


ISSN: 0973-7510
E-ISSN: 2581-690X
Multidrug-resistant (MDR) Acinetobacter is an important pathogen which has a number of virulence characters that enable them to render resistance to antibiotics thus complicating the treatment options, thereby forcing clinicians to rely on last resort antibiotic such as colistin. However, resistance to colistin has also been reported, further increasing the challenge. To detect the rate of colistin resistance and carbapenemase production among MDR Acinetobacter baumannii isolates from a tertiary care hospital in South India. This is a prospective study conducted over a period of 15 months from August 2023 to October 2024 and included 110 isolates of MDR Acinetobacter baumannii. All the isolates were subjected to colistin resistance detection using microbroth dilution method and carbapenemase production using mCIM and eCIM methods. Of the 110 isolates of MDR A. baumannii, 19 (17.27%) showed colistin resistance. The mCIM and eCIM tests showed 70 (63.63%) serine carbapenemase producers and 61 (55.45%) metallo beta-lactamase producers. This study underscores the concerning prevalence of resistance determinants among MDR A. baumannii, providing clinicians and infection control specialists with essential data to guide the formulation of effective empirical treatment strategies and infection control measures.
Multidrug-resistance, Acinetobacter, Carbapenemase, Colistin, Antimicrobial Resistance
Acinetobacter is a Gram-negative, non-motile, aerobic coccobacillus causing bloodstream, skin, soft tissue, wound infections, and ventilator-associated pneumonia (VAP), particularly in ICU patients.1 Multidrug-resistant A. baumannii (MDRAB) has acquired resistance to most antibiotics, including carbapenems, the preferred treatment for severe infections.2,3 However, rising carbapenem-resistant A. baumannii (CRAB) rates have reduced treatment efficacy and increased mortality. Resistance is often mediated by oxacillinases (OXA-23-like, OXA-24-like, OXA-58-like) and the intrinsic blaOXA-51-like gene, which requires insertion sequences for carbapenem resistance. Other mechanisms include carbapenem-hydrolyzing β-lactamases and extended-spectrum β-lactamases (ESBLs).4,5
Phenotypic assays such as the modified carbapenem inactivation method (mCIM) and EDTA-modified carbapenem inactivation method (eCIM), recommended by CLSI, differentiate serine β-lactamases from metallo-β-lactamases, aiding in targeted antibiotic therapy and infection control.4
The global spread of CRAB has renewed reliance on polymyxins, especially colistin, as a “last-resort” antibiotic. However, colistin resistance is increasing.5 Colistin acts by binding the negatively charged lipid A in lipopolysaccharides via electrostatic interactions. Resistance can result from mutations in pmrCAB (encoding the PmrA response regulator, PmrB kinase sensor, and PmrC LPS-modifying protein) and lpxA, lpxC, lpxD (lipid A biosynthesis), or via plasmid-mediated mcr genes (mcr-1 to mcr-5) encoding phosphoethanolamine transferases. These genetic changes alter LPS structure, reducing colistin binding and rendering treatment ineffective.6,7
Therefore this study aims to assess the phenotypic characterization of colistin resistance and carbapenemase production in Acinetobacter baumannii from both clinical and environmental sources which is essential to gain insights into the organism’s pathogenic potential and its ability to persist and spread within healthcare settings.
This is a prospective study conducted in a tertiary care hospital in South India. This study was approved by the Institutional Ethics Committee, JSS Medical College and Hospital, Mysuru, Karnataka, India (JSS|MC |PG|0040|2022-2023) Dated 05-04-2023. Written informed consent was obtained from the participants before enrolling in the study. Clinical and environmental MDR Acinetobacter baumannii were collected for over a 15 month period, from August 2023 to October 2024. Samples such as sputum, endotracheal aspirates, pus, blood, urine, and other body fluids were processed according to established standard protocols.
Multidrug-resistant A. baumannii isolates were identified using the VITEK 2 system (BioMerieux, India), in accordance with the manufacturer’s guidelines.8
The study included 55 clinical MDR A. baumannii isolates along with 55 corresponding environmental isolates.
Patient’s surroundings from whom MDR Acinetobacter were isolated clinically, were screened for the presence of MDR Acinetobacter spp. From each patient 5 environmental samples (Wall, trolley, floor, bathroom, bed and bed rails) were obtained. MDR Acinetobacter isolated from all or any one patient’s environmental site was considered.
All the isolates were subjected to colistin resistance detection using microbroth dilution method. Using the MIKROLATEST kit (LOT: 1710152) and CLSI 2023 guidelines with the proper controls (ATCC Ps. aeruginosa 27853 and ATCC E. coli 25922), the broth microdilution method was carried out.9
Carbapenemase detection
mCIM (Modified Carbapenem Inactivation Method)
For each isolate, 1 µL loopful of test organism from an overnight blood agar culture was emulsified in 2 mL tryptic soy broth (TSB). A 10 µg meropenem disc was added and vortexed for 10-15 sec, later incubated at 35 °C ± 2 °C for 4 hrs 15 min. A 0.5 McFarland suspension of E. coli ATCC® 25922 was prepared in saline or broth, inoculated onto Mueller–Hinton agar (MHA), and allowed to dry. The disc was then transfered from the TSB to the MHA, then incubated for 18-24 hrs at 35 °C ± 2 °C and measured for the inhibition zone (a positive result indicating a carbapenemase enzyme is present when the inhibition zone diameter around the meropenem disk is 6-15 mm, or 16-18 mm with pinpoint colonies within the zone. A negative result shows a zone of 19 mm or larger, meaning no carbapenemase was detected. If the zone is 16-18 mm without pinpoint colonies, or 19 mm or larger with pinpoint colonies, the result is considered indeterminate and requires further testing).10
eCIM (EDTA-Modified Carbapenem Inactivation Method)
To reach a final concentration of 5 mM, a second 2 mL TSB tube was labelled and 20 µL of 0.5 M EDTA was added. Proceeded further as per the mCIM protocol, processing the two tubes simultaneously and putting the meropenem discs from the mCIM and eCIM on the same MHA was followed.10
mCIM and eCIM result interpretation
eCIM Results (to be interpreted only if mCIM is positive):
- Metallo-β-lactamase positive: The zone diameter increases by ≥5 mm in comparison to the mCIM, indicating the presence of metallo-β-lactamase. The inhibition of E. coli ATCC® 25922 is a result of EDTA’s suppression of the enzyme’s activity.
- Metallo-β-lactamase negative: The activity of the enzyme is not significantly affected by EDTA, and an increase of ≤4 mm in the zone diameter relative to the mCIM indicates the presence of a serine carbapenemase.10
Reporting of mCIM and eCIM
- For carbapenemase-positive isolates, report as “Carbapenemase positive”, including the zone diameter and any pinpoint colonies.
- For carbapenemase-negative isolates, report as “Carbapenemase negative”, with the clear zone diameter.
- For inconclusive results, report as “Carbapenemase inconclusive” and recommend additional testing.
- For eCIM, if metallo-β-lactamase positive, report as “Metallo-β-lactamase positive” with the zone diameters for both mCIM and eCIM. If metallo-β-lactamase negative, report as “Metallo-β-lactamase negative”, with the zone diameters for both tests.10
A total of 110 multidrug-resistant (MDR) Acinetobacter baumannii isolates were analysed, comprising 55 clinical and 55 corresponding patient environmental isolates.
All clinical isolates were intermediate to colistin, 41 (78.18%) isolates were sensitive to tigecycline, 10 (18.18%) isolates were sensitive to minocycline, and the majority exhibited resistance to carbapenems, fluoroquinolones, aminoglycosides, and cephalosporins by VITEK 2 method (Table 1).
Table (1): Antimicrobial susceptibility testing of 55 clinical MDR A. baumannii
DRUG |
Sensitive No. |
% |
Intermediate No. |
% |
Resistant No. |
% |
|---|---|---|---|---|---|---|
Colistin |
12 |
21.82 |
43 |
78.18 |
0 |
0.00 |
Tigecycline |
43 |
78.18 |
11 |
20.00 |
1 |
1.82 |
Minocycline |
10 |
18.18 |
6 |
10.91 |
39 |
70.91 |
Gentamycin |
6 |
10.91 |
2 |
3.64 |
47 |
85.45 |
Ceferazone/Sulbactam |
4 |
7.27 |
0 |
0.00 |
51 |
92.73 |
Amikacin |
0 |
0.00 |
1 |
1.82 |
54 |
98.18 |
Cefepime |
0 |
0.00 |
3 |
5.45 |
52 |
94.55 |
Levoflaxacin |
1 |
1.82 |
1 |
1.82 |
53 |
96.36 |
Cotrimoxazole |
2 |
3.64 |
0 |
0.00 |
53 |
96.36 |
Piperacillin/Tazobactam |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Ceftazidime |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Ceftriaxone |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Imipenem |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Meropenem |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Ciprofloxazin |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Carbapenemase detection by mCIM and eCIM showed that, among the 55 clinical isolates, 40 (72.27%) produced serine carbapenemases and 36 (65.45%) produced metallo-β-lactamases (Table 2) (Figure 1).
Table (2): Antimicrobial susceptibility testing of 55 environmental MDR A. baumannii
DRUG |
Sensitive No. |
% |
Intermediate No. |
% |
Resistant No. |
% |
|---|---|---|---|---|---|---|
Colistin |
18 |
32.72 |
37 |
67.27 |
0 |
0 |
Tigecycline |
26 |
47.27 |
22 |
40.00 |
7 |
12.73 |
Minocycline |
11 |
20.00 |
0 |
0.00 |
44 |
80.00 |
Gentamycin |
6 |
10.91 |
4 |
7.27 |
45 |
81.82 |
Ceferazone/Sulbactam |
8 |
14.55 |
4 |
7.27 |
43 |
78.18 |
Amikacin |
0 |
0.00 |
8 |
14.55 |
47 |
85.45 |
Cefepime |
0 |
0.00 |
9 |
16.36 |
46 |
83.64 |
Levoflaxacin |
0 |
0.00 |
8 |
14.55 |
47 |
85.45 |
Cotrimoxazole |
1 |
1.82 |
0 |
0.00 |
54 |
98.18 |
Piperacillin/Tazobactam |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Ceftazidime |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Ceftriaxone |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Imipenem |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Meropenem |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Ciprofloxazin |
0 |
0.00 |
0 |
0.00 |
55 |
100.00 |
Colistin susceptibility testing by the microbroth dilution method revealed that 43 (78.19%) of the clinical MDR A. baumannii isolates were sensitive, while 12 (21.81%) were resistant (Figure 2).
Among the 12 colistin resistant clinical isolates, majority of the colistin resistant isolates were from male individuals 8 and 4 isolates from female individuals. Majority of the isolates were isolated from in-patients 11 with only one from out-patient sample. Majority of the colistin resistant isolates were from ICU (Intensive care unit) with 9 isolates and MICU being the predominant with 4 isolates (Table 3). Two isolates were from wards (one from general male ward and one from private ward) (Table 3). Majority of the colistin resistant isolates were from endotracheal aspirate samples 9 with one urine, sputum and pus samples each respectively (Table 4). Colistin resistant isolates were isolated from only two age groups i.e. 41-60 years with 6 isolates followed by age group 61-80 years with 6 isolates (Table 5). Majority of the colistin resistant isolates were isolated from patients suffering from LRTI (Lower respiratory tract infections) with 4 isolates (Table 6).
Table (3): Carbapenemase production in 55 clinical and 55 environmental MDR A. baumannii
| Tests | Clinical | Environmental | ||
|---|---|---|---|---|
| mCIM No. (%) | eCIM No. (%) | mCIM No. (%) | eCIM No. (%) | |
| Positive | 40 (72.72%) | 36 (65.45%) | 30 (54.54%) | 25 (45.45%) |
| Negative | 15 (27.27%) | 19 (34.54%) | 25 (45.45%) | 30 (54.54%) |
Table (4): ICU and Ward distribution of 11 colistin resistant clinical MDR A. baumannii
ICU |
Total no. (%) |
|---|---|
Respiratory ICU |
1 (9.09%) |
Critical Care Medicine ICU |
2 (18.18%) |
Medicine ICU |
4 (36.36%) |
Neuro ICU |
2 (18.18%) |
Total of ICU |
9 |
Private ward |
1 (9.09%) |
General Medicine- male ward |
1 (9.09%) |
Total of ward |
2 |
Out-patient department |
1 |
Grand Total |
12 |
Table (5): Sample distribution of 12 colistin resistant clinical MDR A. baumannii
Sample |
Total no. (%) |
|---|---|
Pus |
1 (8.33%) |
Endotracheal aspirate |
9 (75%) |
Sputum |
1 (8.33%) |
Urine |
1 (8.33%) |
Grand total |
12 |
Table (6): Age distribution of 12 colistin resistant clinical MDR A. baumannii
Age distribution |
Total no. (%) |
|---|---|
41-60 years |
6 (50%) |
61-80 years |
6 (50%) |
Grand total |
12 |
Among the 55 MDR A. baumannii environmental isolates, all the isolates showed intermediate susceptibility to colistin, 26 (47.27%) were susceptible to tigecycline, and 7 (20%) to minocycline and the majority exhibited resistance to carbapenems, fluoroquinolones, aminoglycosides, and cephalosporins by VITEK 2 method (Table 7).
Table (7): Diagnosis distribution of 12 colistin resistant clinical MDR A. baumannii
Diagnosis |
Total no. (%) |
|---|---|
Chronic kidney disease |
2 (16.67%) |
Lower respiratory tract infection |
4 (33.33%) |
Diabetes mellitus |
1 (8.33%) |
Chronic Obstructive Pulmonary Disease |
1 (8.33%) |
Traumatic Brain Injury |
2 (16.67%) |
Urinary tract infection |
1 (8.33%) |
IC Bleed |
1 (8.33%) |
Grand Total |
12 |
Carbapenemase detection by mCIM and eCIM showed that, among environmental isolates, 30 (54.5%) were positive for serine carbapenemase production and 25 (45.5%) for metallo-β-lactamase production (Table 3) (Figure 1).
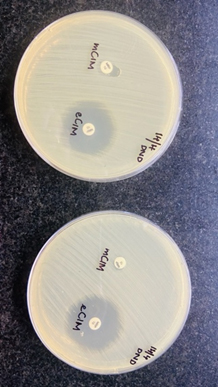
Figure 1. Carbapenemase production by mCIM and eCIM method
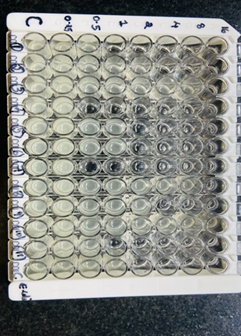
Figure 2. Colistin susceptibility testing by microbroth dilution
Colistin susceptibility testing by the microbroth dilution method revealed that 48 (87.28%) of the environmental isolates were sensitive, 7 (12.72%) isolates were resistant
(Figure 2). Among the 7 environmental colistin resistant isolates, 3 isolates were from floor, 2 isolates from wall, one isolate each from the bathroom and the bed sample.
The present prospective study demonstrates a substantial burden of multidrug-resistant (MDR) Acinetobacter baumannii in both clinical and the patient environment of a tertiary care hospital in South India. The findings align with the evidence that identifies A. baumannii as a highly adaptable nosocomial pathogen, particularly in intensive care settings and capable of persisting in hospital environments while exhibiting both extensive antimicrobial resistance and significant virulence potential.
Demographic analysis in the present study revealed a clear male predominance, with a male-to-female ratio of 3:1 and 67.27% of infections occurring in male patients. This finding is consistent with Huang et al.,11 who reported a ratio of 3.9:1, and is supported by more recent studies showing higher infection rates among males.12,13 The increased susceptibility among males has been attributed to immunological differences, higher prevalence of comorbidities, smoking habits, and greater exposure to invasive procedures.
Age-wise distribution showed the highest prevalence among patients aged 61-80 years, followed by 41-60 years. Similar trends have been reported by Yadav et al.,14 Zhang et al.,15 and Mohanty et al.16 identifying elderly individuals as particularly vulnerable due to immune senescence, prolonged hospitalization, multiple comorbidities, and repeated exposure to broad-spectrum antibiotics.
A substantial majority of clinical isolates (82.35%) were obtained from ICU patients, reinforcing the role of ICUs as epicentres for MDR A. baumannii. This observation aligns with Khoshnood et al.17 Yadav et al.14 and more recent studies reporting ICU-associated prevalence ranging from 55% to over 80%.18,19 Endotracheal aspirates were the predominant specimen type (63.63%), reflecting the strong association of MDR A. baumannii with ventilator-associated pneumonia, as consistently reported in post-2018 studies.20,21
Environmental surveillance demonstrated that most MDR A. baumannii isolates were recovered from beds and bed rails, highlighting the role of high-touch surfaces in pathogen persistence. This finding corroborates reports by Boulesnam et al. and more recent studies by Weber et al.,22 Suleyman et al.,23 and Cruz-Lopez et al.,24 which identified patient surroundings as critical reservoirs facilitating indirect transmission through healthcare workers and contaminated equipment. Although molecular typing was not performed in this study, the phenotypic similarity between clinical and environmental isolates strongly suggests ongoing environmental-to-patient transmission.
In this study, phenotypic detection of virulence markers revealed that clinical MDR A. baumannii isolates expressed stronger virulence traits than corresponding environmental isolates. This observation is consistent with several recent studies reporting enhanced expression of virulence determinants such as biofilm formation, serum resistance, and motility among clinical isolates, attributed to host adaptation and selective pressures within the human body.25,26 Although environmental isolates demonstrated comparatively weaker virulence phenotypes, they remain clinically significant as reservoirs capable of acquiring and disseminating virulence and resistance determinants, as highlighted by Costa et al.27 This dual presence of resistance and virulence underscores the threat posed by A. baumannii in hospital ecosystems.
Colistin resistance among clinical isolates in the present study was 21.81%, while 12.72% of environmental isolates were resistant. These rates exceed many pre-2018 reports but are comparable to post-2018 studies documenting a gradual yet consistent rise in colistin resistance, particularly in Asia. Sharma et al.28 and Pragasam et al.29 reported increasing colistin resistance in Indian tertiary-care hospitals, predominantly among ICU isolates. Novovic et al.30 further emphasized the growing role of chromosomal mutations affecting lipid A biosynthesis and regulatory pathways, leading to both resistance and heteroresistance. The predominance of colistin-resistant isolates in ICU patients and endotracheal aspirate samples in this study is in agreement with findings by Paul et al.31 and Joshi et al.32 who identified prolonged ICU stay, mechanical ventilation, and prior exposure to last-line antibiotics as major risk factors.
Carbapenem resistance in A. baumannii was highly prevalent in the present study and was largely mediated by carbapenemase production. A high proportion of clinical isolates produced serine carbapenemases (72.27%) and metallo-β-lactamases (65.45%). Similar trends have been reported consistently between 2018 and 2025, with widespread dissemination of OXA-type serine carbapenemases, particularly blaOXA-23-like genes.33,34 The increasing detection of NDM-type MBLs reported by Nordmann and Poirel35 and Veeraraghavan et al.36 further supports our findings. The coexistence of serine carbapenemases and MBL activity, as observed in this study, has been increasingly documented in post-2018 literature and represents a serious therapeutic challenge due to extreme drug resistance.37
Tigecycline retained relatively good in-vitro activity against clinical isolates in this study (78.18% susceptibility), though susceptibility was lower among environmental isolates. Comparable findings have been reported between 2018 and 2023, where tigecycline remained one of the few active agents against MDR A. baumannii, albeit with emerging resistance.38,39 Minocycline susceptibility was comparatively low, aligning with recent studies suggesting declining efficacy due to increased clinical usage and selective pressure.40 These observations reinforce the importance of local antibiograms and continuous resistance surveillance, as emphasized in global reviews.41
Overall, when compared with recent studies, the present findings are consistent with the global trend of escalating carbapenem and colistin resistance in A. baumannii, accompanied by enhanced virulence in clinical isolates and persistent environmental contamination. The convergence of antimicrobial resistance, virulence potential, ICU predominance, and environmental persistence underscores the urgent need for stringent infection control practices, targeted environmental cleaning of high-touch surfaces, routine surveillance of both resistance and virulence traits, antimicrobial stewardship, and integration of molecular epidemiological tools to effectively prevent the spread of MDR A. baumannii in healthcare settings.
MDR A. baumannii remains a formidable pathogen in ICU settings, with high resistance rates, multidrug-resistance mechanisms, and substantial environmental persistence. Colistin and tigecycline retained partial activity, but emerging colistin resistance is concerning. The high prevalence of carbapenemases, particularly metallo-β-lactamases, coupled with strong biofilm-forming ability, underscores its capacity for survival and transmission. Frequent contamination of high-touch surfaces such as beds and rails highlights the role of the environment in nosocomial spread. These findings call for reinforced infection control, targeted environmental disinfection, and prudent antibiotic stewardship to limit the impact of this resilient pathogen.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
BM conceptualized the study and applied methodology. MRR performed investigation, collected resources and data curation. BM collected the samples, performed experiments, visualization, project administration and funding acquisition. RPM performed validation and formal analysis. MSS performed supervision. BM wrote the original draft. RPM and MSS wrote, reviewed and revised the manuscript. All authors read and approved the final manuscript for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was approved by the Institutional Ethics Committee, JSS Medical College and Hospital, Mysuru, Karnataka, India (JSS|MC |PG|0040|2022-2023), dated 05-04-2023.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Lee CR, Lee JH, Park M, et al. Biology of Acinetobacter baumannii: Pathogenesis, antibiotic resistance mechanisms, and prospective treatment options. Front Cell Infect Microbiol. 2017;7:55.
Crossref - Nemec A, Krizova L, Maixnerova M, Sedo O, Brisse S, Higgins PG. Acinetobacter seifertii sp. nov., a member of the Acinetobacter calcoaceticus–Acinetobacter baumannii complex isolated from human clinical specimens. Int J Syst Evol Microbiol. 2015;65(3):934-942.
Crossref - Vijayakumar S, Mathur P, Kapil A, et al. Molecular characterization and epidemiology of carbapenem-resistant Acinetobacter baumannii collected across India. Indian J Med Res. 2019;149(2):240-246.
Crossref - Holt K, Kenyon JJ, Hamidian M, et al. Five decades of genome evolution in the globally distributed, extensively antibiotic-resistant Acinetobacter baumannii global clone 1. Microb Genom. 2016;2(2):e000052.
Crossref - Poirel L, Jayol A, Nordmann P. Polymyxins: Antibacterial activity, susceptibility testing, and resistance mechanisms encoded by plasmids or chromosomes. Clin Microbiol Rev. 2017;30(2):557-596.
Crossref - Fleming ID, Krezalek MA, Belogortseva N, et al. Modeling Acinetobacter baumannii wound infections: The critical role of iron. J Trauma Acute Care Surg. 2017;82(3):557-565.
Crossref - Rumbo-Feal S, Gómez MJ, Gayoso C, et al. Whole transcriptome analysis of Acinetobacter baumannii assessed by RNA-sequencing reveals different mRNA expression profiles in biofilm compared to planktonic cells. PLoS One.2013;8(8):e72968.
Crossref - BioMérieux India. BioMérieux Corporate Website. Accessed August 11, 2025. https://www.biomerieux.com/corp/en.html
- MICROXPRESS® A Division of Tulip Diagnostics Pvt Ltd. MicroPro® BMD Kit Technical Details. Accessed August 11, 2025. https://www.microxpress.in/uploads/product/micropro®-bmd-kit_technicaldetails_106720240330.072737.pdf
- Rajshekar D, Sujatha SR, Karthik MVSK, Raveendran S. Evaluation of phenotypic carbapenem inactivation methods among carbapenem resistant gram-negative bacteria isolated from blood culture specimens and their synergy testing. Indian J Microbiol Res. 2024;11(3):175-179.
Crossref - Huang Y, Zhou Q, Wang W, et al. Acinetobacter baumannii Ventilator-Associated Pneumonia: Clinical Efficacy of Combined Antimicrobial Therapy and in vitro Drug Sensitivity Test Results. Front. Pharmacol. 2019;10:92.
Crossref - Lee Y, Yum JH, Kim CK, et al. Role of OXA-23 and AdeABC efflux pump for acquiring carbapenem resistance in an Acinetobacter baumannii strain carrying the blaOXA-66 gene. Ann Clin Lab Sci. 2010;40(1):43-48.
- Alshamrani MM, El-Saed A, Al Zunitan M, Abalkhail M, Abagguey D, Farahat FM. Novel preventive bundle for multidrug-resistant organisms in intensive care setting; tertiary care experience. Heliyon. 2024;10(7):e28072.
Crossref - Yadav SK, Bhujel R, Hamal P, Mishra SK, Sharma S, Sherchand JB. Burden of Multidrug-Resistant Acinetobacter baumannii Infection in Hospitalized Patients in a Tertiary Care Hospital of Nepal. Infect Drug Resist. 2020;13:725-732.
Crossref - Zhang Y, Luan G, Xu Y, et al. Characterization of carbapenem-resistant Acinetobacter baumannii isolates in a Chinese teaching hospital. Front. Microbiol.2015;6:910.
Crossref - Mohanty S, Behera S, Behura R, et al. Antibacterial activity of thiazole and its derivatives: a review. Biointerface Res Appl Chem. 2022;12:2171–2195.
Crossref - Khoshnood S, Savari M, Abbasi Montazeri E, Farajzadeh Sheikh A. Survey on Genetic Diversity, Biofilm Formation, and Detection of Colistin Resistance Genes in Clinical Isolates of Acinetobacter baumannii. Infect Drug Resist. 2020;13:1547-1558.
Crossref - Antunes LC, Visca P, Towner KJ. Acinetobacter baumannii: Evolution of a global pathogen. Pathog Dis. 2019;77(2):ftz005.
Crossref - Singh S, Singh S, Trivedi M, Dwivedi M. An insight into MDR Acinetobacter baumannii infection and its pathogenesis: Potential therapeutic targets and challenges. Microb Pathog. 2024;192:106674.
Crossref - Garnacho-Montero J, Timsit JF. Managing Acinetobacter baumannii infections. Curr Opin Infect Dis. 2019;32(1):69-76.
Crossref - Kaur A, Sharma P, Capalash, N. Curcumin alleviates persistence of Acinetobacter baumannii against colistin. Sci Rep. 2018;8:11029.
Crossref - Weber DJ, Anderson D, Rutala WA. The role of the environment in transmission of multidrug-resistant organisms. Curr Opin Infect Dis. 2020;33(4):338-345.
Crossref - Suleyman G, Alangaden G, Bardossy AC. The role of environmental contamination in Acinetobacter transmission in healthcare settings. Clin Infect Dis. 2021;72(11):e900-e906.
Crossref - Cruz-López F, Villarreal-Trevino L, Morfín-Otero R, Rodriguez-Noriega E. Environmental reservoirs of carbapenem-resistant Acinetobacter baumannii in hospitals. J Hosp Infect. 2023;134:45-53.
Crossref - Harding CM, Hennon SW, Feldman MF. Uncovering the mechanisms of Acinetobacter baumannii virulence. Nat Rev Microbiol. 2018;16(2):91-102.
Crossref - Wong D, Nielsen TB, Bonomo RA, Pantapalangkoor P, Luna B, Spellberg B. Clinical and Pathophysiological Overview of Acinetobacter Infections: a Century of Challenges. Clin Microbiol Rev. 2017;30(1):409-447.
Crossref - Costa DM, Johani K, Melo DS, et al. Biofilm contamination of high-touched surfaces in intensive care units: epidemiology and potential impacts. Lett Appl Microbiol. 2019;68(4):269-276.
Crossref - Sharma A, Thakur IS, Dureja P. Enrichment, isolation and characterization of pentachlorophenol degrading bacterium Acinetobacter sp. ISTPCP-3 from effluent discharge site. Biodegradation. 2009;20:643-650.
Crossref - Pragasam AK, Vijayakumar S, Bakthavatchalam YD, et al. Molecular characterisation of antimicrobial resistance in Pseudomonas aeruginosa and Acinetobacter baumannii during 2014 and 2015 collected across India. Indian J Med Microbiol. 2016;34(4):433-441.
Crossref - Novović K, Jovčić B. Colistin Resistance in Acinetobacter baumannii: Molecular Mechanisms and Epidemiology. Antibiotics (Basel). 2023;12(3):516.
Crossref - Paul M, Daikos GL, Durante-Mangoni E, et al. Colistin alone versus colistin plus meropenem for severe infections caused by carbapenem-resistant Gram-negative bacteria. Lancet Infect Dis. 2018;18(4):391-400.
Crossref - Joshi PR, Acharya M, Kakshapati T, Leungtongkam U, Thummeepak R, Sitthisak S. Co-existence of blaOXA-23 and blaNDM-1 genes of Acinetobacter baumannii isolated from Nepal: antimicrobial resistance and clinical significance. Antimicrob Resist Infect Control. 2017;6:21.
Crossref - Hou C, Yang F. Drug-resistant gene of blaOXA-23, blaOXA-24, blaOXA-51 and blaOXA-58 in Acinetobacter baumannii. Int J Clin Exp Med. 2015;8(8):13859-13863
- Vijayakumar S, Gopi R, Gunasekaran P, et al. Molecular characterization of carbapenem-resistant Acinetobacter baumannii from India. J Glob Antimicrob Resist. 2021;24:89-96.
Crossref - Nordmann P, Poirel L. Epidemiology and diagnostics of carbapenem resistance in Gram-negative bacteria. Clin Infect Dis. 2019;69(Suppl 7):S521-S528.
Crossref - Veeraraghavan B, Shin E, Bakthavatchalam YD, et al.A microbiological and structural analysis of the interplay between sulbactam/durlobactam and imipenem against penicillin-binding proteins (PBPs) of Acinetobacter spp. Antimicrob Agents Chemother. 2025; 69:e01627-24.
Crossref - Dortet L, Poirel L, Errera C, Nordmann P. CarbAcineto NP test for rapid detection of carbapenemase-producing Acinetobacter spp. J Clin Microbiol. 2014;52(7):2359-2364.
Crossref - Falagas ME, Vardakas KZ, Tsiveriotis KP, Triarides NA, Tansarli GS. Effectiveness and safety of tigecycline for multidrug-resistant Acinetobacter baumannii infections. Int J Antimicrob Agents. 2019;54(5):511-520.
Crossref - He T, Wang R, Liu D, et al. Emergence of plasmid-mediated tigecycline resistance mechanisms. Nat Microbiol. 2019;4(9):1450-1456.
Crossref - Ni W, Han Y, Liu J, et al. Minocycline treatment for multidrug-resistant Acinetobacter baumannii infections: A systematic review. Int J Antimicrob Agents. 2022;59(3):106554.
Crossref - Tacconelli E, Carrara E, Savoldi A, et al. WHO priority pathogens list update: Implications for antimicrobial research. Lancet Infect Dis. 2024;24(1):e15-e29.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.