


Monkeypox (MPX) is a double-stranded DNA virus belonging to the Poxviridae family. It can be transmitted through direct contact with infected skin lesions, body fluids, air droplets, sexual contact, and/or contaminated fomites. MPX has a broad range of clinical findings and complications, ranging from mild symptoms to severe fatal complications. To elucidate MPX and its possible resurgence. This review discusses the epidemiology, clinical findings, diagnosis, prevention, and future challenges associated with MPX. A resurgence of MPX has been reported in many non-endemic countries that do not have any relation to the importation of animals or travel. Many transformations occur in MPX, resulting in its ability to infect and spread among humans. Based on its very high rates of spread and variable findings, great caution should be taken worldwide to gauge the next resurgence.
Monkeypox, Epidemiology, Clinical Manifestations, Diagnosis, Future Challenges
MPX (Monkeypox) is a highly infectious disease caused by the monkeypox virus (MPXV), and is primarily transmitted by rodents.1 MPXV is a member of the Orthopoxvirus genus.2 Historically confined to Africa with only animal-to-human spread, a substantial global outbreak occurred in 2022, driven by human transmission outside the continent.3
MPXV, like other orthopoxviruses, is a large oval or brick-shaped virus encased in a corrugated membrane of lipoproteins. Their size generally measures approximately 200-250 nm. This outer layer shields the dense core of double-stranded DNA (dsDNA), enzymes, and transcription factors. The core is biconcave because of fixation artefacts and includes lateral bodies (Figure).3 The central part of the viral genome is highly conserved and contains housing genes, whereas the left and right ends of the genome exhibit greater variability and contain accessory genes that substantially influence virus-host interactions.1
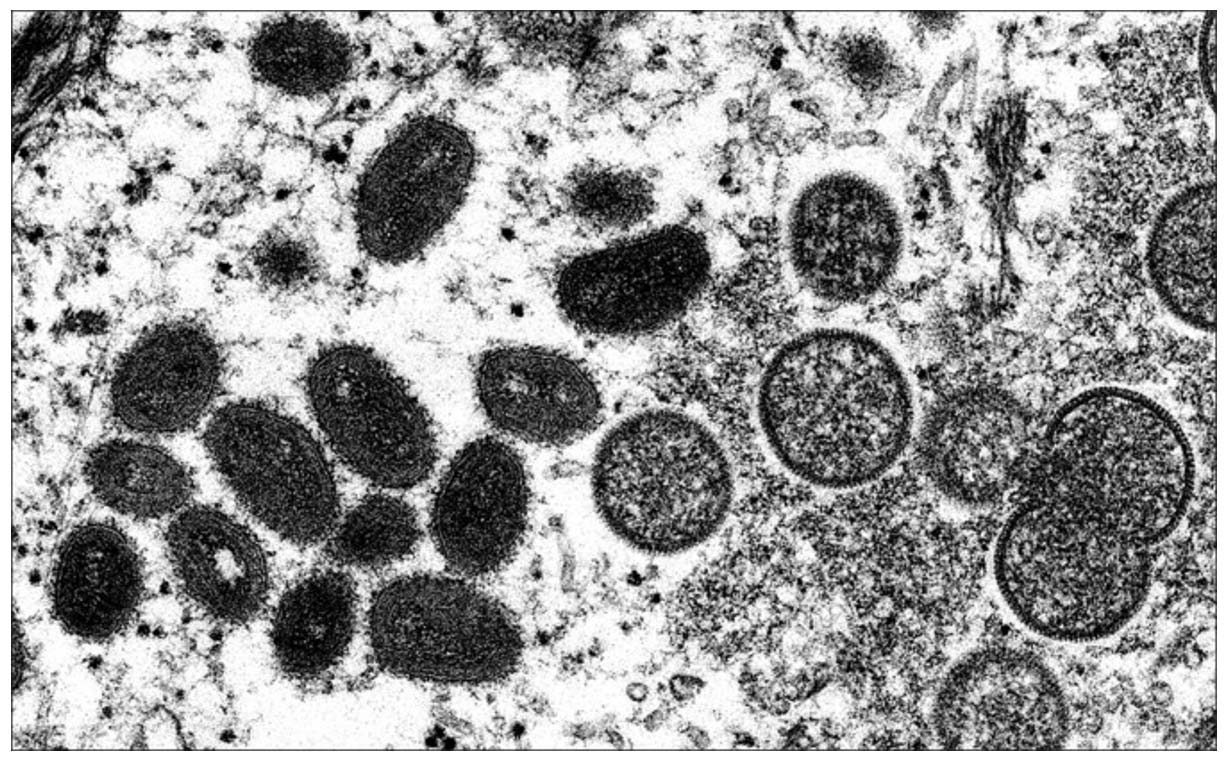
Figure. Electron microscopic (EM) image of Monkeypox particles. Left side shows oval-shaped mature viral particles, and the right side shows crescents and spherical immature virions. (Source: CDC/IMAGE POINT FR/BSIP/Universal Images Group via Getty Images)
There are three monkeypox clades: Clade I (Congo Basin, high mortality, primarily zoonoses), Clade IIa (West Africa, low mortality, primarily zoonoses), and Clade IIb (current global outbreak, low mortality, efficient human-to-human spread).3
Epidemiology
MPXV was first identified in monkeys in 1959, and the first human infection was recorded in 1970 in the Republic of Congo. The patient was diagnosed at nine months when admitted to the hospital.4 This recent surge may be linked to decreased immunity because of the cessation of smallpox vaccinations, which offer substantial protection.5
In 2022, MPXVs were declared to have diverged from the 2018-2019 viruses by approximately 50 single-nucleotide polymorphisms (SNPs).5 These genetic mutations enable the transmission of MPXV from monkeys to humans and between humans.1 The inverted terminal repeats at the ends of the viral genome are highly variable and influence host range and virulence. These mutations enhance viral transmissibility, virulence, and immune evasion.6
In January 2023, several confirmed cases and deaths were reported globally, with the United States having the highest number of cases. Global risk is considered moderate by the WHO, with cases peaking in August 2022 and then stabilising.6 The presence of MPX has been confirmed in the Middle East; however, cases are much less common than those in Europe and the Americas.7
MPXV spreads through contact with infected animals and humans, respiratory droplets, and contaminated objects. Transmission from animals to humans can occur through direct contact with aerosols or contaminated surfaces.5
Pathogenesis
Virulence genes directly affect the disease-causing abilities of orthopoxviruses. All share immunological cross-reactivity, indicating that infection with one can protect from infection with others. The genome includes genes encoding TIR-containing proteins, such as VACV A46 and A52, which inhibit NF-κB, a key factor in innate immunity. MPXV lacks A52 analogues.8
Orthopoxviruses also encode ankyrin repeat (ANK) proteins, which are involved in regulating NF-κB activation. This transcription factor, controlled by IκB family proteins containing ANK repeats, plays a pivotal role in governing genes linked to processes such as apoptosis, inflammation, immune responses, and cell proliferation. As a result, NF-κB is central to antiviral signalling and the initiation of inflammatory pathways. In the MPXV, eight genes are associated with these functions.9 Interestingly, the Poxviridae family is unique among the viruses that possess Kelch-like protein genes. For instance, the MPXV carries a single gene encoding the BTB-Kelch protein that influences the species-specific characteristics of orthopoxviruses during infection.9 Orthopoxviruses encode at least seven genes that inhibit apoptosis, each employing a distinct mechanism. Despite producing substantial amounts of double-stranded RNA (dsRNA), a molecule that typically triggers interferon (IFN) responses, during the later stages of their replication cycle, these viruses exhibit remarkable resistance to IFN. However, the MPXV lacks a functional IFN resistance factor due to the presence of various mutations in the corresponding gene. This unique genetic configuration likely reduces its ability to propagate efficiently in vivo and diminishes its capacity for airborne transmission compared to other orthopoxviruses such as the smallpox virus.9 Recently, it was reported that the VACV-COP protein A35 of the MPXV inhibits MHC class II antigen presentation, priming the immune response and subsequent cytokine and chemokine synthesis. This can lead to serious disease.10
The resurgence of MPX epidemics over the last three decades may be linked to various factors, such as weakened immunity (especially HIV infection), young age (especially younger than eight years), pregnancy, and certain skin conditions (eczema).11 MPX can coexist with other sexually transmitted infections.12 The decline in smallpox vaccinations has likely contributed to the increased number of cases.5
While other DNA viruses replicate in the nucleus, MPXVs replicate in the cytoplasm of host cells. Proteins, such as D8L, A27L, A34R, A26L, and H3L, are vital for cell binding.5
Clinical manifestations and complications
MPX viral infection progresses through incubation, prodromal, rash, and crusting stages.11 Some patients remain asymptomatic, while others complain of rashes and non-inflammatory joint pain.12 Following the MPX viral entrance into the respiratory mucosa, there are two phases:
1) A prodromal phase with non-specific symptoms (fever, headache, myalgia, backache, lymphadenopathy) for up to 5 days; and
2) A rash phase that starts 1-3 days after the fever.11 Vesiculopustular rashes are very painful and start in the face, anal, or genital regions, and then spread centrifugally to involve the trunk, hands, legs, and feet.12 The exanthematous rash usually begins as macular, then progresses to papular, vesicular, and pustular stages.
Complications of MPXV infection may include corneal infection (which can lead to corneal scarring and visual impairment), dehydration,11 conjunctivitis, periorbital edema.12 myalgia, seizures, encephalitis, superadded bacterial infection causing bronchopneumonia,12 sepsis, and acute respiratory distress syndrome.11,13
Diagnosis
Laboratory diagnosis of MPXV is done via the detection of anti-MPXV IgM or a marked increase in anti-MPXV IgG levels in two subsequent samples (10-14 days apart), molecular typing, detection of viral cytopathic effects, immunohistochemistry, electron microscopy, viral cell culture, and sequencing.14
The recommended specimens for laboratory confirmation of MPXV are swabs, lesion crusts, and/or blood samples. However, blood samples are unsuitable for PCR diagnosis because of the short duration of viremia.11
The main cytopathic modifications include a ground glass appearance of the keratinocyte nuclei, cell ballooning, and Guarnieri bodies.14 Neutrophilic infiltration indicates the MPX pustular stage.15
Prevention
To prevent and limit the spread of MPX, it is crucial to avoid close skin-to-skin contact with infected persons and/or contaminated objects, wash hands regularly, and follow infection prevention and control practices.16 Early identification and isolation of patients are necessary because MPXV can be transmitted rapidly by droplets, aerosols, and/or direct contact.12
There is no specific vaccine to prevent MPXV infection; however, the smallpox vaccine provides 85% cross-protection against MPXV infection. The Food and Drug Administration (FDA) has approved multiple vaccines, including Imvamune (Imvanex, MVA-BN, JYNNEOS), ACAM2000 (live-attenuated vaccine), and the Aventis Pasteur Smallpox Vaccine (APSV).6 Smallpox vaccination effectively protected humans from MPXV and other poxviruses.6 The vaccinia virus vaccine was administered by puncturing the skin multiple times with a bifurcated needle containing vaccinia virus. In case of success, a pustule or primary lesion (take) appears at the site of vaccination.17 In Japan, LC16m8 (LC16 KMB) exhibited long-lasting protection against the MPXV as well as broad T cell responses in a phase I/II clinical trial.16 In Russia, VACdelta6 (VACΔ6) is used, a non-adjuvanted smallpox vaccine with the deletion of six virulence genes.17 Some clinical trials in animals showed that BNT166, a multivalent mRNA vaccine encoding MPXV antigens A35, B6, M1, H3, and protects from VACV, Clade I and IIb MPXV, and NHPs from Clade I MPXV, and is 100% effective in preventing mortality.18
Vaccinia immunoglobulin is a hyperimmune globulin approved by the FDA for reducing the adverse effects of vaccinia virus vaccination, but its efficacy has not been proven for MPXV.6
Treatment
Treating monkeypox focuses on supportive care, symptomatic treatment (most importantly hydration and antipyretics), and preventing and treating complications, more specifically secondary bacterial infections. Multiple listed antiviral drugs are effective but non-specific for monkeypox and are recommended for monkeypox virus-infected individuals suffering from severe disease or at risk of developing serious illness.16 These antivirals include Cidofovir, a modified cytosine, which blocks the template strand extension and the 3′-to-5′ exonuclease proofreading activity of the viral DNA polymerase.17 Brincidofovir (CMX001, Tembexa®) inhibits DNA polymerase activity and suppresses viral DNA synthesis. Tecovirimat stops the virus protein VP37 and inhibits the release of intracellular mature viruses (IMVs). It was used in the MPX outbreak in 2022 and achieved a survival rate of greater than 90%.16 ST-357 inhibits the viral poly-A polymerase and could be considered a second-line drug.17
Future challenges
Since the discovery of MPXV in 1970, outbreaks have been confined to endemic countries, particularly in Africa. However, the number of outbreaks has increased over time, exceeding 35, and has been reported in non-endemic countries.19,20
Recently, many cases have emerged in different regions of the world, including the United Kingdom, Europe, the United States, and the Middle East. In 2022, outbreaks of MPXV infection in approximately 86 countries that were non-endemic and/or did not have any epidemiological links to travel or the importation of mammals were reported. Although MPX is not a severe disease, a mortality rate of 8.7% has been reported.21
The main limitations of the current study are the lack of a formal systematic search or meta-analysis, the scarcity of region-specific studies, and underreporting in some countries. These limitations may limit the comprehensiveness of this study.
MPXV can undergo several mutations that enable its resurgence and can cause epidemics. There are multiple modes of transmission for MPXV (including direct contact with infected skin lesions, body fluids, air droplets, sexual contact, and/or contaminated fomites), clinical findings, and complications. There are many challenges, and countries should prepare healthcare programs to guard against any suspected epidemics and avoid crises such as those that occurred with COVID-19.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
Not applicable.
ETHICS STATEMENT
Not applicable.
- Young B, Seifert SN, Lawson C, Koehler H. Exploring the genomic basis of MPX virus-host transmission and pathogenesis. mSphere. 2024;9(12):e00576-24.
Crossref - Isidro J, Borges V, Pinto M, et al. Phylogenomic characterization and signs of microevolution in the 2022 multi-country outbreak of monkeypox virus. Nat Med. 2022;28(8):1569-1572.
Crossref - Americo JL, Earl PL, Moss B. Virulence differences of MPX (monkeypox) virus clades I, IIa, and IIb.1 in a small animal model. Proc Natl Acad Sci U S A. 2023;120(8):e2220415120.
Crossref - Alakunle E, Moens U, Nchinda G, Okeke MI. Monkeypox Virus in Nigeria: Infection Biology, Epidemiology, and Evolution. Viruses. 2020;12(11):1257.
Crossref - Halder SK, Sultana A, Himel MK, Shil A. Monkeypox: Origin, Transmission, Clinical Manifestations, Prevention, and Therapeutic Options. Interdiscip Perspect Infect Dis. 2025;2025:2522741.
Crossref - Karagoz A, Tombuloglu H, Alsaeed M, et al. Monkeypox (MPX) virus: Classification, origin, transmission, genome organization, antiviral drugs, and molecular diagnosis. J Infect Public Health. 2023;16(4):531-541.
Crossref - Ahmed SK, Omar RM, Hussein SH, et al. Middle East countries preparedness for Monkeypox outbreak: A call to action. Int J Surg Lond Engl. 2022;106:106948.
Crossref - Burki T. Investigating monkeypox. Lancet Lond Engl. 2022;399(10343):2254–2255.
Crossref - Shchelkunov SN. Orthopoxvirus Genes That Mediate Disease Virulence and Host Tropism. Adv Virol. 2012;2012:524743.
Crossref - Hatmal MM, Al-Hatamleh MAI, Olaimat AN, et al. Comprehensive literature review of monkeypox. Emerg Microbes Infect. 2025;11(1):2600-2631.
Crossref - Al-Dabbagh J, Mohammad Deeb E, Younis R, Eissa R. The dermatological manifestations and differential diagnosis of monkeypox: A narrative review. Medicine. 2024;103(44):e40359.
Crossref - Abaza H, Agadi K, Anand A, Elsaid M. Clinical Manifestations of Monkeypox. In: Turksen, K. (eds) Cell Biology and Translational Medicine, Volume 19. Advances in Experimental Medicine and Biology, vol 1410. Springer, Cham. 2022:7:11.
Crossref - Adelino TER, Santos SC, Lima MT, et al. Differential diagnosis of exanthematous viruses during the 2022 MPX outbreak in Minas Gerais, Brazil. J Clin Microbiol. 2025;62(6):e00103-24.
Crossref - Sun Y, Nie W, Tian D, Ye Q. Human monkeypox virus: Epidemiologic review and research progress in diagnosis and treatment. J Clin Virol. 2024;171:105662.
Crossref - Moltrasio C, Boggio FL, Romagnuolo M, et al. Monkeypox: A Histopathological and Transmission Electron Microscopy Study. Microorganisms. 2023;11(7):1781.
Crossref - Huang Y, Mu L, Wang W. Monkeypox: epidemiology, pathogenesis, treatment and prevention. Signal Transduct Target Ther. 2022;7:373.
Crossref - Saalbach KP. Treatment and Vaccination for Smallpox and Monkeypox. In: Rezaei, N. (eds) Poxviruses. Advances in Experimental Medicine and Biology, vol 1451. Springer, Cham.
Crossref - Zuiani A, Dulberger CL, Silva NSD, et al. A multivalent mRNA monkeypox virus vaccine (BNT166) protects mice and macaques from orthopoxvirus disease. Cell. 2024;187(6):1363-1373.e12.
Crossref - Kraemer MUG, Tegally H, Pigott DM, et al. Tracking the 2022 monkeypox outbreak with epidemiological data in real-time. Lancet Infect Dis. 2022;22(7):941-942.
Crossref - Farahat RA, Ali I, Ahdal TA, et al. Monkeypox and human transmission: Are we on the verge of another pandemic? Travel Med Infect Dis. 2022;49:102387.
Crossref - Farahat RA, Umar TP, Khan SH, et al. Preparedness of Eastern Mediterranean countries in view of monkeypox emergence during the COVID-19 pandemic: A call for action. Int J Surg. 2022;105:106878.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.