


The dengue virus (DENV), leading to dengue, is a mosquito-borne virus which has become a major global health concern, especially in tropical and subtropical areas. So far, no specific therapeutic drug or effective antiviral medication has been approved, despite the high rates of morbidity and mortality. The primary goal of current management regimens is symptomatic alleviation, underscoring the pressing need for innovative therapeutic approaches. Given their varied pharmacological characteristics and low side effects, medicinal plants and their bioactive phytocompounds have attracted a lot of interest as possible antiviral medicines. Several compounds derived from plants have shown inhibitory actions against various stages of the DENV life cycle, indicating that they may be effective antiviral options. The current review offers a thorough examination of medicinal plants that have been shown to have anti-dengue properties, emphasizing their modes of action and prospects for future drug development.
Dengue, DENV, Phytocompounds, Antiviral, Medicinal Plants
Dengue, an arthropod-borne viral disease has recently grown in importance as a health issue in Asia. It is the root cause of more than 70% of all common ailments. The dengue virus (DENV) is part of the Flavivirus genus within the Flaviviridae family, which comprises over 70 significant pathogens that cause diseases in humans, primarily affecting the intertropical areas. This viral infection is spread to people through the bite of female mosquitoes, predominantly from the Aedes aegypti species, with Aedes albopictus serving as a secondary vector.1
In recent years, the worldwide occurrence of dengue has escalated, marking it as the most rapidly dispersing insect vector-borne disease (VBD).2 An epidemiological assessment reveals that DENV infection reaches about two-fifths of the global population, affecting nearly 390 million individuals yearly. The countries most affected by dengue are Brazil, Argentina, and Mexico. Based on the WHO Global Dengue Surveillance, between January and November 2024, the overall dengue case count reached 13,860,025, alongside a total of 9990 fatalities. Most of these instances originated from the Americas, which recorded 12,669,716 cases and 7713 deaths. The region with the second-highest impact was Southeast Asia, with an aggregate of 693,596 cases and 2002 deaths. Between January 2025 to March 2025, a total of 1,654,640 cases were reported, out of which 603,148 were confirmed cases, 4154 severe cases and 852 deaths were reported. It is important to note that numerous dengue cases are asymptomatic or mild, and some instances might have been incorrectly diagnosed as other febrile illnesses, suggesting that the actual incidence might surpass reported figures.2,3 Furthermore, urban growth and population shifts have significantly contributed to the rising burden in the area.4 As per the report released by The National Centre for Vector Borne Diseases Control (NCVBDC), Government of India, in 2019, there were 157,315 reported cases with 166 fatalities, and in 2024, up to February, 233,400 cases were noted with 236 deaths.5 Figure 1 illustrates the total number of reported dengue cases across different countries, from January 2024 to May 2025, with a color gradient indicating the burden from low (light yellow) to extremely high (dark red). According to the WHO data on global dengue situation, a total of 17,710,747 cases and 12,887 deaths were reported.3 India reported over 232,425 total cases with 200,334 confirmed and 233 deaths.
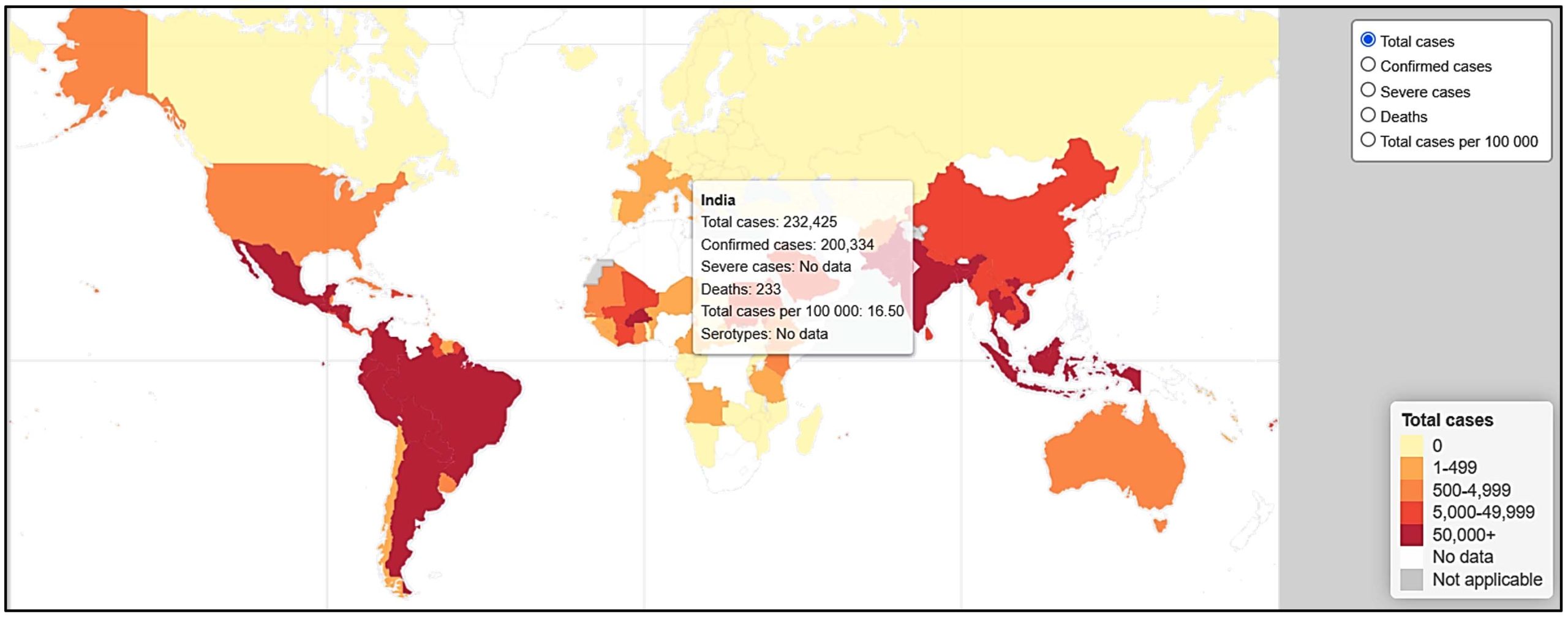
Figure 1. Global distribution of dengue cases (WHO, January 2024-May 2025). The interactive world map presents the total dengue cases reported by country, with color intensity indicating disease burden3
The highest number of cases are reported during the monsoon season, which typically runs from June to September. Dengue is endemic in many parts of India, and outbreaks have occurred in various states, including Delhi, Maharashtra, Tamil Nadu, Karnataka, West Bengal, Rajasthan, Punjab and Kerala (Figure 2). The disease is more common in urban areas, where the mosquito vector breeds in stagnant water and can easily spread the virus from person to person.
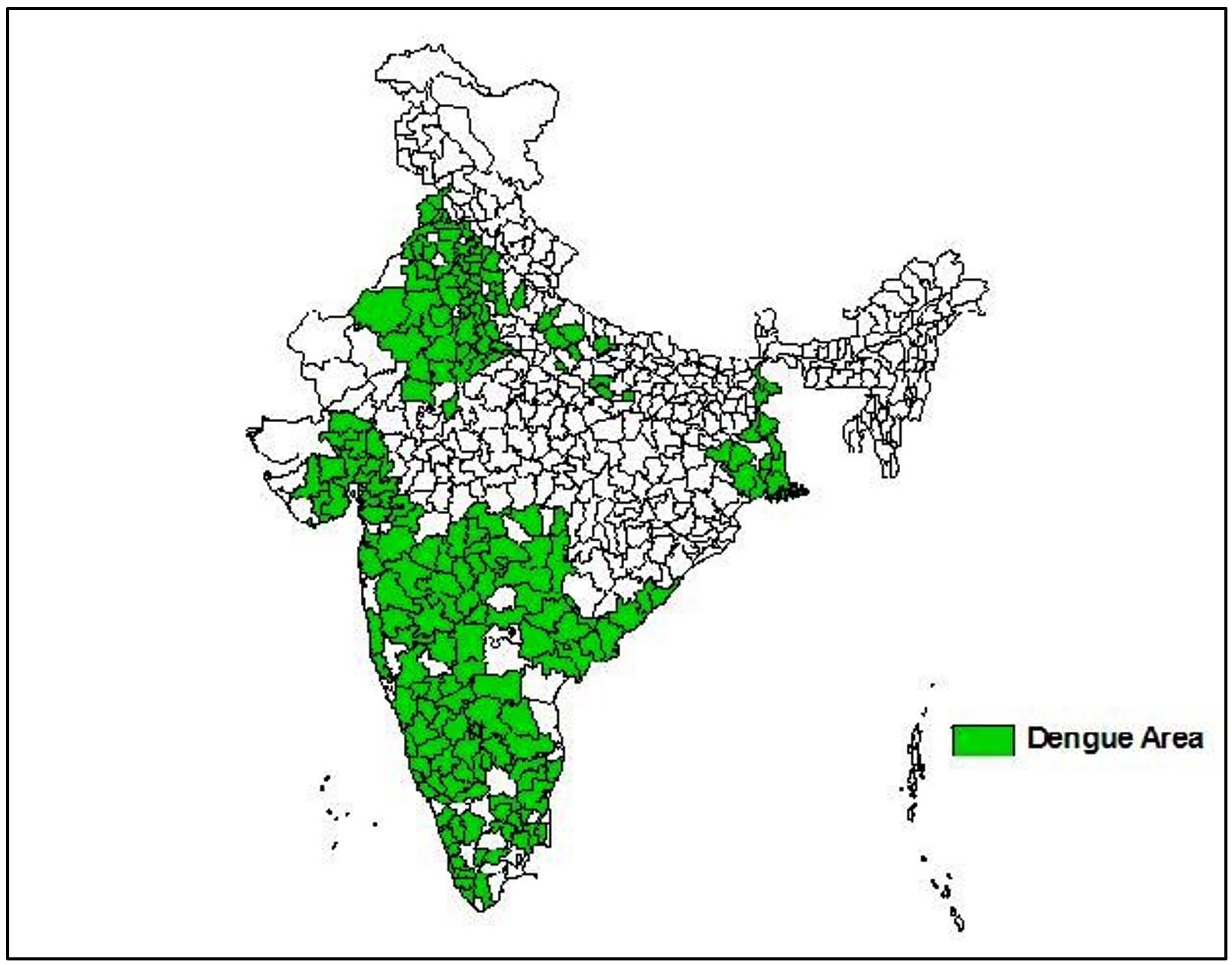
Figure 2. Dengue cases reported recently from several Indian regions have been mapped. (Source: https://ncvbdc.mohfw.gov.in/index4.php?lang=1&level=0&linkid=432&lid=3714, accessed April 2024)
Joint discomfort, rashes, headache, low white blood cell count, moderate asymptomatic dengue fever (DF), severe dengue haemorrhagic fever (DHF), and dengue shock syndrome (DSS) are all symptoms of dengue virus infection. Within 3-14 days of infection, a dengue symptom will appear. Blood pressure drops, blood platelet levels drop, and bleeding all occur as a result of a serious dengue hemorrhagic fever.6 All age groups of people, including infants, toddlers, and adults, are susceptible to the flu-like illness known as dengue fever, although pregnant women and those with weakened immune systems are particularly at risk. Therefore, mortality may be reduced and people could be made aware of this disease.7
Structure, function, replication and transmission of the virus
Structure and function
The dengue virus genome consists of a single strand of RNA. This RNA is classified as positive sense because it can be directly translated into proteins. The viral genome contains ten genes. The genome is translated into one long polypeptide which is then cleaved into ten proteins. Three of these proteins are structural: the capsid (C), envelope (E), and membrane (M) proteins (Figure 3). The remaining seven are non-structural proteins: NS1, NS2A, NS2B, NS3, NS4A, NS4B, and NS5 (Figure 4). These non-structural proteins are involved in the processes of viral replication and assembly. The dengue virus has a spherical shape and with a size of about 50 nm. Nucleocapsid is the core of the virus, which consists of the viral genome along with C proteins. Encasing the nucleocapsid is a membrane known as the viral envelope, which is a lipid bilayer acquired from the host. Within the viral envelope are 180 copies of the E and M proteins that traverse the lipid bilayer. These proteins create a protective external layer that regulates the entry of the virus into human cells.8,9
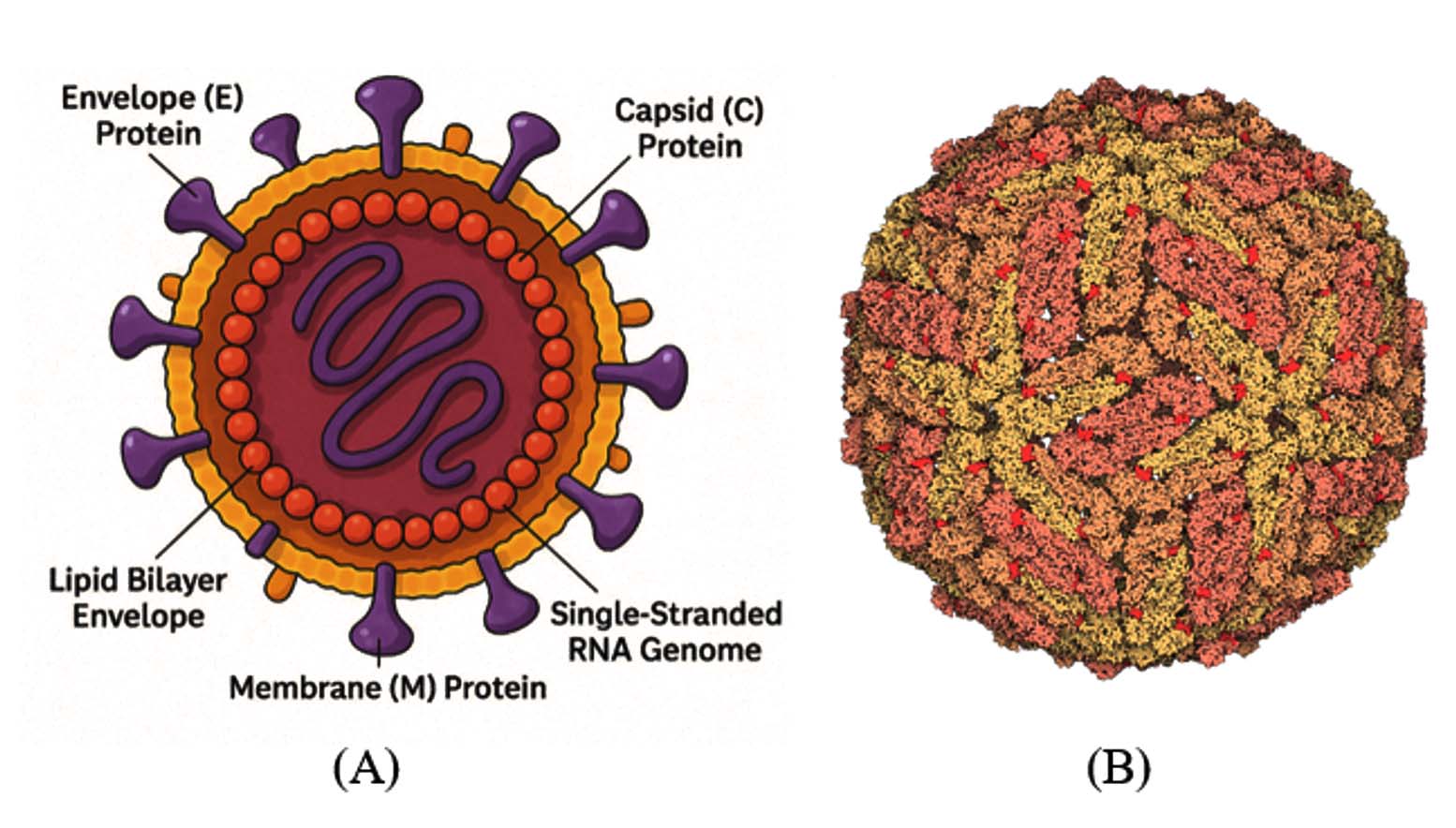
Figure 3. (A) Structural representation of DENV. (B) Structure of major envelope protein E of DENV taken from Protein Data Bank (PDB) (Source: https://www.rcsb.org/structure/1k4r)
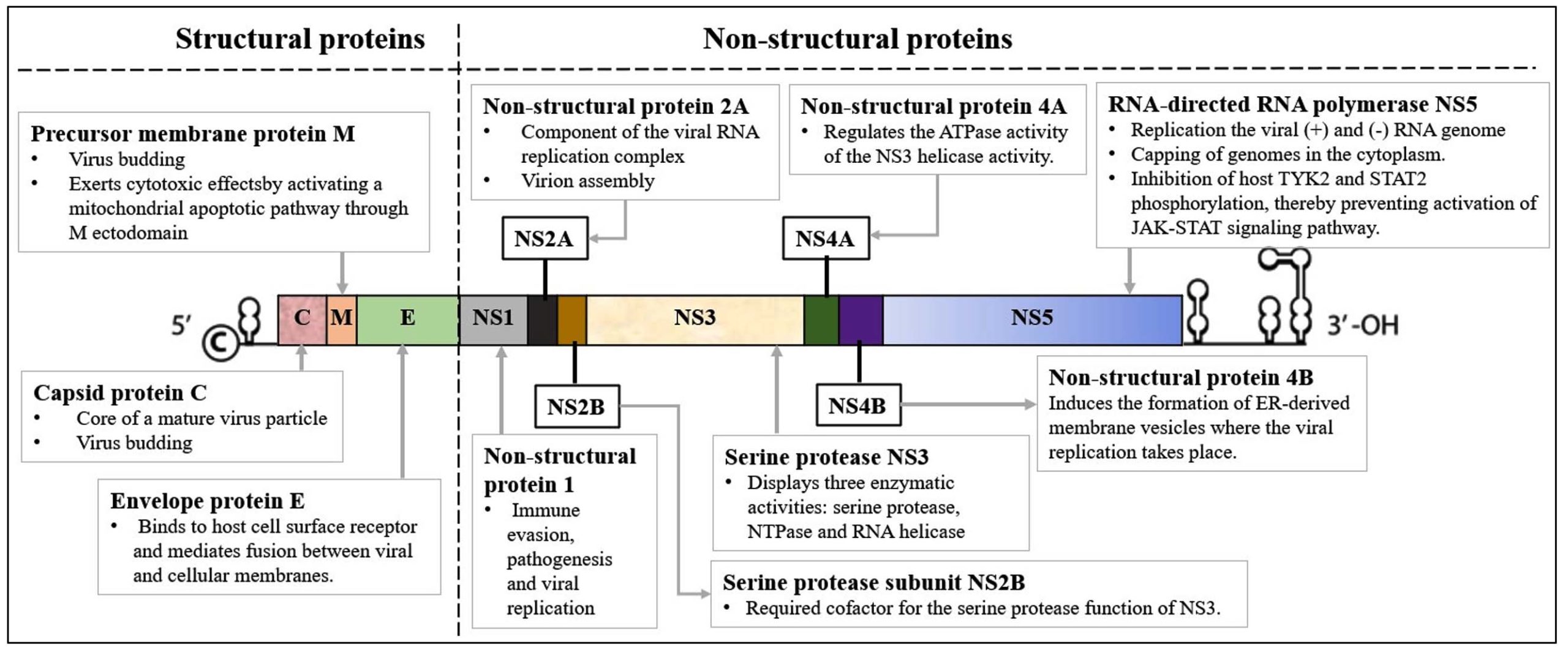
Figure 4. Schematic representation of the viral genome, highlighting structural and non-structural proteins. The genome consists of 5′ and 3′ untranslated regions (UTRs) flanking a single open reading frame (ORF). Structural proteins (C, M, E) are involved in viral entry, fusion, and assembly, while non-structural proteins (NS1-NS5) facilitate viral replication and immune evasion. Each protein is color-coded for distinction, with their respective functions annotated (Source: The image was created in Microsoft PowerPoint 360)
Serotypes and replication
Dengue is caused by four related viruses identified as DENV-1, DENV-2, DENV-3, and DENV-4. These are known as serotypes since they interact differently with antibodies in human blood serum. Although the dengue viruses are alike, sharing around 65% of their genetic makeup, there is still some genetic diversity within each serotype. Regardless of these differences, contracting any of the dengue serotypes leads to the same disease and set of clinical symptoms.8,10 The DENV-2 serotype is notorious for being more lethal than other serotypes.
A cell becomes infected when a virus attaches to the host cell’s surface.11,12 Through receptor-mediated endocytosis, in which the cell membrane creates an endosome, it enters the cell. In order to provide a port for the genetic material to release, the virus penetrates the endosome deeply and waits for the membrane to become negatively charged. Now, the virus present in fluid of the cell starts to multiply. Changes in the pH of the secretory channel during its passage have a significant impact on the virus’s ability to develop. The endocytosis process allows the dengue virus to cling to a host cell’s surface and enter the cell.11 The virus releases its contents into the cytoplasm after merging with the endosomal membrane deep inside the cell. As the virus particle breaks down, the viral genome is released. When the viral RNA (vRNA) is translated into a single polypeptide and then split into 10 proteins, the viral genome is replicated. On the surface of the endoplasmic reticulum (ER), viral assembly occurs when freshly produced RNA and structural proteins protrude. The mechanism via which the immature viral particles are transported is the trans-Golgi network (TGN), where the viral particles evolve and convert into their infectious condition. The mature viruses are subsequently expelled from the cell and can move on to other hosts (Figure 5).
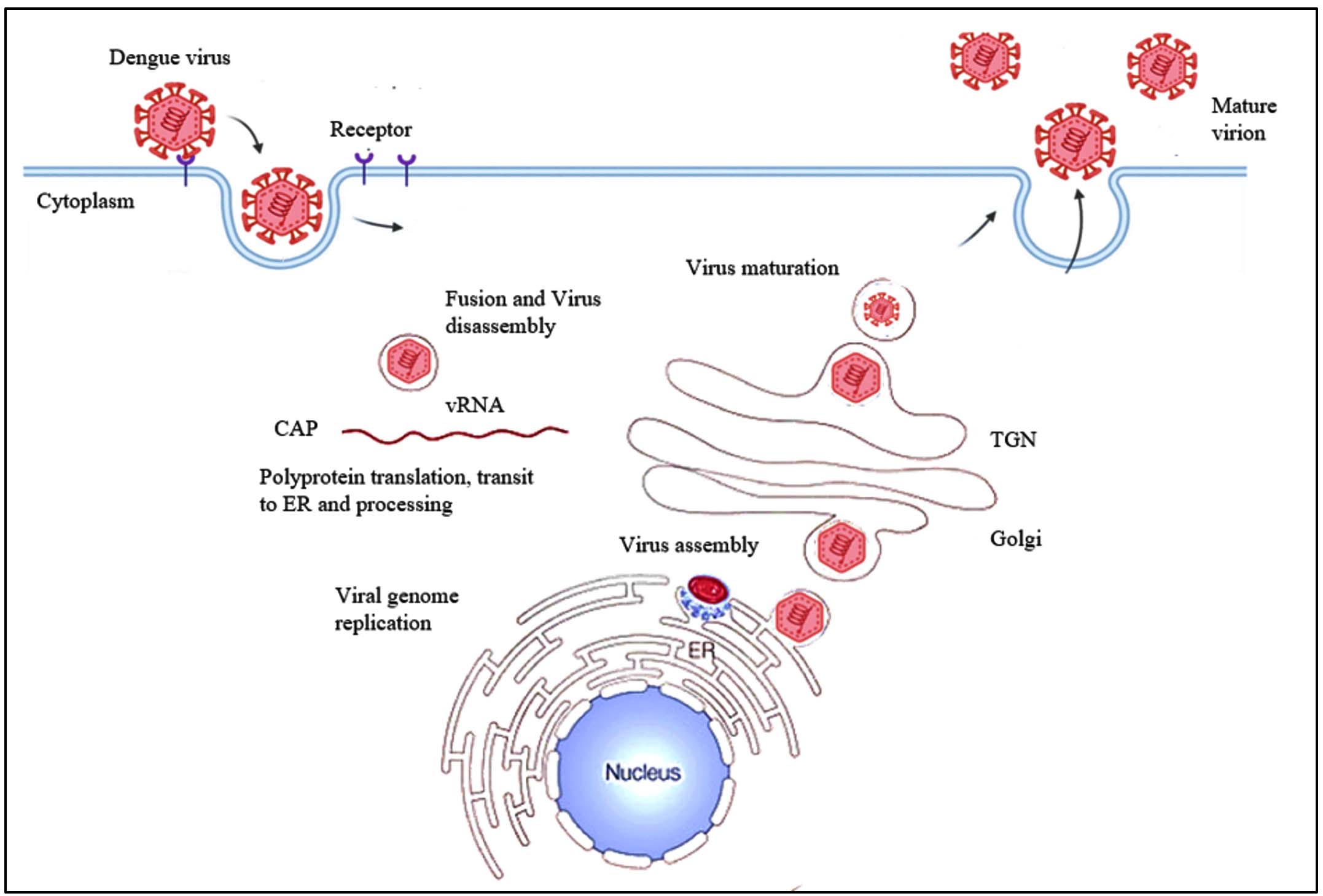
Figure 5. There are multiple crucial steps in the Dengue virus’s replication cycle. First, DENV attaches to certain receptors on the cell surface and penetrates the host cell. The RNA genome of the virus is then discharged into the cytoplasm of the host cell. Viral proteins are produced inside the cell using the viral RNA as a template for translation. These proteins aid in the assembly of fresh viral particles and viral RNA replication. Once generated, the new virus particles leave the host cell by frequently inducing cell death. This release enables the virus to continue its replication cycle and infect nearby cells (Source: The image was created using BioRender and Microsoft PowerPoint 360)
Transmission of DENV
Aedes aegypti is a small, dark mosquito characterized by white lyre shaped patterns and striped legs. This mosquito primarily feeds on mammalian hosts, especially humans, even when other hosts are available. It also feeds several times throughout a single gonotrophic cycle (the cycle of feeding and egg production), which has consequences for the transmission of diseases.13 An egg takes 7-10 days to mature into an adult mosquito. Female Aedes mosquitoes lay eggs on the inner surfaces of water-holding containers. Larvae hatch from mosquito eggs and inhabit water. Larvae develop into pupae. Pupae evolve into adult, flying mosquitoes. Adult female mosquitoes bite humans and animals. Mosquitoes require blood to generate eggs14 (Figure 6).
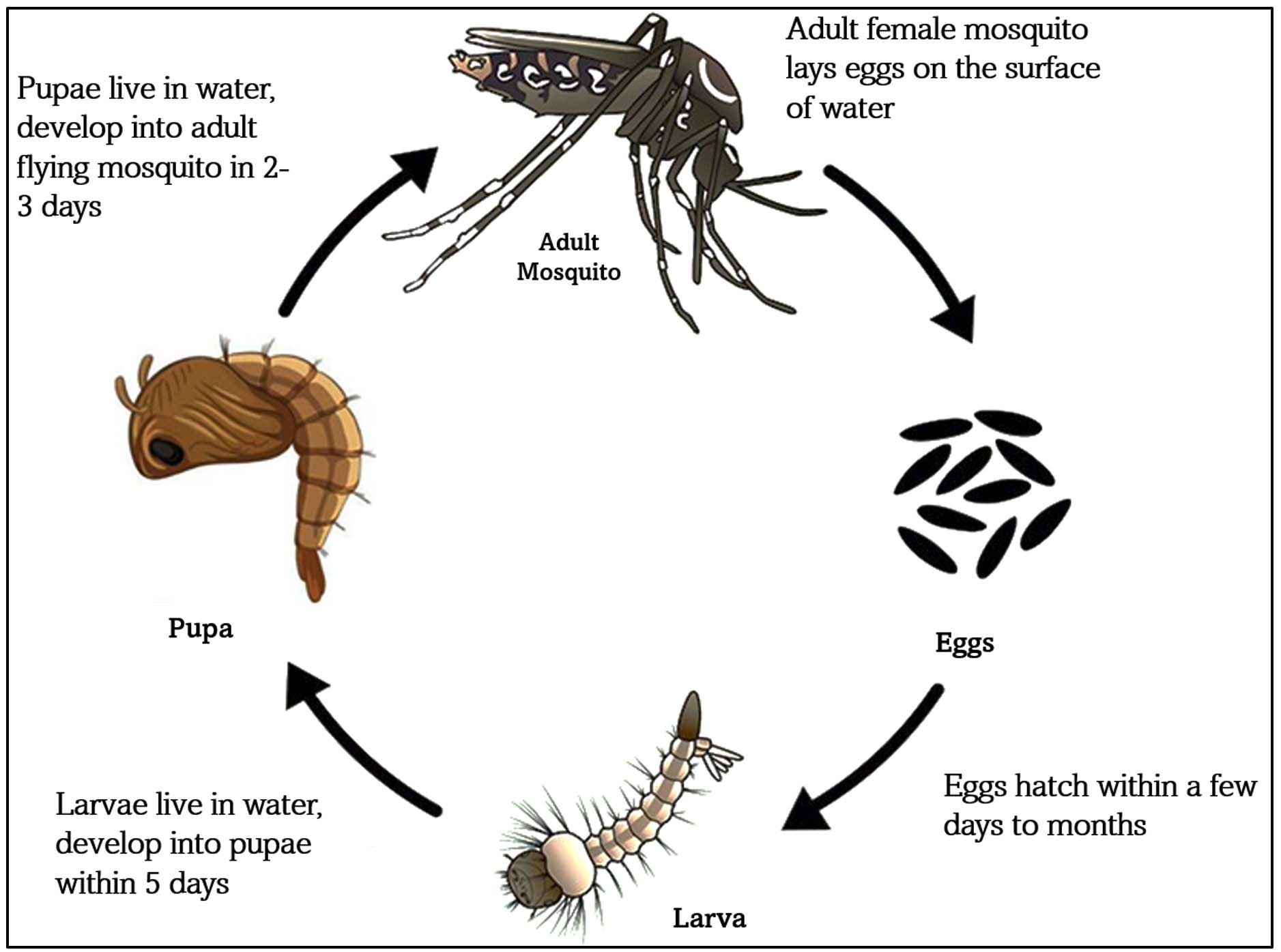
Figure 6. Developmental stages of the Aedes mosquito: egg, larva, pupa, and adult. Adult female mosquitoes require a blood meal for egg production, facilitating disease transmission (Source: The image was created using BioRender and Microsoft PowerPoint 360)
The transmission of all four serotypes is maintained in two cycles: sylvatic (transmission among wild animals) and human. Both the cycles are ecologically and evolutionarily distinct. This is maintained by non-human primates or by a monkey-Aedes-monkey cycle in the sylvatic habitats of West Africa, Southeast Asia, peninsular Malaysia, and eastern Senegal. The incubation period of the DENV ranges from 3-14 days, averaging 4-7 days.13,14
Pathogenesis of DENV infection
DENV pathogenesis involves a complex interplay between viral replication and host immune responses, leading to a wide spectrum of clinical outcomes. Transmission begins when an infected Aedes mosquito introduces the virus into the human host. The virus initially infects dendritic cells and subsequently spreads to macrophages, which serve as major sites for viral replication. During a primary infection, innate immune cells such as natural killer (NK) cells and macrophages play a crucial role in viral clearance. However, antibody-dependent enhancement (ADE) may occur, where non-neutralizing or suboptimal antibodies facilitate increased viral entry into Fc receptor–bearing cells, promoting higher viral loads and disease severity.9,14
In cases of secondary infection with a different DENV serotype, memory T and B cells are rapidly activated. While this adaptive immune response aims to control viral replication, cross-reactive but non-protective antibodies can exacerbate ADE, leading to heightened viral dissemination and immune activation. The resulting immune response involves both innate and adaptive arms. Innate immunity, characterized by NK cell and macrophage activation, induces pro-inflammatory cytokines, contributing to fever and systemic manifestations. Concurrently, B cell activation produces antibodies, while T cells mediate cytotoxicity and cytokine release.14,15
An exaggerated or dysregulated adaptive immune response is associated with increased vascular permeability and endothelial dysfunction, leading to hallmark clinical features such as rash and plasma leakage. Severe cases often progress to thrombocytopenia, a consequence of bone marrow suppression, immune-mediated platelet destruction, and increased peripheral consumption, which together heighten the risk of hemorrhage (Figure 7). Overall, DENV pathogenesis is a dynamic process shaped by viral factors and host immune responses, where ADE and immune dysregulation play pivotal roles in the progression from mild febrile illness to severe dengue.14-16
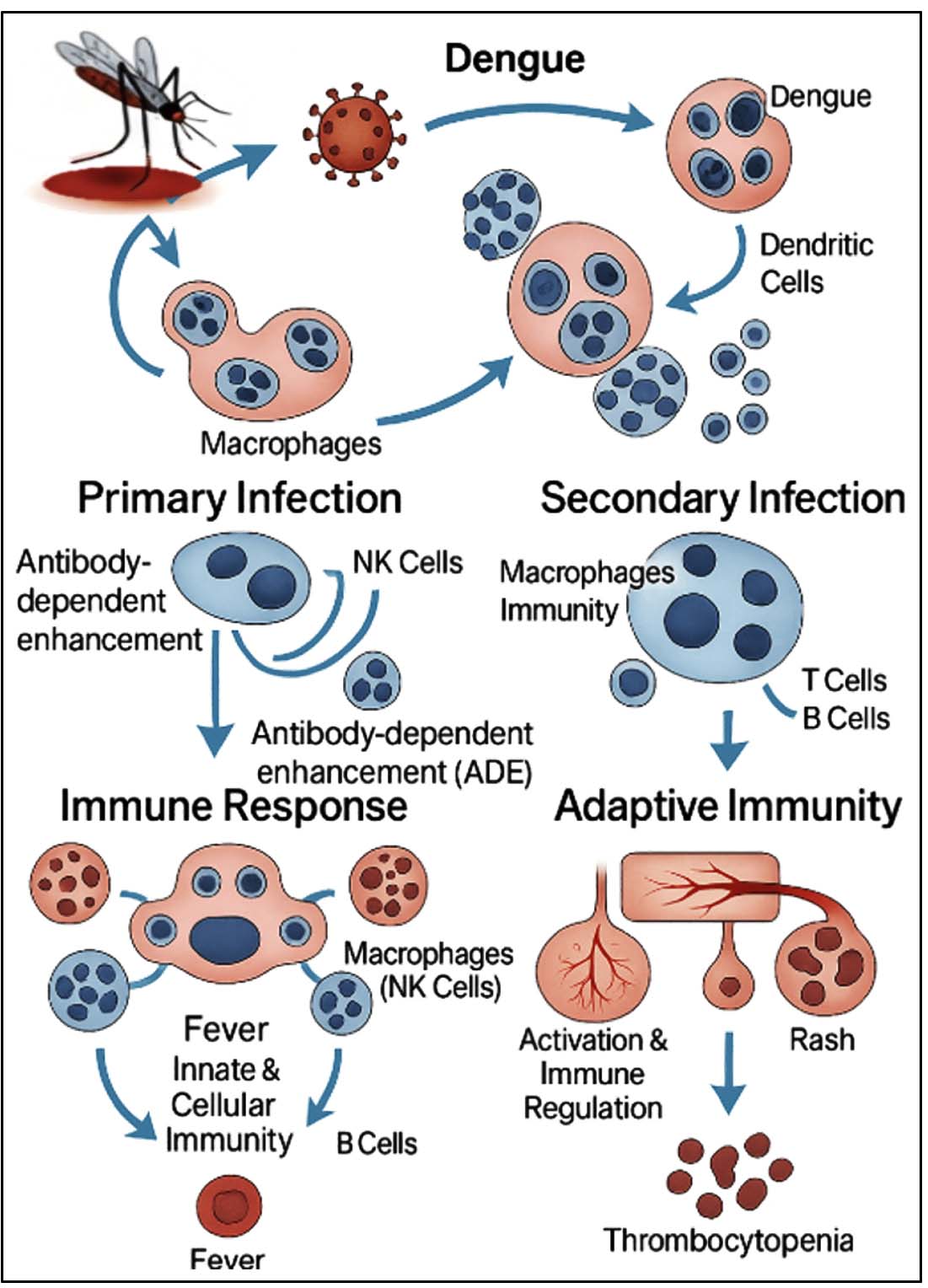
Figure 7. The diagram illustrates dengue virus entry through an infected Aedes mosquito bite, followed by viral replication in dendritic cells and macrophages. During primary infection, innate immunity involving NK cells and antibody production is activated. In secondary infections, memory immune cells may trigger ADE, leading to increased viral replication, cytokine storm, and clinical symptoms such as fever, rash, and thrombocytopenia. The figure highlights how both innate and adaptive immunity contribute to disease progression (Source: The image was created using BioRender and Microsoft PowerPoint 360)
Diagnostic modalities
Early and accurate diagnosis of DENV infection is crucial for prompt treatment, outbreak management, and lowering case fatality rates. Clinical/syndromic diagnosis, laboratory-based techniques, and novel, developing technologies are the main categories into which current diagnostic modalities are divided.9 The usefulness of each technique, which has its own advantages and disadvantages, is frequently contingent upon the stage of the infection, the resources available, and any cocirculating infections in endemic areas. Dengue is categorized by the WHO into three clinical categories: dengue without warning symptoms, dengue with warning signs, and severe dengue which includes DHF and DSS dengue shock syndrome. Signs and symptoms during and after the acute febrile phase serve as the basis for clinical evaluation.9,17-19 New diagnostic platforms have been developed in response to the growing need for quick and easily available diagnostics, particularly in resource-constrained environments and during epidemics (Table 1).
Table (1):
Summary of Dengue Diagnostics modalities9,17-19
Sl. No. |
Diagnostic method |
Target |
Time Window |
Principle |
Advantages |
Limitations |
|---|---|---|---|---|---|---|
1. |
NS1 Antigen Detection (ELISA/RDT) |
NS1 protein |
Day 1 – Day 5 |
Detection of viral NS1 antigen in blood |
Early diagnosis, simple, widely available |
Lower sensitivity in secondary infections and after Day 5 |
2. |
RT-PCR |
Viral RNA |
Day 1 – Day 5 |
Amplifies viral RNA for detection and serotyping |
High sensitivity and specificity, serotype identification |
Expensive, requires specialized equipment and expertise |
3. |
IgM ELISA |
Anti-DENV IgM |
Day 5 onward |
Detects IgM antibodies produced post-infection |
Cost-effective, useful for recent infections |
May cross-react with other flaviviruses |
4. |
IgG ELISA |
Anti-DENV IgG |
Day 5 onward |
Detects IgG for past or secondary infections |
Helps identify secondary infections |
Cross-reactivity and delayed detection |
5. |
PRNT |
Neutralizing bodies |
Post Day 7 |
Quantifies virus-specific neutralizing antibodies |
Gold standard for confirmation |
Time-consuming, requires BSL-3 lab and expertise |
6. |
CRISPR-based |
Viral RNA |
Any |
RNA detection using Cas enzymes and fluorescence |
Ultra-sensitive, rapid, portable |
Still under development and validation |
7. |
LAMP |
Viral RNA |
Day 1 – Day 5 |
Isothermal amplification of viral RNA |
Rapid, no thermal cycler required |
Risk of contamination, primer design complex |
8. |
Biosensors and Microfluidic Devices |
NS1/IgM/IgG |
Any |
Detection via nano/micro-scale analytical platforms |
Point-of-care, low-cost, minimal sample volume |
Limited to pilot studies or prototypes |
Current therapeutic approaches and limitations
There is currently no designated antiviral therapy for dengue illness. The main goal is to alleviate pain symptoms. In most instances, dengue fever can be managed at home with pain relief medications. Hydration, pain relievers, and adequate rest are usually sufficient. Acetaminophen is commonly utilized for pain management. Non-steroidal anti-inflammatory medications such as ibuprofen and aspirin should be avoided, as they may heighten the risk of bleeding. It is essential to closely monitor severe cases of dengue.9,20
Admission is necessary for individuals who have warning signs, have severe dengue fever, or are in other circumstances, such as being an infant, an older adult, pregnant, diabetic, or living alone. IV crystalloids may be started in patients with warning indications, and the fluid rate is adjusted according to the patient’s reaction. If the patient has already had prior boluses of crystalloid and has not responded, colloids are also the treatment of choice for individuals in shock. When the patient remains unstable and the hematocrit drops despite sufficient fluid resuscitation, a blood transfusion is necessary if there is significant bleeding or suspected bleeding. When the platelet count falls below 20,000 cells per microliter and the patient is at high risk of bleeding, platelet transfusion is considered.21
In spite of the high incidence and repeated outbreaks of dengue, there is now no particular antiviral therapy for the illness. Clinical management continues to be supportive, with an emphasis on hydration, symptom management, and careful observation of the course of the illness, particularly during the acute stage. The only licensed dengue vaccine, Dengvaxia, has shown limited efficacy and is associated with increased risk of severe disease in seronegative individuals, thereby restricting its widespread use.22 These therapeutic gaps emphasize the urgent need to investigate other approaches to dengue treatment. Due to their broad-spectrum antiviral properties, multi-target potential, and positive safety profiles, natural products, notably phytochemicals originating from medicinal plants, have become promising candidates in recent years. Numerous laboratory and computational studies have shown that certain plant compounds can disrupt critical phases of the dengue virus life cycle, such as how it enters cells, replicates, and processes proteins. This increasing evidence highlights the promise of plant-based compounds as a legitimate resource for creating new and safer treatments for dengue. For centuries, plants have been utilized across Asia, Africa, and Europe to address a range of illnesses, including those caused by viruses. Their antiviral characteristics are recognized for their ability to block viral replication, endocytosis, genome transcription, and protein production. Compounds found in plants may attach to surface proteins or to the biomembrane, DNA, or RNA of the virus.23 A brief summary of approved and investigational vaccines approved for dengue has been mentioned below in Table 2.
Table (2):
Summary of approved and investigational dengue vaccines
Vaccine type |
Example |
Mechanism of action |
DENV serotypes |
Status/ Stage |
Limitations |
|---|---|---|---|---|---|
Live-attenuated vaccine |
|
Induces both humoral and cellular responses via live, weakened virus |
Tetravalent |
Approved (Dengvaxia, Qdenga) Phase III (Butantan) |
|
Inactivated vaccine |
TDENV-PIV (GSK + WRAIR) |
Chemically inactivated viruses to trigger immunity |
Tetravalent |
Preclinical/Clinical |
|
DNA vaccine |
D1ME100 (TVDV / Vaxfectin®) |
Plasmids encoding E/prM proteins; induces neutralizing antibodies |
Tetravalent |
Phase I |
Lower immunogenicity in humans |
Recombinant subunit vaccine |
V180 (Merck) |
E protein variants expressed in cells to generate antibody responses |
Target-specific
(E protein) |
Completed Phase I |
|
Peptide-based vaccine |
PepGNP-Dengue |
Synthetic epitopes for targeted T-cell responses (CD8+) No antibody generation |
Multivalent (experimental) |
Phase I |
|
mRNA vaccine |
mRNA-prM/E (DENV-1) mRNA-EIII (DENV-1/4) + NS1 (DENV-2/3) |
Encodes DENV proteins in mRNA, delivered via lipid nanoparticles |
Multivalent |
Preclinical |
Needs optimization for efficacy & delivery |
Role of phytochemicals in antiviral therapy
Phytochemicals are bioactive substances that originate from plants. Their medicinal qualities have long been known, and their use in antiviral treatment has gained more scientific attention over the past two decades. Kadir et al. conducted a review of sixty-nine studies spanning from 1997-2012 that focused on plants with potential anti-dengue properties.24 This review highlighted 31 different species from 24 families, including Ocimum sanctum, Carica papaya, Kaempferia parviflora, Phyllanthus urinaria, Piper retrofractum, and Psidium guajava, all noted for their effectiveness against dengue fever, as outlined in 61 studies. Out of these species, 11 yielded around 10 distinct phytochemicals. Some of these compounds include andrographolide, panduratin A, castanospermine, hydroxypanduratin A, carrageenans, turmerone, kappa carrageenan, galactomanan, and others that may hold promise for dengue fever treatment.25
Natural medicines are effective against Ae. aegypti because of their antiviral, larvicidal, and mosquitocidal effects as well as their ability to repel mosquitoes.9 Numerous phytochemicals, including flavonoids, alkaloids, terpenoids, polyphenols, and saponins, have been shown to have potent inhibitory effects on DENV proteins, such as the E protein, the NS5 RNA dependent RNA polymerase, and the NS2B/NS3 protease. In vitro studies have validated the possibility of these substances lowering viral replication or cytopathic consequences in cell cultures, while in silico molecular docking investigations have revealed encouraging interactions between these compounds and viral targets.
Phytochemicals can disrupt different phases of the viral life cycle, such as viral attachment, penetration, replication, assembly, and release, thanks to their varied structures and mechanisms of action. The classes that have received the most attention include alkaloids, flavonoids, terpenoids, phenolics, polyphenols, lignans, and tannins. Several of these molecules have been shown to have broad-spectrum antiviral activity against both DNA and RNA viruses using in vitro, in vivo, and computational modeling techniques.26,28
- Flavonoids including luteolin, quercetin, apigenin and baicalin have shown antiviral activity by blocking viral enzymes like reverse transcriptase, proteases, and RNA-dependent RNA polymerases. Quercetin, for instance, has been shown to be effective against dengue, influenza, and hepatitis viruses by preventing replication and altering the host’s immune response.26,27,29
- Alkaloids like lycorine and berberine have shown notable antiviral effects, including against coronaviruses and flaviviruses, by blocking the production and translation of viral RNA.26,29
- Terpenoids, such as glycyrrhizin and andrographolide, have immunomodulatory effects that lessen the severity of viral pathogenesis by preventing viral binding and replication.28,29
- Phenolic compounds, including resveratrol, curcumin, and epigallocatechin gallate (EGCG), have been shown to reduce the production of pro-inflammatory cytokines and target diverse viral targets, making them useful in treating cellular inflammation caused by severe viral infections.27,28
- It is known that tannins and lignans prevent infection of host cells by interfering with the viral proteins and thus inhibiting the integrity of the envelope.27
In addition to having a direct impact on viruses, these chemicals also affect essential host pathways like NF-κB, MAPK, and interferon signaling, which are essential to the host’s immune response. They are appealing candidates for drug development due to their multitarget character, often reduced toxicity, and improved safety profiles.28 Tables 3 and 4 displays the major medicinal plants available in India that have been reported against DENV infection. The extracts and the isolated phytocompounds from different plant species that have been shown to have anti-dengue property are described in the sections that follow Table 3. Classification of phytochemicals with reported anti-dengue activity and their mechanism of action.
Table (3):
Classification of phytochemicals with reported anti-dengue activity and their mechanism of action
Phytochemical class |
Representative compounds |
DENV mechanism |
|---|---|---|
Flavonoids26,27,29 |
Luteolin, Quercetin, Myricetin, Hesperidin, Apigenin, Baicalin, Catechin |
Inhibition of NS2B/NS3 proteases, and RNA-dependent RNA polymerases, suppression of viral RNA replication, modulation of NF-κB–mediated cytokine production. |
Alkaloids26,29 |
Carpaine, Lycorine, Berberine |
Inhibition of viral RNA synthesis, immunomodulatory effects in infected monocytes |
Terpenoids28,29 |
Glycyrrhizin, Panduratin A, Tumerone, Hydroxypanduratin A, Andrographolide |
inhibition of NS5 polymerase, NS2B/NS3 protease, RNA-dependent RNA polymerase, reduction of viral replication. |
Phenolics27,28 |
Resveratrol, Curcumin, Gallic acid, Rosmarinic acid, Epigallocatechin gallate (EGCG) |
Reduction of pro-inflammatory cytokines, inhibition of viral entry and RNA replication. |
Tannins26,29 |
Geraniin, Tannic acid, Ellagic acid, Punicalagin |
Inhibition of viral attachment and entry, binding to E protein. |
Lignans28 |
Arctigenin, Phyllanthin, Sesamin, Hypophyllanthin, |
Inhibition of viral replication, interference with protein synthesis, modulation of host signaling. |
Table (4):
Anti-dengue phytocompounds, mechanisms and experimental evidence30,31
Plant/ Source |
Major Phytocompound |
Target Serotype |
Target / Mechanism |
Experimental Model |
|---|---|---|---|---|
Glycyrrhiza glabra (Licorice) |
Glycyrrhizic acid, derivatives |
DENV-1–4 |
Inhibits NS2B/NS3 protease, E protein; interferon induction |
Vero, A549 cells, mice |
Curcuma longa |
Curcumin |
DENV-2 |
Inhibits viral entry and RNA replication |
Low cytotoxicity; in vitro |
Andrographis paniculata |
Andrographolide |
DENV-2 |
Inhibits NS5 polymerase; reduces inflammation |
In vitro, in silico |
Phyllanthus spp. |
Crude extract |
DENV-1–4 |
Targets entry, polyprotein production, assembly |
Vero, C6/36, LLC-MK2 cells |
Azadirachta indica |
Bioflavonoids |
DENV-2 |
NS2B/NS3 protease inhibition |
Molecular docking, in vitro |
Nephelium lappaceum |
Geraniin |
DENV-2 |
Binds to E protein; entry inhibition |
In vitro |
Boesenbergia rotunda |
Flavonoids |
DENV-2 |
Inhibits NS2B/NS3 protease |
Enzyme-based assay |
Uncaria tomentosa |
Pentacyclic oxindole alkaloids |
DENV-2 |
Immunomodulatory and antiviral effects |
Human monocytes |
Carica papaya |
Carpaine |
DENV (general) |
Platelet augmentation; increased IL-6 & TPO |
Human clinical observation & reports |
Rosmarinus officinalis |
Rosmarinic acid |
DENV-2 |
Docking to viral proteins (E, NS3) |
In silico |
Cissampelos pareira |
Crude extract |
DENV-1–4 |
Broad-spectrum replication inhibition |
In vitro against all serotypes |
Psidium guajava |
Catechin |
DENV |
RNA synthesis inhibition |
In vitro & in silico |
Piper retrofractum |
Crude extract |
DENV-2 |
Viral inhibition (53.53% at 12.5 µg/ml) |
In vitro |
Camellia sinensis (Green tea) |
EGCG, catechins |
DENV |
Blocks viral entry and RNA synthesis |
In vitro |
Scutellaria baicalensis |
Scutellarin |
DENV (general) |
Reduces inflammation; inhibits replication |
In silico & in vitro |
Tinospora cordifolia |
Berberine, Magnoflorine |
DENV‑1–4 |
Inhibits structural & NS proteins; suppresses cytokine storm & vascular leakage |
In silico docking, literature review |
Boerhavia diffusa |
Crude extract |
DENV (general) |
Platelet augmentation; antioxidant, antiviral |
Clinical use in dengue patients |
Ocimum sanctum |
Eugenol |
DENV‑2 |
Inhibits DENV‑2 replication; entry/early stages |
Vero cell assays |
Gallic acid (various plants) |
Gallic acid, isobutyl gallate |
DENV‑2 |
Inhibits viral replication in both prophylactic and therapeutic use |
In vitro assays |
Sterculia quadrifida |
Stem bark extract |
DENV‑3 |
Reduces TNF‑α, IL‑1β, IL‑6 levels |
In vivo rat model |
Quercetin, luteolin, apigenin, kaempferol, and other flavonoids have several antiviral effects, such as blocking the NS5 polymerase and decreasing cytokine release. Resveratrol, curcumin, EGCG, and other polyphenols have antioxidant and immunomodulatory effects that are helpful in treating dengue-related inflammation and endothelial leakage.32 Although mechanisms are not fully understood, crude extracts frequently have a wider serotype coverage and may operate by synergistic bioactive interactions. In silico screening is becoming more and more prevalent in forecasting phytocompound binding to conserved dengue viral proteins (NS2B/NS3, NS5, E), which speeds up the process of discovering new medications.33
Dengue continues to pose a significant global health challenge, with rising incidence and limited therapeutic options. While conventional treatment remains largely supportive, medicinal plants and their phytochemicals present a promising frontier in anti-dengue therapy. Evidence from in vitro, in vivo, and in silico studies demonstrates that many plant-derived compounds can inhibit critical steps of the DENV life cycle, ranging from viral entry and replication to modulation of host immune responses. Phytocompounds from medicinal plants have been shown to stop the reproduction of DENV and lessen inflammation related to the illness. These phytocompounds have also been demonstrated to have additional advantageous characteristics, like anti-inflammatory, antioxidant, and immunomodulatory actions, which may improve the immunological response to dengue virus infection. Before the compounds may be utilised as a treatment for dengue fever, more research is required to estimate the efficacy and safety of these compounds in human clinical trials. In addition, the use of medicinal plants as a source of organic components raises questions about the standardisation and quality control of herbal extracts as well as the necessity of employing sustainable harvesting methods to avoid overusing natural resources.
In conclusion, natural substances derived from medicinal plants have demonstrated promise as antiviral agents against the dengue virus. Further research is necessary to evaluate the effectiveness and safety of these compounds as well as to find additional naturally occurring compounds with antiviral activity that can be used in the development of novel treatments for dengue fever.
ACKNOWLEDGMENTS
The authors acknowledge the support and infrastructure offered by Davangere University, Davangere, India, The Oxford College of Engineering, Bangalore, India, JSS Academy of Higher Education and Research (JSS AHER), Mysuru, India, JSS Science and Technology University, Mysuru, India and ICAR-National Institute of Veterinary Epidemiology and Disease Informatics (NIVEDI), Bengaluru, India.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
TSD, AJ, CSr and SMG conceptualized the study. AJ, BS, PT and DC applied methodology. CSr, CSh and SSP performed investigation. AJ and BS performed data curation. CSr, CSh, TSD, SMG and SSP performed data validation. CSh and SMG performed formal analysis and supervised the study. TSD, AJ, DC wrote the original draft. PT and SMG wrote, reviewed and revised the manuscript. All authors read and approved the final manuscript for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analysed during this study are included in the manuscript.
ETHICS STATEMENT
Not Applicable.
- Lim A, Shearer FM, Sewalk K, et al. The overlapping global distribution of dengue, chikungunya, Zika and yellow fever. Nat Commun. 2025;16(1):3418.
Crossref - Zhang WX, Zhao TY, Wang CC, et al. Assessing the global dengue burden: Incidence, mortality, and disability trends over three decades. PLoS Negl Trop Dis. 2025;19(3):e0012932.
Crossref - World Health Organization. Dengue: global situation, surveillance and progress – 2024 update. Weekly Epidemiological Record [Internet]. 2025;100(52):665-678. Available from: https://www.who.int/publications/i/item/who-wer10052-665-678
- Mutheneni SR, Morse AP, Caminade C, Upadhyayula SM. Dengue burden in India: recent trends and importance of climatic parameters. Emerg. Microbes Infect. 2017;6(1):e70.
Crossref - National Centre for Vector Borne Disease Control. Dengue situation in India [Internet]. New Delhi: Ministry of Health and Family Welfare, Government of India. Available from: https://ncvbdc.mohfw.gov.in/index4.php?lang=1&level=0&linkid=431&lid=3715
- Altamish M, Khan M, Baig MS, et al. Therapeutic Potential of Medicinal Plants against Dengue Infection: A Mechanistic Viewpoint. ACS Omega. 2022;7(28):24048-24065.
Crossref - Ali F, Chorsiya A, Anjum V, Khasimbi S, Ali A. A systematic review on phytochemicals for the treatment of dengue. Phytother Res. 2021;35(4):1782-1816.
Crossref - Roy SK, Bhattacharjee S. Dengue virus: epidemiology, biology, and disease aetiology. Can J Microbiol. 2021;67(10): 687-702.
Crossref - Khan MB, Yang ZS, Lin CY, et al. Dengue overview: An updated systemic review. J Infect Public Health. 2023;16(10):1625-1642.
Crossref - Guzman MG, Halstead SB, Artsob H, et al. Dengue: A continuing global threat. Nat Rev Microbiol. 2010;8(12 Suppl):S7-S16.
Crossref - Saleh MSM, Kamisah Y. Potential Medicinal Plants for the Treatment of Dengue Fever and Severe Acute Respiratory Syndrome-Coronavirus. Biomolecules 2020;11(1):42.
Crossref - Dhiman M, Sharma L, Dadhich A, Dhawan P, Sharma MM. Traditional Knowledge to Contemporary Medication in the Treatment of Infectious Disease Dengue: A Review. Front Pharmacol. 2022;13:750494.
Crossref - Wint W, Jones P, Kraemer M, Alexander N, Schaffner F. Past, present and future distribution of the yellow fever mosquito Aedes aegypti: The European paradox. Sci Total Environ. 2022;847:157566.
Crossref - Mathew A, Rothman A.L. Understanding the contribution of cellular immunity to dengue disease pathogenesis. Immunol Rev. 2008;225(1):300–313.
- Nanaware N, Banerjee A, Mullick Bagchi S, Bagchi P, Mukherjee A. Dengue virus infection: a tale of viral exploitations and host responses. Viruses. 2021;13(10):1967.
Crossref - Guzman MG, Harris E. Dengue. Lancet. 2015;385(9966):453-465. doi: 10.1016/S0140-6736(14)60572-9
- World Health Organization. Dengue guidelines for diagnosis, treatment, prevention and control: new edition [Internet]. Geneva: World Health Organization; 2009. Available from: https://www.who.int/publications/i/item/9789241547871
- Patel SK, Surve J, Parmar J, Ahmed K, Bui FM, Al-Zahrani FA. Recent Advances in Biosensors for Detection of COVID-19 and Other Viruses. IEEE Rev Biomed Eng. 2023;16:22-37.
Crossref - Kostyusheva A, Brezgin S, Babin Y, et al. CRISPR-Cas systems for diagnosing infectious diseases. Methods. 2022;203:431-446.
Crossref - Zeyaullah M, Muzammil K, AlShahrani AM, et al. Preparedness for the dengue epidemic: vaccine as a viable approach. Vaccines. 2022;10(11):1940.
Crossref - Schaefer TJ, Panda PK, Wolford RW. Dengue Fever. [Updated 2024 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
- Tully D, Griffiths CL. Dengvaxia: the world’s first vaccine for prevention of secondary dengue. Ther Adv Vaccines Immunother. 2021;9:25151355211015839.
Crossref - Pal D, Lal P. Herbal Drugs and Medicinal Plants in Controlling and Treatment of Diseases Caused by Dengue Virus (DEN-1 & 2): Ethnopharmacology, Chemistry, Clinical and Preclinical Studies. In: Pal D, ed. Anti-Viral Metabolites from Medicinal Plants. Reference Series in Phytochemistry. Springer, Cham. 2023.
Crossref - Abd Kadir SL, Yaakob H, Mohamed Zulkifli R. Potential anti-dengue medicinal plants: a review. J Nat Med. 2013;67(4):677-689.
Crossref - Hasani SJ, Sgroi G, Esmaeilnejad B, et al. Recent advances in the control of dengue fever using herbal and synthetic drugs. Heliyon. 2025;11(3):e41939.
Crossref - Mehta SK, Pradhan RB. Phytochemicals in antiviral drug development against human respiratory viruses. Drug Discov Today. 2024;29(9):104107.
Crossref - Behl T, Rocchetti G, Chadha S, et al. Phytochemicals from Plant Foods as Potential Source of Antiviral Agents: An Overview. Pharmaceuticals. 2021;14(4):381.
Crossref - Ghildiyal R, Prakash V, Chaudhary VK, Gupta V, Gabrani R. Phytochemicals as Antiviral Agents: Recent Updates. In: Swamy, M, ed. Plant-derived Bioactives. Springer, Singapore. 2020;279-295.
Crossref - Adeosun WB, Loots DT. Medicinal Plants against Viral Infections: A Review of Metabolomics Evidence for the Antiviral Properties and Potentials in Plant Sources. Viruses. 2024;16(2):218.
Crossref - Vats P, Rolta R, Salaria D, et al. Comparative analysis of phytocompounds and repurposed drugs against dengue virus serotypes employing an in silico study. Sci Rep. 2025;15(1):44405.
Crossref - Alagarasu K, Patil P, Kaushik M, et al. In Vitro Antiviral Activity of Potential Medicinal Plant Extracts Against Dengue and Chikungunya Viruses. Front Cell Infect Microbiol. 2022;12:866452.
Crossref - Lim SYM, Chieng JY, Pan Y. Recent insights on anti-dengue virus (DENV) medicinal plants: review on in vitro, in vivo and in silico discoveries. All Life. 2020;14(1):1-33.
Crossref - Rehman B, Ahmed A, Khan S, Saleem N, Naseer F, Ahmad S. Exploring plant-based dengue therapeutics: from laboratory to clinic. Trop Dis Travel Med Vaccines. 2024;10:23.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.