basil (18 ± 0.9 mm), Sugandhmantri (16 ± 0.18 mm), and Palmarosa (16 ± 0.18 mm). Moderate efficacy was exhibited by Eucalyptus, Spearmint, and Lemongrass EOs. Ginger EO had the lowest efficacy (12 ± 0.16) and Peppermint EO did not show any effect against any of the MDR strains (Figure 3B).
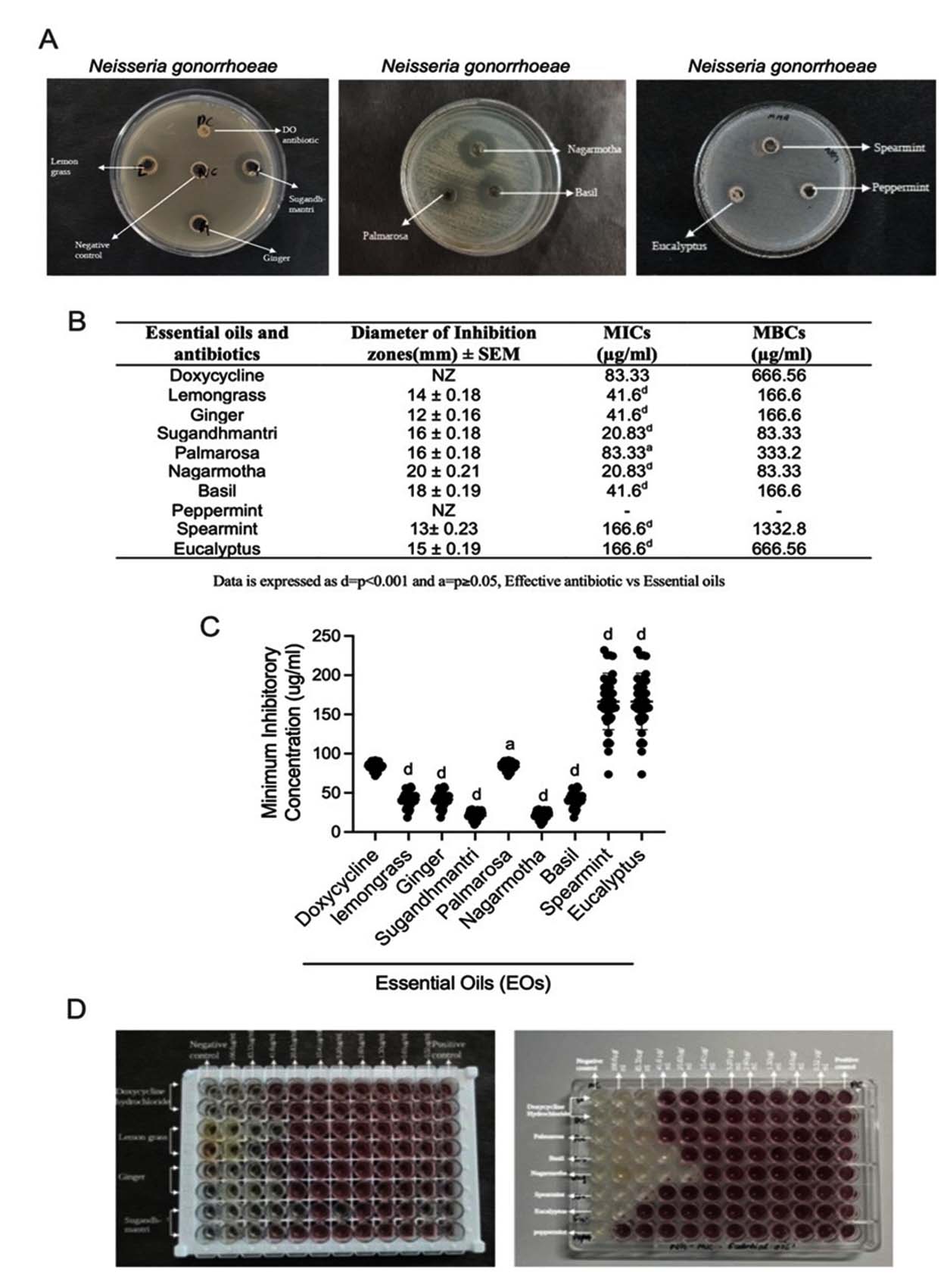
Figure 3. (A & B) Antibacterial effect, MICs and MBCs of EOs against MDR-NG. (C & D) MICs of antibiotics and EOs against MDR-NG on a 96-well plate. Data is expressed as d = P<0.001, a = P≥0.05, Effective antibiotic Vs EOs
Minimum Inhibitory Concentrations (MICs) and Minimum Bactericidal Concentration (MBC) determination
Figures 3C and 3D present the MIC and MBC values of antibacterial EOs against MDR isolates of NG, determined using the broth microdilution method. Nagarmotha and Sugandhmantri were the most effective, with a MIC of 20.83 µg/ml and an MBC of 83.33 µg/ml exhibited by both oils. Lemongrass, Ginger, and Basil exhibited MICs of 41.6 µg/ml and MBCs of 166.6 µg/ml, while Palmarosa showed MIC of 83.33 µg/ml and an MBC of 333.2 µg/ml. Eucalyptus and Spearmint showed the MIC values (166.6 µg/ml), with MBCs of 666.56 µg/ml and 1332.8 µg/ml, respectively. Doxycycline hydrochloride had a MIC of 83.33 µg/ml and an MBC of 666.56 µg/ml.
Biofilm inhibition of EOs
Nagarmotha exhibited a significant reduction in biofilm formation. The lowest OD of 0.28 was observed at 1/2 MIC, indicating strong biofilm inhibition by Nagarmotha EO. The inhibition percentage followed a similar trend, showing the highest inhibition of 50.87% at 1/2 MIC, which decreased to 15.78% at 1/8 MIC (Figure 4B). Similarly, Sugandhmantri demonstrated a dose-dependent reduction of biofilm formation, with an OD of 0.32 at 1/2 MIC, increasing to 0.51 at 1/8 MIC. The corresponding biofilm inhibition percentages were 43.85% at 1/2 MIC, 24.56% at 1/4 MIC, and 10.52% at 1/8 MIC, indicating moderate biofilm inhibition (Figure 4C).
In contrast, the inhibition percentage for Doxycycline was 29.82% at 1/2 MIC, dropping significantly to 0% at 1/8 MIC (showing OD value of 0.57) (Figure 4A). The results indicated that Doxycycline was less effective in eradicating biofilm at low concentrations, as compared to Nagarmotha and Sugandhmantri.
The OD and biofilm inhibition percentages of Nagarmotha, Doxycycline, and Sugandhmantri were presented in Figure 4.
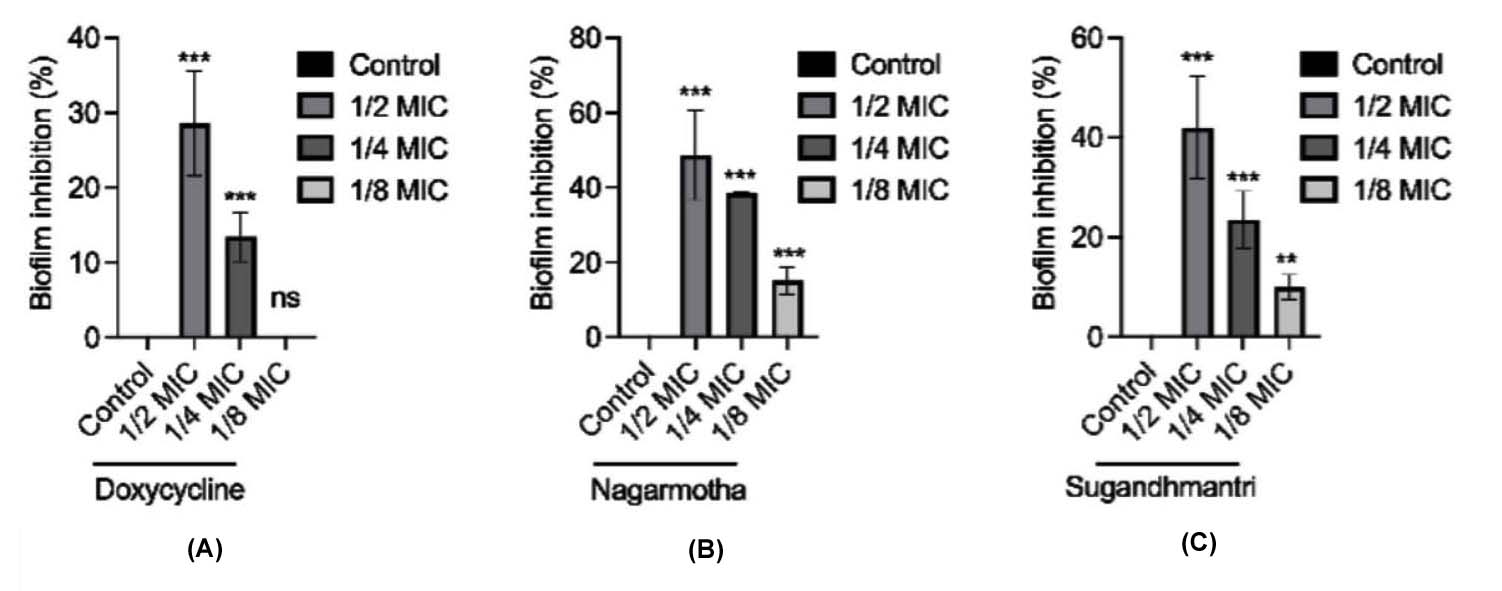
Figure 4. Inhibition of biofilm formation (A) Resistant antibiotic (B & C) Active EOs
GC-MS analysis of Nagarmotha and Sugandhmantri EOs
The GC-MS analysis of Nagarmotha identified the presence of four major sesquiterpenes (Figure 5A). Cyprene was identified as the predominant compound (45.648%), followed by caryophyllene (11.375%), copaene (6.129%), and aciphyllene (5.623%).
The GC-MS analysis of Sugandhmantri revealed a varied profile of compounds, with Linalool (40.19%) being the most abundant, followed by Terpinen-4-ol (22.11%) and Isolongifolol (10.96%) as shown in (Figure 5B). Other notable constituents include L-Alpha-Terpineol (3.25%), Alpha-Cadinol (3.59%), Gamma-Terpinene (1.80%), Beta-Phellandrene (1.29%), O-Cymene (1.58%), and 3-Carene (0.88%).
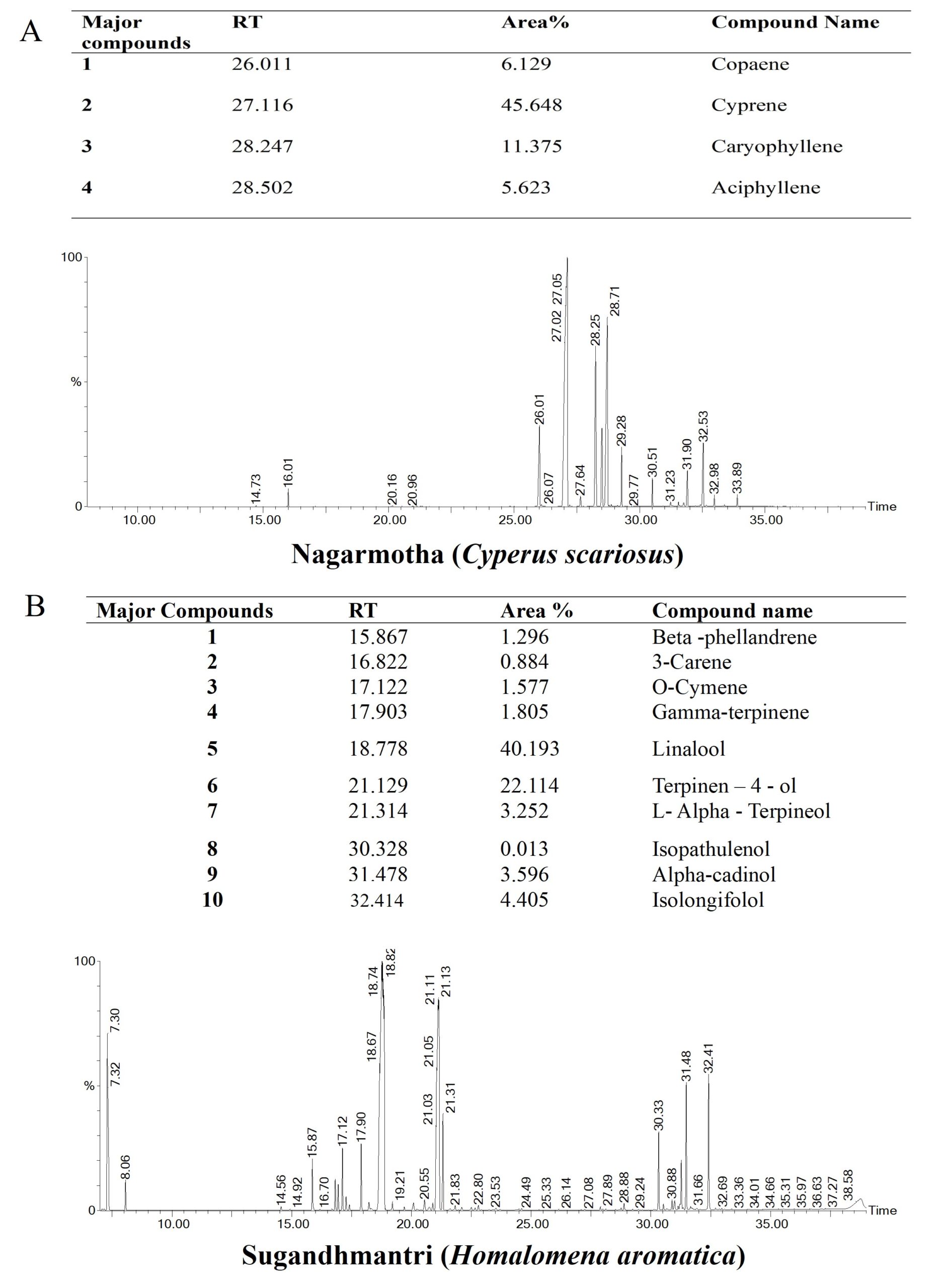
Figure 5. GC-MS chromatogram showing the major chemical constituents of (A) Nargarmotha (B) Sugandhmantri EOs, respectively
Plant compounds, including EOs, have long been used in traditional medicine to manage microbial infections. EOs are rich in secondary metabolites that can reduce the growth of bacteria, yeasts, and molds.20,21 Recent studies have demonstrated that EOs derived from plants such as Clove and Tea tree exhibit potent antibacterial activity against human pathogens, which suggests their potential as viable alternatives or adjuncts to present day antimicrobials.22 Despite the promising results regarding the antimicrobial efficacy of EOs, there is a notable scarcity of studies specifically addressing their role in the management of STIs. This gap is particularly concerning given the rising rates of antibiotic resistance in STIs. Therefore, the present work was focused on evaluating the antibacterial and biofilm inhibition efficacy of plant EOs for controlling the NG infection.
The need for alternative approaches against MDR-NG has led to increasing interest in plant derived antimicrobials. For instance, Coscinium fenestratum extracts have shown MIC values of 56.39 μg/mL against NG, including 11 clinical isolates.23 Similarly, Bridelia retusa extracts have exhibited inhibitory effects on reference gonococcal strains, with MIC values ranging from 16 to 312 μg/mL.24 Research has also highlighted the antibacterial properties of Jacaranda cuspidifolia hexane extracts, which displayed an MIC of 25200 μg/mL,25 while ether extracts from Cassia alata roots were effective at an MIC of 1043 μg/mL.26 In another report, Syzygium cumini leaf extracts have demonstrated bactericidal properties against NG, although at relatively higher MIC values, reaching up to 500 μg/mL.24 Furthermore, solvent extracts of Terminalia sericea (1000 μg/mL), Hypericum aethiopicum root extract (300 μg/mL), and Tarchonanthus camphoratus (500 μg/mL) demonstrated notable antimicrobial effects. Similar observations were made with Aloe ferox.27 Essential oil obtained from Croton gratissimus exhibited strong antibacterial effect with an MIC of 1000 μg/mL. Early screening of 46 Guatemalan plants also identified seven species with inhibitory effects exceeding 10 mm diameter in disc diffusion tests.28 The findings of this study demonstrated that EOs from Nagarmotha, Sugandhmantri and Palmarosa exhibited lower MIC values compared to conventional antibiotics. Among the tested essential oils, Nagarmotha exhibited the lowest MIC and MBC values against NG (20.83 µg/mL and 83.33 µg/mL, respectively), indicating comparatively strong in vitro antibacterial activity. Rahman and Anwar reported MIC and MBC values of 80 µg/mL and 320 µg/mL, respectively, against Escherichia coli.29 Similarly, Jha et al. demonstrated antimicrobial effect of EOs against drug resistant organisms including E. coli, Klebsiella pneumoniae, Staphylococcus aureus, and Enterococci, with MIC values ranging from 95 to 250 µg/mL.30 Mitra et al. reported that Sugandhmantri exhibited antimicrobial effects against MDR E. coli, S. aureus, and K. pneumoniae, with MIC values between 134 and 1075 µg/mL,31 which are higher than the MIC observed against NG in the present study.
Eucalyptus demonstrated MIC and MBC values of 166.6 µg/mL and 666.6 µg/mL, respectively, against NG. In contrast, previous studies have reported MIC values of 3000-4000 µg/mL and MBC values of 3600-9000 µg/mL against Pseudomonas aeruginosa, E. coli, Bacillus subtilis, Listeria innocua, and Staphylococcus aureus.32 Basil has been reported to inhibit Clostridium perfringens with an MIC value of 5000 µg/mL,33 which is higher than the MIC value of 41.6 µg/mL observed against NG in the current study. Additionally, Lemongrass exhibited an MIC of 41.6 µg/mL against NG, whereas Burt reported MIC values of 0.6 µg/mL for E. coli and S. aureus, and 2.5 µg/mL for Salmonella typhimurium.34 These findings suggest that the tested EOs exhibit a notable antibacterial effect against NG compared to other bacterial pathogens previously reported, indicating their potential as promising alternatives for managing MDR-NG.
Biofilm formation by NG adds an additional layer of complexity in addressing infections, as biofilms enhance both antimicrobial resistance (AMR) and antibiotic tolerance. Studies have shown that NG can develop biofilms on abiotic surfaces, including glass, plastic, and human epithelial cells from the urethra and cervix.35 Evidence also suggests that biofilms in cervical infections, indicating their role in the pathogen’s persistence within the host.36 Once a biofilm is established, eliminating NG becomes more challenging, contributing to its resistance to antibiotics and leading to persistent or recurrent infections. Nagarmotha oil exhibited 50.87% biofilm inhibition at ½ MIC concentration, followed by Sugandhmantri with 43.85% inhibition at ½ MIC concentration. Although studies on the biofilm inhibition potential of EOs against NG are limited, Jurado et al. demonstrated a 20% reduction in biofilm formation in the presence of EOs from Cinnamomum cassia and Melaleuca alternifolia against NG.12
Studies have shown that various bioactive phytochemicals exert antimicrobial activity by disrupting membrane integrity and cell wall stability, leading to increased ion permeability, enzyme inactivation, impaired proton translocation, and inhibition of ATP synthesis, ultimately resulting in bacterial cell death.10,37 Terpenoids, particularly monoterpenes like thymol and carvacrol, are known for their membrane-disrupting effects. It has been reported that Thymus vulgaris essential oil, alter membrane potential and increase permeability in E. coli, leading to cell lysis.38 The high percentage of Sesquiterpenes, including Copaene, Cyprene, Caryophyllene, and Aciphyllene, detected in the Nagarmotha, correlates with its significant antimicrobial properties. The antibacterial action of Nagarmotha is primarily attributed to its sesquiterpene-rich composition, which suggests that these compounds disrupt microbial cytoplasmic membranes, increasing permeability and allowing ions to pass through. This finding aligns with previous reports,30 further supporting the antimicrobial role of Cyperene. Additionally, Linalool (40.19%) and Terpinen-4-ol (22.11%) were identified as the dominant phytoconstituents in Sugandhmantri EO, suggesting their crucial role in enhancing antimicrobial efficacy.39,40 Although the exact mechanism of action of EOs against NG was not investigated in this study, the Terpenoid constituents are likely to contribute to the observed antibacterial potential, possibly through membrane associated interactions.
Nagarmotha and Sugandhmantri have been reported to exhibit significant antibacterial and antibiofilm effect against MDR-NG. Their potent antibacterial effects are likely due to the presence of bioactive terpenoids, which disrupt microbial membranes and inhibit biofilm formation. The significantly low MIC and MBC values observed suggest that these essential oils could serve as promising alternatives to conventional antibiotics. As antimicrobial resistance in NG is increasing at an alarming rate, the findings of this study highlight the positive leads in exploration of antiNG compounds for clinical applications.
Limitations
Although the present work provides valuable insights into the antibacterial and antibiofilm activities of selected EOs against MDR-NG, the study has some limitations. The findings are based solely on in vitro experiments, and in vivo or clinical validation was not performed. Additionally, the cytotoxicity and safety profiles of the tested essential oils were not evaluated. Therefore, further investigations involving in vivo studies and clinical validation are required to confirm their safety and therapeutic potential.
ACKNOWLEDGMENTS
The authors express their gratitude to Indira Gandhi National Tribal University, Amarkantak, India, for providing the laboratory facilities necessary for this research. Special thanks to Birsamunda Government Medical College, Shahdol, and the District Hospital Anuppur, Madhya Pradesh, India, for providing the clinical samples. The authors thank Dr. Mohammed Tausif Ur Rahman, Assistant Professor, Department of English & Foreign Languages, Indira Gandhi National Tribal University, Amarkantak, M.P., for English language editing of the manuscript.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
PS and RS conceptualized and supervised the study. NK and NKK prepared figures and performed data visualization. SKM performed experiments, data analysis, and wrote the manuscript. PS and RS critically reviewed and revised the manuscript. All authors read and approved the final manuscript for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, Indira Gandhi National Tribal University (Ref. No. IGNTU/IEC/2025/05A).
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- World Health Organization. Antimicrobial resistance. Geneva: WHO. 2023. Accessed January 10, 2026. https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance
- Tien V, Punjabi C, Holubar MK. Antimicrobial resistance in sexually transmitted infections. J Travel Med. 2020;27(1):taz101.
Crossref - Quillin SJ, Seifert HS. Neisseria gonorrhoeae host adaptation and pathogenesis. Nat Rev Microbiol. 2018;16(4):226-240.
Crossref - World Health Organization. Multi-drug resistant gonorrhoea. WHO 2025. Accessed January 10, 2026. https://www.who.int/news-room/fact-sheets/detail/Multi-drug-resistant- gonorrhoea
- Aitolo GL, Adeyemi OS, Afolabi BL, Owolabi AO. Neisseria gonorrhoeae antimicrobial resistance: past to present to future. Curr Microbiol. 2021;78(3):867-878.
Crossref - Unemo M, Shafer WM. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: past, evolution, and future. Clin Microbiol Rev. 2014;27(3):587-613.
Crossref - Alirol E, Wi TE, Bala M, et al. Multidrug-resistant gonorrhea: a research and development roadmap to discover new medicines. PLoS Med. 2017;14(7):e1002366.
Crossref - Mlynarczyk-Bonikowska B, Majewska A, Malejczyk M, Mlynarczyk G, Majewski S. Multiresistant Neisseria gonorrhoeae: a new threat in second decade of the XXI century. Med Microbiol Immunol. 2020;209(2):95-108.
Crossref - Alvarez-Martinez FJ, Barrajon-Catalán E, Herranz-Lopez M, Micol V. Antibacterial plant compounds, extracts, and essential oils: an updated review on their effects and putative mechanisms of action. Phytomedicine. 2021;90:153626.
Crossref - Caceres M, Hidalgo W, Stashenko E, Torres R, Ortiz C. Essential oils of aromatic plants with antibacterial, anti-biofilm and anti-quorum sensing activities against pathogenic bacteria. Antibiotics. 2020;9(4):147.
Crossref - Sagar PK, Sharma P, Singh R. Inhibition of quorum-sensing-regulated virulence factors and biofilm formation by Eucalyptus globulus against multidrug-resistant Pseudomonas aeruginosa. J Pharmacopuncture. 2022;25(1):37-45.
Crossref - Jurado P, Uruen C, Martinez S, et al. Essential oils of Pinus sylvestris, Citrus limon and Origanum vulgare exhibit high bactericidal and anti-biofilm activities against Neisseria gonorrhoeae and Streptococcus suis. Biomed Pharmacother. 2023;168:115703.
Crossref - Jain A, Katewa SS, Chaudhary BL, Galav P. Folk herbal medicines used in birth control and sexual diseases by tribals of southern Rajasthan, India. J Ethnopharmacol. 2004;90(1):171-177.
Crossref - Kamatenesi-Mugisha M, Oryem-Origa H, Odyek O, Makawiti DW. Medicinal plants used in the treatment of fungal and bacterial infections in and around Queen Elizabeth Biosphere Reserve, Western Uganda. Afr J Ecol. 2008;46:90-97.
Crossref - Peltzer K, Mngqundaniso N, Petros G. HIV/AIDS/STI/TB knowledge, beliefs and practices of traditional healers in KwaZulu-Natal, South Africa. AIDS Care. 2006;18(6):608-613.
Crossref - Vermani K, Garg S. Herbal medicines for sexually transmitted diseases and AIDS. J Ethnopharmacol. 2002;80(1):49-66.
Crossref - Juhi, Halwai V, Singh R, et al. Identification and antimicrobial susceptibility patterns of Neisseria gonorrhoeae, Ureaplasma spp., and Mycoplasma spp. isolated from tribal women. J Pure Appl Microbiol. 2024;18(3):1580-1592.
Crossref - Pan J, Singh A, Hanning K, Hicks J, Williamson A. A role for the ATP-dependent DNA ligase lig E of Neisseria gonorrhoeae in biofilm formation. BMC Microbiol. 2024;24(1):29.
Crossref - Bhargava VP, Netam AK, Singh R, Sharma P. Identification of phytochemicals of Cassia tora by GC-MS and correlation with reported pharmacological activities. Int J Biol Pharm Allied Sci. 2020;9(12):3302-3312.
Crossref - Burt SA, Reinders RD. Antibacterial activity of selected plant essential oils against Escherichia coli O157:H7. Lett Appl Microbiol. 2003;36(3):162-167.
Crossref - Chorianopoulos NG, Giaouris ED, Skandamis PN, Haroutounian SA, Nychas GJ. Disinfectant test against monoculture and mixed-culture biofilms composed of technological, spoilage and pathogenic bacteria: bactericidal effect of essential oil and hydrosol of Satureja thymbra and comparison with standard acid-base sanitizers. J Appl Microbiol. 2008;104(6):1586-1596.
Crossref - Swamy MK, Akhtar MS, Sinniah UR. Antimicrobial properties of plant essential oils against human pathogens and their mode of action: an updated review. Evid Based Complement Alternat Med. 2016;2016:3012462.
Crossref - Chomnawang MT, Trinapakul C, Gritsanapan W. In vitro antigonococcal activity of Coscinium fenestratum stem extract. J Ethnopharmacol. 2009;122(3):445-449.
Crossref - Jadhav N, Kulkarni S, Mane A, et al. Antimicrobial activity of plant extracts against sexually transmitted pathogens. Nat Prod Res. 2015;29(16):1562-1566.
Crossref - Arruda ALA, Vieira CJB, Sousa DG, Oliveira RF, Castilho RO. Jacaranda cuspidifolia Mart. (Bignoniaceae) as an Antibacterial Agent. J Med Food. 2011;14(12):1604-1608.
Crossref - Otto RB, Ameso S, Onegi B. Assessment of antibacterial activity of crude leaf and root extracts of Cassia alata against Neisseria gonorrhoeae. Afr Health Sci. 2014;14(4):840-848.
Crossref - Kambiz L, Afolayan AJ. Extracts from Aloe ferox and Withania somnifera inhibit Candida albicans and Neisseria gonorrhoeae. Afr J Biotechnol. 2008;7(1):012-015.
Crossref - Caceres A, Menendez H, Mendez E, et al. Antigonorrhoeal activity of plants used in Guatemala for the treatment of sexually transmitted diseases. J Ethnopharmacol. 1995;48(2):85-88.
Crossref - Rahman MS, Anwar MN. Antibacterial and cytotoxic activity of longiverbenone isolated from the rhizome of Cyperus scariosus. Bangladesh J Microbiol. 2008;25(1):82-84.
Crossref - Jha V, Patel R, Devkar S, et al. Essential oil and phytoconstituent (Linalool) from Homalomena aromatica Schott. rhizomes exhibit antibacterial and synergistic effects with beta-lactam antibiotics against Carbapenem-resistant Enterobacteriaceae (CRE) and Methicillin Resistant S. aureus (MRSA) pathogens. Chem Sci Int J. 2022;31(2):1-14.
Crossref - Mitra SD, Shailaja S, Harshitha N, Mitra J. Essential oil and phytoconstituent (Linalool) from Homalomena aromatica Schott. Rhizomes exhibit antibacterial and synergistic effects with beta-lactam antibiotics against Carbapenem-resistant Enterobacteriaceae and Methicillin-resistant Staphylococcus aureus pathogens. Ind Crops Prod. 2023;198:116666.
Crossref - Chouhan S, Sharma K, Guleria S. Antimicrobial activity of some essential oils present status and future perspectives. Medicines. 2017;4(3):58.
Crossref - Radaelli M, da Silva BP, Weidlich L, et al. Antimicrobial activities of six essential oils commonly used as condiments in Brazil against Clostridium perfringens. Braz J Microbiol. 2016;47(2):424-430.
Crossref - Burt S. Essential oils: their antibacterial properties and potential applications in foods–a review. Int J Food Microbiol. 2004;94(3):223-253.
Crossref - Greiner LL, Edwards JL, Shao J, Rabinak C, Entz D, Apicella MA. Biofilm formation by Neisseria gonorrhoeae. Infect Immun. 2005;73(4):1964-1970.
Crossref - Steichen CT, Shao JQ, Ketterer MR, Apicella MA. Gonococcal cervicitis: a role for biofilm in pathogenesis. J Infect Dis. 2008;198(12):1856-1861.
Crossref - Radulovic NS, Blagojevic PD, Stojanovic-Radic ZZ, Stojanovic NM. Antimicrobial plant metabolites: structural diversity and mechanism of action. Curr Med Chem. 2013;20(7):932-952.
Crossref - Xu J, Zhou F, Ji BP, Pei RS, Xu N. The antibacterial mechanism of carvacrol and thymol against Escherichia coli. Lett Appl Microbiol. 2008;47(3):174-179.
Crossref - Guimaraes AC, Meireles LM, Lemos MF, et al. Antibacterial activity of terpenes and terpenoids present in essential oils. Molecules. 2019;24(13):2471.
Crossref - Guo F, Chen Q, Liang Q, et al. Antimicrobial activity and proposed action mechanism of linalool against Pseudomonas fluorescens. Front Microbiol. 2021;12:562094.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.