


ISSN: 0973-7510
E-ISSN: 2581-690X
As an obligate intracellular, Gram-negative microorganism, Chlamydia trachomatis represents a prevalent sexually transmitted pathogen. It disproportionately impacts women of reproductive age, resulting in a spectrum of reproductive health complications. Despite the significant public health implications of this infection, its epidemiological characteristics in India remain inadequately documented, with a limited number of studies conducted. Endocervical swabs and serum samples were collected from 75 participants. A solid-phase immunochromatographic assay was employed for the detection of antigens within the endocervical specimens. In accordance with the manufacturer’s protocols, an enzyme immunoassay was utilized to ascertain the presence of IgM, IgG, and IgA antibodies in the serum specimens. For the purposes of this investigation, we recruited 75 patients exhibiting various symptoms indicative of lower genital tract infections. Among the symptomatic cohort, thirteen cases tested positive for chlamydia antibodies. Notably, two of these thirteen patients exhibited the presence of both IgG and IgA antibodies. Chlamydia antibodies were identified in 17.3% (13/75) of the symptomatic patients, as determined by the results of the antibody detection assays. In relation to patients diagnosed with cervicitis, 61.5% tested positive and 19.4% tested negative for chlamydia antibodies (P value = 0.0040).
Chlamydia trachomatis, Reproductive Tract Infections, Endocervical Swab, Cervicitis
As one of the most frequently reported sexually transmitted infections, Chlamydia trachomatis (CT) represents a considerable public health challenge, predominantly affecting reproductive-aged women and causing diverse reproductive complications.1,2 In India, limited studies have reported CT prevalence rates of 3%-45% among pregnant women attending antenatal clinics and 18%-30% among individuals with sexually transmitted diseases.3-6 A proportion of CT-infected women remain asymptomatic, symptomatic cases may present with urethritis, cervicitis, or acute salpingitis and are more likely to experience serious reproductive complications, including ectopic pregnancy, infertility, and pelvic inflammatory disease (PID).7-9 Negative obstetric outcomes, such as preterm labor, low birth weight, and premature rupture of membranes, have been linked to CT infection in pregnant women.10 Despite long being considered the diagnostic gold standard, the efficacy of endocervical swab culture is sensitive to variables. These include collection technique, transport and storage conditions, and swab material, with some (e.g., calcium alginate and dacron-on-plastic) proving toxic to cells and others (e.g., cotton-on-wood) being less inhibitory. A shift has occurred towards the more common use of non-culture-based diagnostic techniques for CT detection, notably direct immunofluorescence, enzyme immunoassays, and PCR.11 Early diagnosis followed by appropriate treatment can effectively prevent long-term complications,2 highlighting the need for timely identification and management of at-risk individuals using anti-chlamydial therapy.4 This study was conducted to address the scarcity of data on the epidemiology of CT infections in the Indian context.
This prospective cohort investigation was rigorously executed within the Department of Microbiology at Mahatma Gandhi Medical College and Research Institute, Puducherry, over the period from December 2010 to June 2012. Institutional Human Ethics Committee (IHEC) approval was obtained. The primary objective of the study was to yield comprehensive data regarding the prevalence and immunological response to Chlamydia trachomatis among symptomatic women, thereby addressing a notable deficiency in regional epidemiological literature.
Participants
A total of 75 women presenting clinical manifestations suggestive of lower genital tract infection were recruited subsequent to thorough informed consent protocols. Each participant underwent an exhaustive interview and clinical examination, during which intricate demographic data, extensive medical and sexual histories, risk factor evaluations for C. trachomatis infection, obstetric histories (when applicable), and any pertinent comorbid conditions were meticulously recorded utilizing a structured proforma. Findings from the physical examination, encompassing general, systemic, pelvic, and speculum evaluations, were systematically documented to facilitate the correlation of clinical presentations with laboratory results.
Specimen collection and processing
Endocervical swabs were procured by initially removing excess mucus from the exocervix with a sterile swab. Subsequently, a second sterile swab was introduced into the endocervical canal beyond the squamocolumnar junction, gently rotated for 15-20 seconds to ensure adequate sampling, and withdrawn with care to avert contamination from vaginal or exocervical cells. The obtained swabs were immediately placed in sterile transport tubes and preserved at ambient temperature for a duration of up to one hour prior to processing. This standardized methodology ensured the optimal preservation of antigen integrity for subsequent testing.
Antigen detection
The identification of chlamydial antigen was executed employing the SD BIOLINE Chlamydia rapid immunochromatographic assay (Korea), which utilizes a solid-phase chromatographic technique predicated on antigen-antibody interactions. The test apparatus detects the presence of C. trachomatis antigen via the formation of a coloured test line, signifying a positive outcome. A solitary control band indicates a negative result, while the absence of a control band renders the test invalid. Results were visually interpreted with precision at 15 minutes to ensure consistency and reliability across all samples.
Serum sample collection and antibody detection
Venous blood samples (5 ml) were collected aseptically, subjected to centrifugation at 2000 rpm for 3 minutes, and the resultant serum was aliquoted into labelled vials and stored at -20 °C until further analysis. Serological assessment for antibodies against C. trachomatis (IgG, IgA, IgM) was performed utilizing the NOVALISA ELISA kit (Germany), adhering strictly to the detailed manufacturer’s protocol. The assay operates on an enzyme-linked immunosorbent principle wherein microtiter wells pre-coated with chlamydial antigen bind specific antibodies present in the patient serum. Following incubation and washing phases, bound antibodies were detected utilizing horseradish peroxidase-conjugated secondary antibodies, with colour development quantified as optical density at 450 nm. Results were interpreted relative to a calibrated cut-off value, facilitating categorization into positive, negative, or equivocal (gray zone), with equivocal results subjected to retesting for confirmation.
Statistical analysis
Descriptive statistics were utilized to aggregate clinical characteristics, laboratory results, and demographic information of patients. Absolute frequencies and percentages were employed to clarify categorical data, while the mean ± standard deviation was utilized to describe continuous variables. In order to compare continuous variables across different groups, Student’s t-test was applied when the data conformed to a normal distribution; conversely, suitable non-parametric alternatives were employed when this assumption was not met. The chi-square test, which is occasionally referred to as Fisher’s exact test, was employed to investigate the relationships between categorical variables. To identify independent predictors and control for confounding variables, multivariate logistic regression was employed to further explore potential risk factors that were identified in the univariate analysis. All statistical analyses were conducted using standardized software, and a P-value of less than 0.05 was regarded as statistically significant to ensure comprehensive data interpretation.
The study comprised 75 cases in all, all of which had different symptoms that pointed to a lower genital tract infection. Table 1 provides a summary of the research patients’ demographic information.
Table (1):
Demographic details of the study patients
| Parameter | Symptomatic patients (n = 75) |
|---|---|
| Age (mean ± SD) | 29.4 ± 6.3 (20-48) |
| Age at marriage | 20.7 ± 3.5 (15-32) |
| No. of years after marriage | 9.17 ± 6.9 (0-26) |
| Marital status | |
| Married | 68 (90.7%) |
| Second partner | 1 (1.3%) |
| Widow | 2 (2.7%) |
| Single | 4 (5.3%) |
Detection of Chlamydia antigen and antibodies
Table 2 provides a summary of the antigen and antibody (IgM/IgG/IgA) detection test results. None of the women with symptoms tested positive for the Chlamydia antigen.
13 patients tested positive for chlamydia antibodies. Of these 13 patients, two had both IgG and IgA antibody positive results.
Table (2):
Results of Chlamydia antigen and antibodies detection tests
| Symptomatic patients (n = 75) No. of positives | |
|---|---|
| Antigen | 0 |
| Antibody | |
| IgG | 7 |
| IgA | 3 |
| IgM | 5 |
Prevalence of chlamydia infection
Patients positive for one or more types of chlamydia antibodies were considered to be infected with chlamydia. Therefore, 17.3% (13/ 75) of the symptomatic cases had a chlamydia infection.
Comparison of the chlamydia antibody positive and negative groups
The symptomatic patients were separated into groups that were chlamydia antibody positive and chlamydia antibody negative group based on the findings of the antibody detection tests. The primary diagnosis, risk factors, symptoms/signs and investigations of these two groups were compared subsequently.
Primary diagnosis
A comparison of the primary diagnosis of the antibody positive and negative patients is shown in Table 3. 61.5% of patients positive for chlamydia antibodies had cervicitis, while only 19.4% of those negative for chlamydia antibodies had cervicitis (P-value 0.0040). This suggests a significant association between cervicitis and chlamydia infection.
Table (3):
Primary diagnosis of the symptomatic patients
Primary diagnosis |
Chlamydia antibody positive (n = 13) |
Chlamydia antibody negative (n = 62) |
P-value |
|---|---|---|---|
Cervicitis |
8 (61.5%) |
12 (19.4%) |
0.0040 |
PID |
3 (23.1%) |
31 (50.0%) |
0.1425 |
Infertility |
1 (7.7%) |
19 (30.6%) |
0.1646 |
BOH |
1 (7.7%) |
0 |
0.1733 |
Risk factors for Chlamydia infection
Table 4 provides a summary of the possible risk variables for chlamydia infections that were examined in our investigation. The risk of chlamydia antibody positive was found to be 13.25 times higher for those aged ≤25. Similarly, it was shown that the first three years of sexual engagement were linked to a higher chance of testing positive for chlamydia antibodies.
Table (4):
Risk factors for Chlamydia trachomatis infection
No. |
Risk factor |
Positive (n = 13) (%) |
Negative (n = 62) (%) |
Relative risk (95% confidence limits) |
P-value |
|---|---|---|---|---|---|
1. |
Age ≤25 yrs |
11 (84.6) |
11 (17.7) |
13.25 (3.20-54.94) |
|
2. |
Age at marriage (mean ± SD) |
21.4 ± 2.4 |
20.5 ± 3.6 |
– |
0.4050 |
3. |
Sexually active period ≤3 yrs* |
11 (84.6) |
10 (16.1) |
14.14 (3.42-58.50) |
|
4. |
Multiple sexual partners |
1 (7.7%) |
0 |
6.17 (3.67-10.35) |
0.1733 |
* Sexually active period was considered as the number of years after marriage
Symptoms and signs
A comparison of the symptoms and signs of the antibody positive and negative patients is shown in Table 5. Cervicitis and mucopurulent cervical discharge were the two symptoms found to be significantly associated with chlamydia antibody positivity.
Table (5):
Comparison of Symptoms and Signs
No. |
Symptoms/signs |
Chlamydia Antibody positive (n = 13) |
Chlamydia Antibody negative (n = 62) |
P-value |
|---|---|---|---|---|
1. |
Fever |
0 |
2 |
1.0000 |
2. |
Presence of vaginal discharge |
12 |
51 |
0.6790 |
3. |
Foul smelling discharge |
4 |
6 |
0.0643 |
4. |
Dyspareunia |
5 |
23 |
1.0000 |
5. |
Perineal itching |
4 |
17 |
1.0000 |
6. |
Dysuria |
3 |
1 |
0.7439 |
7. |
Abdominal/pelvic pain |
5 |
23 |
1.0000 |
8. |
Mucopurulent Cervical discharge |
5 |
6 |
0.0186 |
9. |
Cervical erosion |
3 |
7 |
0.3637 |
10. |
Cervicitis |
8 |
13 |
0.0059 |
11. |
Adnexa tenderness |
1 |
11 |
0.6790 |
12. |
Abnormal menstrual history |
4 |
17 |
1.0000 |
Investigations
Table 6 displays a comparison of the results of several tests conducted on patients who tested positive and negative for antibodies. Chlamydia antibody positivity was shown to be substantially correlated with the presence of chronic cervicitis in USG.
Table (6):
Comparison of Investigations
| No. | Investigation | Chlamydia antibody positive (n = 13) | Chlamydia antibody Negative (n = 62) | P-value |
|---|---|---|---|---|
| 1. | Papanicolaou smear | |||
| Inflammatory | 12 | 51 | 0.6790 | |
| Normal | 1 | 11 | ||
| 2. | Trans Vaginal Sonogram | |||
| Chronic cervicitis | 8 | 14 | 0.0170 | |
| PID | 4 | 31 | ||
| Normal | 1 | 17 | ||
| 3. | Hysterosalpingogram | |||
| Abnormal | 0 | 1 | 1.0000 | |
| Normal | 13 | 61 | ||
The prevalence rate of CT infection based on antibody detection among symptomatic patients was 17.3% (13/75). Our findings were consistent with another study, which found a frequency of 14% in symptomatic people and 21.8% in symptomatic STD patients.12 According to few other studies, the prevalence of CT in women with PID, infertility, or STDs ranged from 15%-60%.13 With reference to Table 1, the mean age group of symptomatic cases was 29.4 ± 6.3 (range 20-48), age at marriage was 20.7 ± 3.5 (range 15-32), number of years after marriage 9.17 ± 6.9 (range 0-26). With reference to Table 3, 61.5% Patients positive for Chlamydia antibody had cervicitis as shown in Figure 1, while only 19.4% of those negative for Chlamydia antibody had cervicitis (P-value 0.0040) which suggests significant association between cervicitis and Chlamydia infection.
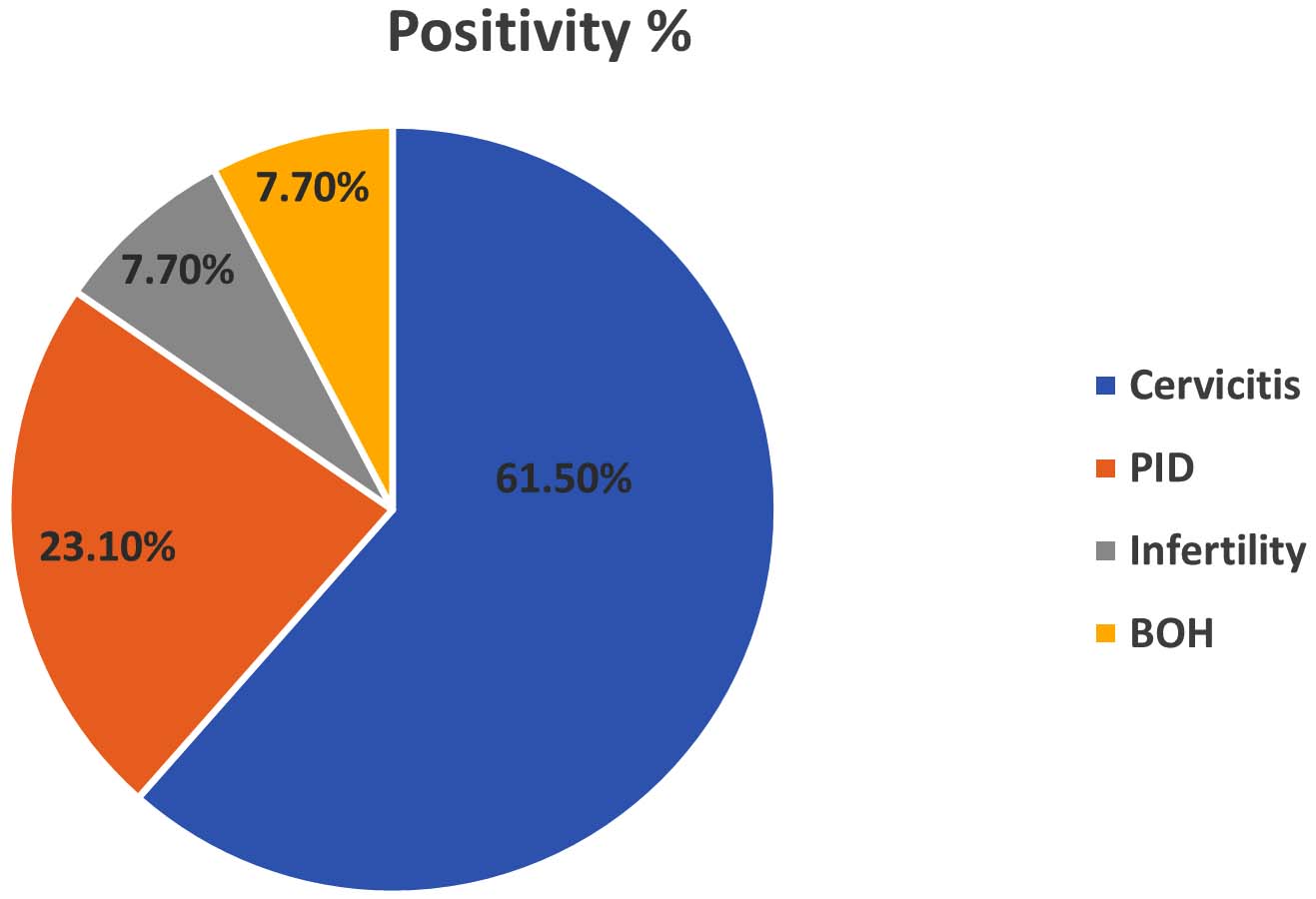
Figure 1. Positivity percentage based on primary diagnosis of symptomatic patients
Another study confirmed the previous results, citing CT infection as the primary cause of mucopurulent cervicitis, which accounts for half of the 1 million PID cases reported in the United States annually.14
In our study, 23.1% of patients positive for Chlamydia antibody had PID and 50% of patients negative for Chlamydia antibody had PID. Another study quotes CT as an important cause of PID and the rate of untreated infection in short term PID diagnosis ranging from 2%-4.5%.15
Regarding infertility, 30.6% of patients negative for Chlamydia antibody had infertility compared to 7.7% of Chlamydia antibody positive cases. Study done by Kalantar et al. has similar findings with no evidence of organisms in infertile women.16 In contrary, few researchers report that CT plays an important role in infertility, In a study 25.4%, 45.3% of seropositivity was seen in infertile women indicating higher prevalence.17,18
With reference to Table 4, Potential risk factors studied were age <25 years, age at marriage, sexually active period less than or equal to three years and multiple sexual partners. In our study, age <25 years was found to be associated with 13.25 times increased risk for Chlamydia CT antibody positivity.
Among the thirteen Chlamydia-positive patients, 69.2% were between the ages of
20 and 30, and 30.8% between the ages of 30 and 40, with no cases older than 40, indicating a substantial correlation with reproductive age. The first three years of sexual activity was associated with a 14.14 fold increased risk of Chlamydia trachomatis (CT) antibody positivity (P < 0.0001) and multiple sexual partners carried a 6.17-fold higher risk. The average marriage age was not significantly different between antibody-positive (21.4 ± 2.4) and antibody-negative groups (20.5 ± 3.6). These findings are in line with another study that emphasizes young age, early sexual activity, and multiple partners as key risk factors for CT infection.19
With reference to Tables 5 and 6, Cervicitis (P = 0.0059) and mucopurulent cervical discharge (P = 0.0186) were significantly associated with Chlamydia positivity, consistent with previous reports citing cervicitis and mucopurulent discharge as common features. Menstrual irregularities and other symptoms such as fever, dyspareunia, and pelvic pain were not significantly associated. With reference to Table 6, on transvaginal sonography, chronic cervicitis was significantly associated with CT antibody positivity (P = 0.0170). PAP smear results were inflammatory in 12 individuals and normal in one in the antibody-positive group; similar patterns were observed in the antibody-negative group.
Antibody detection by ELISA showed positivity for IgG in 7 patients (54%), IgM in 5 (38%), and IgA in 3 (23%), with two patients positive for both IgG and IgA (Figure 2).
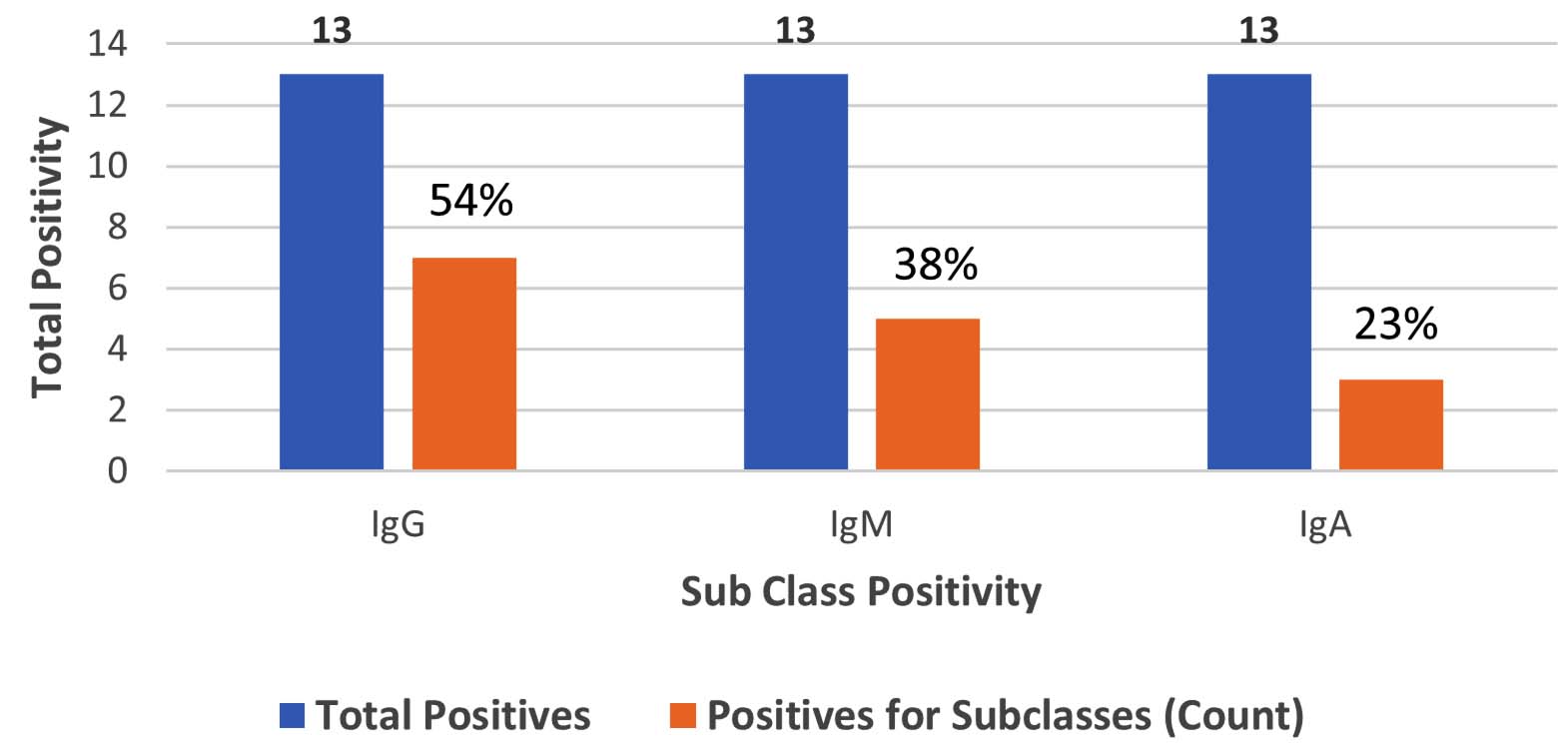
Figure 2. Total positives, Positives for subclasses by immunoglobulins
According to several studies high titres of IgM and IgG are associated with recurrent spontaneous abortion and preterm delivery.20-24 Another study reveals a correlation between a high titre of IgG and tubal factor infertility, ectopic pregnancy.25
Antigen detection using a rapid immunochromatographic test (ICT) was negative in all symptomatic patients, likely due to the poor sensitivity of the kit used. Similar low positivity rates with ICT have been reported in other studies, emphasizing the need for good quality assurance. Additionally, they may result in false positives because of cross-reactivity with other microorganisms.26,27 In cases of chronic or persistent infection, Nucleic acid amplification test (NAAT) was often positive while antigen detection and culture remained negative, likely due to lower bacterial load and viability.28,29
The study outcomes revealed a remarkably increased occurrence of Chlamydia trachomatis infection in symptomatic individuals (17.3%). Individuals aged 25 years or younger, as well as those in the initial three years of sexual activity, exhibited a significant correlation with an augmented risk of chlamydia antibody positivity. Cervicitis showed a significant association with CT infection, and specifically, cervicitis along with mucopurulent cervical discharge were identified as the two symptoms most strongly linked to chlamydia antibody positivity. Additionally, the presence of chronic cervicitis on transvaginal sonogram was significantly associated with CT antibody positivity. In contrast, rapid immunochromatographic tests (ICT) for detecting CT antigen from endocervical samples were found to be less sensitive compared to enzyme immunoassays (EIA). Finally, antibody detection by ELISA emerged as a convenient and practical approach for diagnosing CT infection in this setting. The primary constraint of this investigation is the limited sample size. An expanded sample size could not be acquired due to financial constraints. The determination of antibody titre was not achievable, as it was impractical within this particular framework.
ACKNOWLEDGMENTS
The authors would like to express their heartfelt gratitude to the Mahatma Gandhi Medical College and Research Institute, Puducherry, for providing the necessary assistance and facilities to complete this study. The authors also recognise the important efforts and cooperation of all healthcare professionals who participated in this study.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
This study was conducted in accordance with the guidelines and approval of the Institutional Human Ethics Committee (IHEC), Mahatma Gandhi Medical College and Research Institute, Puducherry, India.
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Rodrigues R, Sousa C, Vale N. Chlamydia trachomatis as a current health problem: challenges and opportunities. Diagnostics. 2022;12(8):1795.
Crossref - Leon SR, Konda KA, Klausner JD, et al. Chlamydia trachomatis infection and associated risk factors in a low-income marginalized urban population in coastal Peru. Rev Panam Salud Publica. 2009;26(1):39-45.
Crossref - Alexander R, Mathai E, Nayyar V, Mathew M, Jasper P. Low prevalence of chlamydial endocervical infection in antenatal South Indian women. Genitourin Med. 1993;69(3):240-241.
Crossref - Sawhney MP, Batra RB. Chlamydia trachomatis seropositivity during pregnancy. Indian J Dermatol Venereol Leprol. 2003;69(6):394-395.
- George JA, Panchatcharam TS, Paramasivam R, Balasubramanian S, Chakrapani V, Murugan G. Evaluation of diagnostic efficacy of PCR methods for Chlamydia trachomatis infection in genital and urine specimens. Jpn J Infect Dis. 2003;56(3):88-92.
- Joyee AG, Thyagarajan SP, Reddy EV, Venkatesan C, Ganapathy M. Genital chlamydial infection in STD patients: its relation to HIV infection. Indian J Med Microbiol. 2005;23(1):37-40.
Crossref - Stamm WE. Chlamydia trachomatis infections: progress and problems. J Infect Dis. 1999;179(Suppl 2):S380-S383.
Crossref - Rours GIJG, Duijts L, Moll HA, et al. Chlamydia trachomatis infection during pregnancy associated with preterm delivery: a population-based prospective cohort study. Eur J Epidemiol. 2011;26(6):493-502.
Crossref - Malik A, Jain S, Hakim S, Shukla I, Rizvi M. Chlamydia trachomatis infection and female infertility. Indian J Med Res. 2006;123(6):770-775.
- den Heijer CDJ, Hoebe CJPA, Driessen JHM, et al. Chlamydia trachomatis and the risk of pelvic inflammatory disease, ectopic pregnancy, and female infertility: a retrospective cohort study among primary care patients. Clin Infect Dis. 2019;69(9):1517-1525. doi: 10.1093/cid/ciz429. Published correction appears in Clin Infect Dis. 2020;70(11):2459.
Crossref - Black CM. Current methods of laboratory diagnosis of Chlamydia trachomatis infections. Clin Microbiol Rev. 1997;10(1):160-184.
Crossref - Alexiou ZW, Hoenderboom BM, Hoebe CJPA, et al. Prevalence and risk factors for Chlamydia trachomatis seropositivity and seropersistence among women: A prospective cohort study. PLoS One. 2025;20(8):e0328449.
Crossref - Land JA, Van Bergen JEAM, Morre SA, Postma MJ. Epidemiology of Chlamydia trachomatis infection and cost-effectiveness of screening. Hum Reprod Update. 2010;16(2):189-204.
Crossref - Hassan QU, Mufti AH, Mufti S. Seroprevalence of Chlamydia Trachomatis infection in Kashmiri women of reproductive age with mucopurulent cervicitis, infertility and ectopic pregnancy – a hospital based study. The New Indian Journal of OBGYN. 2024;11(1):46-50.
- Gigli S, Gennarini M, Ninkova RV, et al. Cross-Sectional Imaging of pelvic inflammatory Disease: diagnostic pearls and pitfalls on CT and MR. Diagnostics. 2025;15(16):2001.
Crossref - Kalantar SM, Kazemi MJ, Sheikhha MH, Aflatoonian A, Kafilzadeh F. Detection of Chlamydia trachomatis in infertile couples. J Fertil Steril. 2007;1(2):79-84.
Crossref - Sharma K, Aggarwal A, Arora U. Seroprevalence of Chlamydia trachomatis in infertility. Indian J Med Sci. 2002;56(5):216-217.
- Surana A, Nirwan PS, Gaur S. Seroprevalence Of Primary Infertility and Acute Pelvic Inflammatory Disease Caused by Chlamydia in Ajmer Region. Natl J Community Med. 2011;2(03):487-91.
- Keegan MB, Diedrich JT, Peipert JF. Chlamydia trachomatis infection: screening and management. J Clin Outcomes Manag. 2014;21(1):30-38.
- Tang W, Mao J, Li KT, et al. Pregnancy and fertility-related adverse outcomes associated with Chlamydia trachomatis infection: a global systematic review and meta-analysis. Sex Transm Infect. 2020;96(5):322-329.
Crossref - Xia Q, Wang T, Xian J, et al. Relation of Chlamydia trachomatis infections to ectopic pregnancy. Medicine.2020;99(1):e18489.
Crossref - Olson-Chen C, Balaram K, Hackney DN. Chlamydia trachomatis and Adverse Pregnancy Outcomes: Meta-analysis of Patients With and Without Infection. Matern Child Health J. 2018;22(6):812-821.
Crossref - He W, Jin Y, Zhu H, Zheng Y, Qian J. Effect of Chlamydia trachomatis on adverse pregnancy outcomes: a meta-analysis. Arch Gynecol Obstet. 2020;302(3):553-567.
Crossref - Ahmadi A, Ramazanzadeh R, Sayehmiri K, Sayehmiri F, Amirmozafari N. Association of Chlamydia trachomatis infections with preterm delivery; a systematic review and meta-analysis. BMC Pregnancy and Childbirth. 2018;18(1):240.
Crossref - Zuo Y, Jiang TT, Teng Y, Han Y, Yin YP, Chen XS. Associations of Chlamydia trachomatis serology with fertility-related and pregnancy adverse outcomes in women: a systematic review and meta-analysis of observational studies. EBioMedicine. 2023;94:104696.
Crossref - Li SL, Lin HL, Mi HF, et al. Evaluation of the diagnostic performance of an immunochromatographic test for Chlamydia trachomatis. Pract Lab Med. 2024;40:e00412.
Crossref - Serafini A, Mei C, Mattei R, De Santi M, Brandi G. Comparison of real-time PCR assay with a commercial rapid test based on the immunochromatographic principle for the detection of Chlamydia trachomatis in seminal fluid and urine specimens. Infez Med. 2021;29(4):562-567.
Crossref - Sharma V, Khan MM. Current Progress and Future Perspective of Chlamydia trachomatis Infection: A Rising Threat to Women Health. Curr Microbiol. 2025;82(7):314.
Crossref - Greer L, Wendel GD. Rapid Diagnostic Methods in Sexually Transmitted Infections. Infect Dis Clin North Am. 2008;22(4):601-617.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.