


ISSN: 0973-7510
E-ISSN: 2581-690X
Pyomyositis and osteomyelitis are rare but serious infections of soft tissues and the musculoskeletal system in infants, particularly when caused by Methicillin-resistant Staphylococcus aureus (MRSA). We present a case involving MRSA pyomyositis and osteomyelitis following intramuscular hepatitis B vaccination in a 30 day-old male. The infant exhibited increasing swelling and pain in the left thigh three days post-vaccination. Imaging revealed an intramuscular abscess and early signs of osteomyelitis. Cultures from pus and tissue confirmed MRSA. The infant was treated with surgical drainage, debridement, and intravenous vancomycin, leading to a positive recovery. This case highlights the critical need for strict aseptic procedures during vaccination and early recognition and management of rare post-vaccination infections in infants to prevent serious outcomes.
Methicillin-resistant Staphylococcus aureus, Pyomyositis, Osteomyelitis, Vaccination, Infant
Infant infections continue to be a major cause of illness and death worldwide, especially in low- and middle-income countries. Among these, soft tissue and musculoskeletal infections in infants are relatively uncommon but can develop quickly and lead to life-threatening complications. Diagnosis is often delayed because of nonspecific symptoms, infants’ inability to express their discomfort, and limited diagnostic tools during early life. One rare but often underrecognized musculoskeletal infection in infants is pyomyositis, a pus-forming infection of skeletal muscle that may progress to systemic sepsis and increased morbidity when diagnosis and treatment are delayed.1,2 Pyomyositis in infants is typically caused by Staphylococcus aureus, with Methicillin-resistant Staphylococcus aureus (MRSA) increasingly identified as a causative agent.3 MRSA is a significant pathogen due to its resistance to β-lactam antibiotics and its association with both community-acquired and healthcare-associated infections.4 In infants, MRSA can cause invasive musculoskeletal infections through hematogenous dissemination or direct inoculation following invasive procedures.5,6
Immunization is an essential public health approach, and intramuscular injections are commonly used to deliver vaccines to infants. However, on rare occasions, incorrect injection techniques, contamination of injection materials, or weakened immune systems in the host can increase the risk of local infectious complications in infants. Although adverse events after immunization are usually mild and resolve on their own, serious soft tissue infections like pyomyositis and osteomyelitis are uncommon but significant complications that require increased vigilance and immediate treatment.5
Case presentation
A 30 day-old male infant, born at term, was referred to Dr. Soetomo General Hospital with progressive swelling and pain in the left thigh. The symptoms began three days after receiving the birth dose of intramuscular hepatitis B (HB-0) vaccine at a public health center. The swelling gradually increased in size and was accompanied by intermittent fever and irritability. The infant had been previously taken to a public health center multiple times and received compounded oral antipyretic medication for symptomatic treatment of fever; however, the symptoms persisted, and no documentation of neonatal sepsis evaluation or intravenous antibiotic therapy was available. The patient was initially brought to a private hospital, then referred to a secondary care facility, and was ultimately transferred to our hospital several weeks after symptom onset because of worsening local findings and suspicion of deep tissue infection.
On admission, the patient was afebrile, alert, and breastfeeding well. Physical examination revealed marked swelling, tenderness, and warmth in the left thigh without erythema. Laboratory results showed leukocytosis (WBC 45,700 µL), thrombocytosis (platelets 596,000 µL), anemia (Hb 10.3 g/dL), and elevated inflammatory markers (CRP 7.8 mg/dL, ESR 108 mm/hour). An ultrasound of the left thigh showed diffuse thickening of the anterior compartment muscles extending from the proximal to distal femur, involving the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius, with evidence of intramuscular abscess formation mainly in the left vastus lateralis muscle. Periosteal thickening and cortical irregularities were also observed along the anterior femoral shaft, suggesting early osteomyelitis. The findings were consistent with pyomyositis and early osteomyelitis.
The patient underwent surgery on hospital day 8. Under general anesthesia, an ultrasound-guided aspiration was performed, yielding 10 cc of purulent, blood-streaked material. Incision and drainage via a lateral femoral approach were carried out, followed by extensive debridement and wound irrigation using normal saline and povidone-iodine. Superficial pus, deep pus, and tissue samples were sent for Gram staining and aerobic culture. Culture on blood and chocolate agar from all three specimens, which included superficial pus, deep pus, and tissue, showed white, round, smooth, and opaque colonies exhibiting beta-hemolysis. No bacterial growth was observed on MacConkey agar from any of the specimens. Gram stains of all three samples consistently revealed Gram-positive cocci (Figures 1, 2 and 3).
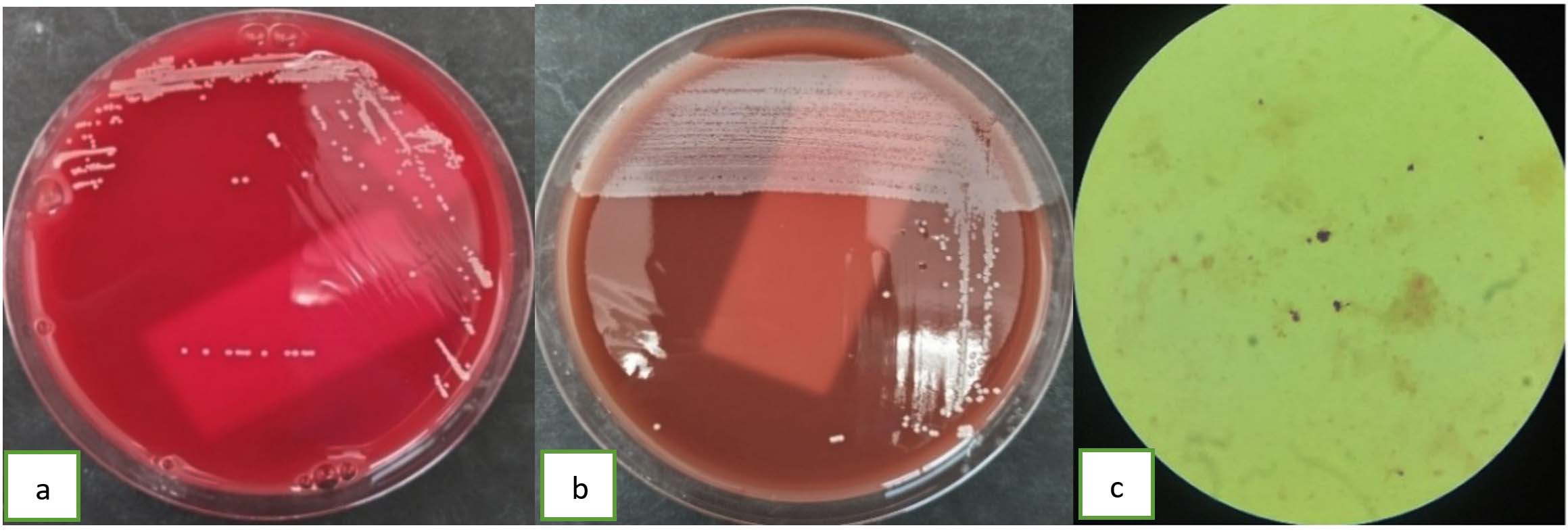
Figure 1. (a). Staphylococcus aureus in blood agar (b). Staphylococcus aureus in chocolate agar, and (c). Staphylococcus aureus in a Gram stain from the patient’s superficial pus cultures
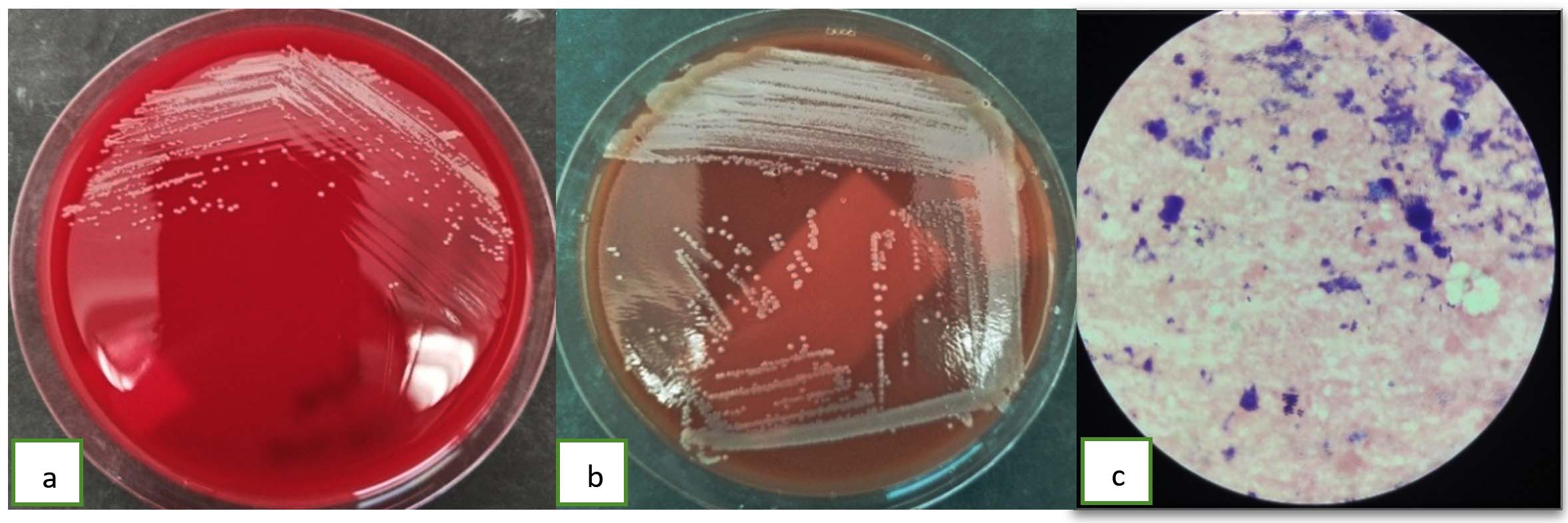
Figure 2. (a). Staphylococcus aureus in blood agar (b). Staphylococcus aureus in chocolate agar, and (c). Staphylococcus aureus in a Gram stain from the patient’s deep pus cultures
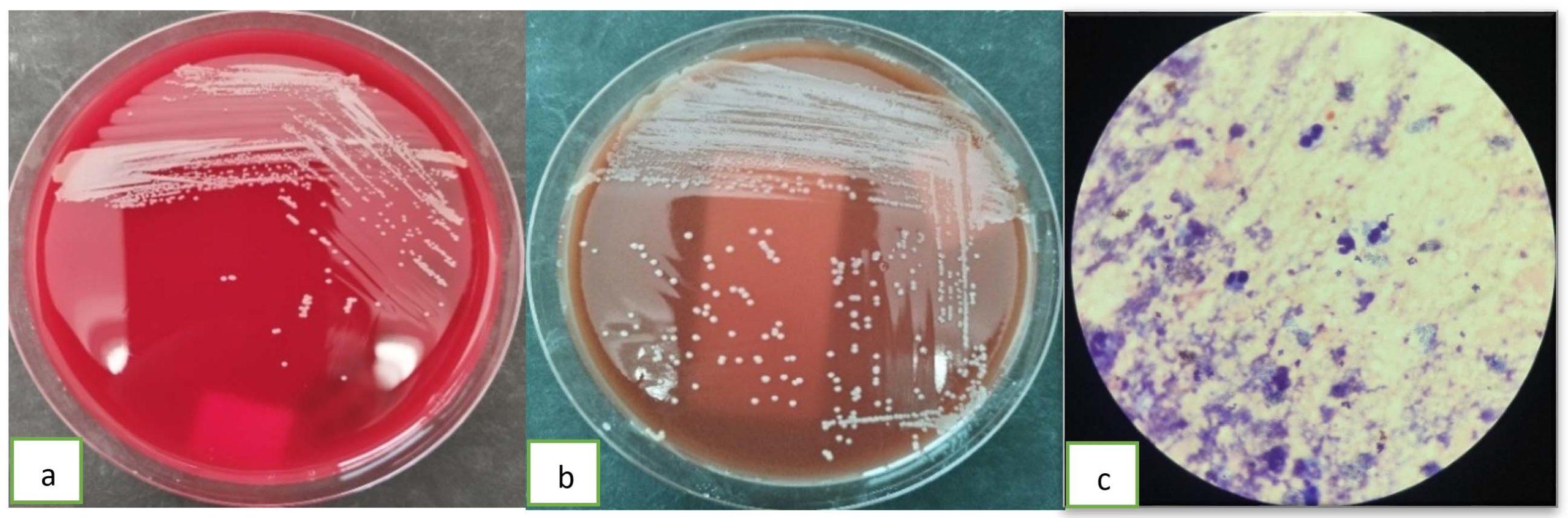
Figure 3. (a). Staphylococcus aureus in blood agar (b). Staphylococcus aureus in chocolate agar, and (c). Staphylococcus aureus in a Gram stain from the patient’s tissue cultures
Identification of the microorganism and antimicrobial susceptibility testing were performed using the VITEK 2 automated system (BioMerieux, Hazelwood, MO, USA). A Penrose drain was placed, and the wound was closed in layers. Postoperatively, the patient was started on empirical intravenous cefoperazone-sulbactam. On postoperative day 2 (hospital day 10), culture results from all three specimens (tissue, superficial pus, and deep pus) identified Methicillin-resistant Staphylococcus aureus (MRSA). Based on these results, intravenous vancomycin was initiated as definitive therapy. The patient remained clinically stable after surgery, with no further fever and improvement in local inflammation. A single packed red blood cell (PRBC) transfusion (40 mL) was given to address anemia. The patient continued to improve under multidisciplinary care. He was discharged on hospital day 18 with signs of gradual clinical improvement, including reduced thigh swelling and sustained absence of fever.
Post-vaccination infection is a rare but serious complication, particularly when involving resistant pathogens such as Methicillin-resistant Staphylococcus aureus (MRSA).7,8 In this case, the infant developed pyomyositis and osteomyelitis at the site of the hepatitis B vaccine injection. Based on available medical records, the vaccination was administered at a primary healthcare center; however, detailed documentation regarding vaccination practices (skin antisepsis, injection technique, needle handling, and post-injection monitoring) was unavailable, precluding formal assessment of adherence to aseptic technique and representing an important limitation of this report. Although a direct causal relationship cannot be definitively established, the temporal association between intramuscular vaccination and subsequent invasive MRSA infection raises important considerations regarding injection safety practices in infants.
From a pathophysiological perspective, a biologically plausible pathway may explain this association, whereby injection-related microtrauma facilitates inoculation of cutaneous flora into deeper tissues, particularly in infants with an immature immune system and underdeveloped skin barrier. While vaccination itself is not causative, breaches in aseptic technique during intramuscular injection may increase the risk of bacterial entry at the injection site.8,9 This observation underscores the importance of strict adherence to aseptic injection practices, adequate training of primary healthcare workers, and vigilant surveillance of adverse events following immunization (AEFI).10 Strengthening these preventive measures aims to minimize the risk of rare yet serious post-injection complications while maintaining confidence in routine immunization programs.
In addition to limitations in vaccination practice documentation, detailed documentation of the early medical evaluations at the referring facilities was limited. Available information suggests that the patient received symptomatic treatment during the initial course of illness, without comprehensive sepsis evaluation appropriate for young infants or empiric intravenous antibiotic therapy. This delay in appropriate evaluation and treatment may have contributed to disease progression and deep tissue involvement. In addition, the lack of early antimicrobial coverage against MRSA could have facilitated ongoing infection. This represents an important limitation of the present report and underscores the need for strict adherence to fever protocols for neonates and young infants at primary healthcare facilities.
The susceptibility of infants to invasive MRSA infection is further influenced by host factors, including reduced neutrophil function, impaired phagocytic activity, and suboptimal pro-inflammatory cytokine responses, which collectively increase vulnerability to invasive infections.11 In this case, both blood and pus cultures yielded MRSA, supporting the diagnosis of an invasive infection. Staphylococcus aureus possesses multiple virulence factors that facilitate adhesion to host tissues, invasion, and evasion of host immune defenses, enabling dissemination to deep soft tissue and bone. Invasive musculoskeletal infections may occur through hematogenous spread or direct inoculation and typically present with localized swelling, tenderness, and fever.12
The resistance profile of the isolate in this case was consistent with patterns commonly observed in community-associated MRSA (CA-MRSA), which typically exhibit resistance to β-lactam antibiotics while remaining susceptible to non-β-lactam agents such as vancomycin and linezolid.13 The occurrence of deep soft tissue and bone involvement in an otherwise healthy infant raises concern for a potentially virulent strain. Certain CA-MRSA lineages harbor virulence determinants, including Panton-Valentine leukocidin (PVL), which have been associated with severe skin and soft tissue infections and invasive musculoskeletal disease, even in patients without traditional risk factors.14,15 However, molecular characterization and virulence factor profiling were not performed in this case, representing an important limitation of this report. Future studies incorporating molecular typing may help clarify the epidemiology and virulence profiles of invasive MRSA strains in early infancy.
Given the severity of infection in a young male infant and the involvement of catalase-producing Staphylococcus aureus, an underlying primary immunodeficiency, particularly chronic granulomatous disease (CGD), should be considered. Comprehensive immunologic evaluation was not performed due to resource limitations and prioritization of acute clinical management. Although there was no history of recurrent infections or family history suggestive of immunodeficiency, the absence of formal immunologic testing precludes definitive exclusion of CGD or other inborn errors of immunity and represents an important limitation of this report.
Although pyomyositis is more commonly encountered in tropical regions and predominantly affects young children aged 2-5 years, its occurrence in early infancy is rare. In this case, MRSA was isolated from both aspirated abscess material and blood cultures, confirming invasive musculoskeletal infection. Procedure-related factors during intramuscular injection may have facilitated bacterial entry into deeper tissues, particularly if microtrauma or breaches in aseptic technique occurred.16,17
Infant osteomyelitis has unique features, including rapid spread from the metaphysis to the epiphysis because of vascular anastomoses in infants. Infection may extend between bone and nearby muscle tissues, as seen in this case, where both areas were affected.18 Managing MRSA infections requires proper antibiotic treatment. Empirically, infants suspected of having severe Staphylococcus aureus infections are often given intravenous vancomycin, especially when MRSA is a concern.19 In this case, the patient received vancomycin guided by susceptibility testing.
Vancomycin is frequently used to treat invasive MRSA infections in children, but its administration requires careful monitoring due to risks of nephrotoxicity and treatment failure linked to subtherapeutic levels. In cases of osteomyelitis and pyomyositis, especially in infants, treatment is often extended over several weeks, depending on the severity and clinical response. Monitoring clinical signs and laboratory markers, such as C-reactive protein, is crucial for evaluating treatment effectiveness. Along with antimicrobial therapy, surgical drainage or aspiration is often necessary to manage abscesses and obtain microbiological samples for targeted treatment.20
Complications of invasive MRSA infections in infants may include sepsis and long-term musculoskeletal sequelae; therefore, early recognition and aggressive, targeted management are crucial to improve clinical outcomes.21 In the present case, timely referral and appropriate antimicrobial therapy after culture confirmation may have contributed to the favorable clinical response. This report highlights the importance of maintaining a high index of suspicion for deep soft tissue and musculoskeletal infection in young infants presenting with localized swelling and fever following intramuscular procedures, to facilitate prompt diagnostic evaluation and intervention. Systematic reporting of rare but serious post-injection infections is essential to improve clinical awareness and inform preventive strategies, while reinforcing the overall safety and public health value of routine immunization programs.22
Methicillin-resistant Staphylococcus aureus (MRSA) is an opportunistic pathogen capable of causing severe soft tissue and bone infections in infants. Improper injection technique or compromised host immunity may allow MRSA to invade deep tissues, leading to pyomyositis and osteomyelitis. Strict adherence to aseptic procedures during vaccination and prompt recognition and management of rare complications are essential to prevent progression to systemic infection and improve patient outcomes.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
DATA AVAILABILITY
All datasets generated or analyzed during this study are included in the manuscript.
ETHICS STATEMENT
Not applicable.
INFORMED CONSENT
Written informed consent was obtained from the participant before enrolling in the study.
- Weber S, Schlaeppi C, Barbey F, et al. Clinical Characteristics and Management of Children and Adolescents Hospitalized With Pyomyositis. Pediatr Infect Dis J. 2024;43(9):831-840.
Crossref - Habeych ME, Trinh T, Crum-Cianflone NF. Purulent infectious myositis (formerly tropical pyomyositis). J Neurol Sci. 2020;413:116767.
Crossref - Nasiroglu O, Camargo S, Khan M. Pyomyositis resulting in abscess in an infant and in osteomyelitis in a healthy teenager without fever case reports and literature review. J Pediatr Surg Case Rep. 2021;65:101712.
Crossref - Liu WT, Chen EZ, Yang L, et al. Emerging resistance mechanisms for 4 types of common anti-MRSA antibiotics in Staphylococcus aureus: A comprehensive review. Microb Pathog. 2021;156:104915.
Crossref - Garbo V, Venuti L, Albano C, et al. Investigating Osteomyelitis as a Rare Adverse Effect of Vaccination in the Pediatric Population. Pathogens. 2024;13(11):972.
Crossref - Qiao Y, Liu X, Li B, et al. Treatment of MRSA-infected osteomyelitis using bacterial capturing, magnetically targeted composites with microwave-assisted bacterial killing. Nat Commun. 2020;11(1):4446.
Crossref - Park JW, Park S, Lee E, et al. Latent factors affecting safer injection practices that can reduce infections and how education can improve them. PLoS One. 2024;19(10):e0308567.
Crossref - Silva L, Lemos S, Cabral J, Alves C. Intramuscular abscess following routine newborn immunization: a case report. J Med Case Rep Case Series. 2022;3(2):108.
Crossref - Rincon JC, Wang D, Polcz VE, et al. Innate immune training in the neonatal response to sepsis. Mol Med. 2025;31(1):159.
Crossref - Jabbar F, Kadhim KA, Alhilfi RA, et al. Advancements in monitoring adverse events following immunization in Iraq: Insights from the CIVIE project 2022-2023. Vaccine. 2026;72:128121.
Crossref - Kumar SKM, Bhat BV. Distinct mechanisms of the newborn innate immunity. Immunol Lett. 2016;173:42-54.
Crossref - Rasquel-Oliveira FS, Ribeiro JM, Martelossi-Cebinelli G, et al. Staphylococcus aureus in inflammation and pain: update on pathologic mechanisms. Pathogens. 2025;14(2):185.
Crossref - Alghamdi BA, Al-Johani I, Al-Shamrani JM, et al. Antimicrobial resistance in Methicillin-resistant Staphylococcus aureus. Saudi J Biol Sci. 2023;30(4):103604.
Crossref - Alzomor O, Alfawaz T, Alshahrani D. Invasive community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) infection in children: case series and literature review. Int J Pediatr Adolesc Med. 2017;4(3):119-123.
Crossref - Rallis D, Atzemoglou N, Kapetaniou K, Giaprou LE, Baltogianni M, Giapros V. Molecular Epidemiology Clinical Manifestations, Decolonization Strategies, and Treatment Options of Methicillin-Resistant Staphylococcus aureus Infection in Neonates. Pathogens. 2025;14(2):155.
Crossref - Radcliffe C, Gisriel S, Niu YS, Peaper D, Delgado S, Grant M. Pyomyositis and Infectious Myositis: A Comprehensive, Single-Center Retrospective Study. Open Forum Infect Dis. 2021;8(4):ofab098.
Crossref - Higuchi C, Otsuki D, Kobayashi M, et al. Characteristics of pyomyositis at a pediatric hospital in Osaka, Japan. Cureus. 2025;17(6):e86325.
Crossref - Desimpel J, Posadzy M, Vanhoenacker FM. The Many Faces of Osteomyelitis: A Pictorial Review. J Belg Soc Radiol. 2017;101(1):24.
Crossref - Sanchez PJ, Moallem M, Cantey JB, Milton A, Michelow IC. Empiric therapy with vancomycin in the neonatal intensive care unit: let’s “get smart” globally! J Pediatr (Rio J). 2016;92(5):432-435.
Crossref - Kalu IC, Kao CM, Fritz SA. Management and Prevention of Staphylococcus aureus Infections in Children. Infect Dis Clin North Am. 2022;36(1):73-100.
Crossref - Wu X, Wang C, He L, et al. Clinical characteristics and antibiotic resistance profile of invasive MRSA infections in newborn inpatients: a retrospective multicenter study from China. BMC Pediatr. 2023;23(1):264.
Crossref - Tang CT, Nguyen DT, Ngo TH, et al. An outbreak of severe infections with community-acquired MRSA carrying the Panton-Valentine leukocidin following vaccination. PLoS One. 2007;2(9):e822.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.